
History and Current Status of Mediterranean Spotted Fever (MSF) in the Crimean Peninsula and Neighboring Regions along the Black Sea Coast

Abstract
:1. Introduction
2. Historic Summary of MSF in Crimea
3. History of MSF in Other Regions of the Black Sea Basin (1931–1990s)
4. Epidemiological Status of MSF in Crimea and Other Countries in the Black Sea Region (1990–2021)
5. Description of Main Clinical Features of MSF in Crimea
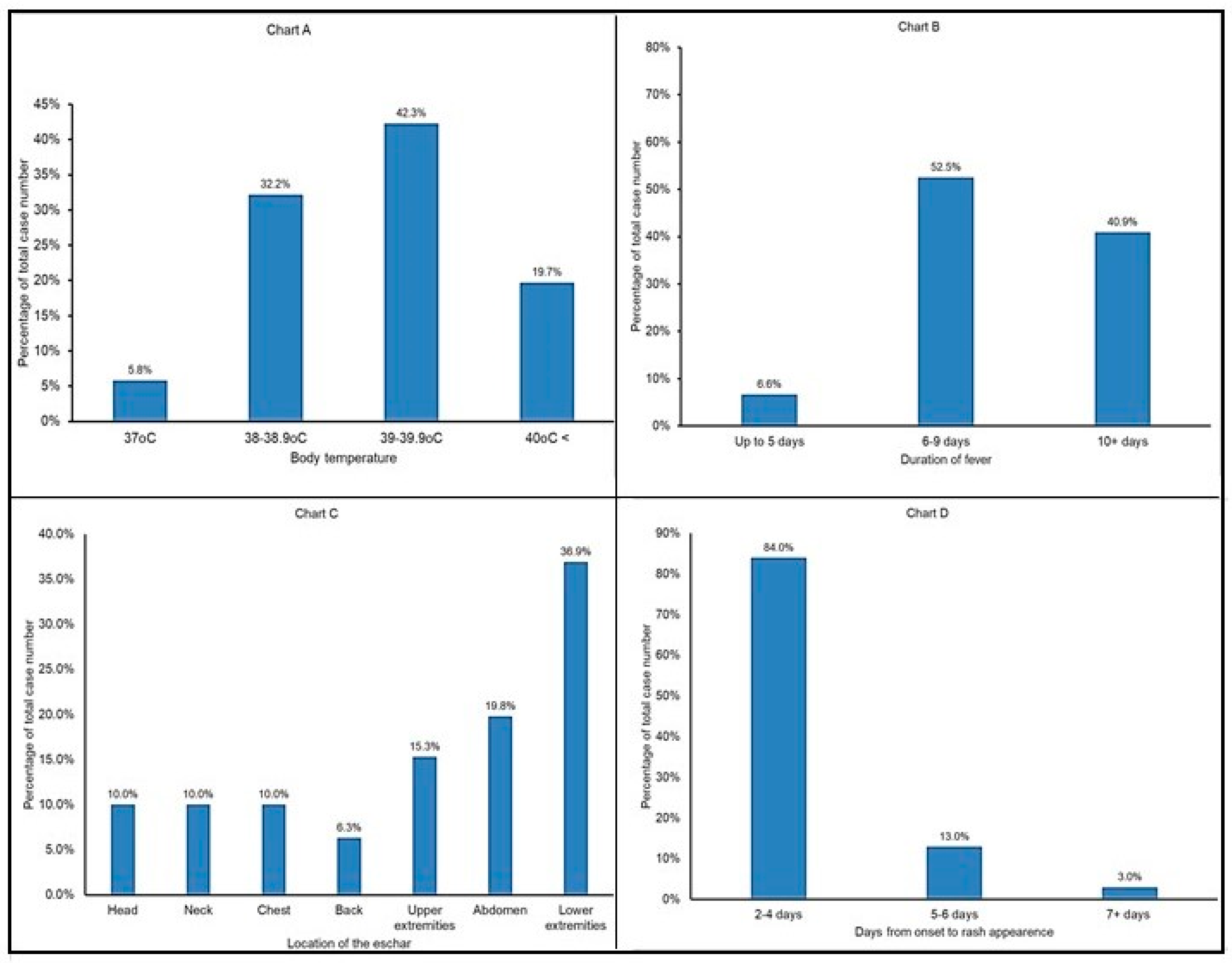
6. Analysis of Recent Clinical Cases of MSF in Crimea
7. Vector and Host Associations of Rickettsia conorii in Crimea and Other Countries in the Black Sea Region
8. Contemporary Tick Surveillance Efforts in Countries Adjacent to the Black Sea
9. Implications of Other Rickettsia and Rickettsioses Sympatric to R. conorii conorii and MSF in Black-Sea-Area Countries
10. Conclusions and Highlights
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Conor, A.; Bruch, A. Une fièvre éruptive observée en Tunisie. Bull. Soc. Pathol. Exot. Filial. 1910, 8, 492–496. (In French) [Google Scholar]
- Olmer, D. Sur une infection épidémique, avec exantheme de nature indéterminée. Mars. Med. 1925, 22, 1291–1293. (In French) [Google Scholar]
- Boinet, M.M.; Pieri, J. Epidémies d’exantheme infectieux de nature indéterminée, observées sur le littoral méditerranéen. Presse Medicale 1927, 89, 173–182. (In French) [Google Scholar]
- Blanc, G.; Caminopetros, J. Etudes épidémiologiques et expérimentales sur la fièvre boutonneuse, faites à l’Institut Pasteur d’Athènes. Arch. Inst. Pasteur Tunis 1932, 20, 343–394. (In French) [Google Scholar]
- Durand, P.; Conseil, E. Transmission expérimentale de la fièvre boutonneuse par Rhipicephalus sanguineus. Comptes Rendus Hebdomadaires des Séances de l’Académie des Sciences 1930, 190, 1244–1246. (In French) [Google Scholar]
- Zhu, Y.; Fournier, P.-E.; Eremeeva, M.; Raoult, D. Proposal to create subspecies of Rickettsia conorii based on multi-locus sequence typing and an emended description of Rickettsia conorii. BMC Microbiol. 2005, 5, 11. [Google Scholar] [CrossRef] [PubMed]
- Parola, P.; Paddock, C.D.; Socolovschi, C.; Labruna, M.B.; Mediannikov, O.; Kernif, T.; Abdad, M.Y.; Stenos, J.; Bitam, I.; Fournier, P.-E.; et al. Update on tick-borne rickettsioses around the world: A geographic approach. Clin. Microbiol. Rev. 2013, 26, 657–702. [Google Scholar] [CrossRef]
- Rovery, C.; Brouqui, P.; Raoult, D. Questions on Mediterranean spotted fever a century after its discovery. Emerg. Infect. Dis. 2008, 14, 1360–1367. [Google Scholar] [CrossRef]
- Xu, N.; Gai, W.; Zhang, Y.; Wang, W.; Wang, G.; Dasch, G.A.; Eremeeva, M.E. Confirmation of Rickettsia conorii subspecies indica infection by next-generation sequencing, Shandong, China. Emerg. Infect. Dis. 2021, 27, 2691–2694. [Google Scholar] [CrossRef]
- Gu, X.L.; Wang, R.; Zhou, C.-M.; Cui, J.-T.; Li, Z.-M.; Jiang, Z.-Z.; Li, B.; Peng, Q.-M.; Zhang, W.-K.; Han, H.-J.; et al. Natural Mediterranean Spotted fever foci, Qingdao, China. Emerg. Infect. Dis. 2022, 28, 2524–2527. [Google Scholar] [CrossRef]
- Gray, J.; Dantas-Torres, F.; Estrada-Peña, A.; Levin, M. Systematics and ecology of the brown dog tick, Rhipicephalus sanguineus. Ticks Tick Borne Dis. 2013, 4, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Dantas-Torres, F.; Otranto, D. Rhipicephalus sanguineus (Brown dog tick). Trends Parasitol. 2022, 38, 993–994. [Google Scholar] [CrossRef] [PubMed]
- Torina, A.; de Mera, I.G.F.; Alongi, A.; Mangold, A.J.; Blanda, V.; Scarlata, F.; Di Marco, V.; de la Fuente, J. Rickettsia conorii Indian tick typhus strain and R. slovaca in humans, Sicily. Emerg. Infect. Dis. 2012, 18, 1008–1010. [Google Scholar] [CrossRef]
- de Sousa, R.; Ismail, N.; Doria-Nobrega, S.; Costa, P.; Abreu, T.; Francca, A.; Amaro, M.; Proencca, P.; Brito, P.; Poccas, J.; et al. The presence of eschars, but not greater severity, in Portuguese patients infected with Israeli spotted fever. Ann. N. Y. Acad. Sci. 2005, 1063, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Chisu, V.; Masala, G.; Foxi, C.; Socolovschi, C.; Raoult, D.; Parola, P. Rickettsia conorii israelensis in Rhipicephalus sanguineus ticks, Sardinia, Italy. Ticks Tick Borne Dis. 2014, 5, 446–448. [Google Scholar] [CrossRef]
- Brouqui, P.; Parola, P.; Fournier, P.E.; Raoult, D. Spotted fever rickettsioses in southern and eastern Europe. FEMS Immunol. Med. Microbiol. 2007, 49, 2–12. [Google Scholar] [CrossRef]
- Renvoisé, A.; Delaunay, P.; Blanchouin, E.; Cannavo, I.; Cua, E.; Socolovschi, C.; Parola, P.; Raoult, D. Urban family cluster of spotted fever rickettsiosis linked to Rhipicephalus sanguineus infected with Rickettsia conorii subsp. caspia and Rickettsia massiliae. Ticks Tick Borne Dis. 2012, 3, 389–392. [Google Scholar] [CrossRef]
- Piras, M.A.; Calia, G.; Saba, F.; Gakis, C.; Andreoni, G. Glucose-6-phosphate dehydrogenase deficiency in male patients with Mediterranean spotted fever in Sardinia. J. Infect. Dis. 1983, 147, 607–608. [Google Scholar] [CrossRef]
- Raoult, D.; Lena, D.; Perrimont, H.; Gallais, H.; Walker, D.H.; Casanova, P. Hemolysis with Mediterranean spotted fever and glucose-6-phosphate-dehydrogenase deficiency. Trans. R. Soc. Trop. Med. Hyg. 1986, 80, 961–962. [Google Scholar] [CrossRef]
- Chaumentin, G.; Zenone, T.; Bibollet, C.; Denoyel, G.A.; Boibieux, A.; Biron, F.; Peyramond, D. Malignant boutonneuse fever and polymyalgia rheumatica: A coincidental association? Infection 1997, 25, 320–322. [Google Scholar] [CrossRef]
- Alymov, A.Y. Marseille fever. Soviet Med. 1939, 13, 30–33. (In Russian) [Google Scholar]
- Andreev, M.F. Clinical and epidemiological observations of the Marseille spotted fever. Clin. Med. 1941, 19, 80–88. (In Russian) [Google Scholar]
- Andreev, M.F. A case of Marseille fever observed in winter. Ter. Arkhiv 1940, 18, 208–215. (In Russian) [Google Scholar]
- Pakshin, M.F.; Nikitin, A.M. Data from a study of a natural focus of Marseilles fever in one of the Crimean districts over a 40-year period (1947–1986). Med. Parazitol. 1988, 4, 46–48. (In Russian) [Google Scholar]
- Pakshin, M.F.; Pestenko, V.I.; Kostetskii, N.V. On the epidemiology of Marseilles fever in the Crimea and means for its eradication. Zhurnal Mikrobiol. Epidemiol. Immunobiol. 1960, 31, 61–64. (In Russian) [Google Scholar]
