
Performance of Urine Reagent Strips in Detecting the Presence and Estimating the Prevalence and Intensity of Schistosoma haematobium Infection

Abstract
:1. Introduction
2. Methods
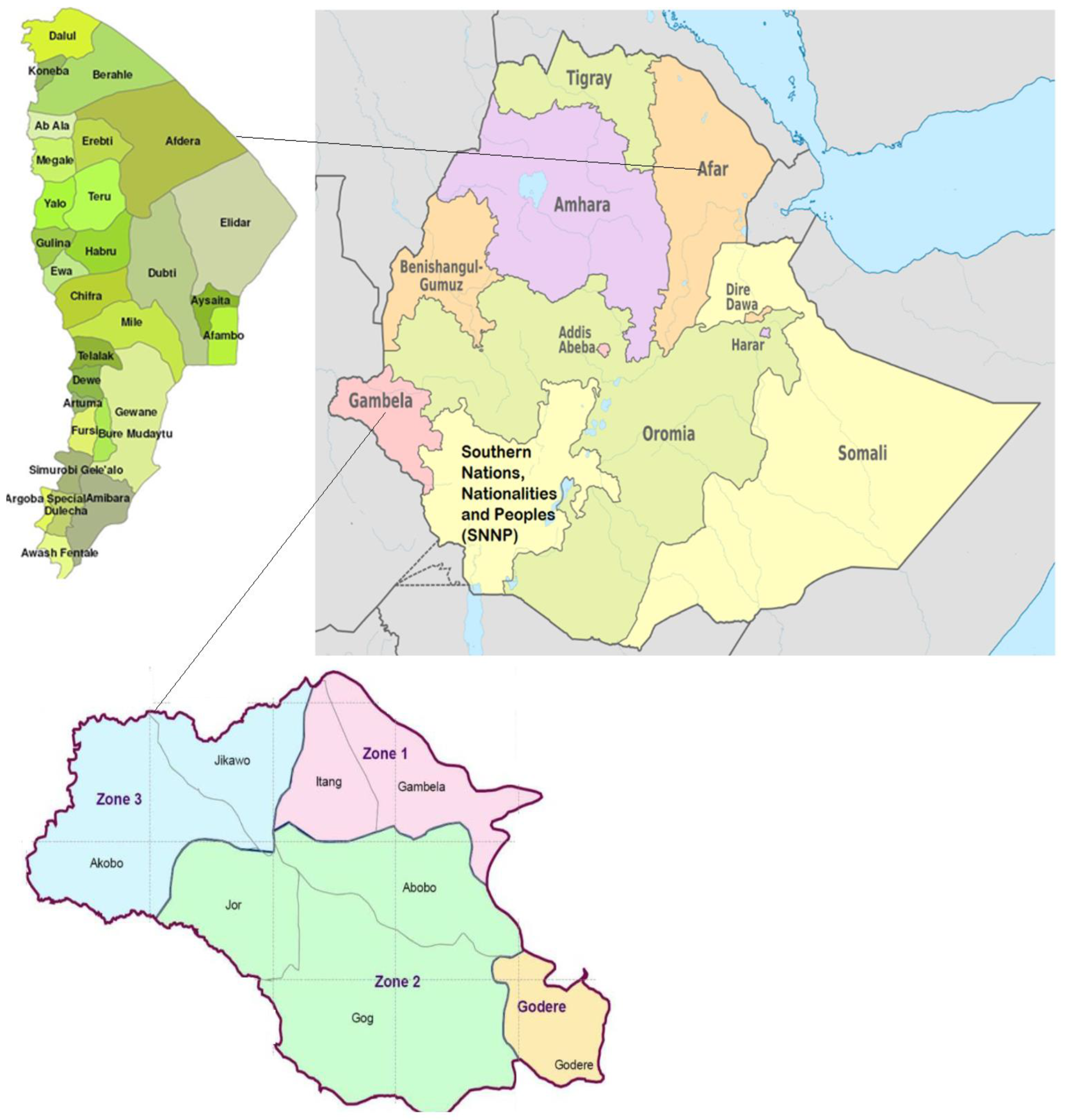
2.1. Study Area and Population
2.2. Study Design and Sample Size
2.3. Urine Sample Collection and Examination for Schistosoma haematobium Infection
2.4. Ethical Consideration
2.5. Data Analysis
3. Results
3.1. Prevalence of S. haematobium Infection Using Urine Filtration and Urine Reagent Strips
3.2. Intensity of S. haematobium Infection Using Urine Filtration and Urine Reagent Strips
3.3. Comparison of the Urine Filtration and the Urine Reagent Strips in Detecting the Presence and Estimating the Intensity of S. haematobium Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Webster, B.L.; Southgate, V.R.; Littlewood, D.T. A revision of the interrelationships of Schistosoma including the recently described Schistosoma guineensis. Int. J. Parasitol. 2006, 36, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Gray, D.J.; Ross, A.G.; Li, Y.S.; McManus, D.P. Diagnosis and management of schistosomiasis. Br. Med. J. 2011, 342, d2651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mutapi, F.; Maizels, R.; Fenwick, A.; Woolhouse, M. Human schistosomiasis in the post mass drug administration era. Lancet Infect. Dis. 2017, 17, e42–e48. [Google Scholar] [CrossRef] [Green Version]
- McManus, D.P.; Dunne, D.W.; Sacko, M.; Utzinger, J.; Vennervald, B.J.; Zhou, X.N. Schistosomiasis. Nat. Rev. Dis. Primers 2018, 4, 13. [Google Scholar] [CrossRef] [PubMed]
- Geleta, S.; Alemu, A.; Getie, S.; Mekonnen, Z.; Erko, B. Prevalence of urinary schistosomiasis and associated risk factors among Abobo Primary School children in Gambella Regional State, southwestern Ethiopia: A cross sectional study. Parasit Vectors 2015, 8, 215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, A.; Erko, B.; Woldemichael, T.; Kloos, H. Epidemiology and Ecology of Health and Disease in Ethiopia; Berhane, Y., Mariam, D.H., Kloos, H., Eds.; Shama Books: Addis Ababa, Ethiopia, 2005; pp. 660–673. [Google Scholar]
