
Design and Experimental Testing of an Ankle Rehabilitation Robot

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design of the Ankle Rehabilitation Robot
2.1.1. Motivation of the Adopted Solutions
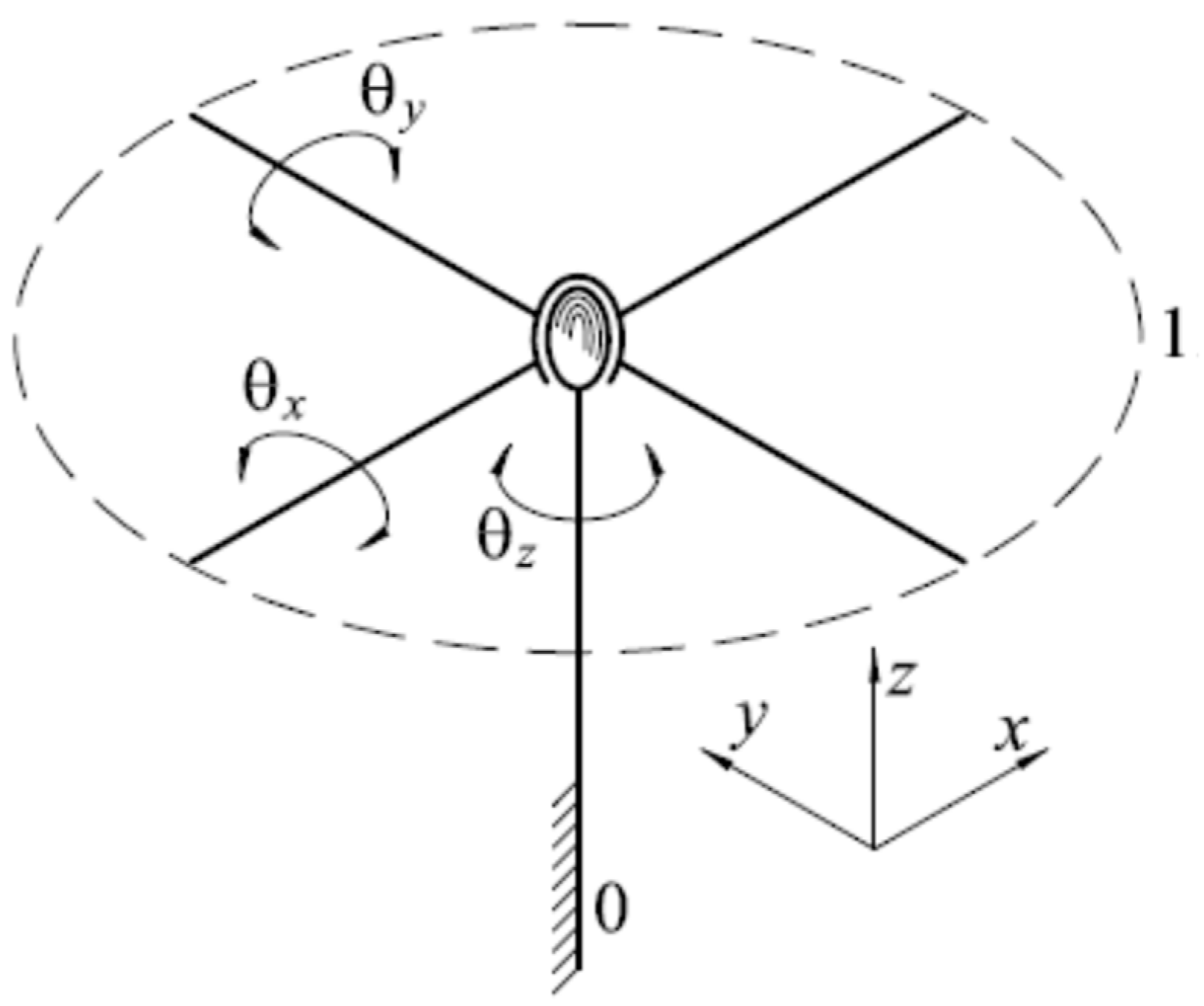
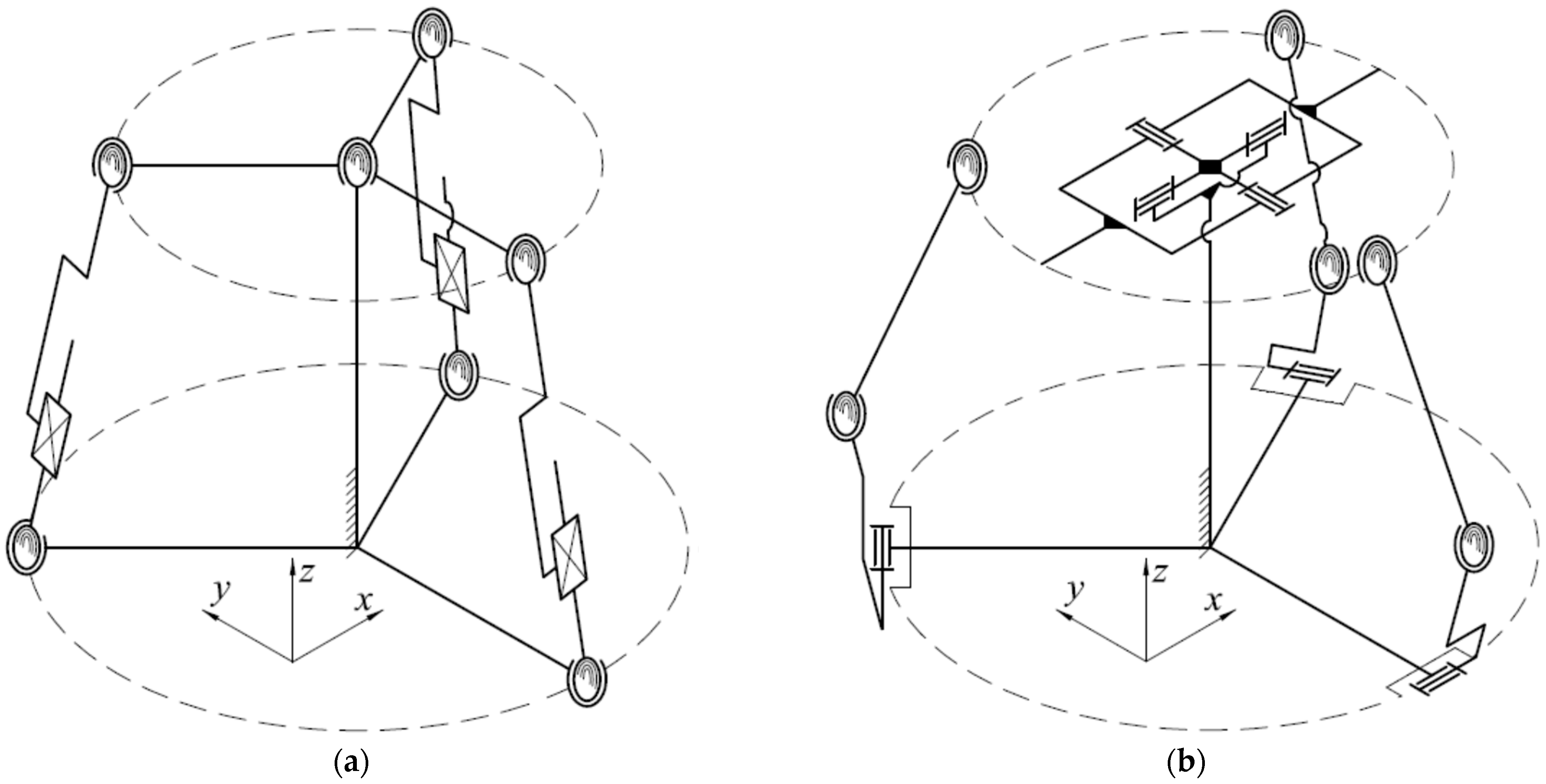
2.1.2. Structural Synthesis
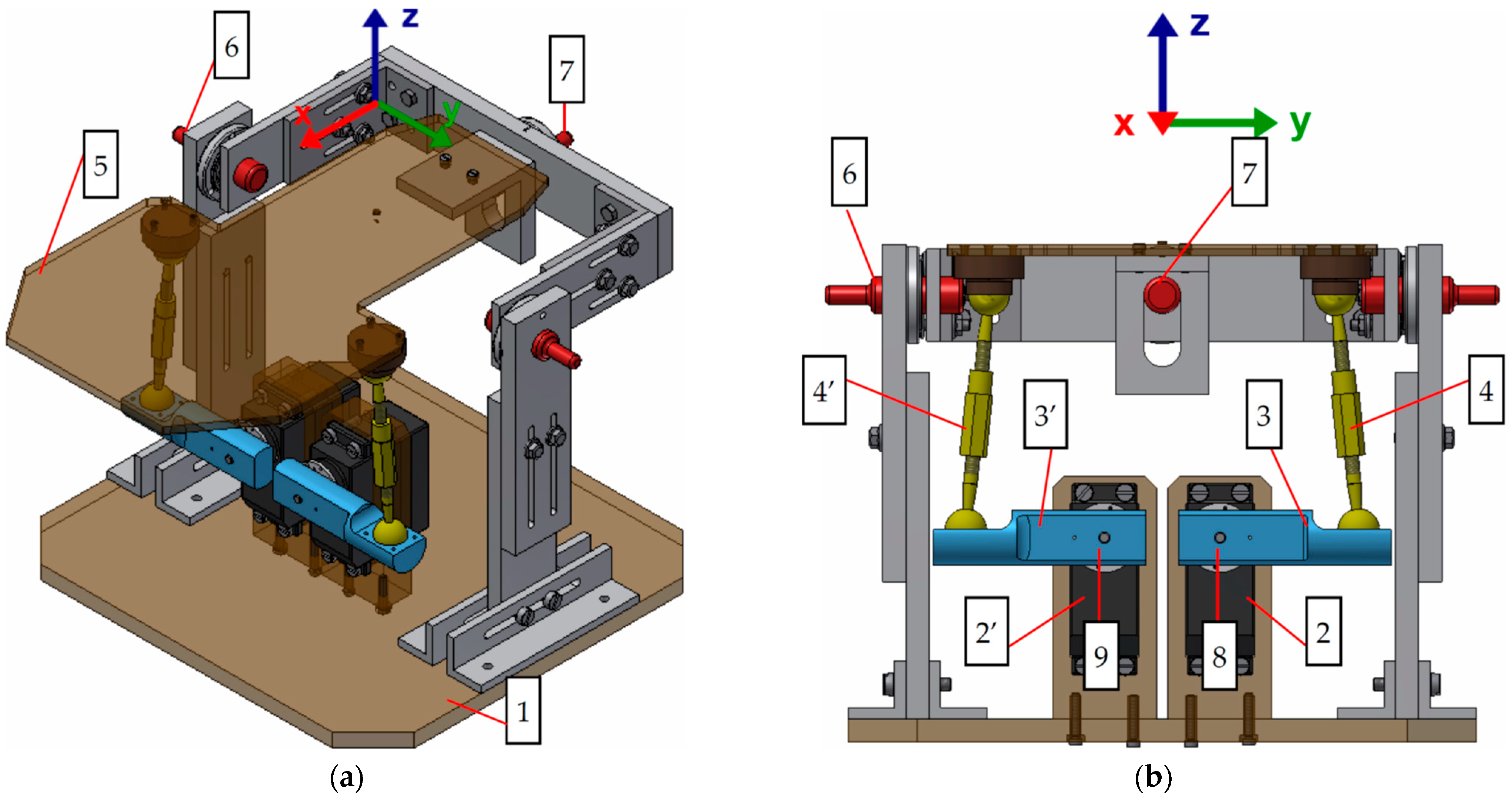
2.1.3. Design Solutions
- RP maintenance (C1)—these criteria take into account the actuator and mechanism type (joints type);
- Simplicity in use (C2)—ease of programming and use by the end user;
- RP cost (C3)—takes into account the cost prices of the components;
- RP overall dimensions (C4)—the overall dimensions and the mass of the platform are very important in choosing the technical solution;
- Minimum blocking probability (C5)—depends on the joints type;
- The DnL range of motion (C6)—the RP should cover the range of motion for both AJ movements considered for rehabilitation.
3. Results
3.1. Mathematical Modeling and Simulation
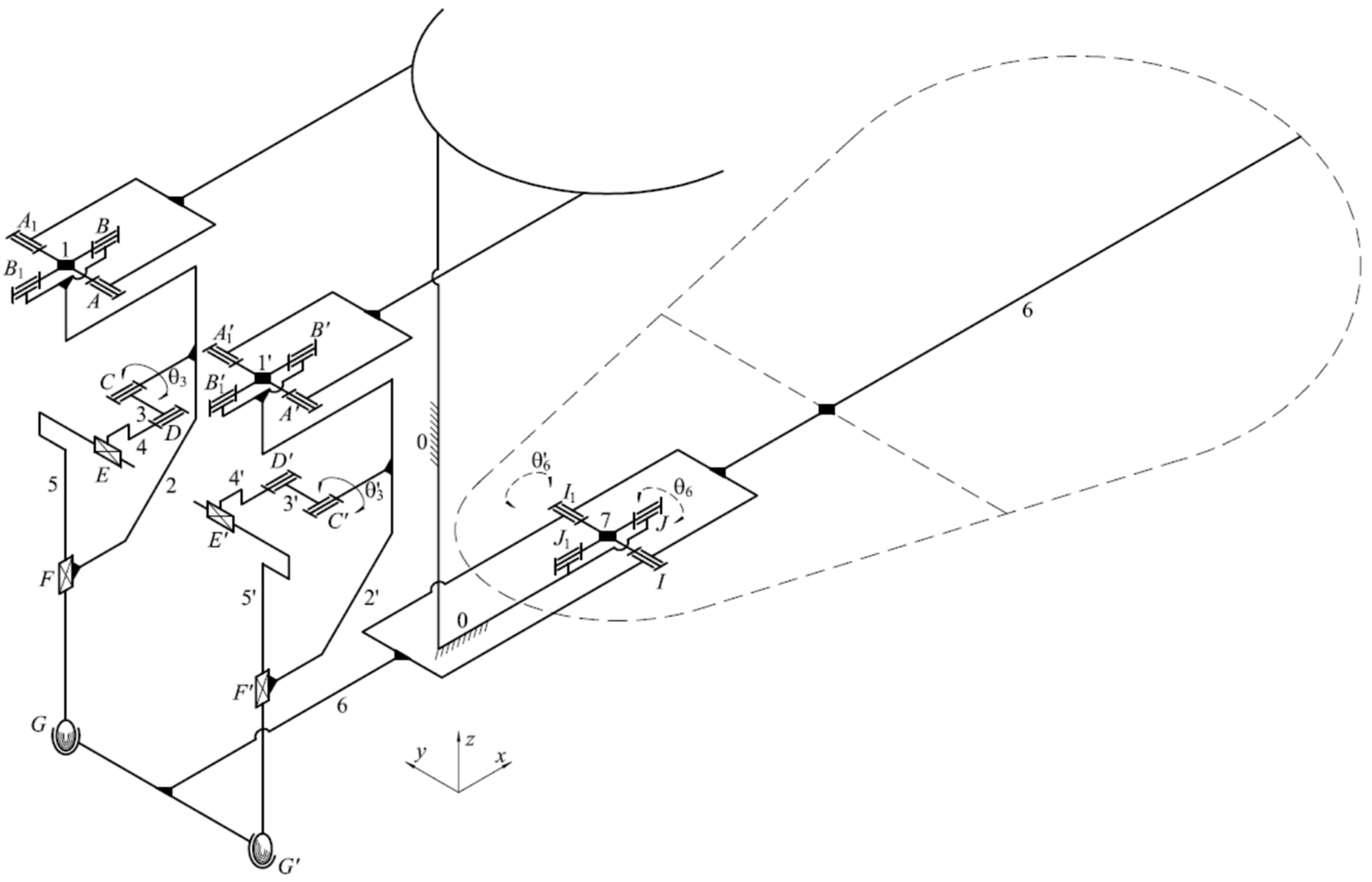
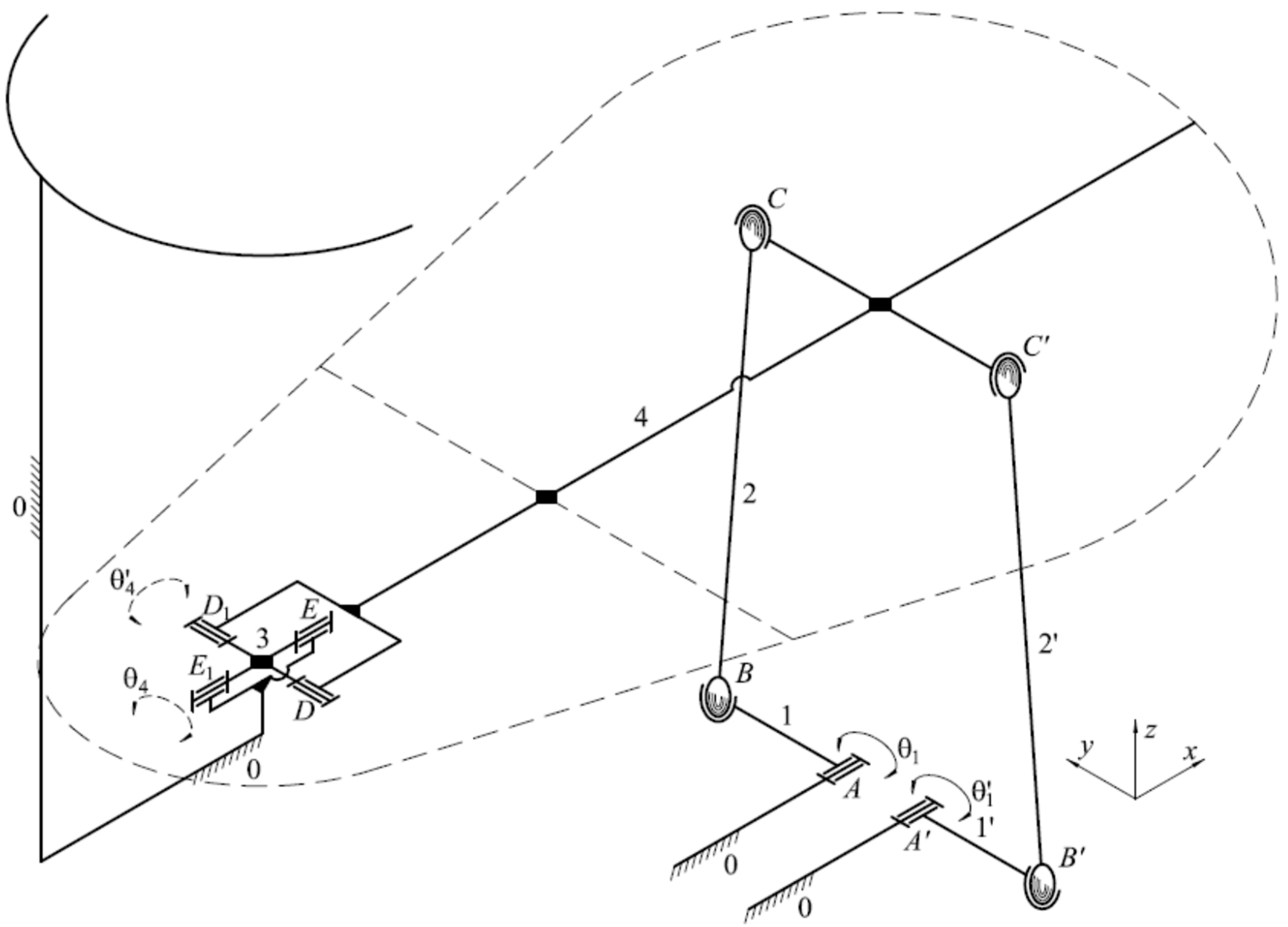
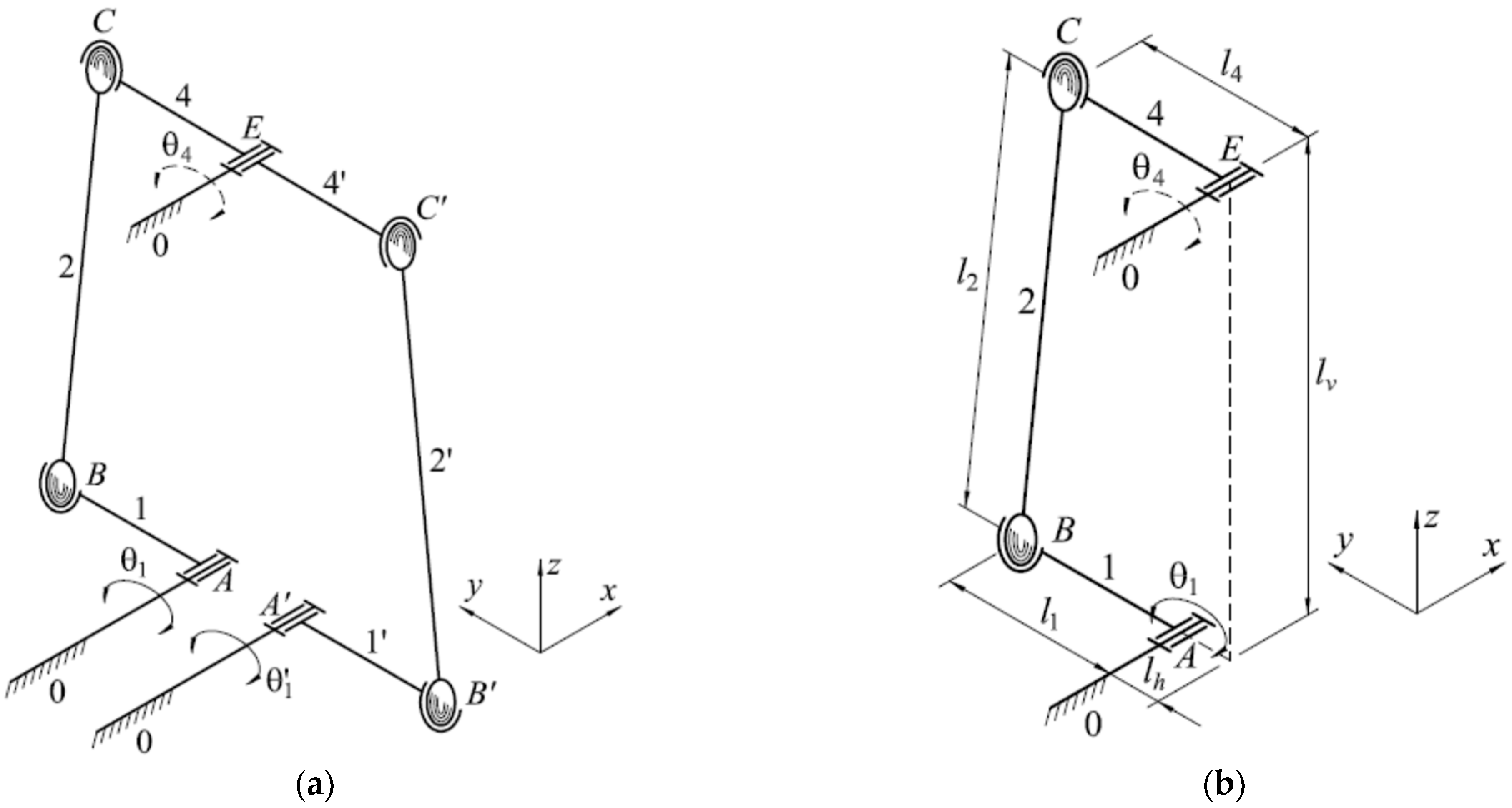
3.1.1. Mathematical Modeling of the DS-3 Design Solution
3.1.2. Dimensional Synthesis and Simulation of the DS-3 Design Solution
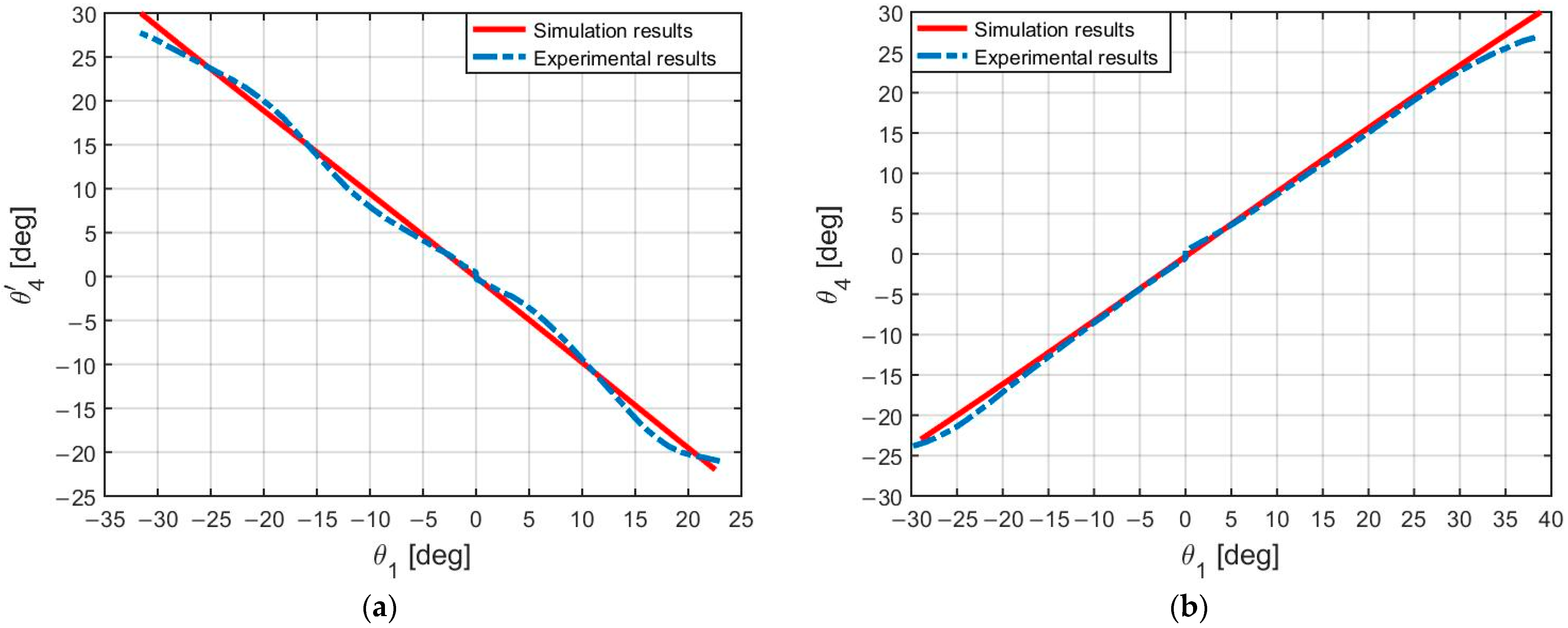
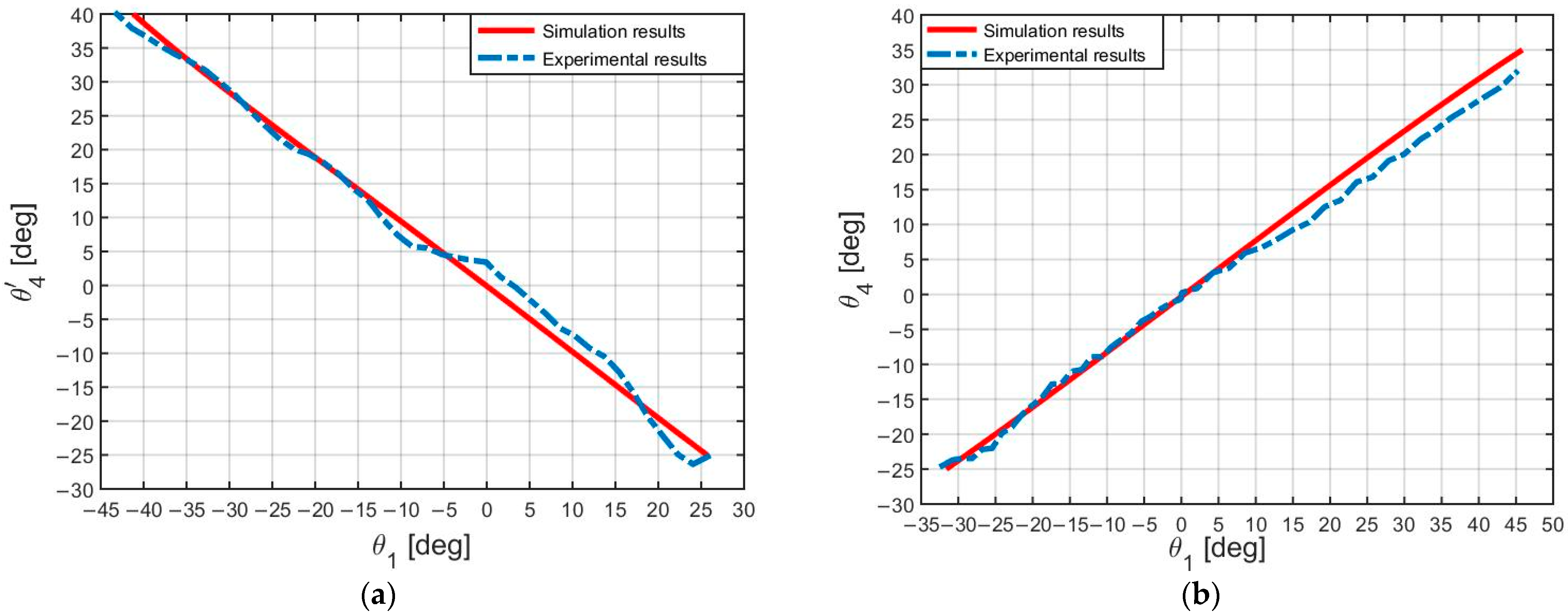
3.2. Experimental Results
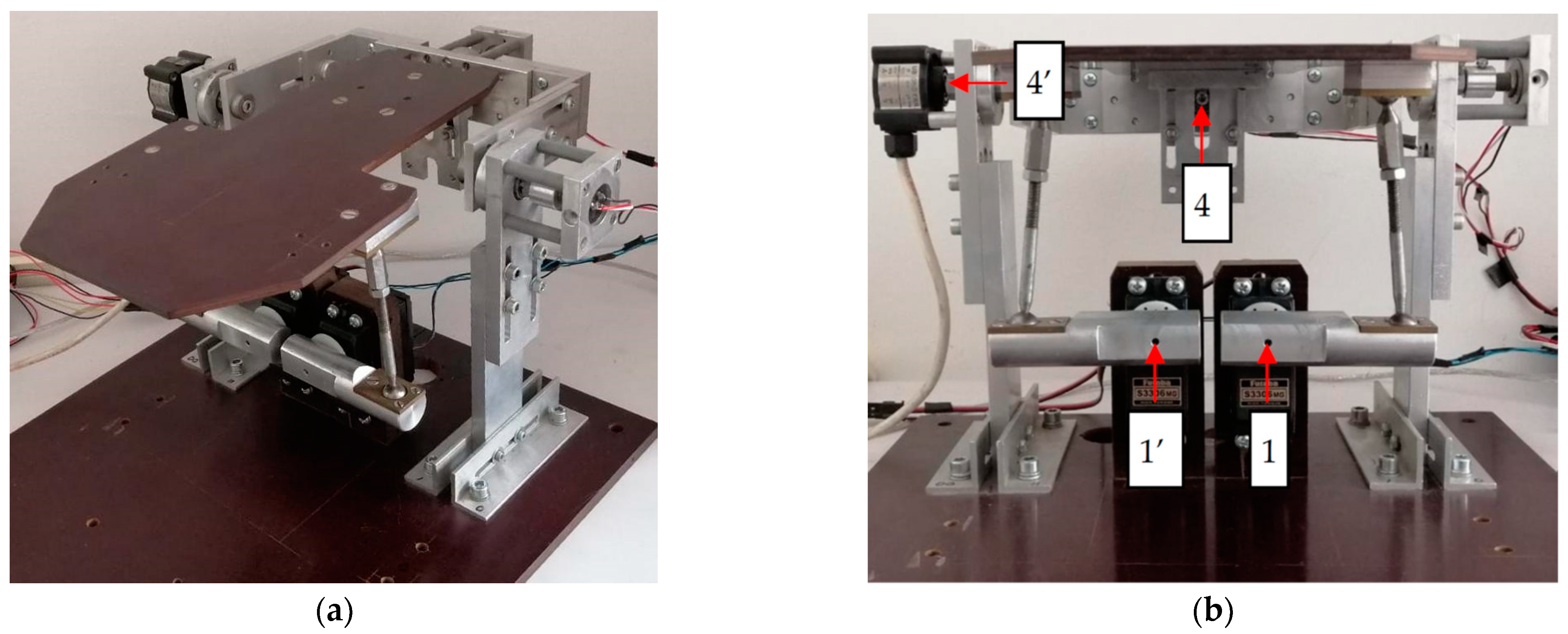
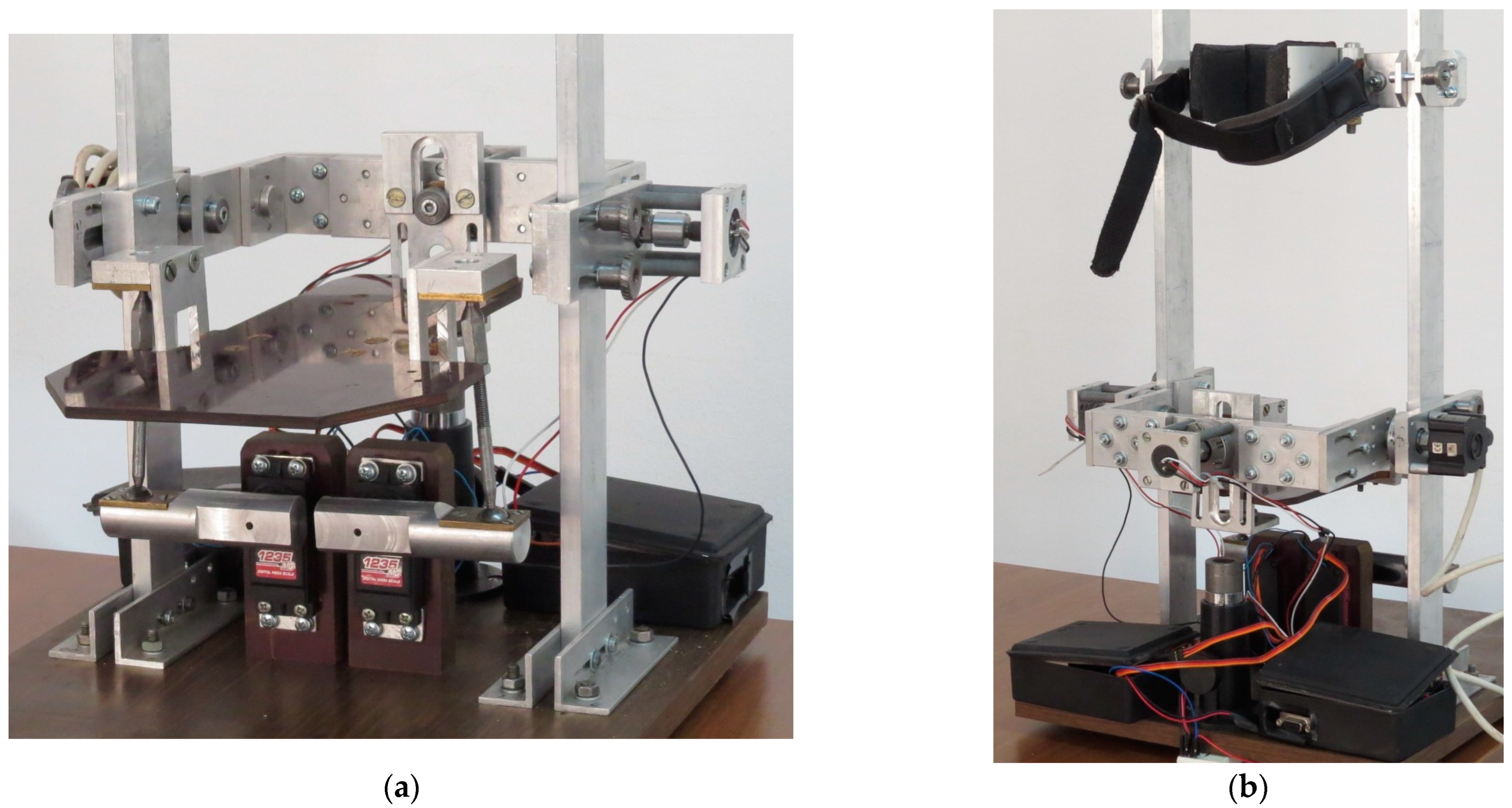
3.2.1. Experimental Platform
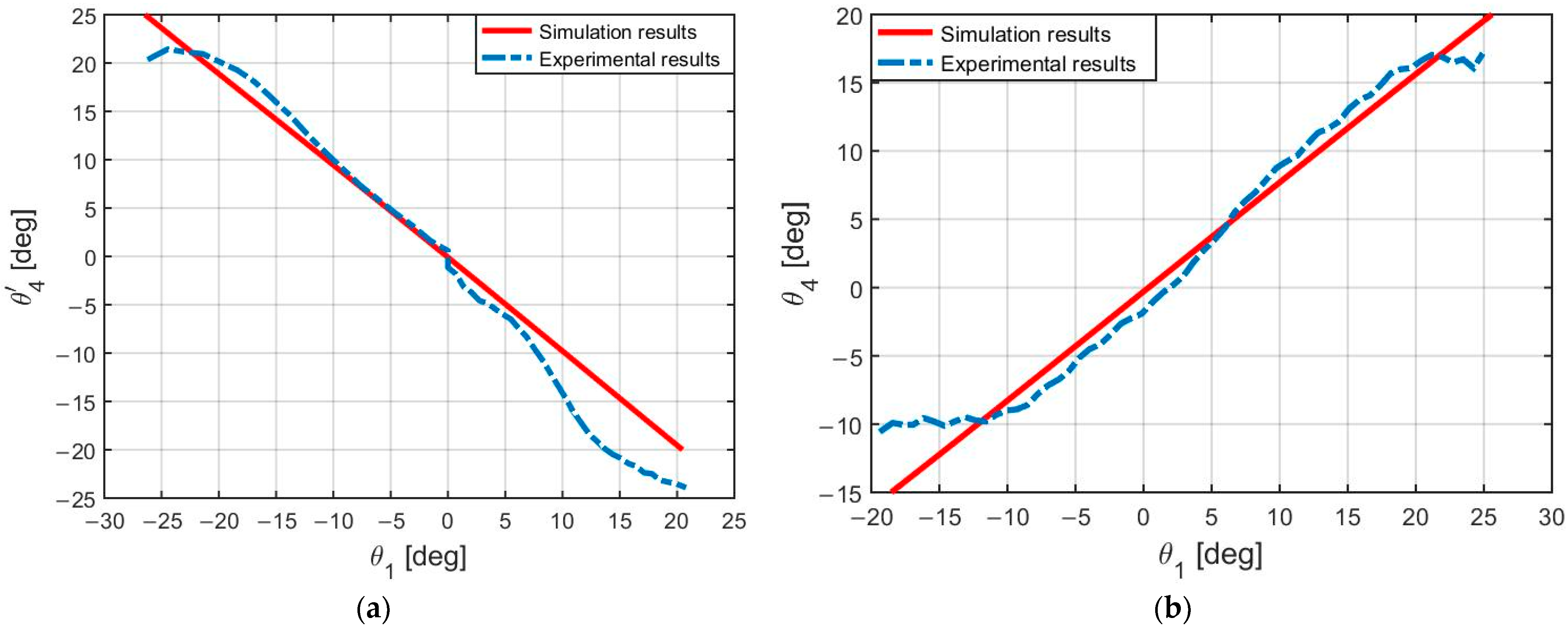
3.2.2. Experimental Tests and Results
3.2.3. Ethical Issues
3.2.4. Safety Issues
3.3. New Proposed Design
4. Discussion
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Valderrabano, V.; Barg, A.; Paul, J.; Pagenstert, G.; Wiewiorski, M. Foot and ankle injuries in professional soccer player. Sport Orthop. Traumatol. 2014, 30, 98–105. [Google Scholar] [CrossRef]
- Park, S.; Hwang, Y.; Kim, H.; Kim, Y. Development of ankle rehabilitation robot with adjustable robotic mechanism. J. Robot. Mechatron. 2016, 28, 157–166. [Google Scholar]
