

HPV and Other Risk Factors Involved in Pharyngeal Neoplasm—Clinical and Morphopathological Correlations in the Southwestern Region of Romania
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
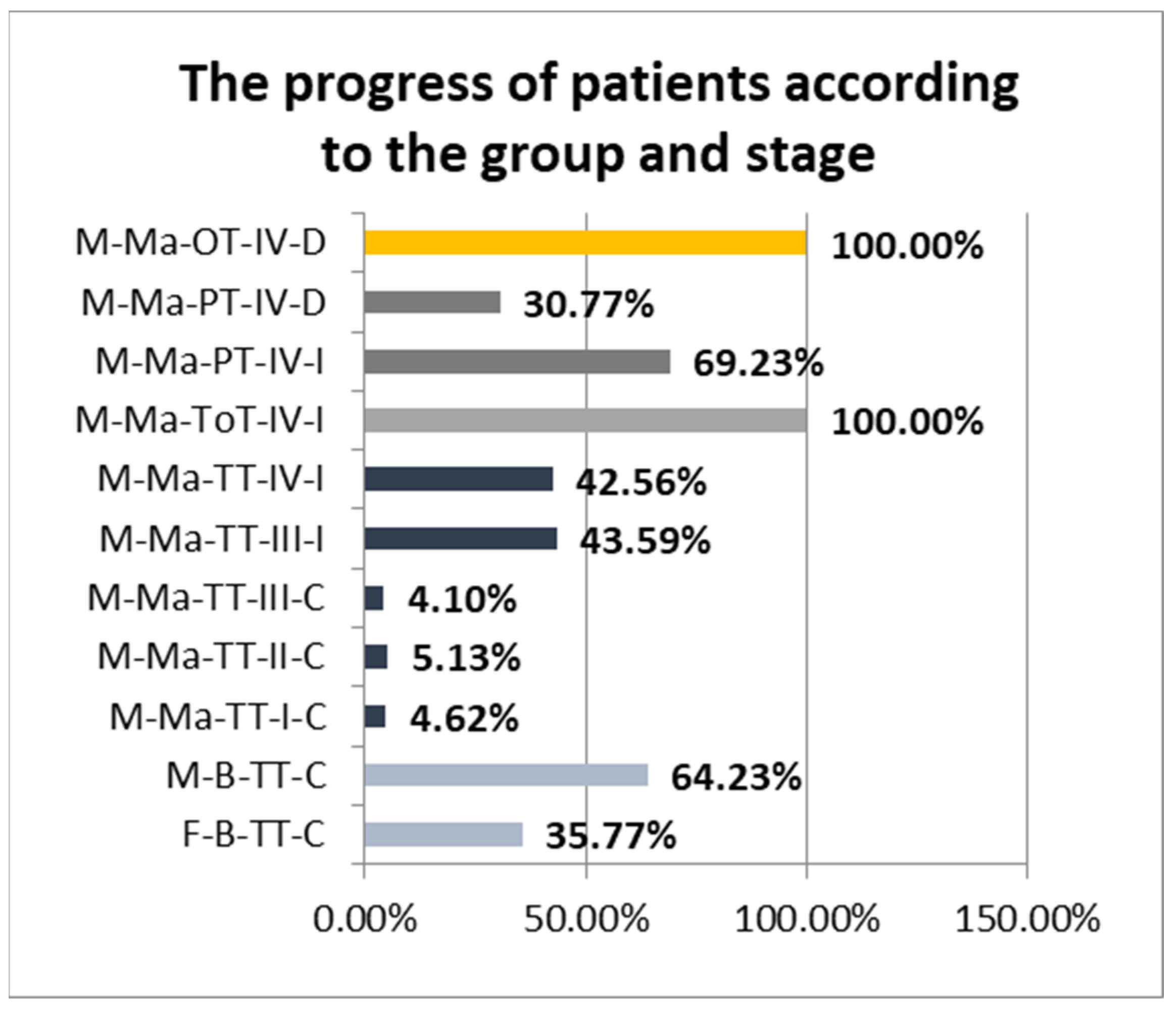
3.1. Results in Terms of Clinical Aspects and Risk Factors
- -
- 4.62% Stage I, completely cured after treatment;
- -
- 5.13% Stage II, completely cured after treatment;
- -
- 4.1% Stage III completely cured after treatment;
- -
- 43.59% Stage III improved after treatment;
- -
- 42.56% Stage IV improved after treatment.