- Degarege, A.; Mekonnen, Z.; Levecke, B.; Legesse, M.; Negash, Y.; Vercruysse, J.; Erko, B. Prevalence of Schistosoma haematobium Infection among School-Age Children in Afar Area, Northeastern Ethiopia. PLoS ONE 2015, 10, e0133142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayele, B.; Erko, B.; Legesse, M.; Hailu, A.; Medhin, G. Evaluation of circulating cathodic antigen (CCA) strip for diagnosis of urinary schistosomiasis in Hassoba school children, Afar, Ethiopia. Parasite 2008, 15, 69–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deribew, K.; Yewhalaw, D.; Erko, B.; Mekonnen, Z. Urogenital schistosomiasis prevalence and diagnostic performance of urine filtration and urinalysis reagent strip in schoolchildren, Ethiopia. PLoS ONE 2022, 17, e0271569. [Google Scholar] [CrossRef]
- Negussu, N.; Mengistu, B.; Kebede, B.; Deribe, K.; Ejigu, E.; Tadesse, G.; Mekete, K.; Sileshi, M. Ethiopia Schistosomiasis and Soil-Transmitted Helminthes Control Programme: Progress and Prospects. Ethiop. Med. J. 2017, 55, 75–80. [Google Scholar] [PubMed]
- Ezeamama, A.E.; Bustinduy, A.L.; Nkwata, A.K.; Martinez, L.; Pabalan, N.; Boivin, M.J.; King, C.H. Cognitive deficits and educational loss in children with schistosome infection-A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2018, 12, e0005524. [Google Scholar] [CrossRef] [PubMed]
- Colley, D.G. Morbidity control of schistosomiasis by mass drug administration: How can we do it best and what will it take to move on to elimination? Trop. Med. Health 2014, 42, 25–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stothard, J.R.; Stanton, M.C.; Bustinduy, A.L.; Sousa-Figueiredo, J.C.; Van Dam, G.J.; Betson, M.; Waterhouse, D.; Ward, S.; Allan, F.; Hassan, A.A.; et al. Diagnostics for schistosomiasis in Africa and Arabia: A review of present options in control and future needs for elimination. Parasitology 2014, 141, 1947–1961. [Google Scholar] [CrossRef] [PubMed]
- Ochodo, E.A.; Gopalakrishna, G.; Spek, B.; Reitsma, J.B.; van Lieshout, L.; Polman, K.; Lamberton, P.; Bossuyt, P.M.; Leeflang, M.M. Circulating antigen tests and urine reagent strips for diagnosis of active schistosomiasis in endemic areas. Cochrane Database Syst. Rev. 2015, 11, CD009579. [Google Scholar] [CrossRef] [Green Version]
- Peters, P.A.; Mahmoud, A.A.; Warren, K.S.; Ouma, J.H.; Siongok, T.K. Field studies of a rapid, accurate means of quantifying Schistosoma haematobium eggs in urine samples. Bull. World Health Organ. 