- Kesar, T.M.; Perumal, R.; Jancosko, A.; Reisman, D.S.; Rudolph, K.S.; Higginson, J.S.; Binder-Macleod, S.A. Novel patterns of functional electrical stimulation have an immediate effect on dorsiflexor muscle function during gait for people poststroke. Phys. Ther. 2011, 91, 1717–1728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.J.; Kim, Y.; Cho, K.J. Development of a pneumatic artificial muscle-based ankle rehabilitation robot. Int. J. Precis. Eng. Manuf. 2016, 17, 1251–1259. [Google Scholar]
- Lobo-Prat, J.; Siviy, C.; Reinkensmeyer, D.J. Design and validation of an ankle foot exoskeleton for running. PLoS ONE 2018, 13, e0201184. [Google Scholar]
- Cheung, C.C.; Ng, S.K.; Chan, W.W. Design and control of a wearable ankle rehabilitation robot. IEEE ASME Trans. Mechatron. 2012, 18, 366–375. [Google Scholar]
- Paradiso, R.; Marconi, L.; Farina, D. A novel robotic device for ankle rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2009, 17, 287–295. [Google Scholar]
- Park, H.; Jeong, G.W.; Kim, Y.J. Development of a gait enhancing mobile shoe using machine learning algorithms. PLoS ONE 2018, 13, e0201907. [Google Scholar]
- Dong, M.; Zhou, Y.; Li, J.; Rong, X.; Fan, W.; Zhou, X.; Kong, Y. State of the art in parallel ankle rehabilitation robot: A systematic review. J. NeuroEng. Rehabil. 2021, 18, 1–15. [Google Scholar] [CrossRef]
- Girone, M.; Burdea, G.; Bouzit, M. The Rutgers ankle orthopedic rehabilitation interface. In Proceedings of the ASME Dynamic Systems and Control Division, Nashville, TN, USA, 14–19 November 1999; pp. 305–312. [Google Scholar]
- Yoon, J.; Ryu, J.; Lim, K.B. Reconfgurable ankle rehabilitation robot for various exercises: Research articles. J. Robot. Syst. 2005, 22, 15–33. [Google Scholar] [CrossRef]
- Dai, J.S.; Zhao, T.; Nester, C. Sprained ankle physiotherapy based mechanism synthesis and stifness analysis of a robotic rehabilitation device. Auton. Robot. 2004, 16, 207–218. [Google Scholar] [CrossRef]
- Liu, G.; Gao, J.; Yue, H.; Zhang, X.; Lu, G. Design and kinematics analysis of parallel robots for ankle rehabilitation. In Proceedings of the IEEE/RSJ International Conference on Intelligent Robots & Systems, Beijing, China, 9–15 October 2006; IEEE: Piscataway, NJ, USA, 2006; pp. 253–258. [Google Scholar]