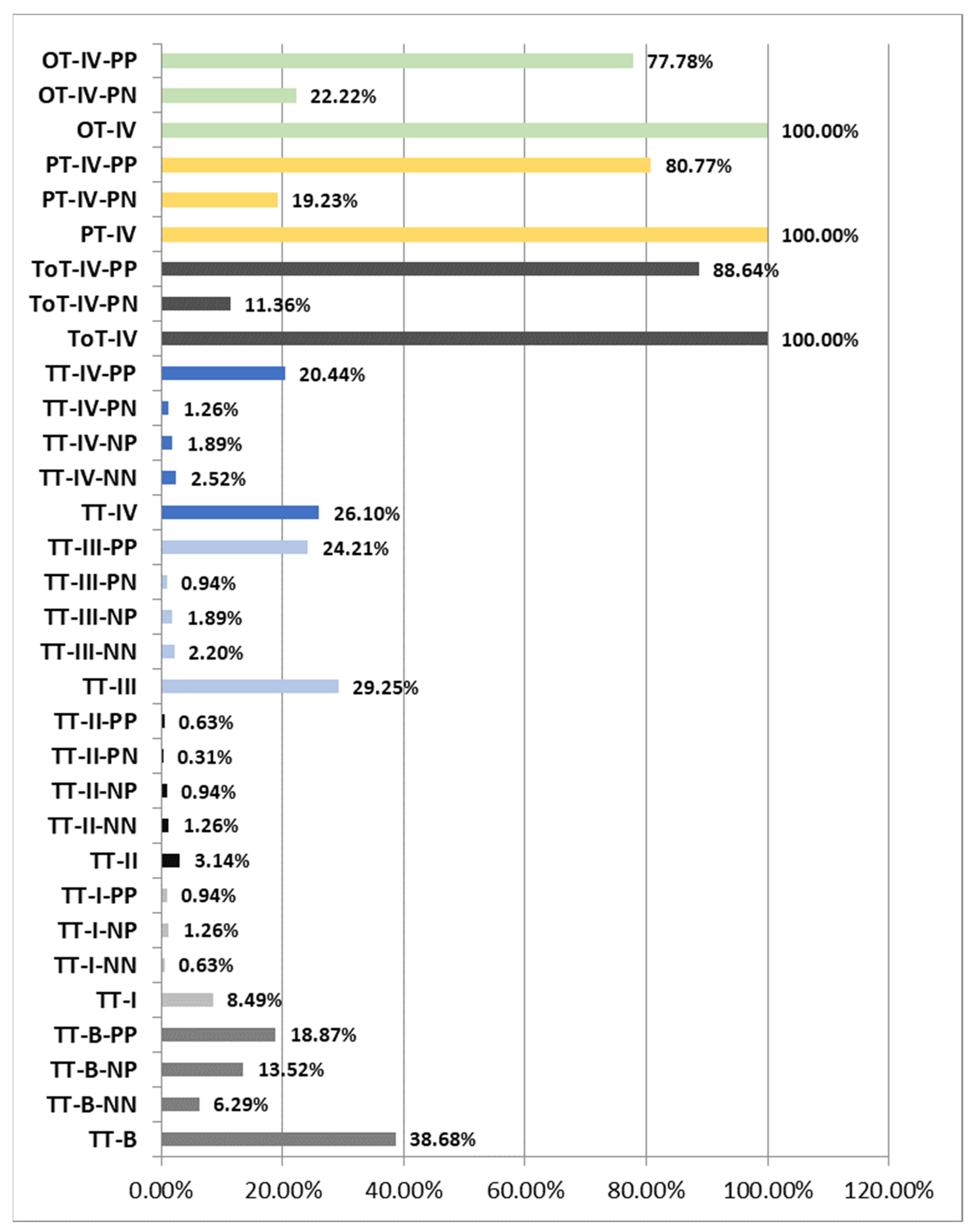
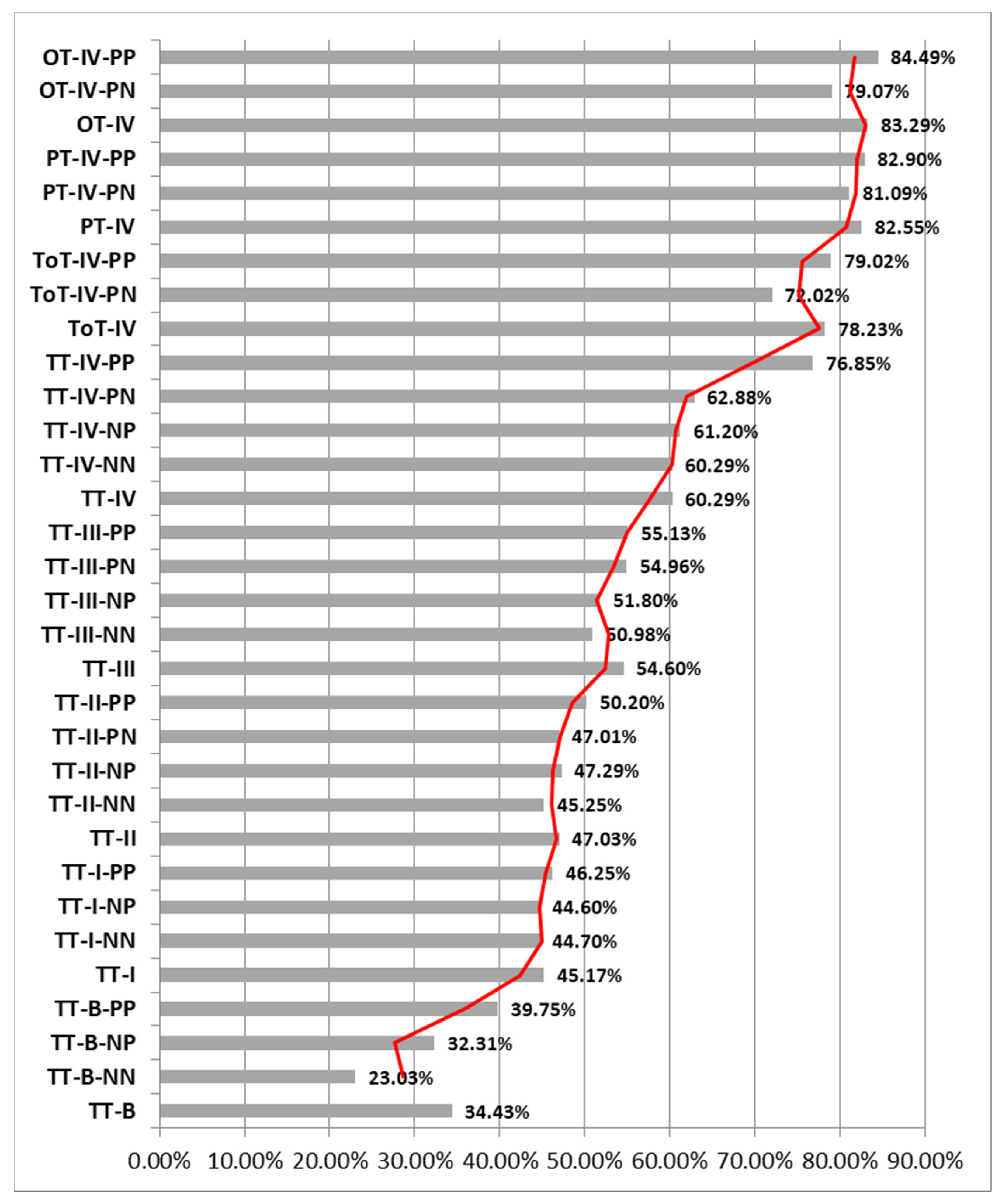
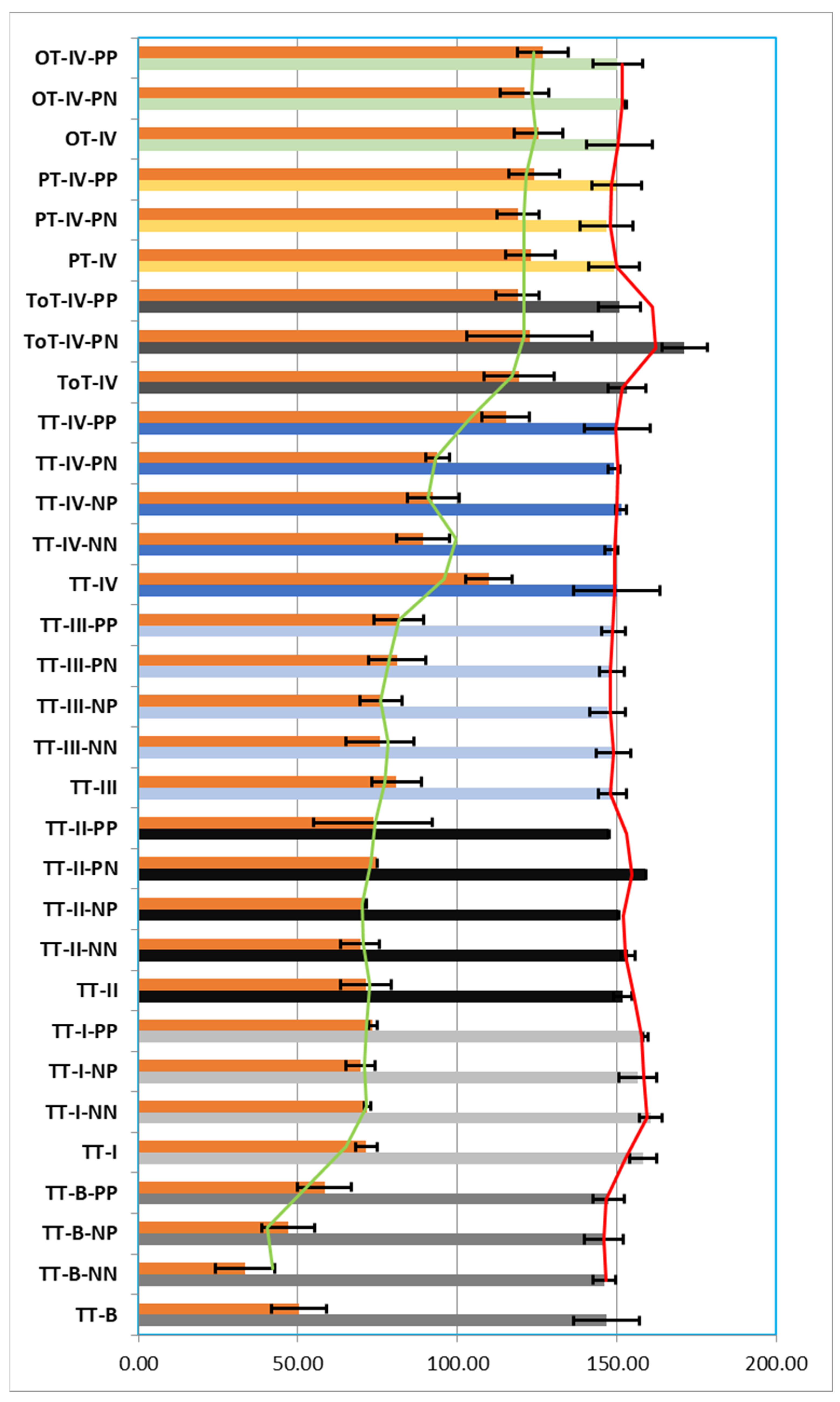
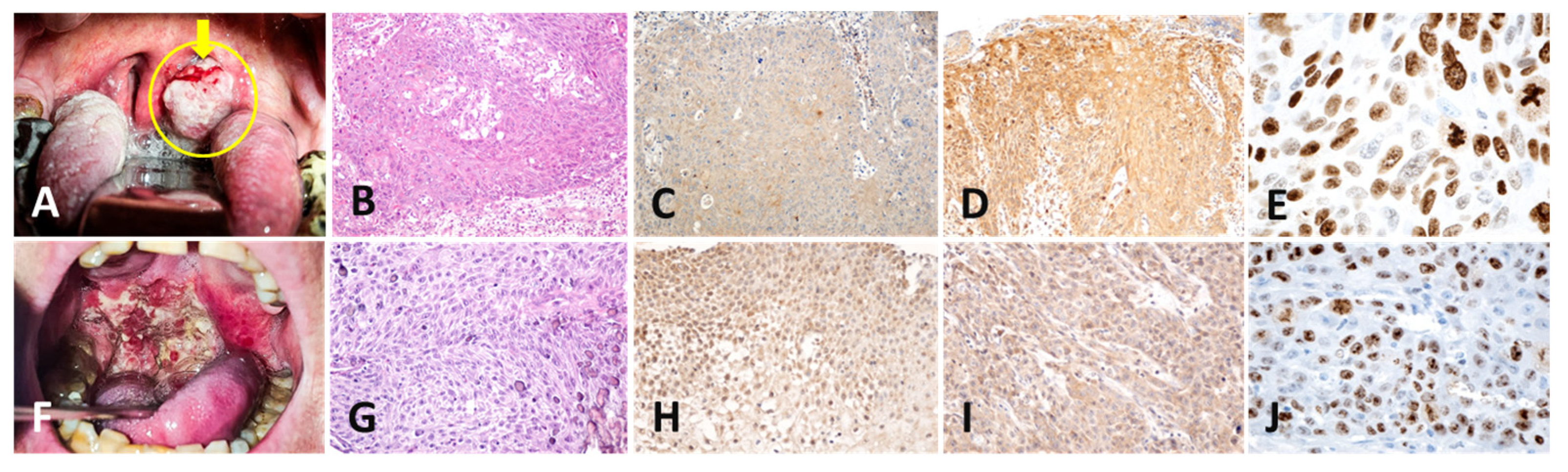
3.2. Results of the Histological and Immunohistochemical Study
- The analyzed TT-B-NN had a mean number of nuclei/field 40× of 146.13 nuclei (±9.24 nuclei), of which a percentage of 23.03% of the total nuclei/field was immunomarked, and 77.08% of the nuclei showed a negative reaction for the anti-Ki67 antibody;
- The analyzed TT-B-NP had a mean number of nuclei/field 40× of 146.03 nuclei (±8.44 nuclei), of which a percentage of 32.31% of the total nuclei/field was immunomarked and 67.84% of the nuclei showed a negative reaction for the anti-Ki67 antibody;
- The analyzed TT-B-PP had a mean number of nuclei/field 40× of 147.47 nuclei (±8.49 nuclei), of which a percentage of 39.75% of the total nuclei/field was immunomarked, and 60.37% of the nuclei showed a negative reaction for the anti-Ki67 antibody. We thus observed that in cases of premalignant tumors, the percentage of Ki67-positive nuclei increased proportionally with the presence of immunoreactivity against the two anti-p16 and anti-HPV antibodies (Figure 2, Figure 3 and Figure 4).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Smokeless Tobacco and Some Tobacco-specific N-Nitrosamines; IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, No. 89; International Agency for Research on Cancer: Lyon, France, 2007. Available online: https://www.ncbi.nlm.nih.gov/books/NBK326497/ (accessed on 1 April 2022).
- Plummer, M.; de Martel, C.; Vignat, J.; Ferlay, J.; Bray, F.; Franceschi, S. Global burden of cancers attributable to infections in 2012: A synthetic analysis. Lancet Glob. Health 2016, 4, e609–e616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ndiaye, C.; Mena, M.; Alemany, L.; Arbyn, M.; Castellsagué, X.; Laporte, L.; Bosch, F.X.; de Sanjosé, S.; Trottier, H. HPV DNA, E6/E7 mRNA, and p16INK4a detection in head and neck cancers: A systematic review and meta-analysis. Lancet Oncol. 2014, 15, 1319–1331, Erratum in Lancet Oncol. 2015, 16, e262. [Google Scholar] [CrossRef] [PubMed]