1976, 54, 159–162. [Google Scholar] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, C.H.; Bertsch, D. Meta-analysis of Urine Heme Dipstick Diagnosis of Schistosoma haematobium Infection, Including Low-Prevalence and Previously-Treated Populations. PLoS Negl. Trop. Dis. 2013, 7, e2431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elsiddig, H.A.; Khider, E.; Nour, S.M.; Abdelrafie, A.M.; Mogadam, M.B. Prevalence of urinary Schistosomiasis among schoolchildren in White Nile State, Sudan. Afr. Educ. Res. J. 2019, 7, 29–32. [Google Scholar] [CrossRef]
- Senghor, B.; Diallo, A.; Sylla, S.N.; Doucouré, S.; Ndiath, M.O.; Gaayeb, L.; Djuikwo-Teukeng, F.F.; Bâ, C.T.; Sokhna, C. Prevalence and intensity of urinary Schistosomiasis among schoolchildren in the district of Niakhar, region of Fatick, Senegal. Parasit Vectors 2014, 7, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sady, H.; Al-Mekhlafi, H.M.; Mahdy, M.A.; Lim, Y.A.; Mahmud, R.; Surin, J. Prevalence and associated factors of Schistosomiasis among children in Yemen: Implications for an effective control program. PLoS Negl. Trop. Dis. 2013, 7, e2377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diagnostic Target Product Profiles for Monitoring, Evaluation and Surveillance of Schistosomiasis Control Programmes; World Health Organization: Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/9789240031104 (accessed on 13 October 2022).
- Brown, M.A.; Holt, J.L.; Mangos, G.J.; Muray, N.; Curtis, J.; Homer, C. Microscopic hematuria in pregnancy: Relevance to pregnancy outcome. Am. J. Kidney Dis. 2005, 45, 667–673. [Google Scholar] [CrossRef] [PubMed]
- McDonald, M.M.; Swagerty, D.; Wetzel, L. Assessment of microscopic hematuria in adults. Am. Fam. Physician 2006, 73, 1748–1754. [Google Scholar] [PubMed]
- Hatz, C.; Savioli, L.; Mayombana, C.; Dhunputh, J.; Kisumku, U.M.; Tanner, M. Measurement of schistosomiasis-related morbidity at community level in areas of different endemicity. Bull. World Health Organ. 1990, 68, 777–787. [Google Scholar] [PubMed]
- Doehring, E.; Reider, F.; Schmidt-Ehry, G.; Ehrich, J.H.H. Reduction of pathological findings in urine and bladder lesions in infection with Schistosoma haematobium after treatment with praziquantel. J. Infect. Dis. 1985, 152, 807–810. [Google Scholar] [CrossRef] [PubMed]
