
Variability of High-Risk Human Papillomavirus and Associated Factors among Women in Sub-Saharan Africa: A Systematic Review and Meta-Analysis
 , , , , ,
, , , , ,
Abstract
:1. Background
2. Methods
2.1. Design
2.2. Data Sources and Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Patient and Public Involvement
2.5. Study Selection and Quality Assessment
2.6. Data Extraction
2.7. Data Analysis
3. Results
3.1. Study Characteristics
3.2. Pooled Prevalence of HR-HPV
3.3. Subgroup Analysis
3.4. Laboratory Methods to Detect HR-HPV Infection from the Included Studies
3.5. Factors Associated with HR-HPV Infection from the Included Studies
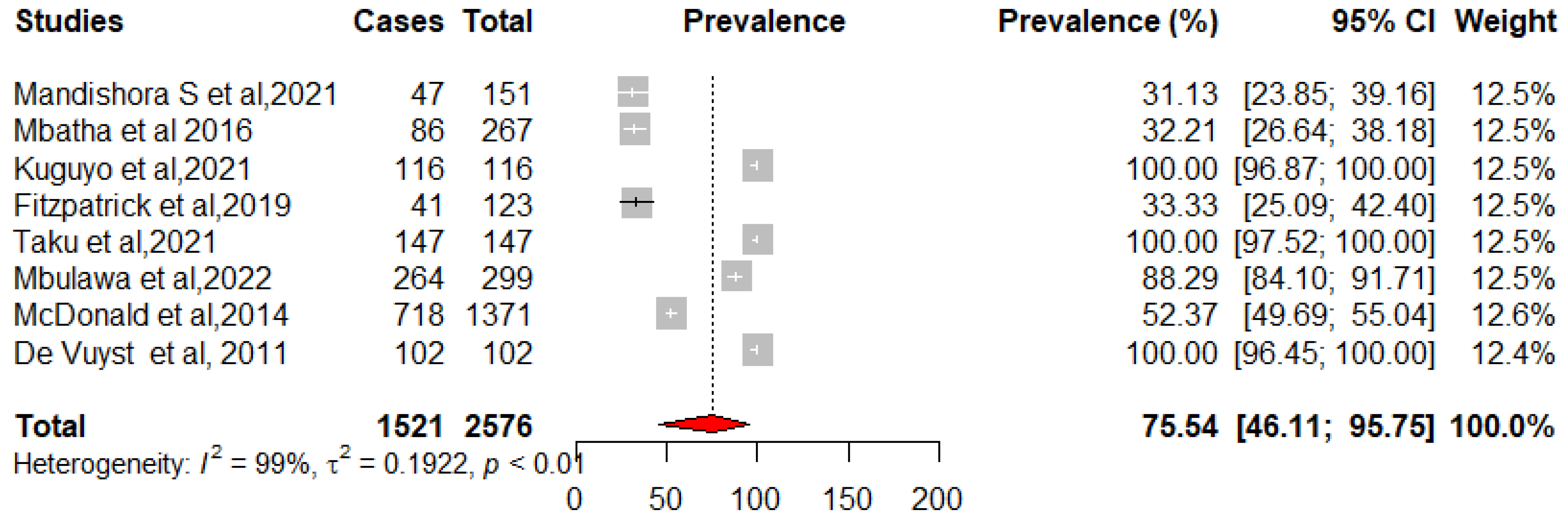
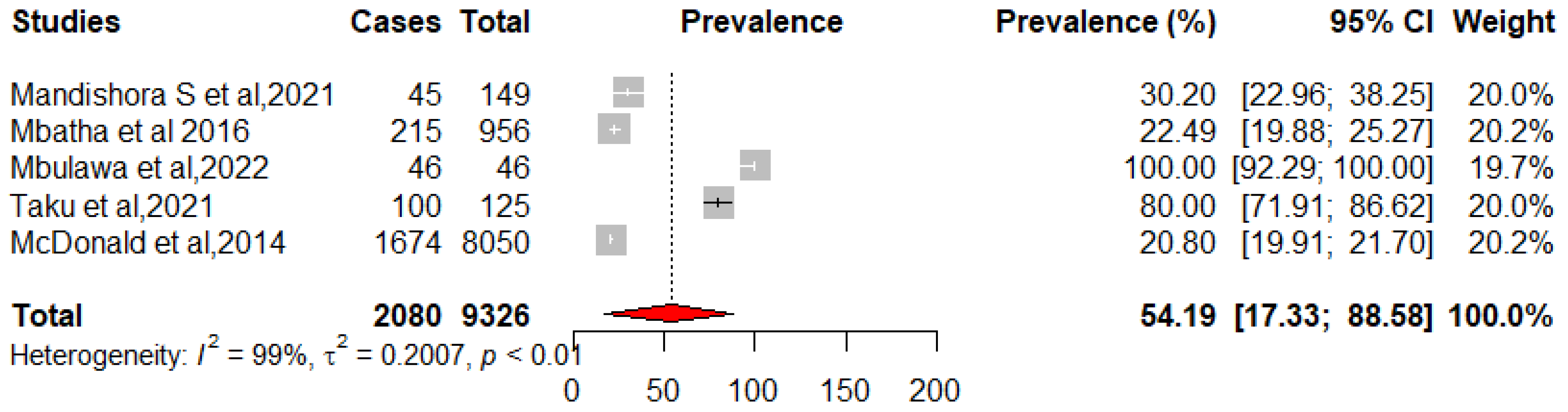
3.6. Prevalence of HPV Infection in HIV+ Women When Compared to HIV− Women
3.7. Cervical Lesions and HR-HPV Infection in the Included Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AIDS | Acquired immunodeficiency syndrome |
| CC | Cervical Cancer |
| CIRCB | “Chantal BIYA” International Reference Centre for research on HIV/AIDS prevention and management |
| HIV | Human Immunodeficiency Virus |
| HPV | human papilloma virus |
| HR-HPV | high risk oncogenic Human Immunodeficiency Virus |
| HSIL | high-grade intraepithelial lesion |
| ICC | Invasive Cervical Cancer |
| LR-HPV | Low Risk non-Human Papilloma Virus |
| LSIL | low-grade intraepithelial lesion |
| PLHIV | People Living with HIV |
| RT-PCR | Real-Time Polymerase Chain Reaction |
| UNSD | United Nations Statistic Division |
References
- Hoory, T.; Monie, A.; Gravitt, P.; Wu, T.C. Molecular epidemiology of human papillomavirus. J. Formos. Med. Assoc. Taiwan Yi Zhi. Mars. 2008, 107, 198–217. [Google Scholar] [CrossRef] [Green Version]
- Hildesheim, A.; Schiffman, M.; Bromley, C.; Wacholder, S.; Herrero, R.; Rodriguez, A.C.; Bratti, M.C.; Sherman, M.E.; Scarpidis, U.; Lin, Q.-Q.; et al. Human Papillomavirus Type 16 Variants and Risk of Cervical Cancer. J. Natl. Cancer Inst. 2001, 93, 315–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banura, C.; Franceschi, S.; van Doorn, L.J.; Arslan, A. Infection with human papillomavirus and HIV among young women in Kampala, Uganda. J. Infect. Dis. 2008, 197, 555. [Google Scholar] [CrossRef] [PubMed]
- Shope, R.E.; Hurst, E.W. Infectious Papillomatosis of Rabbits: With a Note on the Histopathology. J. Exp. Med. 1933, 58, 607–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- zur Hausen, H. Papillomaviruses causing cancer: Evasion from host-cell control in early events in carcinogenesis. J. Natl. Cancer Inst. 2000, 92, 690–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egawa, N.; Egawa, K.; Griffin, H.; Doorbar, J. Human Papillomaviruses; Epithelial Tropisms, and the Development of Neoplasia. Viruses 2015, 7, 3863–3890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beachler, D.C.; Weber, K.M.; Margolick, J.B.; Strickler, H.D. Risk factors for oral HPV infection among a high prevalence population of HIV-positive and at-risk HIV-negative adults. Cancer Epidemiol. Biomark. Prev. 2012, 21, 122. [Google Scholar] [CrossRef] [Green Version]