- Kreimer, A.R.; Clifford, G.M.; Boyle, P.; Franceschi, S. Human papillomavirus types in head and neck squamous cell carcinomas worldwide: A systematic review. Cancer Epidemiol. Biomark. Prev. 2005, 14, 467–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taberna, M.; Mena, M.; Pavón, M.A.; Alemany, L.; Gillison, M.L.; Mesía, R. Human papillomavirus-related oropharyngeal cancer. Ann. Oncol. 2017, 28, 2386–2398. [Google Scholar] [CrossRef]
- Wang, M.B.; Liu, I.Y.; Gornbein, J.A.; Nguyen, C.T. HPV-Positive Oropharyngeal Carcinoma: A Systematic Review of Treatment and Prognosis. Otolaryngol. Head Neck Surg. 2015, 153, 758–769. [Google Scholar] [CrossRef]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human Papillomavirus and Survival of Patients with Oropharyngeal Cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [Green Version]
- Husain, N.; Neyaz, A. Human papillomavirus associated head and neck squamous cell carcinoma: Controversies and new concepts. J. Oral Biol. Craniofacial Res. 2017, 7, 198–205. [Google Scholar] [CrossRef] [Green Version]
- Castellsagué, X. Natural history and epidemiology of HPV infection and cervical cancer. Gynecol. Oncol. 2008, 110 (Suppl. S2), S4–S7. [Google Scholar] [CrossRef]
- Dahlstrom, K.R.; Calzada, G.; Hanby, J.D.; Garden, A.S.; Glisson, B.S.; Li, G.; Roberts, D.B.; Weber, R.S.; Sturgis, E.M. An evolution in demographics, treatment, and outcomes of oropharyngeal cancer at a major cancer center: A staging system in need of repair. Cancer 2013, 119, 81–89. [Google Scholar] [CrossRef] [Green Version]
- Sandulache, V.C.; Hamblin, J.; Lai, S.; Pezzi, T.; Skinner, H.D.; Khan, N.A.; Dioun, S.M.; Hartman, C.; Kramer, J.; Chiao, E.; et al. Oropharyngeal squamous cell carcinoma in the veteran population: Association with traditional carcinogen exposure and poor clinical outcomes. Head Neck 2015, 37, 1246–1253. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Fakhry, C.; D’souza, G. Projected Association of Human Papillomavirus Vaccination with Oropharynx Cancer Incidence in the US, 2020-2045. JAMA Oncol. 2021, 7, e212907. [Google Scholar] [CrossRef] [PubMed]