- Saglia, J.A.; Tsagarakis, N.G.; Dai, J.S.; Caldwell, D.G. A high-performance redundantly actuated parallel mechanism for ankle rehabilitation. Int. J. Robot. Res. 2009, 28, 1216–1227. [Google Scholar] [CrossRef]
- Malosio, M.; Negri, S.P.; Pedrocchi, N.; Vicentini, F.; Caimmi, M.; Tosatti, L.M. A spherical parallel three degrees-of-freedom robot for ankle-foot neuro-rehabilitation. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–September 2012; pp. 3356–3359. [Google Scholar]
- Ayas, M.S.; Altas, I.H. Fuzzy logic based adaptive admittance control of a redundantly actuated ankle rehabilitation robot. Control Eng. Pract. 2017, 59, 44–54. [Google Scholar] [CrossRef]
- Ai, Q.; Zhu, C.; Zuo, J.; Meng, W.; Liu, Q.; Xie, S.; Yang, M. Disturbance-estimated adaptive backstepping sliding mode control of a pneumatic muscles-driven ankle rehabilitation robot. Sensors 2018, 18, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamwal, P.K.; Hussain, S.; Ghayesh, M.H.; Rogozina, S.V. Impedance control of an intrinsically compliant parallel ankle rehabilitation robot. IEEE Trans. Ind. Electron. 2016, 63, 3638–3647. [Google Scholar] [CrossRef]
- Zhang, M.; Cao, J.; Zhu, G.; Miao, Q.; Zeng, X.; Xie, S.Q. Reconfgurable workspace and torque capacity of a compliant ankle rehabilitation robot (CARR). Robot. Auton. Syst. 2017, 98, 213–221. [Google Scholar] [CrossRef] [Green Version]
- Tsoi, Y.H.; Xie, S.Q.; Graham, A.E. Design, modeling and control of an ankle rehabilitation robot. In Design and Control of Intelligent Robotic Systems; Liu, D., Wang, L., Tan, K.C., Eds.; Springer: Berlin/Heidelberg, Germany, 2009; pp. 377–399. [Google Scholar]
- Wang, C.; Fang, Y.; Guo, S.; Chen, Y. Design and kinematical performance analysis of a 3—RUS/RRR redundantly actuated parallel mechanism for ankle rehabilitation. J. Mech. Robot. 2013, 5, 041003. [Google Scholar] [CrossRef]
- Valles, M.; Cazalilla, J.; Valera, A.; Mata, V.; Page, A.F.; Diaz-Rodriguez, M. A 3-PRS parallel manipulator for ankle rehabilitation: Towards a low-cost robotic rehabilitation. Robotica 2017, 35, 1939–1957. [Google Scholar] [CrossRef]
- Li, J.; Zuo, S.; Zhang, L.; Dong, M. Mechanical design and performance analysis of a novel parallel robot for ankle rehabilitation. J. Mech. Robot. 2020, 12, 051007. [Google Scholar] [CrossRef]