- Kulagin, S.M.; Tarasevich, I.V.; Rubakin, P.E.; Nikitina, M.; Krupina, Z.N. On the eradication of Marseilles fever. Certain observations on Marseilles fever in Sevastopol. Zhurnal Mikrobiol. Epidemiol. Immunobiol. 1960, 31, 117–121. (In Russian) [Google Scholar]
- Zdrodovskii, P.; Golinevitch, E.M. Experimental observations of Marseille fever. In Rickettsiae and Rickettsioses; Zdrodovskii, P., Ed.; USSR Academy of Medical Science: Moscow, Russia, 1948; pp. 216–224. (In Russian) [Google Scholar]
- Avetisova, A.S. Observations of Marseille fever. Zhurnal Mikrobiol. Epidemiol. Immunobiol. 1952, 12, 26–31. (In Russian) [Google Scholar]
- Combiesco, D. Sur une épidémie de fièvre boutonneuse observée à Constantza-Roumanie. Arch. Roum. Pathol. Exp. Microbiol. 1948, 14, 99–112. (In French) [Google Scholar]
- Combiescu, D.; Dumitrescu, N.; Russ, M.; Dinculescu, M. Consideraţii epidemiologice asurpa unor cazuri de febră butonoasă ivite in ultimii 41 de ani. Cultivarea Rickettsiei conori şi caracterele tulpinii izolate dintr’un focar autohton de febră butonoasă. Stud. Cercet. Inframicrobiol. Microbiol. Parazitol. 1953, IV, 99–107. (In Romanian) [Google Scholar]
- Pitigoi, D.; Olaru, I.D.; Badescu, D.; Rafila, A.; Arama, V.; Hristea, A. Mediterranean spotted fever in southeastern Romania. Biomed. Res. Int. 2013, 2013, 395806. [Google Scholar] [CrossRef]
- Alexandrov, E.; Alexandrova, D.; Kamarinchev, B.; Kantardjiev, T.; Dimitrova, Z. Marseilles fever (Mediterranean spotted fever) in Bulgaria-state and problems. In Contemporary State of the Rickettsioses in the World and in Bulgaria; Alexandrov, E., Kazar, J., Hechemy, K., Kantardjiev, T., Eds.; Prof. Marin Drinov Academic Publishing House: Sofia, Bulgaria, 2007; pp. 80–93. [Google Scholar]
- Alexandrov, E.G.; Mitov, D.G.; Kamarinchev, B.D.; Bogdanov, N.R. Current features of Mediterranean spotted fever in Bulgaria. In Rickettsiae and Rickettsial Diseases at the Turn of the Third Millenium; Raoult, D., Brouqui, P., Eds.; Elsevier: Paris, France, 1999; pp. 279–281. [Google Scholar]
- Rehacek, J.; Tarasevich, I.V. Rickettsia conorii. In Acari-Borne Rickettsiae and Rickettsioses in Eurasia; Rehacek, J., Tarasevich, I.V., Eds.; Veda Publishing House of the Slovak Academy of Sciences: Bratislava, Slovakia, 1988; pp. 14–48. [Google Scholar]
- Kuloglu, F.; Rolain, J.M.; Akata, F.; Eroglu, C.; Celik, A.D.; Parola, P. Mediterranean spotted fever in the Trakya region of Turkey. Ticks Tick Borne Dis. 2012, 3, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Mert, A.; Ozaras, R.; Tabak, F.; Bilir, M.; Ozturk, R. Mediterranean spotted fever: A review of fifteen cases. J. Dermatol. 2006, 33, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Celebi, B.; Yesilyurt, M.; Kilic, S. A Rickettsia case caused by Rickettsia conorii. Mikrobiyol. Bul. 2018, 52, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Uzunlulu, M.; Gönenç, I.; Kaya, S.; Selvi, E.; Arslan, F. A case of Mediterranean spotted fever mimicking severe sepsis. J. Vector Borne Dis. 2022, 59, 298–301. [Google Scholar] [CrossRef] [PubMed]
- Kuloglu, F.; Rolain, J.M.; Fournier, P.E.; Akata, F.; Tugrul, M.; Raoult, D. First isolation of Rickettsia conorii from humans in the Trakya (European) region of Turkey. Eur. J. Clin. Microbiol. Infect. Dis. 2004, 23, 609–614. [Google Scholar] [CrossRef]
- McCormick, D.W.; Kugeler, K.J.; Marx, G.E.; Jayanthi, P.; Dietz, S.; Mead, P.; Hinckley, A.F. Effects of COVID-19 pandemic on reported Lyme Disease, United States, 2020. Emerg. Infect. Dis. 2021, 27, 2715–2717. [Google Scholar] [CrossRef]
- Sulik, M.; Toczylowski, K.; Grygorczuk, S. Epidemiology of tick-borne encephalitis in Poland (2010–2019) and the impact of the COVID-19 pandemic on the notified incidence of the disease. Przegl. Epidemiol. 2021, 75, 76–85. [Google Scholar] [CrossRef]
- Piotrowski, M.; Rymaszewska, A. The impact of a pandemic COVID-19 on the incidence of borreliosis in Poland. Acta Parasitol. 2022, 67, 1007–1009. [Google Scholar] [CrossRef]
- Pen’kovskaya, N.A. Epidemiological features of Mediterranean spotted fever in the Crimea at the modern stage. Krims’kiy Ter. Zhurnal 2014, 1, 140–145. (In Russian) [Google Scholar]
- Eremeeva, M.E.; Shpynov, S.N.; Tokarevich, N.K. Modern approaches to laboratory diagnosis of rickettsial diseases. Russ. J. Infect. Immun. 2014, 4, 113–134. [Google Scholar] [CrossRef]
- Zvereva, N.N.; Saifullin, M.A.; Karan, L.S.; Bazarova, M.V.; Saifullin, R.F.; Smetanina, S.V. The case of tick-borne spotted fever in a child arriving from the Crimea. Det. Infektsii 2018, 17, 69–72. [Google Scholar] [CrossRef]
- Vladimirova, N.; Minkova, A.; Bogdanov, N.R.; Ivanova, S.; Petkova, K.; Getsova, Z. Acute Infectious Diseases in Bulgaria in 2022 (Basic Epidemiological Indicators); Department of Epidemiology, National Center for Infectious and Parasitic Diseases: Sofia, Bulgaria, 2022; pp. 1–54. Available online: https://www.ncipd.org/index.php?option=com_content&view=featured&Itemid=1086&lang=bg (accessed on 26 June 2023). (In Bulgarian)
- Baltadzhiev, I.; Kevorkyan, A.; Popivanova, N. Mediterranean spotted fever in child and adult patients: Investigation from an endemic region in Bulgaria. Cent. Eur. J. Public Health 2020, 28, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Pishmisheva, M.; Stoycheva, M.; Vatev, N.; Semerdjieva, M. Mediterranean spotted fever in children in the Pazardjik region, South Bulgaria. Pediatr. Infect. Dis. J. 2014, 33, 542–544. [Google Scholar] [CrossRef] [PubMed]
- Nenova, M. Mediterranean spotted fever in Varna region. In Contemporary State of the Rickettsioses in the World and in Bulgaria; Alexandrov, E., Kazar, J., Hechemy, K., Kantardjiev, T., Eds.; Prof. Marin Drinov Academic Publishing House: Sofia, Bulgaria, 2007; pp. 94–106. [Google Scholar]
- Popivanova, N.; Baltadzhiev, I.; Zaprianov, Z. Mediterranean spotted fever in the Plovdiv region of Bulgaria. In Contemporary State of the Rickettsioses in the World and in Bulgaria; Alexandrov, A., Kazar, J., Hechemy, K., Kantardjiev, T., Eds.; Prof. Marin Drinov Academic Publishing House: Sofia, Bulgaria, 2007; pp. 116–129. [Google Scholar]
- Pishmisheva, P. Mediterranean spotted fever in Pazardzhic region-clinic, paraclinic, treatment, specific forms of rickettsiosis, epidemiology. In Contemporary State of the Rickettsioses in the World and in Bulgaria; Alexandrov, A., Kazar, J., Hechemy, K., Kantardjiev, T., Eds.; Prof. Marin Drinov Academic Publishing House: Sofia, Bulgaria, 2007; pp. 107–115. [Google Scholar]