- Halec, G.; Schmitt, M.; Dondog, B.; Sharkhuu, E.; Wentzensen, N.; Gheit, T.; Tommasino, M.; Kommoss, F.; Bosch, F.X.; Franceschi, S.; et al. Biological activity of probable/possible high-risk human papillomavirus types in cervical cancer. Int. J. Cancer 2013, 132, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Jung, A.C.; Briolat, J.; Millon, R.; de Reyniès, A.; Rickman, D.; Thomas, E.; Abecassis, J.; Clavel, C.; Wasylyk, B. Biological and clinical relevance of transcriptionally active human papillomavirus (HPV) infection in oropharynx squamous cell carcinoma. Int. J. Cancer 2010, 126, 1882–1894. [Google Scholar] [CrossRef] [PubMed]
- Holzinger, D.; Schmitt, M.; Dyckhoff, G.; Benner, A.; Pawlita, M.; Bosch, F.X. Viral RNA patterns and high viral load reliably define oropharynx carcinomas with active HPV16 involvement. Cancer Res. 2012, 72, 4993–5003. [Google Scholar] [CrossRef] [Green Version]
- Smeets, S.J.; Hesselink, A.T.; Speel, E.-J.M.; Haesevoets, A.; Snijders, P.J.; Pawlita, M.; Meijer, C.J.; Braakhuis, B.J.; Leemans, C.R.; Brakenhoff, R.H. A novel algorithm for reliable detection of human papillomavirus in paraffin embedded head and neck cancer specimen. Int. J. Cancer 2007, 121, 2465–2472. [Google Scholar] [CrossRef]
- Pannone, G.; Rodolico, V.; Santoro, A.; Muzio, L.L.; Franco, R.; Botti, G.; Aquino, G.; Pedicillo, M.C.; Cagiano, S.; Campisi, G.; et al. Evaluation of a combined triple method to detect causative HPV in oral and oropharyngeal squamous cell carcinomas: p16 Immunohistochemistry, Consensus PCR HPV-DNA, and In Situ Hybridization. Infect. Agents Cancer 2012, 7, 4. [Google Scholar] [CrossRef]
- Rietbergen, M.M.; Brakenhoff, R.H.; Bloemena, E.; Witte, B.I.; Snijders, P.J.F.; Heideman, D.A.M.; Boon, D.; Koljenovic, S.; Jong, R.J.B.-D.; Leemans, C.R. Human papillomavirus detection and comorbidity: Critical issues in selection of patients with oropharyngeal cancer for treatment De-escalation trials. Ann. Oncol. 2013, 24, 2740–2745. [Google Scholar] [CrossRef]