- Ugbomoiko, U.S.; Obiezue, R.N.N.; Ogunniyi, T.A.B.; Ofoezie, I.E. Diagnostic accuracy of different urine dipsticks to detect urinary schistosomiasis: A comparative study in five endemic communities in Osun and Ogun states, Nigeria. J. Helminthol. 2009, 83, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Picon, D.; Sturrock, H.J.; Sabasio, A.; Lado, M.; Kolaczinski, J.; Brooker, S. The performance of haematuria reagent strips for the rapid mapping of urinary schistosomiasis: Field experience from Southern Sudan. Trop. Med. Int. Health 2009, 14, 1484–1487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lengeler, C.; Mshinda, H.; Morona, D.; de Savigny, D. Urinary schistosomiasis-testing with urine filtration and reagent sticks for hematuria provides a comparable prevalence estimate. Acta Trop. 1993, 53, 39–50. [Google Scholar] [CrossRef]
- Mott, K.E.; Dixon, H.; Osei-Tutu, E.; England, E.C. Relation between intensity of Schistosoma haematobium infection and clinical haematuria and proteinuria. Lancet 1983, 321, 1005–1008. [Google Scholar] [CrossRef]
- Taylor, P.; Chandiwana, S.K.; Matanhire, D. Evaluation of the reagent strip test for haematuria in the control of Schistosoma haematobium infection in schoolchildren. Acta Trop. 1990, 47, 91–100. [Google Scholar] [CrossRef]
- Van Etten, L.; Kremsner, P.G.; Krijger, F.W.; Deelder, A.M. Day-to-day variation of egg output and schistosome circulating antigens in urine of Schistosoma haematobium-infected school children from Gabon and follow-up after chemotherapy. Am. J. Trop. Med. Hyg. 1997, 57, 337–341. [Google Scholar] [CrossRef]
- Knopp, S.; Ame, S.M.; Hattendorf, J.; Ali, S.M.; Khamis, I.S.; Bakar, F.; Khamis, M.A.; Person, B.; Kabole, F.; Rollinson, D.; et al. Urogenital schistosomiasis elimination in Zanzibar: Accuracy of urine filtration and haematuria reagent strips for diagnosing light intensity Schistosoma haematobium infections. Parasites Vectors 2018, 11, 552. [Google Scholar] [CrossRef]
- Weerakoon, K.G.; Gordon, C.A.; McManus, D.P. DNA Diagnostics for Schistosomiasis Control. Trop. Med. Infect. Dis. 2018, 3, 81. [Google Scholar] [CrossRef] [PubMed]
- WHO. Schistosomiasis: Progress Report 2001–2011, Strategic Plan 2012–2020; World Health Organization: Geneva, Switzerland, 2017; Available online: https://apps.who.int/iris/handle/10665/78074 (accessed on 24 September 2022).
- WHO. Helminth Control in School-Age Children: A Guide for Managers of Control Programmes; World Health Organization: Geneva, Switzerland, 2011; Available online: https://apps.who.int/iris/handle/10665/44671 (accessed on 24 September 2022).