- Badial, R.M.; Dias, M.C.; Stuqui, B.; Melli, P.P.D.S. Detection and genotyping of human papillomavirus (HPV) in HIV-infected women and its relationship with HPV/HIV co-infection. Medicine 2018, 97, e9545. [Google Scholar] [CrossRef]
- Bansal, D.; Elmi, A.A.; Skariah, S.; Haddad, P.; Abu-Raddad, L.J.; Al Hamadi, A.H.; Mohamed-Nady, N.; Affifi, N.M.; Ghedira, R.; Hassen, E.; et al. Molecular epidemiology and genotype distribution of Human Papillomavirus (HPV) among Arab women in the State of Qatar. J. Transl. Med. 2014, 12, 300. [Google Scholar] [CrossRef] [Green Version]
- Barrett, T.J.; Silbar, J.D.; McGinley, J.P. Genital warts—A venereal disease. J. Am. Med. Assoc. 1954, 154, 333–334. [Google Scholar] [CrossRef]
- Bogale, A.L.; Belay, N.B.; Medhin, G.; Ali, J.H. Molecular epidemiology of human papillomavirus among HIV infected women in developing countries: Systematic review and meta-analysis. Virol. J. 2020, 17, 179. [Google Scholar] [CrossRef] [PubMed]
- Clifford, G.M.; Gonçalves, M.A.G.; Franceschi, S.; HPV and HIV Study Group. Human papillomavirus types among women infected with HIV: A meta-analysis. AIDS 2006, 20, 2337–2344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akarolo-Anthony, S.N.; Al-Mujtaba, M.; Famooto, O.A.; Dareng, O.E.; Olaniyan, O.B.; Offiong, R.; Wheeler, C.M.; A Adebamowo, C. HIV associated high-risk HPV infection among Nigerian women. BMC Infect. Dis. 2013, 13, 521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilboudo, M.; Zohoncon, T.M.; Traore, E.M.A.; Traore, I.M.A.; Kande, A.; Djigma, F.W.; Obiri-Yeboah, D.; Gyebre, Y.M.C.; Simpore, J.; Maïmouna, I.; et al. Characterization of High-risk Oncogenic Human Papillomavirus Genotypes in Histologically Confirmed Ear, Nose and Throat (Ent) Cancers in Burkina Faso. Asian Pac. J. Cancer Prev. APJCP 2019, 20, 3429–3435. [Google Scholar] [PubMed]
- Atashili, J.; Adimora, A.A.; Ndumbe, P.M.; Ikomey, G.M.; Rinas, A.C.; Myers, E.; Joseph, E.; Smith, J.S.; Miller, W.C. High prevalence of cervical squamous intraepithelial lesions in women on antiretroviral therapy in Cameroon: Is targeted screening feasible? Cancer Epidemiol. 2012, 36, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Bergström, R.; Sparén, P.; Adami, H.O. Trends in cancer of the cervix uteri in Sweden following cytological screening. Br. J. Cancer 1999, 81, 159–166. [Google Scholar] [CrossRef]