- Prigge, E.-S.; Arbyn, M.; von Knebel Doeberitz, M.; Reuschenbach, M. Diagnostic accuracy of p16INK4aimmunohistochemistry in oropharyngeal squamous cell carcinomas: A systematic review and meta-analysis. Int. J. Cancer 2017, 140, 1186–1198. [Google Scholar] [CrossRef] [Green Version]
- Garnaes, E.; Frederiksen, K.; Kiss, K.; Andersen, L.; Therkildsen, M.H.; Franzmann, M.B.; Specht, L.; Andersen, E.; Norrild, B.; Kjaer, S.K.; et al. Double positivity for HPV DNA/p16 in tonsillar and base of tongue cancer improves prognostication: Insights from a large population-based study. Int. J. Cancer 2016, 139, 2598–2605. [Google Scholar] [CrossRef]
- Marklund, L.; Näsman, A.; Ramqvist, T.; Dalianis, T.; Munck-Wikland, E.; Hammarstedt, L. Prevalence of human papillomavirus and survival in oropharyngeal cancer other than tonsil or base of tongue cancer. Cancer Med. 2012, 1, 82–88. [Google Scholar] [CrossRef]
- Mirghani, H.; Amen, F.; Moreau, F.; Guigay, J.; Hartl, D.; Guily, J.L.S. Oropharyngeal cancers: Relationship between epidermal growth factor receptor alterations and human papillomavirus status. Eur. J. Cancer 2014, 50, 1100–1111. [Google Scholar] [CrossRef]
- Warnakulasuriya, S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009, 45, 309–316. [Google Scholar] [CrossRef]
- Dissanayaka, W.; Pitiyage, G.; Kumarasiri, P.V.R.; Liyanage, R.L.P.R.; Dias, D.; Tilakaratne, W.M. Clinical and histopathologic parameters in survival of oral squamous cell carcinoma. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 113, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Koontongkaew, S. The tumor microenvironment contribution to development, growth, invasion and metastasis of head and neck squamous cell carcinomas. J. Cancer 2013, 4, 66–83. [Google Scholar] [CrossRef]
- Gandini, S.; Botteri, E.; Iodice, S.; Boniol, M.; Lowenfels, A.B.; Maisonneuve, P.; Boyle, P. Tobacco smoking and cancer: A meta-analysis. Int. J. Cancer 2008, 122, 155–164. [Google Scholar] [CrossRef]