- Biggs, H.M.; Behravesh, C.B.; Bradley, K.K.; Dahlgren, F.S.; Drexler, N.A.; Dumler, J.S.; Folk, S.M.; Kato, C.Y.; Lash, R.R.; Levin, M.L.; et al. Diagnosis and management of tickborne rickettsial diseases: Rocky Mountain spotted fever and other spotted fever group rickettsioses, ehrlichioses, and anaplasmosis-United States. MMWR Recomm. Rep. 2016, 65, 1–44. [Google Scholar] [CrossRef]
- O’Reilly, M.; Paddock, C.; Elchos, B.; Goddard, J.; Childs, J.; Currie, M. Physician knowledge of the diagnosis and management of Rocky Mountain spotted fever: Mississippi, 2002. Ann. N. Y. Acad. Sci. 2003, 990, 295–301. [Google Scholar] [CrossRef]
- National Center for Infectious and Parasitic Diseases. Epidemiological Bulletin; National Center for Infectious and Parasitic Diseases: Sofia, Bulgaria, 2022; Available online: https://www.ncipd.org/index.php?option=com_content&view=featured&Itemid=730&lang=en (accessed on 26 June 2023).
- Macrotrends. Bulgaria Population 1950–2023. Macrotrends. Available online: https://www.macrotrends.net/countries/BGR/bulgaria/population (accessed on 25 June 2023).
- National Centre for Surveillance and Control of Communicable Diseases [Institutul Naţional de Sanatate Publica]. Report of Communicable Diseases; National Centre for Surveillance and Control of Communicable Diseases [Institutul Naţional de Sanatate Publica]: Bucharest, Romania, 2016; pp. 70–73. Available online: http://www.cnscbt.ro/ (accessed on 26 June 2023).
- Serban, R.; Pistol, A.; Neguţ, M.; Cucuiu, R. Rickettsia conorii infection in Romania, 2000–2008. Bacteriol. Virusol. Parazitol. Epidemiol. 2009, 54, 177–183. [Google Scholar]
- Andersson, M.O.; Marga, G.; Banu, T.; Dobler, G.; Chitimia-Dobler, L. Tick-borne pathogens in tick species infesting humans in Sibiu County, central Romania. Parasitol. Res. 2018, 117, 1591–1597. [Google Scholar] [CrossRef]
- Ionita, M.; Silaghi, C.; Mitrea, I.L.; Edouard, S.; Parola, P.; Pfister, K. Molecular detection of Rickettsia conorii and other zoonotic spotted fever group rickettsiae in ticks, Romania. Ticks Tick Borne Dis. 2016, 7, 150–153. [Google Scholar] [CrossRef]
- Mihalca, A.D.; Dumitrache, M.O.; Sándor, A.D.; Magdaş, C.; Oltean, M.; Györke, A.; Matei, I.A.; Ionică, A.; D’amico, G.; Cozma, V.; et al. Tick parasites of rodents in Romania: Host preferences, community structure and geographical distribution. Parasites Vectors 2012, 5, 266. [Google Scholar] [CrossRef]
- Sengoz, G.; Yildirim, F.; Yasar, K.K.; Tozalgan, U.; Aydin, O.A. Fifty-six cases with Mediterranean spotted fever: Evaluation of tick-borne spotted diseases in Turkey. Turkderm-Turk. Arch. Dermatol. Venerol. 2009, 43, 139–143. [Google Scholar]
- Ozkan, A.; Ozkalemkas, F.; Ali, R.; Karadogan, S.; Ozkocaman, V.; Ozcelik, T.; Tunali, A. Mediterranean spotted fever: Presentation with pancytopenia. Am. J. Hematol. 2006, 81, 646–647. [Google Scholar] [CrossRef] [PubMed]
- Gafarova, M.T. Marseilles Fever (Epidemiology, Clinic and Diagnosis); Tarpan: Simferopol, Ukraine, 2004; p. 98. [Google Scholar]
- Gafarova, M.T.; Verbenets, E.A.; Achkasova, T.A.; Schomoylov, D.K.; Midikari, A.C. Epidemiology and clinical features of Marseille fever in Crimea. Infect. Dis. News Opin. Educ. 2017, 2, 61–66. (In Russian) [Google Scholar]
- Verbenets, E.A. Comparative characteristics of clinico-epdemiological features of Marseille during time-course of disease. Tauride Med. Biol. Bull. 2009, 12, 23–26. (In Russian) [Google Scholar]
- Klymchuk, M.D.; Dorofeev, Y.O.; Lezhentsev, B.M.; Tovpinec, N.N. An outbreak of tick-borne rickettsosis (Marseille fever) in the Crimea. Infect. Bolezn. 1999, 3, 10–12. (In Ukranian) [Google Scholar]
- Popova, A.Y.; Kulichenko, A.N.; Maletskaya, O.V.; Vasilenko, N.F.; Shaposhnikova, L.I.; Kotenev, E.S.; Dubyansky, V.M.; Volynkina, A.S.; Lisitskaya, Y.V.; Samarina, I.V.; et al. Epidemiologic situation by natural-foci infections in the Crimea Federal District in 2014–2015. Zhurnal Mikrobiol. Epidemiol. Immunobiol. 2016, 93, 62–69. [Google Scholar] [CrossRef]
- Verbenets, E.A. Modern Epidemiological and Clinical Features of Marseilles Fever at the Present Stage, Optimization of Epidemiological Surveillance. Abstract of the Dissertation for the Degree of Candidate of Medical Sciences: 14.02.02 Verbenets Elena Anatolyevna; L. V. Gromashevsky Institute of Epidemiology and Infectious Diseases: Kiev, Ukraine, 2013. (In Ukranian) [Google Scholar]
- Mansueto, P.; Vitale, G.; Cascio, A.; Seidita, A.; Pepe, I.; Carroccio, A.; di Rosa, S.; Rini, G.B.; Cillari, E.; Walker, D.H. New insight into immunity and immunopathology of rickettsial diseases. Clin. Dev. Immunol. 2012, 2012, 967852. [Google Scholar] [CrossRef]
- Colomba, C.; Siracusa, L.; Trizzino, M.; Gioè, C.; Giammanco, A.; Cascio, A. Myocarditis in Mediterranean spotted fever: A case report and a review of the literature. JMM Case Rep. 2016, 3, e005039. [Google Scholar] [CrossRef] [PubMed]
- Doyle, A.; Bhalla, K.S.; Jones, J.M.; Ennis, D.M. Myocardial involvement in rocky mountain spotted fever: A case report and review. Am. J. Med. Sci. 2006, 332, 208–210. [Google Scholar] [CrossRef]
- Akimov, I.A.; Nebogatkin, I.V. Ticks of the genus Rhipicephalus (Acari, Ixodidae) and their distribution in Ukraine. Vestn. Zool. 2013, 47, e28–e34. [Google Scholar] [CrossRef]
- Klyushkina, E.A. About the tick Rhipicephalus sanguineus Latreille—A carrier of Marseille fever. J. Microbiol. 1966, 11, 146. (In Russian) [Google Scholar]
- Klyushkina, E.A. Distribution and biology of tick Rh. sanguineus Latr. in Crimea. Med. Parazitol. Parazitic Dis. 1968, 46–50. (In Russian) [Google Scholar]
- Evstafiev, I.L.; Pyshkin, V.B.; Evstafief, A.I.; Tovpinets, N.N. Electronic databases and geoinformation technologies in environmental and biomedical research. Cult. Peoples Black Sea Region. 2005, 7–10. (In Russian) [Google Scholar]
- Evstafiev, I.L.; Tovpinets, N.N. Rhipicephalus sanguineus (Ixodidae) in the Crimea: Environmental and epizootological aspects. Vestn. Zool. 2002, 36, 85–91. (In Russian) [Google Scholar]
- Nebogatkin, I.V.; Tovpinets, N.N. The outbreak of bloody tick Rhipicephalus sanguineus (Ixodide) on the Kerch Peninsula. Vestn. Zool. 1997, 81. (In Russian) [Google Scholar]