- Hong, D.; Gong, M.; Li, S.; Lu, W. Design of a Portable and Lightweight Ankle Rehabilitation Robot for Home Use by Stroke Patients. J. Healthc. Eng. 2020, 1–9. [Google Scholar]
- Liu, H.; Jin, R.; Xie, S.; Zhang, X.; Wang, F. Design and Development of a Wearable Ankle Rehabilitation Robot Based on Three-Dimensional Acceleration Sensor. Appl. Sci. 2019, 9, 4058. [Google Scholar]
- Zhou, Z.; Jiang, Y.; Huang, H.; Wei, Q. Design and Control of a Modular Ankle Rehabilitation Robot. J. Healthc. Eng. 2019, 1–12. [Google Scholar]
- Aghaebrahimian, A.; Abdi, A.; Faraji, M. A Smartphone-Based User Interface for an Ankle Rehabilitation Robot. J. Rehabil. Robot. 2019, 3, 63–70. [Google Scholar]
- Kamal, A.; Lemaire, E.D.; Sawan, M. Design and Evaluation of a Gamified User Interface for Home-Based Ankle Rehabilitation. J. Med. Syst. 2021, 45, 1–10. [Google Scholar]
- Wang, L.; Chen, C.; Zheng, R.; Liu, H. Design of a User-Friendly Interface for an Ankle Rehabilitation Robot. IEEE Access 2020, 8, 135509–135517. [Google Scholar]
- Chen, X.; Chen, S.; Chen, W.; Chen, Y.; Guo, X.; Liu, G. Clinical Efficacy and Safety of Home-Based Rehabilitation for Post-Stroke Ankle-Foot Dysfunction Using Ankle Rehabilitation Robot: A Randomized, Controlled Pilot Trial with 24 Weeks of Follow-Up. Clin. Rehabil. 2018, 32, 1174–1184. [Google Scholar]
- Li, R.; Zhang, Y.; Xu, Z.; Li, M. Robot-Assisted Ankle Rehabilitation Training Improves Ankle Function in Patients with Acute Ankle Sprain: A Randomized Controlled Trial. J. Orthop. Surg. Res. 2020, 15, 1–9. [Google Scholar]
- Wang, K.; Wang, Z.; Liu, H. Pilot Study on the Clinical Effect of a Home-Based Ankle Rehabilitation Robot. J. Rehabil. Robot. 2018, 2, 31–38. [Google Scholar]
- Shah Nazar, P.; Pott, P.P. Ankle Rehabilitation Robotic Systems for domestic use—A systematic review. Curr. Dir. Biomed. Eng. 2022, 8, 65–68. [Google Scholar] [CrossRef]
- Cioi, D.; Burdea, G.; Engsberg, J.R.; Janes, W. Ankle control and strength training for children with cerebral palsy using the Rutgers Ankle CP: A case study. In Proceedings of the IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011; p. 5975432. [Google Scholar]