- Marron, M.; Boffetta, P.; Zhang, Z.-F.; Zaridze, D.; Wünsch-Filho, V.; Winn, D.M.; Wei, Q.; Talamini, R.; Szeszenia-Dabrowska, N.; Sturgis, E.M.; et al. Cessation of alcohol drinking, tobacco smoking and the reversal of head and neck cancer risk. Int. J. Epidemiol. 2010, 39, 182–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.-C.A.; Marron, M.; Benhamou, S.; Bouchardy, C.; Ahrens, W.; Pohlabeln, H.; Lagiou, P.; Trichopoulos, D.; Agudo, A.; Castellsague, X.; et al. Active and involuntary tobacco smoking and upper aerodigestive tract cancer risks in a multicenter case-control study. Cancer Epidemiol. Biomark. Prev. 2009, 18, 3353–3361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parise, O., Jr. Câncer de Boca: Aspectos Básicos e Terapêuticos; Sarvier: São Paulo, Brazil, 2000. [Google Scholar]
- Choudhari, S.K.; Chaudhary, M.; Gadbail, A.R.; Sharma, A.; Tekade, S. Oxidative and antioxidative mechanisms in oral cancer and precancer: A review. Oral Oncol. 2014, 50, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Reidy, J.; McHugh, E.; Stassen, L. A review of the relationship between alcohol and oral cancer. Surgeon 2011, 9, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Migeon, B.R. Why females are mosaics, x-chromosome inactivation, and sex differences in disease. Gend. Med. 2007, 4, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Pessach, I.M.; Notarangelo, L.D. X-linked primary immunodeficiencies as a bridge to better understandingX-chromosome related autoimmunity. J. Autoimmun. 2009, 33, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Dziegielewski, P.T.; Nguyen, T.J.; Jeffery, C.C.; O’connell, D.A.; Harris, J.R.; Seikaly, H. The effects of geography on survival in patients with oral cavity squamous cell carcinoma. Oral Oncol. 2015, 51, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Segel, J.E.; Lengerich, E.J. Rural-urban differences in the association between individual, facility, and clinical characteristics and travel time for cancer treatment. BMC Public Health 2020, 20, 196. [Google Scholar] [CrossRef] [PubMed]