- Demma, L.J.; Traeger, M.S.; Nicholson, W.L.; Paddock, C.D.; Blau, D.M.; Eremeeva, M.E.; Dasch, G.A.; Levin, M.L.; Singleton, J.; Zaki, S.R.; et al. Rocky Mountain spotted fever from an unexpected tick vector in Arizona. N. Engl. J. Med. 2005, 353, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Hansford, K.M.; Pietzsch, M.E.; Cull, B.; Medlock, J.M.; Wall, R. Overwintering of the brown dog tick in residential properties in England–raising awareness. Vet. Rec. 2015, 177, 156. [Google Scholar] [CrossRef] [PubMed]
- Uspensky, I.; Ioffe-Uspensky, I. The dog factor in brown dog tick Rhipicephalus sanguineus (Acari: Ixodidae) infestations in and near human dwellings. Int. J. Med. Microbiol. 2002, 291 (Suppl. S33), 156–163. [Google Scholar] [CrossRef]
- Levin, M.L.; Killmaster, L.F.; Zemtsova, G.E. Domestic dogs (Canis familiaris) as reservoir hosts for Rickettsia conorii. Vector-Borne Zoonotic Dis. 2012, 12, 28–33. [Google Scholar] [CrossRef]
- Solano-Gallego, L.; Kidd, L.; Trotta, M.; Di Marco, M.; Caldin, M.; Furlanello, T.; Breitschwerdt, E. Febrile illness associated with Rickettsia conorii infection in dogs from Sicily. Emerg. Infect. Dis. 2006, 12, 1985–1988. [Google Scholar] [CrossRef]
- Parola, P.; Socolovschi, C.; Raoult, D. Deciphering the relationships between Rickettsia conorii conorii and Rhipicephalus sanguineus in the ecology and epidemiology of Mediterranean spotted fever. Ann. N. Y. Acad. Sci. 2009, 1166, 49–54. [Google Scholar] [CrossRef]
- Levin, M.L.; Killmaster, L.; Eremeeva, M.; Dasch, G. Effects of Rickettsia conorii infection on the survival of Rhipicephalus sanguineus ticks. Clin. Microbiol. Infect. 2009, 15 (Suppl. S2), 277–278. [Google Scholar] [CrossRef] [PubMed]
- Socolovschi, C.; Bitam, I.; Raoult, D.; Parola, P. Transmission of Rickettsia conorii conorii in naturally infected Rhipicephalus sanguineus. Clin. Microbiol. Infect. 2009, 15 (Suppl. S2), 319–321. [Google Scholar] [CrossRef] [PubMed]
- Levin, M.L.; Killmaster, L.; Zemtsova, G.; Grant, D.; Mumcuoglu, K.Y.; Eremeeva, M.E.; Dasch, G.A. Incongruent effects of two isolates of Rickettsia conorii on the survival of Rhipicephalus sanguineus ticks. Exp. Appl. Acarol. 2009, 49, 347–359. [Google Scholar] [CrossRef] [PubMed]
- Socolovschi, C.; Matsumoto, K.; Brouqui, P.; Raoult, D.; Parola, P. Experimental infection of Rhipicephalus sanguineus with Rickettsia conorii conorii. Clin. Microbiol. Infect. 2009, 15 (Suppl. S2), 324–325. [Google Scholar] [CrossRef] [PubMed]
- Eremeeva, M.E.; Dasch, G.A. Challenges posed by tick-borne rickettsiae: Eco-epidemiology and public health implications. Front. Public Health 2015, 3, 55. [Google Scholar] [CrossRef]
- Dantas-Torres, F.; Latrofa, M.S.; Annoscia, G.; Giannelli, A.; Parisi, A.; Otranto, D. Morphological and genetic diversity of Rhipicephalus sanguineus sensu lato from the New and Old Worlds. Parasites Vectors 2013, 6, 213. [Google Scholar] [CrossRef]
- Kent, R.J. Molecular methods for arthropod bloodmeal identification and applications to ecological and vector-borne disease studies. Mol. Ecol. Resour. 2009, 9, 4–18. [Google Scholar] [CrossRef]
- Beati, L.; Kelly, P.J.; Matthewman, L.A.; Mason, P.R.; Raoult, D. Prevalence of rickettsia-like organisms and spotted fever group rickettsiae in ticks (Acari: Ixodidae) from Zimbabwe. J. Med. Entomol. 1995, 32, 787–792. [Google Scholar] [CrossRef]
- Alieva, E.E.; Bondarenko, E.I.; Maliy, K.D.; Shvalov, A.N.; Verbenets, E.A.; Gafarova, M.T. The role of Rhipicephalus sanguineus mites parasitizing on dogs in the spread of tick-borne rickettsiosis pathogens in Sevastopol. New Microbes New Infect. 2020, 36, 100704. [Google Scholar] [CrossRef]
- Gafarova, M.T.; Bondarenko, E.I.; Maliy, K.D.; Alieva, E.E.; Evstafiev, I.L.; Tovpinec, N.N.; Malaya, N.K.; Kubyshkin, A.V. Prevalence of causative agents of transmissive tick-borned ricketsious in the Crimean Peninsula. Klin. Lab. Diagn. Russ. Clin. Lab. Diagn. 2022, 67, 170–176. [Google Scholar] [CrossRef]
- Kartashov, M.Y.; Tikhonov, S.N.; Mikryukova, T.P.; Kovalenko, I.S.; Ternovoi, V.A.; Barinova, O.Y.; Netesov, S.V. Genotyping of rickettsial isolates circulating in the Crimean Peninsula. Mol. Genet. Microbiol. Virol. 2018, 33, 110–117. [Google Scholar] [CrossRef]
- Rogovskyy, A.S.; Nebogatkin, I.V.; Scoles, G.A. Ixodid ticks in the megapolis of Kyiv, Ukraine. Ticks Tick Borne Dis. 2017, 8, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Rogovskyy, A.; Batool, M.; Gillis, D.C.; Holman, P.J.; Nebogatkin, I.V.; Rogovska, Y.V.; Rogovskyy, M.S. Diversity of Borrelia spirochetes and other zoonotic agents in ticks from Kyiv, Ukraine. Ticks Tick Borne Dis. 2018, 9, 404–409. [Google Scholar] [CrossRef]
- Livanova, N.N.; Fomenko, N.V.; Akimov, I.A.; Ivanov, M.J.; Tikunova, N.V.; Armstrong, R.; Konyaev, S.V. Dog survey in Russian veterinary hospitals: Tick identification and molecular detection of tick-borne pathogens. Parasites Vectors 2018, 11, 591. [Google Scholar] [CrossRef] [PubMed]
- Golinevitch, H. A propos de la différenciation de quelques rickettsies du groupe de la fièvre poupree à tiques. Arch. Inst. Pasteur Tunis 1960, 37, 13–22. (In French) [Google Scholar]
- Eremeeva, M.E.; Balayeva, N.M.; Ignatovich, V.F.; Raoult, D. Proteinic and genomic identification of spotted fever group rickettsiae isolated in the former USSR. J. Clin. Microbiol. 1993, 31, 2625–2633. [Google Scholar] [CrossRef]
- Fournier, P.E.; Zhu, Y.; Ogata, H.; Raoult, D. Use of highly variable intergenic spacer sequences for multispacer typing of Rickettsia conorii strains. J. Clin. Microbiol. 2004, 42, 5757–5766. [Google Scholar] [CrossRef]
- Sukhiashvili, R.; Zhgenti, E.; Khmaladze, E.; Burjanadze, I.; Imnadze, P.; Jiang, J.; John, H.S.; Farris, C.M.; Gallagher, T.; Obiso, R.J.; et al. Identification and distribution of nine tick-borne spotted fever group Rickettsiae in the Country of Georgia. Ticks Tick Borne Dis. 2020, 11, 101470. [Google Scholar] [CrossRef]
- Christova, I.; Van de Pol, J.; Yazar, S.; Velo, E.; Schouls, L. Identification of Borrelia burgdorferi sensu lato, Anaplasma and Ehrlichia species, and spotted fever group rickettsiae in ticks from Southeastern Europe. Eur. J. Clin. Microbiol. Infect. Dis. 2003, 22, 535–542. [Google Scholar] [CrossRef]
- Karasartova, D.; Gureser, A.S.; Gokce, T.; Celebi, B.; Yapar, D.; Keskin, A.; Celik, S.; Ece, Y.; Erenler, A.K.; Usluca, S.; et al. Bacterial and protozoal pathogens found in ticks collected from humans in Corum province of Turkey. PLoS Negl. Trop. Dis. 2018, 12, e0006395. [Google Scholar] [CrossRef]