- Roy, A.; Forrester, L.W.; Macko, R. Short-term ankle motor performance with ankle robotics training in chronic hemiparetic stroke. J. Rehabil. Res. Dev. 2011, 48, 417–429. [Google Scholar] [CrossRef]
- Kim, J.; Hwang, S.; Sohn, R.; Lee, Y.; Kim, Y. Development of an Active Ankle Foot Orthosis to Prevent Foot Drop and Toe Drag in Hemiplegic Patients: A Preliminary Study. Appl. Bionics Biomech. 2011, 8, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Ward, J.; Sugar, T.; Boehler, A.; Standeven, J.; Engsberg, J.R. Stroke Survivors’ Gait Adaptations to a Powered Ankle Foot Orthosis. Adv. Robot. 2011, 25, 1879–1901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forrester, L.W.; Roy, A.; Krebs, H.I.; Macko, R.F. Ankle training with a robotic device improves hemiparetic gait after a stroke. Neurorehabilit. Neural Repair 2011, 25, 369–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamwal, P.K.; Sie, S.Q. An Adaptive Wearable Parallel Robot for the Treatment of Ankle Injuries. IEEE/ASME Trans. Mechatron. 2014, 19, 64–75. [Google Scholar] [CrossRef]
- Blanchette, A.K.; Noel, M.; Richards, C.L.; Nadeau, S.; Bouyer, L.J. Modifications in ankle dorsiflexor activation by applying a torque perturbation during walking in persons post-stroke: A case series. J. Neuroeng. Rehabil. 2014, 11, 98. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, K.Z.; Lewek, M.D.; Sawicki, G.S. A neuromechanics-based powered ankle exoskeleton to assist walking post-stroke: A feasibility study. J. Neuroeng. Rehabil. 2015, 12, 23. [Google Scholar] [CrossRef] [Green Version]
- Koller, J.R.; Remy, C.D.; Ferris, D.P. Comparing neural control and mechanically intrinsic control of powered ankle exoskeletons. In Proceedings of the IEEE International Conference on Rehabilitation Robotics, London, UK, 17–20 July 2017; pp. 294–299. [Google Scholar]
- Ren, Y.; Wu, I.N.; Yang, C.Y.; Xu, T.; Harvey, R.L.; Zhang, L.Q. Developing a Wearable Ankle Rehabilitation Robotic Device for in-Bed Acute Stroke Rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 589–596. [Google Scholar] [CrossRef]