- Li, L.T.; Jiang, G.; Chen, Q.; Zheng, J.N. Ki67 is a promising molecular target in the diagnosis of cancer (review). Mol. Med. Rep. 2015, 11, 1566–1572. [Google Scholar] [CrossRef] [Green Version]
- Nobori, T.; Miura, K.; Wu, D.J.; Lois, A.; Takabayashi, K.; Carson, D.A. Deletions of the cyclin-dependent kinase-4 inhibitor gene in multiple human cancers. Nature 1994, 368, 753–756. [Google Scholar] [CrossRef]
- Stone, S.; Jiang, P.; Dayananth, P.; Tavtigian, S.V.; Katcher, H.; Parry, D.; Peters, G.; Kamb, A. Complex structure and regulation of the P16 (MTS1) locus. Cancer Res. 1995, 55, 2988–2994. [Google Scholar]
- Zhou, P.; Yu, Y.-F.; Lian, C.-L.; Wang, J.; Zhuo, R.-G.; Wu, S.-G. Survival Outcomes and Treatment Decision by Human Papillomavirus Status Among Patients with Stage IVC Head and Neck Squamous Cell Carcinoma. Front. Oncol. 2021, 11, 668066. [Google Scholar] [CrossRef]
- Wilde, D.C.; Castro, P.D.; Bera, K.; Lai, S.; Madabhushi, A.; Corredor, G.; Koyuncu, C.; Lewis, J.S.; Lu, C.; Frederick, M.J.; et al. Oropharyngeal cancer outcomes correlate with p16 status, multinucleation and immune infiltration. Mod. Pathol. 2022, 35, 1045–1054. [Google Scholar] [CrossRef]
- Oguejiofor, K.; Hall, J.; Mani, N.; Douglas, C.; Slevin, N.; Homer, J.; Hall, G.; West, C. The prognostic significance of the biomarker p16 in oropharyngeal squamous cell carcinoma. Clin. Oncol. 2013, 25, 630–638. [Google Scholar] [CrossRef]
- Balgkouranidou, I.; Liloglou, T.; Lianidou, E.S. Lung cancer epigenetics: Emerging biomarkers. Biomark. Med. 2013, 7, 49–58. [Google Scholar] [CrossRef] [Green Version]
- Sinha, P.; Thorstad, W.; Nussenbaum, B.; Haughey, B.; Adkins, D.; Kallogjeri, D.; Lewis, J.S., Jr. Distant metastasis in p16-positive oropharyngeal squamous cell carcinoma: A critical analysis of patterns and outcomes. Oral Oncol. 2014, 50, 45–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McBride, A.A.; Warburton, A. The role of integration in oncogenic progression of HPV-associated cancers. PLoS Pathog. 