- Keskin, A.; Bursali, A.; Keskin, A.; Tekin, S. Molecular detection of spotted fever group rickettsiae in ticks removed from humans in Turkey. Ticks Tick Borne Dis. 2016, 7, 951–953. [Google Scholar] [CrossRef]
- Orkun, O. Comprehensive screening of tick-borne microorganisms indicates that a great variety of pathogens are circulating between hard ticks (Ixodoidea: Ixodidae) and domestic ruminants in natural foci of Anatolia. Ticks Tick Borne Dis. 2022, 13, 102027. [Google Scholar] [CrossRef] [PubMed]
- Orkun, O.; Cakmak, A. Molecular identification of tick-borne bacteria in wild animals and their ticks in Central Anatolia, Turkey. Comp. Immunol. Microbiol. Infect. Dis. 2019, 63, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Orkun, O.; Karaer, Z.; Çakmak, A.; Nalbantoğlu, S. Spotted fever group rickettsiae in ticks in Turkey. Ticks Tick Borne Dis. 2014, 5, 213–218. [Google Scholar] [CrossRef]
- Orkun, O.; Karaer, Z.; Çakmak, A.; Nalbantoğlu, S. Identification of tick-borne pathogens in ticks feeding on humans in Turkey. PLoS Negl. Trop. Dis. 2014, 8, e3067. [Google Scholar] [CrossRef] [PubMed]
- Oztoprak, N.; Celebi, G.; Aydemir, H.; Pişkin, N.; Bektaş, S.; Koca, R.; Kuloğlu, F. Mediterranean spotted fever due to contact with dog-tick. Mikrobiyoloji Bul. 2008, 42, 701–706. [Google Scholar]
- Polat, E.; Altinkum, S.M.; Bagdatli, Y.; Baykara, O. The tick fauna in Istanbul, Turkey, from 2013 to 2017 and identification of their pathogens by multiplex PCR: An epidemiological study. Exp. Appl. Acarol. 2021, 84, 825–834. [Google Scholar] [CrossRef]
- Gargili, A.; Palomar, A.M.; Midilli, K.; Portillo, A.; Kar, S.; Oteo, J.A. Rickettsia species in ticks removed from humans in Istanbul, Turkey. Vector Borne Zoonotic Dis. 2012, 12, 938–941. [Google Scholar] [CrossRef]
- Orkun, O.; Çakmak, A.; Nalbantoğlu, S.; Karaer, Z. Molecular detection of a novel Babesia sp. and pathogenic spotted fever group rickettsiae in ticks collected from hedgehogs in Turkey: Haemaphysalis erinacei, a novel candidate vector for the genus Babesia. Infect. Genet. Evol. 2019, 69, 190–198. [Google Scholar] [CrossRef]
- Christova, I.; Dimitrov, H.; Trifonova, I.; Gladnishka, T.; Mitkovska, V.; Stojanova, A.; Taseva, E.; Ivanova, V. Detection of human tick-borne pathogens in rodents from Bulgaria. Acta Zool. Bulg. 2012, 64 (Suppl. S4), 111–114. [Google Scholar]
- Christova, I.; Schouls, L.; van de Pol, I.; Park, J.; Panayotov, S.; Lefterova, V.; Kantardjiev, T.; Dumler, J.S. High prevalence of granulocytic Ehrlichiae and Borrelia burgdorferi sensu lato in Ixodes ricinus ticks from Bulgaria. J. Clin. Microbiol. 2001, 39, 4172–4174. [Google Scholar] [CrossRef] [PubMed]
- Gladnishka, T.K.; Tasseva, E.I.; Christova, I.S.; Nikolov, M.A.; Lazarov, S.P. Detection of Borrelia burgdorferi sensu lato, Anaplasma phagocytophilum and spotted fever group rickettsiae in ticks from the region of Sofia, Bulgaria (Acari: Parasitiformes: Ixodidae). Eur. Arachnol. Acta Zool. Bulg. 2005, 58 (Suppl. S1), 339–343. [Google Scholar]
- Nader, J.; Król, N.; Pfeffer, M.; Ohlendorf, V.; Marklewitz, M.; Drosten, C.; Junglen, S.; Obiegala, A. The diversity of tick-borne bacteria and parasites in ticks collected from the Strandja Nature Park in south-eastern Bulgaria. Parasites Vectors 2018, 11, 165. [Google Scholar] [CrossRef] [PubMed]
- Burgdorfer, W. Hemolymph test. A technique for detection of rickettsiae in ticks. Am. J. Trop. Med. Hyg. 1970, 19, 1010–1014. [Google Scholar] [CrossRef]
- Borsan, S.D.; Ionică, A.M.; Galon, C.; Toma-Naic, A.; Peştean, C.; Sándor, A.D.; Moutailler, S.; Mihalca, A.D. High diversity, prevalence, and co-infection rates of tick-borne pathogens in ticks and wildlife hosts in an urban area in Romania. Front. Microbiol. 2021, 12, 645002. [Google Scholar] [CrossRef]
- Mihalca, A.D.; Dumitrache, M.O.; Magdaş, C.; Gherman, C.M.; Domşa, C.; Mircean, V.; Ghira, I.V.; Pocora, V.; Ionescu, D.T.; Barabási, S.S.; et al. Synopsis of the hard ticks (Acari: Ixodidae) of Romania with update on host associations and geographical distribution. Exp. Appl. Acarol. 2012, 58, 183–206. [Google Scholar] [CrossRef]
- Dumitrache, M.O.; Kiss, B.; Dantas-Torres, F.; Latrofa, M.S.; D’Amico, G.; Sándor, A.D.; Mihalca, A.D. Seasonal dynamics of Rhipicephalus rossicus attacking domestic dogs from the steppic region of southeastern Romania. Parasites Vectors 2014, 7, 97. [Google Scholar] [CrossRef]
- Sándor, A.D.; Dumitrache, M.O.; D’Amico, G.; Kiss, B.J.; Mihalca, A.D. Rhipicephalus rossicus and not R. sanguineus is the dominant tick species of dogs in the wetlands of the Danube Delta, Romania. Vet. Parasitol. 2014, 204, 430–432. [Google Scholar] [CrossRef]
- Mărcuţan, I.D.; Kalmár, Z.; Ionică, A.M.; D’Amico, G.; Mihalca, A.D.; Vasile, C.; Sándor, A.D. Spotted fever group rickettsiae in ticks of migratory birds in Romania. Parasites Vectors 2016, 9, 294. [Google Scholar] [CrossRef]
- Kuscu, F.; Orkun, O.; Ulu, A.; Kurtaran, B.; Komur, S.; Inal, A.S.; Erdogan, D.; Tasova, Y.; Aksu, H.S.Z. Rickettsia sibirica mongolitimonae infection, Turkey, 2016. Emerg. Infect. Dis. 2017, 23, 1214–1216. [Google Scholar] [CrossRef]
- Emiroglu, M.; Celebi, B.; Alkan, G.; Yilmaz, Y. The first human case of Rickettsia slovaca from Turkey. Ticks Tick Borne Dis. 2021, 12, 101755. [Google Scholar] [CrossRef]
- Komitova, R.; Lakos, A.; Aleksandrov, A.; Christova, I.; Murdjeva, M. A case of tick-transmitted lymphadenopathy in Bulgaria associated with Rickettsia slovaca. Scand. J. Infect. Dis. 2003, 35, 213. [Google Scholar] [CrossRef] [PubMed]
- Zaharia, M.; Popescu, C.P.; Florescu, S.A.; Ceausu, E.; Raoult, D.; Parola, P.; Socolovschi, C. Rickettsia massiliae infection and SENLAT syndrome in Romania. Ticks Tick Borne Dis. 2016, 7, 759–762. [Google Scholar] [CrossRef]
- Weinberger, M.; Keysary, A.; Sandbank, J.; Zaidenstein, R.; Itzhaki, A.; Strenger, C.; Leitner, M.; Paddock, C.D.; Eremeeva, M.E. Fatal Rickettsia conorii subsp. israelensis infection, Israel. Emerg. Infect. Dis. 2008, 14, 821–824. [Google Scholar] [CrossRef] [PubMed]
- Demeester, R.; Claus, M.; Hildebrand, M.; Vlieghe, E.; Bottieau, E. Diversity of life-threatening complications due to Mediterranean spotted fever in returning travelers. J. Travel Med. 2010, 17, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Parola, P.; Rovery, C.; Rolain, J.M.; Brouqui, P.; Davoust, B.; Raoult, D. Rickettsia slovaca and R. raoultii in tick-borne rickettsioses. Emerg. Infect. Dis. 2009, 15, 1105–1108. [Google Scholar] [CrossRef]