- Yeung, L.F.; Ockenfeld, C.; Pang, M.K.; Wai, H.W.; Soo, O.Y.; Li, S.W.; Tong, K.Y. Randomized controlled trial of robotassisted gait training with dorsiflexion assistance on chronic stroke patients wearing ankle-foot-orthosis. J. Neuroeng. Rehabil. 2018, 15, 51. [Google Scholar] [CrossRef] [Green Version]
- Awad, L.N.; Esquenazi, A.; Francisco, G.E.; Nolan, K.J.; Jayaraman, A. The ReWalk ReStore™ soft robotic exosuit: A multi-site clinical trial of the safety, reliability, and feasibility of exosuit-augmented post-stroke gait rehabilitation. J. Neuroeng. Rehabil. 2020, 17, 80. [Google Scholar] [CrossRef]
- Racu, C.M.; Doroftei, I. Design, modelling and simulation aspects of an ankle rehabilitation device. IOP Conf. Ser. Mater. Sci. Eng. 2016, 145, 052008. [Google Scholar] [CrossRef] [Green Version]
- Racu, C.M.; Doroftei, I. Design Aspects of a New Device for Ankle Rehabilitation. Appl. Mech. Mater. 2015, 809, 986–991. [Google Scholar] [CrossRef]
- Racu, C.M.; Doroftei, I. Ankle rehabilitation device with two degrees of freedom and compliant joint. IOP Conf. Ser. Mater. Sci. Eng. 2015, 95, 012054. [Google Scholar] [CrossRef] [Green Version]
- Racu, C.M.; Doroftei, I. New Concepts of Ankle Rehabilitation Devices—Part I: Theoretical Aspects. In New Advances in Mechanism and Machine Science; Doroftei, I., Pisla, D., Lovasz, E., Eds.; Springer: Cham, Switzerland, 2018; pp. 223–231. [Google Scholar]
- Racu, C.M.; Doroftei, I. New Concepts of Ankle Rehabilitation Devices—Part II: Design and Simulation. In New Advances in Mechanism and Machine Science; Doroftei, I., Pisla, D., Lovasz, E., Eds.; Springer: Cham, Switzerland, 2018; pp. 233–239. [Google Scholar]
- Racu, C.M.; Doroftei, I. Preliminary results and evaluation of an ankle rehabilitation device. IOP Conf. Ser. Mater. Sci. Eng. 2020, 997, 012088. [Google Scholar] [CrossRef]
- Parenteau, C.S.; Viano, D.C.; Petit, P.Y. Biomechanical properties of human cadaveric ankle-subtalar joints in quasi-static loading. J. Biomech. Eng. 1998, 120, 105–111. [Google Scholar] [CrossRef]
- Doroftei, I.; Racu, C.M.; Baudoin, Y. Development of a Robotic Platform for Ankle Joint Rehabilitation. Acta Tech. Napoc. Ser. Appl. Math. Mech. Eng. 2021, 64, 301–310. [Google Scholar]







