2017, 13, e1006211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pett, M.; Coleman, N. Integration of high-risk human papillomavirus: A key event in cervical carcinogenesis? J. Pathol. 2007, 212, 356–367. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibody | Manufacturer | Clone | Antigenic Exposure | Secondary Antibody | Dilution | Labeling |
|---|---|---|---|---|---|---|
| Anti-Ki67 | Dako | MIB-1 | EDTA, pH 9 | Monoclonal mouse anti-human Ki67 | 1:50 | Cells in division in the G1, S, G2 and M phase |
| Anti-p16 | Invitrogen | 1D7D2 | Citrate, pH 6 | p16INK4a antibody (1D7D2) | 1:1000 | Tumor suppressor protein |
| Anti-HPV | Abcam | K1H8 | Citrate, pH 6 | Mouse monoclonal (K1H8) to HPV | 1:50 | HPV-infected cells |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mogoantă, C.A.; Ciolofan, M.S.; Istrate-Ofițeru, A.-M.; Mogoantă, S.-Ș.; Roșu, G.-C.; Anghelina, F.; Căpitanescu, A.-N.; Opriscan, I.C.; Ionovici, N.; Mitroi, M.R.; et al. HPV and Other Risk Factors Involved in Pharyngeal Neoplasm—Clinical and Morphopathological Correlations in the Southwestern Region of Romania. Pathogens 2023, 12, 984. https://doi.org/10.3390/pathogens12080984
Mogoantă CA, Ciolofan MS, Istrate-Ofițeru A-M, Mogoantă S-Ș, Roșu G-C, Anghelina F, Căpitanescu A-N, Opriscan IC, Ionovici N, Mitroi MR, et al. HPV and Other Risk Factors Involved in Pharyngeal Neoplasm—Clinical and Morphopathological Correlations in the Southwestern Region of Romania. Pathogens. 2023; 12(8):984. https://doi.org/10.3390/pathogens12080984
Chicago/Turabian StyleMogoantă, Carmen Aurelia, Mircea Sorin Ciolofan, Anca-Maria Istrate-Ofițeru, Stelian-Ștefăniță Mogoantă, Gabriela-Camelia Roșu, Florin Anghelina, Alina-Nicoleta Căpitanescu, Ioana Cristina Opriscan, Nina Ionovici, Mihaela Roxana Mitroi, and et al. 2023. "HPV and Other Risk Factors Involved in Pharyngeal Neoplasm—Clinical and Morphopathological Correlations in the Southwestern Region of Romania" Pathogens 12, no. 8: 984. https://doi.org/10.3390/pathogens12080984