- Igolkina, Y.; Rar, V.; Krasnova, E.; Filimonova, E.; Tikunov, A.; Epikhina, T.; Tikunova, N. Occurrence and clinical manifestations of tick-borne rickettsioses in Western Siberia: First Russian cases of Rickettsia aeschlimannii and Rickettsia slovaca infections. Ticks Tick Borne Dis. 2022, 13, 101927. [Google Scholar] [CrossRef]
- Santibáñez, S.; Portillo, A.; Ibarra, V.; Santibáñez, P.; Metola, L.; García-García, C.; Palomar, A.M.; Cervera-Acedo, C.; Alba, J.; Blanco, J.R.; et al. Epidemiological, clinical, and microbiological characteristics in a large series of patients affected by Dermacentor-Borne-Necrosis-Erythema-Lymphadenopathy from a unique centre from Spain. Pathogens 2022, 11, 528. [Google Scholar] [CrossRef]
- Dong, Z.; Yang, Y.; Wang, Q.; Xie, S.; Zhao, S.; Tan, W.; Yuan, W.; Wang, Y. A case with neurological abnormalities caused by Rickettsia raoultii in northwestern China. BMC Infect. Dis. 2019, 19, 796. [Google Scholar] [CrossRef]
- Li, H.; Zhang, P.-H.; Huang, Y.; Du, J.; Cui, N.; Yang, Z.-D.; Tang, F.; Fu, F.-X.; Cui, X.-M.; Fan, Y.-D.; et al. Isolation and identification of Rickettsia raoultii in human cases: A surveillance study in 3 medical centers in China. Clin. Infect. Dis. 2018, 66, 1109–1115. [Google Scholar] [CrossRef]
- Hocquart, M.; Drouet, H.; Levet, P.; Raoult, D.; Parola, P.; Eldin, C. Cellulitis of the face associated with SENLAT caused by Rickettsia slovaca detected by qPCR on scalp eschar swab sample: An unusual case report and review of literature. Ticks Tick Borne Dis. 2019, 10, 1142–1145. [Google Scholar] [CrossRef] [PubMed]
- Selmi, M.; Bertolotti, L.; Tomassone, L.; Mannelli, A. Rickettsia slovaca in Dermacentor marginatus and tick-borne lymphadenopathy, Tuscany, Italy. Emerg. Infect. Dis. 2008, 14, 817–820. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.H.; Jia, Y.; Dong, Z.; Zhang, Y.; Xie, S.; Liu, Q.; Wang, Y. Rickettsia aeschlimannii infection in a woman from Xingjiang, Northwestern China. Vector-Borne Zoonotic Dis. 2022, 22, 55–57. [Google Scholar] [CrossRef]
- Tosoni, A.; Mirijello, A.; Ciervo, A.; Mancini, F.; Rezza, G.; Damiano, F.; Cauda, R.; Gasbarrini, A.; Addolorato, G. Human Rickettsia aeschlimannii infection: First case with acute hepatitis and review of the literature. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 2630–2633. [Google Scholar] [PubMed]
- Mokrani, N.; Parola, P.; Tebbal, S.; Dalichaouche, M.; Aouati, A.; Raoult, D. Rickettsia aeschlimannii infection, Algeria. Emerg. Infect. Dis. 2008, 14, 1814–1815. [Google Scholar] [CrossRef]
- Pretorius, A.M.; Birtles, R.J. Rickettsia aeschlimannii: A new pathogenic spotted fever group rickettsia, South Africa. Emerg. Infect. Dis. 2002, 8, 874. [Google Scholar] [CrossRef]
- Lu, M.; Li, F.; Liao, Y.; Shen, J.-J.; Xu, J.-M.; Chen, Y.-Z.; Li, J.-H.; Holmes, E.C.; Zhang, Y.-Z. Epidemiology and diversity of Rickettsiales bacteria in humans and animals in Jiangsu and Jiangxi provinces, China. Sci. Rep. 2019, 9, 13176. [Google Scholar] [CrossRef]
- Tijsse-Klasen, E.; Sprong, H.; Pandak, N. Co-infection of Borrelia burgdorferi sensu lato and Rickettsia species in ticks and in an erythema migrans patient. Parasites Vectors 2013, 6, 347. [Google Scholar] [CrossRef]
- de Sousa, R.; Dos Santos, M.L.; Cruz, C.; Almeida, V.; Garrote, A.R.; Ramirez, F.; Seixas, D.; Manata, M.J.; Maltez, F. Rare case of rickettsiosis caused by Rickettsia monacensis, Portugal, 2021. Emerg. Infect. Dis. 2022, 28, 1068–1071. [Google Scholar] [CrossRef]
- Koetsvelda, J.; Tijsse-Klasen, E.; Herremans, T.; Hovius, J.W.; Sprong, H. Serological and molecular evidence for spotted fever group Rickettsia and Borrelia burgdorferi sensu lato co-infections in the Netherlands. Ticks Tick-Borne Dis. 2016, 7, 371–377. [Google Scholar] [CrossRef]
- Eldin, C.; Virgili, G.; Attard, L.; Edouard, S.; Viale, P.; Raoult, D.; Parola, P. Rickettsia massiliae infection after a tick bite on the eyelid. Travel Med. Infect. Dis. 2018, 26, 66–68. [Google Scholar] [CrossRef] [PubMed]
- Revilla-Marti, P.; Cecilio-Irazola, Á; Gayán-Ordás, J.; Sanjoaquín-Conde, I.; Linares-Vicente, J.A.; Oteo, J.A. Acute myopericarditis associated with tickborne Rickettsia sibirica mongolitimonae. Emerg. Infect. Dis. 2017, 23, 2091–2093. [Google Scholar] [CrossRef] [PubMed]
- Loarte, M.D.C.; Melenotte, C.; Cassir, N.; Cammilleri, S.; Dory-Lautrec, P.; Raoult, D.; Parola, P. Rickettsia mongolitimonae encephalitis, Southern France, 2018. Emerg. Infect. Dis. 2020, 26, 362–364. [Google Scholar] [CrossRef] [PubMed]
- Echevarria-Zubero, R.; Porras-López, E.; Campelo-Gutiérrez, C.; Rivas-Crespo, J.C.; Lucas, A.M.-D.; Cobo-Vázquez, E. Lymphangitis-associated rickettsiosis by Rickettsia sibirica mongolitimonae. J. Pediatr. Infect. Dis. Soc. 2021, 10, 797–799. [Google Scholar] [CrossRef] [PubMed]
- Angelakis, E.; Richet, H.; Raoult, D. Rickettsia sibirica mongolitimonae infection, France, 2010–2014. Emerg. Infect. Dis. 2016, 22, 880–882. [Google Scholar] [CrossRef] [PubMed]
- Nouchi, A.; Monsel, G.; Jaspard, M.; Jannic, A.; Angelakis, E.; Caumes, E. Rickettsia sibirica mongolitimonae infection in a woman travelling from Cameroon: A case report and review of the literature. J. Travel Med. 2017, 25, 1–3. [Google Scholar] [CrossRef]
- Fournier, P.E.; Allombert, C.; Supputamongkol, Y.; Caruso, G.; Brouqui, P.; Raoult, D. Aneruptive fever associated with antibodies to Rickettsia helvetica in Europe and Thailand. J. Clin. Microbiol. 2004, 42, 816–818. [Google Scholar] [CrossRef]
- Baseri, N.; Salehi-Vaziri, M.; Mostafavi, E.; Amiri, F.B.; Latifian, M.; Stenos, J.; Esmaeili, S. Investigation of Rickettsia conorii in patients suspected of having Crimean-Congo hemorrhagic fever. Pathogens 2022, 11, 973. [Google Scholar] [CrossRef]
- Cascio, A.; Colomba, C.; Antinori, S.; Paterson, D.L.; Titone, L. Clarithromycin versus azithromycin in the treatment of Mediterranean spotted fever in children: A randomized controlled trial. Clin. Infect. Dis. 2002, 34, 154–158. [Google Scholar] [CrossRef]
- Kenyon, R.H.; Williams, R.G.; Oster, C.N.; Pedersen, C.E. Prophylactic treatment of Rocky Mountain spotted fever. J. Clin. Microbiol. 1978, 8, 102–104. [Google Scholar] [CrossRef]