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Actuation Type | Number of DOF | Control Strategies | Study with Patients |
|---|---|---|---|---|
| Girone et al. [10] | Pneumatic | 6 | Position control; force control | Yes |
| Yoon et al. [11] | Pneumatic | 4 | Position control | No |
| Dai et al. [12] | Electric | 4 | N/A | No |
| Liu et al. [13] | Electric | 3 | Position control; force control | No |
| Saglia et al. [14] | Electric | 2 | Position control; assistive control; admittance control | No |
| Malosio et al. [15] | Electric | 3 | Position control; admittance control | No |
| Ayas et al. [16] | Electric | 2 | Trajectory tracking; admittance adaptive control | No |
| Ai et al. [17] | Pneumatic | 2 | Adaptive backstepping sliding mode control | No |
| Jamwal et al. [18] | Pneumatic | 3 | Position control; adaptive control; adaptive impedance control | Yes |
| Zhang et al. [19] | Pneumatic | 3 | Position control; adaptive patient-cooperative control; adaptive trajectory tracking | Yes |
| Tsoi et al. [20] | Electric | 3 | Joint force control; impedance control | No |
| Wang et al. [21] | Electric | 3 | Position control | No |
| Valles et al. [22] | Electric | 3 | Position control; force control | No |
| Li et al. [23] | Electric | 3 | Position control; patient-passive compliant exercise; isotonic exercise; patient-active exercise | No |
| Reference | Actuation Type | Number of DOF | Function |
|---|---|---|---|
| Cioi et al. [34] | Pneumatic | 6 | Ankle rehabilitation for children with epilepsy |
| Girone et al. [10] | Pneumatic | 6 | AJ rehabilitation |
| Roy et al. [35] | Electric | 3 | Ankle training with a robotic device to improve hemiparetic gait after a stroke |
| Kim et al. [36] | Electric | 2 | Active ankle–foot orthosis for foot drop |
| Ward et al. [37] | Electric | 2 | Powered ankle–foot orthosis |
| Forrester et al. [38] | Electric | 3 | “AnkleBot” training on paretic ankle motor control in chronic stroke |
| Jamwal et al. [39] | Pneumatic | 3 | Treatment for an ankle sprain through physical therapy |
| Blanchette et al. [40] | Electro-hydraulic | 2 | Robotized ankle–foot orthosis |