{kind=link}
| Variables | Category | Number Examined | Percent Positive Based on Urine Filtration | Percent Positive Based on Urine Reagent Strips |
|---|---|---|---|---|
| Age in years | 5 to 9 | 665 | 27.1 | 28.7 |
| 10 to 15 | 623 | 36.4 | 35.8 | |
| p-value | <0.001 | 0.007 | ||
| Gender | Female | 538 | 30.1 | 30.0 |
| Male | 750 | 32.7 | 33.7 | |
| p-value | 0.342 | 0.155 | ||
| Villages | Buri | 352 | 34.4 | 38.9 |
| Kusra | 256 | 25.4 | 26.2 | |
| Hassoba | 131 | 0.76 | 3.1 | |
| Kelhat | 34 | 20.6 | 20.6 | |
| Andada | 37 | 10.8 | 13.5 | |
| Abobo | 478 | 43.7 | 40.6 | |
| p-value | <0.001 | <0.001 | ||
| Regions | Afar | 810 | 24.4 | 27.16 |
| Gambella | 478 | 43.7 | 40.59 | |
| p-value | <0.001 | <0.001 |
| Urine Filtration | Urine Reagent Strips | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | Categories | Number Examined | Mean UEC | Light Infections (%) | Heavy Infections (%) | Trace (+/−) | Weak (+) | Moderate (++) | High (+++) |
| Age (years) | 5 to 9 | 665 | 11.36 | 25.86 | 1.20 | 5.71 | 8.87 | 10.08 | 4.06 |
| 10 to 15 | 623 | 14.10 | 34.99 | 1.44 | 6.58 | 10.59 | 13.16 | 5.46 | |
| p-value | 0.279 | 0.001 | 0.085 | ||||||
| Gender | Female | 538 | 7.54 | 29.61 | 0.56 | 6.89 | 9.50 | 10.43 | 3.17 |
| Male | 750 | 16.42 | 30.80 | 1.87 | 5.60 | 9.87 | 12.40 | 5.87 | |
| p-value | <0.01 | 0.106 | 0.072 | ||||||
| Villages | Buri | 352 | 15.18 | 32.67 | 1.70 | 5.68 | 11.93 | 14.20 | 7.10 |
| Kusra | 256 | 23.23 | 25.4 | 1.95 | 3.91 | 10.94 | 7.42 | 3.91 | |
| Hassoba | 131 | 1.00 | 0.76 | 0.00 | 2.29 | 0.76 | 0.00 | 0.00 | |
| Kelhat | 34 | 2.57 | 20.59 | 0.00 | 8.82 | 5.88 | 0.00 | 5.88 | |
| Andada | 37 | 8.75 | 10.81 | 0.00 | 0.00 | 5.41 | 8.11 | 0.00 | |
| Abobo | 478 | 8.82 | 42.47 | 1.26 | | 9.00 | 10.46 | 16.11 | 5.02 | |
| p-value | <0.01 | <0.001 | <0.001 | ||||||
| Regions | Afar | 810 | 17.18 | 23.09 | 1.36 | 4.44 | 9.26 | 8.89 | 4.57 |
| Gambella | 478 | 8.82 | 42.47 | 1.26 | 9.00 | 10.46 | 16.11 | 5.02 | |
| p-value | <0.01 | <0.001 | 0.001 | ||||||
| Level of Hematuria Using the Urine Reagent Strips | |||||
|---|---|---|---|---|---|
| Egg Count per 10 mL Urine Using the Urine Filtration | Negative | Trace (+/−) | Weak (+) | Moderate (++) | High (+++) |
| Negative | 767 | 22 | 48 | 35 | 9 |
| 1–5 | 93 | 38 | 47 | 40 | 16 |
| 6–10 | 10 | 13 | 15 | 24 | 15 |
| 11–15 | 4 | 3 | 4 | 16 | 6 |
| 16–30 | 0 | 2 | 4 | 19 | 6 |
| 31–49 | 0 | 1 | 5 | 6 | 3 |
| ≥50 | 0 | 0 | 2 | 9 | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Degarege, A.; Animut, A.; Negash, Y.; Erko, B. Performance of Urine Reagent Strips in Detecting the Presence and Estimating the Prevalence and Intensity of Schistosoma haematobium Infection. Microorganisms 2022, 10, 2062. https://doi.org/10.3390/microorganisms10102062
Degarege A, Animut A, Negash Y, Erko B. Performance of Urine Reagent Strips in Detecting the Presence and Estimating the Prevalence and Intensity of Schistosoma haematobium Infection. Microorganisms. 2022; 10(10):2062. https://doi.org/10.3390/microorganisms10102062
Chicago/Turabian StyleDegarege, Abraham, Abebe Animut, Yohannes Negash, and Berhanu Erko. 2022. "Performance of Urine Reagent Strips in Detecting the Presence and Estimating the Prevalence and Intensity of Schistosoma haematobium Infection" Microorganisms 10, no. 10: 2062. https://doi.org/10.3390/microorganisms10102062