- Clements, M.L.; Dumler, J.S.; Fiset, P.; Wisseman, C.L.; Snyder, M.J., Jr.; Levine, M.M. Serodiagnosis of Rocky Mountain spotted fever: Comparison of IgM and IgG enzyme-linked immunosorbent assays and indirect fluorescent antibody test. J. Infect. Dis. 1983, 148, 876–880. [Google Scholar] [CrossRef] [PubMed]
- van Eekeren, L.E.; de Vries, S.G.; Wagenaar, J.F.P.; Spijker, R.; Grobusch, M.P.; Goorhuis, A. Under-diagnosis of rickettsial disease in clinical practice: A systematic review. Travel Med. Infect. Dis. 2018, 26, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Leitner, M.; Rzotkiewicz, S.; Yitzhaki, S.; Keysary, A. Polymerase chain reaction-based diagnosis of Mediterranean spotted fever in serum and tissue samples. Am. J. Trop. Med. Hyg. 2002, 67, 166–169. [Google Scholar] [CrossRef] [PubMed]
- Mendes do Nascimento, E.M.; Colombo, S.; Nagasse-Sugahara, T.; Angerami; Resende, M.; da Silva, L.; Katz, G.; dos Santos, F. Evaluation of PCR-based assay in human serum samples for diagnosis of fatal cases of spotted fever group rickettsiosis. Clin. Microbiol. Infect. 2009, 15 (Suppl. S2), 232–234. [Google Scholar] [CrossRef]
- Kato, C.; Chung, I.; Paddock, C. Estimation of Rickettsia rickettsii copy number in the blood of patients with Rocky Mountain spotted fever suggests cyclic diurnal trends in bacter[a]emia. Clin. Microbiol. Infect. 2016, 22, 394–396. [Google Scholar] [CrossRef]
- Brouqui, P.; Bacellar, F.; Baranton, G.; Birtles, R.; Bjoërsdorff, A.; Blanco, J.; Caruso, G.; Cinco, M.; Fournier, P.; Francavilla, E.; et al. Guidelines for the diagnosis of tick-borne bacterial diseases in Europe. Clin. Microbiol. Infect. 2004, 10, 1108–1132. [Google Scholar] [CrossRef]
- Bechah, Y.; Socolovschi, C.; Raoult, D. Identification of rickettsial infections by using cutaneous swab specimens and PCR. Emerg. Infect. Dis. 2011, 17, 83–86. [Google Scholar] [CrossRef]
- Mouffok, N.; Socolovschi, C.; Renvoise, A.; Parola, P.; Raoult, D. Diagnosis of rickettsioses from eschar swab samples, Algeria. Emerg. Infect. Dis. 2011, 17, 1968–1969. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.M.; Hudson, B.J.; Watts, M.R.; Karagiannis, T.; Fisher, N.J.; Anderson, C.; Roffey, P. Diagnosis of Queensland tick typhus and African tick bite fever by PCR of lesion swabs. Emerg. Infect. Dis. 2009, 15, 963–965. [Google Scholar] [CrossRef]
- Blanda, V.; D’Agostino, R.; Giudice, E.; Randazzo, K.; La Russa, F.; Villari, S.; Vullo, S.; Torina, A. New real-time PCRs to differentiate Rickettsia spp. and Rickettsia conorii. Molecules 2020, 25, 4431. [Google Scholar] [CrossRef]
- Kato, C.Y.; Chung, I.H.; Robinson, L.K.; Austin, A.L.; Dasch, G.A.; Massung, R.F. Assessment of real-time PCR assay for detection of Rickettsia spp. and Rickettsia rickettsii in banked clinical samples. J. Clin. Microbiol. 2013, 51, 314–317. [Google Scholar] [CrossRef]
- Giulieri, S.; Jaton, K.; Cometta, A.; Trellu, L.T.; Greub, G. Development of a duplex real-time PCR for the detection of Rickettsia spp. and typhus group rickettsia in clinical samples. FEMS Immunol. Med. Microbiol. 2012, 64, 92–97. [Google Scholar] [CrossRef]
- Chung, I.H.; Robinson, L.K.; Stewart-Juba, J.J.; Dasch, G.A.; Kato, C.Y. Analytically sensitive Rickettsia species detection for laboratory diagnosis. Am. J. Trop. Med. Hyg. 2022, 106, 1352–1357. [Google Scholar] [CrossRef]
- Wichianchot, S.; Hongsrichan, N.; Maneeruttanarungroj, C.; Pinlaor, S.; Iamrod, K.; Purisarn, A.; Donthaisong, P.; Karanis, P.; Nimsuphan, B.; Rucksaken, R. A newly developed droplet digital PCR for Ehrlichia canis detection: Comparisons to conventional PCR and blood smear techniques. J. Vet. Med. Sci. 2022, 84, 831–840. [Google Scholar] [CrossRef]
- Xu, Q.; Zhang, W.; Wang, Q.; Fu, X.; Han, J.; Huang, Y. Detection of co-infection with Orientia tsutsugamushi and hemorrhagic fever with renal syndrome by next-generation sequencing. Int. J. Neurosci. 2023, 133, 701–704. [Google Scholar] [CrossRef] [PubMed]
- Elliott, I.; Batty, E.M.; Ming, D.; Robinson, M.T.; Nawtaisong, P.; de Cesare, M.; Newton, P.N.; Bowden, R. Oxford Nanopore MinION sequencing enables rapid whole genome assembly of Rickettsia typhi in a resource-limited setting. Am. J. Trop. Med. Hyg. 2020, 102, 408–414. [Google Scholar] [CrossRef]
- Stafford, I.A.; Centeno, F.H.; Al Mohajer, M.; Parkerson, G.; Woc-Colburn, L.; Burgos-Lee, A.J.; Rac, M.; Dunn, J.; Muldrew, K. Successful detection of unrecognized Rickettsia typhi in pregnancy using cell-free next-generation sequencing. Case Rep. Obstet. Gynecol. 2020, 2020, 6767351. [Google Scholar] [CrossRef] [PubMed]
- Chaorattanakawee, S.; Korkusol, A.; Tippayachai, B.; Promsathaporn, S.; Poole-Smith, B.K.; Takhampunya, R. Amplicon-based next generation sequencing for rapid identification of Rickettsia and ectoparasite species from entomological surveillance in Thailand. Pathogens 2021, 10, 215. [Google Scholar] [CrossRef] [PubMed]
- Greay, T.L.; Evasco, K.L.; Evans, M.L.; Oskam, C.L.; Magni, P.A.; Ryan, U.M.; Irwin, P.J. Illuminating the bacterial microbiome of Australian ticks with 16S and Rickettsia-specific next-generation sequencing. Curr. Res. Parasitol. Vector Borne Dis. 2021, 1, 100037. [Google Scholar] [CrossRef]
- Dasch, G.A.; Ramaiah, A.; Holmes, Z.C.; Zambrano, M.L.; Shirey, T.B. Use of the Ion Torrent PGM for determining the genomic sequences of Francisella and Coxiella-like endosymbionts and Rickettsia directly from hard ticks. In Contemporary Acarology; Skvarla, M.J., Ochoa, R., Rodrigues, J.C.V., Hutcheson, H.J., Eds.; Springer Verlag: Berlin/Heidelberg, Germany, 2017; Chapter 1; Volume 1, pp. 1–35. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Symptom or Clinical Finding | MSF in Crimea | MSF in Bulgaria | MSF in Turkey | MSF in Romania | ||||
|---|---|---|---|---|---|---|---|---|
| Alymov 1939 & Andreev 1941 [21,22] | Gafarova 2004 [63] | Popivanova et al., 2007 [50] | Pishmisheva et al., 2014 a [48] | Baltadzhiev et al., 2020 b [47] | Mert et al., 2006 [36] | Kuloglu et al., 2012 [35] | Pitigoi et al., 2013 [31] | |
| Number of cases observed | Unknown | 137 | 774 | 257 (1253) | 544 | 15 | 128 | 171 |
| Incubation period | 5–10 | 2–15 (5–7 average) | 3–10< days | 1–14 days (3.2 days average) | 5–7 days | 0–6 days | NR | |
| Acute onset | yes | yes | yes | yes | yes | yes | yes | yes |
| Fever | 100% (39–40 °C) | 100% (39–40 °C) | 99.24% | 98.8% | 99.14–100% | 100% (39.5–40 °C) | 100% | 99.4% |
| Fever (duration) | 10–15 days | 5–10 days | 3–7< days | 2.5 d (average) | NR | 7–14 days | 1–8 days | |