| Takahashi et al. [41] | Pneumatic | 2 | An exoskeleton supplies plantar flexion assistance |
| Koller et al. [42] | Pneumatic | 2 | Powered ankle exoskeletons using neural measurements |
| Ren et al. [43] | Electric | 2 | Wearable AJ RR for in-bed acute stroke rehabilitation |
| Yeung et al. [44] | Electric | 2 | Robot-assisted ankle–foot orthosis to provide assistance post stroke |
| Awad et al. [45] | Electric | 2 | ReWalk ReStore dorsi flexor and plantar flexor |
| The Center of the AJ Is Aligned with the Rotation Center of the Robot | The Center of the AJ and the Rotation Center of the Robot Are not Coincident | ||
|---|---|---|---|
| Parallel Rotational Axes of DgLs | Collinear Rotational Axes of DgLs | Parallel Rotational Axes of DgLs | Collinear Rotational Axes of DgLs |
DS-1 | DS-2 | DS-3 | DS-4 |
| The Center of the AJ Is Aligned with the Rotation Center of the Robot | The Center of the AJ and the Rotation Center of the Robot Are not Coincident | ||
|---|---|---|---|
| Parallel Rotational Axes of DgLs | Collinear Rotational Axes of DgLs | Parallel Rotational Axes of DgLs | Collinear Rotational Axes of DgLs |
DS-5 | DS-6 | DS-7 | DS-8 |
| DS-1 | DS-2 | DS-3 | DS-4 | DS-5 | DS-6 | DS-7 | DS-8 | |
|---|---|---|---|---|---|---|---|---|
| C1 | 5 | 5 | 5 | 5 | 4 | 4 | 4 | 4 |
| C2 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 |
| C3 | 5 | 5 | 5 | 5 | 4 | 4 | 4 | 4 |
| C4 | 4 | 3 | 5 | 4 | 3 | 2 | 4 | 3 |
| C5 | 4 | 4 | 5 | 4 | 3 | 3 | 3 | 3 |
| C6 | 4 | 3 | 5 | 3 | 4 | 4 | 5 | 5 |
| Total | 27 | 25 | 30 | 26 | 23 | 22 | 25 | 24 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doroftei, I.; Cazacu, C.-M.; Alaci, S. Design and Experimental Testing of an Ankle Rehabilitation Robot. Actuators 2023, 12, 238. https://doi.org/10.3390/act12060238
Doroftei I, Cazacu C-M, Alaci S. Design and Experimental Testing of an Ankle Rehabilitation Robot. Actuators. 2023; 12(6):238. https://doi.org/10.3390/act12060238
Chicago/Turabian StyleDoroftei, Ioan, Cristina-Magda Cazacu, and Stelian Alaci. 2023. "Design and Experimental Testing of an Ankle Rehabilitation Robot" Actuators 12, no. 6: 238. https://doi.org/10.3390/act12060238