| Headache | 83% | 33.69% | 18.7% (61.93%) | 33.62–34.11% | 87% | 66.9% | 43.1% (n = 151) | |
| Myalgia (arthralgia) | 54.7% | 74.13% | 40.08% (78.77%) | 74.13–68.23% | 93% | 60.3% | 43.4% (n = 152) d | |
| Malaise (adynamia) | 50% | NR | 68.31–54.11% | NR | NR | NR | ||
| Arthralgia | 29.2% | NR | 100% | NR | NR | |||
| Chills | yes | 67.39% | NR | 67.45–60% | 100% | NR | NR | |
| Eschar | 72% | 81% | 77.04% | 72.76% (67.2%) | 76.93–73.68% | 13% | 70.3% | 67.3% |
| Lymphadenitis | 32% | 23.3% | 13.3% | Not observed | NR | NR | NR | |
| Painful lymph nodes | 16% | 45% | Mostly absent | 54.09% (10.93%) | 39.2% a | NR | NR | NR |
| Persisting pigmentation in the area of eschar and/or rash | 2–3 years | 2–3 months | Yes [after rash} | NR | NR | NR | NR | NR |
| Rash, onset | 2–4 days | 2–7< days | 3–5 days | NR | 3–5 days | 2nd day of fever | 12 h to 10 days | NR |
| Rash, duration, days | 1–4 days | 4–5 days | NR | NR | NR | NR | NR | |
| Rash appearance | Polymorphic, maculopapular to papulo-petechial | Polymorphic: maculopapular (73%) to roseo-papular (23.3%) | Papular (49.9%), maculopapular (50.09%) and hemorrhagic 915.69%) | Maculopapular a | Maculopapular | Maculopapular, also petechiae in 4 cases | Maculopapular and petechial | Maculopapular or purpuric |
| Rash, occurrence | 80–100% | 77.4% | 99.27% | 100% (98.2%) | 100% | 100% | 95.3% (10.6%) | 98.2% |
| Rash, location | Trunk to palm and soles | Trunk to face, palms and soles | Palms and soles, sometimes face and head | Face, palms and soles | Face, body trunk and limbs including palms and feet | Limbs and trunk (centripetal type) | Palms and soles | NR |
| Hypotension | 36% | 21.8% | NR | NR | NR | NR | NR | NR |
| Hepatomegaly | 40% | 42.3% (n = 58) | 60.29% | 83.27% (78.93%) | 46.44–23.68% | 13% | 11.6% | NR |
| Splenomegaly | 32% | 2.2% | 46.44% | Yes a1 | 13.84–63.15% b | 13% | 5.6% | NR |
| Euphoria | 64% | NR | NR | NR | NR | NR | NR | |
| Depression | 16% | NR | NR | NR | NR | NR | ||
| Insomnia | 80% | NR | NR | NR | NR | NR | ||
| Severity of disease | ||||||||
| Severe | 12% | 14.6% | 33.85% | 2.7% | 29.5% a | 0% | 10.9% | 0% |
| Average|Moderate severity | 20% | 83.2% | 56.68% | 97.3% | 41.16–32.79 | 100% | 89.1% | 100% |
| Decreased appetite (anorexia) | 58.3% | 57.35% | NR | 57.32–70.58% | NR | NR | NR | |
| Nausea (vomiting) | 14.4% | 11.29% (17.66%) | NR | 11.2 (17.67) 52.94 (50.98)% | NR | NR | NR | |
| Abdominal pain | + | + | 6.73% | NR | 6.68–23.52% | NR | NR | NR |
| Diarrhea | + | + | 1.82% | NR | 1.72–5.88% | NR | NR | NR |
| Sore throat | No | No | 0.36% | NR | 0.43–8.23% | 20% c | NR | 16.8% (n = 149) d |
| Conjunctivitis | NR | 16% (n = 20) | 5.1% | NR | 20% | 19.8% | ||
| Laboratory findings: | ||||||||
| Leukopenia | + | + | 3.86% | NR | NR b | 13% | 12.7% | NR |
| Monocytosis | + | + | NR | NR | NR b | NR | NR | NR |
| Leucocytosis | + | 11.3% | 9.62% | NR | NR b | 74% | 32% | 31.8% (n = 170) |
| Thrombocytopemia | _ | 11.03% | ↓ most cases | NR | NR b | 33% | 52.5% | 50.9% (n = 159) |
| Erythrocyte precipitation rate | ↑, 72% | 84.5% (n = 137) | NR | NR b | ↑, 100% (n = 7) | NR | ↑, 55.1% (n = 138) | |
| ↑ C-reactive protein | NR | 98% | NR | |||||
| Proteinuria | 32% | 29.9% | NR | NR | NR | NR | ||
| Elevation of liver enzymes (AST and/or ALT) | AST: 34.3% ALT: 72.7% | 58.1% (54.46%) | >50% a1 | 60% | 72% | 78.5% (n = 158) | ||
| Fatality | <2% | None | 9.44% [adults] | 0% | 3.5% (4.1%) b | None | 1.6% | 0% |
| Feature or Symptom | Etiological Agent | |||||
|---|---|---|---|---|---|---|
| R. raoultii | R. slovaca | R. aeschlimanii | R. monacensis | R. massiliae | R. sibirica mongolotimonae | |
| Number of cases b | 72 | 143 | 10 | 12 | 9 | 56 |
| Case geography | France, Slovakia, Poland, Russia, China, Romania, Spain | France, Slovakia, Italy, Germany, Hungary, Spain, Poland, Romania, Russia | South Africa, Greece, Algeria, Italy, Morocco, Russia, China | Spain, Italy, Portugal, Netherlands, South Korea, China | Italy, France, Romania, Greece, Tunisia, Argentina | France, Spain, Portugal, Greece, Egypt, Algeria, Sri Lanka, Turkey |
| Primary tick vector | Dermacentor sp. | Dermacentor sp. | Hyalomma sp. | Ixodes sp. | Rhipicephalus sp. | Hyalomma sp., Rhipicephalus sp. |
| Prevalence in ticks c | 1.8–58% | 1.7–24.3% | 0.8–77.2% | 0.5–57% | 2–92% | 4–8% |
| Fever | 37% (n = 70) | 21.8% (n = 133) | 80% (39–40 °C) | 100% (38–40 °C) | 100% | 100% |
| Eschar | 20.3% (n = 69) | 40.5% (n = 116) | 80% | 75% (n = 8) | 100% | 94.6% |
| Rash | 5.6% | 8% (n = 124) | 60% | 87.5% (n = 8) | 80% | 73% |
| Rash, type | Not specified in reports | Frequently not specified in reports | Maculopapular | Macular, maculopapular or erythematous | Maculopapular to purpuric rash | Maculopapular |
| Headache | 25% | 53% d | 50% | 75% (n = 8) | 44% | Reported very rarely |
| Lymphadenopathy | 32.9% (n = 70) | 60.8% (n = 120) | NR | 50% (n = 8) | 22% | 57.7% (n = 26) |
| Lymphangitis | NR | NR | NR | NR | NR | 37.5% |
| Complications, atypical symptoms | Pulmonary edema, lethargy, | Alopecia, asthenia, cellulitis of the face | Acute hepatitis, arthritis, retina hemorrhage | NR | Acute vision loss, seizure, myalgia | Encephalitis, myopericarditis, retinal vasculitis |
| Co-infection | Tick-borne encephalitis virus, B. miyamotoi, Tacheng tick virus, R. slovaca | Coxiella burnetii, R. raoultii | B. burgdorferi | B. burgdorferi, O. tsutsugamushi | NR | NR |
| References | [129,130,131,132,133] | [7,126,129,130,131,134,135] | [130,136,137,138,139] | [140,141,142,143] | [144] | [123,145,146,147,148,149] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gafarova, M.T.; Eremeeva, M.E. History and Current Status of Mediterranean Spotted Fever (MSF) in the Crimean Peninsula and Neighboring Regions along the Black Sea Coast. Pathogens 2023, 12, 1161. https://doi.org/10.3390/pathogens12091161
Gafarova MT, Eremeeva ME. History and Current Status of Mediterranean Spotted Fever (MSF) in the Crimean Peninsula and Neighboring Regions along the Black Sea Coast. Pathogens. 2023; 12(9):1161. https://doi.org/10.3390/pathogens12091161
Chicago/Turabian StyleGafarova, Muniver T., and Marina E. Eremeeva. 2023. "History and Current Status of Mediterranean Spotted Fever (MSF) in the Crimean Peninsula and Neighboring Regions along the Black Sea Coast" Pathogens 12, no. 9: 1161. https://doi.org/10.3390/pathogens12091161