- Adam, Y.; van Gelderen, C.J.; de Bruyn, G.; McIntyre, J.A.; Turton, D.A.; Martinson, N.A. Predictors of persistent cytologic abnormalities after treatment of cervical intraepithelial neoplasia in Soweto, South Africa: A cohort study in a HIV high prevalence population. BMC Cancer 2008, 8, 211. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.Y.; Tiggelaar, S.M.; Sahasrabuddhe, V.V.; Smith, J.S.; Jiang, C.Q.; Mei, R.B.; Wang, X.G.; Li, Z.A.; Qiao, Y.L. HPV Prevalence and Cervical Intraepithelial Neoplasia among HIV-infected Women in Yunnan Province, China: A Pilot Study. Asian Pac. J. Cancer Prev. APJCP 2012, 13, 91–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berraho, M.; Amarti-Riffi, A.; El-Mzibri, M.; Bezad, R.; Benjaafar, N.; Benideer, A.; Matar, N.; Qmichou, Z.; Abda, N.; Attaleb, M.; et al. HPV and cofactors for invasive cervical cancer in Morocco: A multicentre case-control study. BMC Cancer 2017, 17, 435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catarino, R.; Vassilakos, P.; Tebeu, P.M.; Schäfer, S.; Bongoe, A.; Petignat, P. Risk factors associated with human papillomavirus prevalence and cervical neoplasia among Cameroonian women. Cancer Epidemiol. 2016, 40, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Ali, K.E.; Mohammed, I.A.; Difabachew, M.N.; Demeke, D.S.; Haile, T.; Hove, R.-J.T.; Kumssa, T.H.; Woldu, Z.L.; Haile, E.L.; Tullu, K.D. Burden and genotype distribution of high-risk Human Papillomavirus infection and cervical cytology abnormalities at selected obstetrics and gynecology clinics of Addis Ababa, Ethiopia. BMC Cancer 2019, 19, 768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beyazit, F.; Sılan, F.; Gencer, M.; Aydin, B.; Paksoy, B.; Unsal, M.A.; Ozdemir, O. The prevelance of human papillomavirus (HPV) genotypes detected by PCR in women with normal and abnormal cervico-vaginal cytology. Ginekol. Pol. 2018, 89, 62–67. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hariri, S.; Unger, E.R.; Sternberg, M.; Dunne, E.F.; Swan, D.; Patel, S.; Markowitz, L.E. Prevalence of genital human papillomavirus among females in the United States, the National Health and Nutrition Examination Survey, 2003–2006. J. Infect. Dis. 2011, 204, 566–573. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veroniki, A.A.; Jackson, D.; Viechtbauer, W.; Bender, R.; Bowden, J.; Knapp, G.; Kuss, O.; Higgins, J.P.; Langan, D.; Salanti, G. Methods to estimate the between-study variance and its uncertainty in meta-analysis. Res. Synth. Methods 2016, 7, 55–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mbulawa, Z.Z.A.; Phohlo, K.; Garcia-Jardon, M.; Williamson, A.-L.; Businge, C.B. High human papillomavirus (HPV)-35 prevalence among South African women with cervical intraepithelial neoplasia warrants attention. PLoS ONE 2022, 17, e0264498. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chikandiwa, A.; Chimoyi, L.; Pisa, P.T.; Chersich, M.F.; Muller, E.E.; Michelow, P.; Mayaud, P.; Delany-Moretlwe, S. Prevalence of anogenital HPV infection, related disease and risk factors among HIV-infected men in inner-city Johannesburg, South Africa: Baseline findings from a cohort study. BMC Public Health 2017, 17, 425. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. European Environment Agency. 2020. Available online: https://www.eea.europa.eu/data-and-maps/indicators/oxygen-consuming-substances-in-rivers/r-development-core-team-2006 (accessed on 14 May 2022).
- De Vuyst, H.; Ndirangu, G.; Moodley, M.; Tenet, V.; Estambale, B.; Meijer, C.J.; Snijders, P.J.; Clifford, G.; Franceschi, S. Prevalence of human papillomavirus in women with invasive cervical carcinoma by HIV status in Kenya and South Africa. Int. J. Cancer 2012, 131, 949–955. [Google Scholar] [CrossRef] [Green Version]
- Safaeian, M.; Kiddugavu, M.; Gravitt, P.E.; Gange, S.J.; Ssekasanvu, J.; Murokora, D.; Sklar, M.; Serwadda, D.; Wawer, M.J.; Shah, K.V.; et al. Determinants of incidence and clearance of high-risk HPV infections in rural Rakai, Uganda. Cancer Epidemiol. Biomark. Prev. 2008, 17, 1300–1307. [Google Scholar] [CrossRef] [Green Version]
- Kumakech, E.; Berggren, V.; Wabinga, H.; Lillsunde-Larsson, G.; Helenius, G.; Kaliff, M.; Karlsson, M.; Kirimunda, S.; Musubika, C.; Andersson, S. Significantly Reduced Genoprevalence of Vaccine-Type HPV-16/18 Infections among Vaccinated Compared to Non-Vaccinated Young Women 5.5 Years after a Bivalent HPV-16/18 Vaccine (Cervarix®) Pilot Project in Uganda. PLoS ONE 2016, 11, e0160099. [Google Scholar]
- Veldhuijzen, N.J.; Braunstein, S.L.; Vyankandondera, J.; Ingabire, C.; Ntirushwa, J.; Kestelyn, E.; Tuijn, C.; Wit, F.W.; Umutoni, A.; Uwineza, M.; et al. The epidemiology of human papillomavirus infection in HIV-positive and HIV-negative high-risk women in Kigali, Rwanda. BMC Infect. Dis. 2011, 11, 333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouassa, R.-S.M.; Nodjikouambaye, Z.A.; Sadjoli, D.; Adawaye, C.; Péré, H.; Veyer, D.; Matta, M.; Robin, L.; Tonen-Wolyec, S.; Moussa, A.M.; et al. High prevalence of cervical high-risk human papillomavirus infection mostly covered by Gardasil-9 prophylactic vaccine in adult women living in N’Djamena, Chad. PLoS ONE 2019, 14, e0217486. [Google Scholar]
- Ferré, V.M.; Gbeasor-Komlanvi, A.F.; Collin, G.; Dagnra, A.C.; Le Hingrat, Q.; Jaquet, A.; Salou, M.; Descamps, D.; Charpentier, C.; Ekouevi, D.K. Prevalence of Human Papillomavirus, Human Immunodeficiency Virus, and Other Sexually Transmitted Infections among Men Who Have Sex with Men in Togo: A National Cross-sectional Survey. Clin. Infect. Dis. 2019, 69, 1019–1026. [Google Scholar] [PubMed]
- Kuassi-Kpede, A.P.; Dolou, E.; Zohoncon, T.M.; Traore, I.M.A.; Katawa, G.; Ouedraogo, R.A.; Traore, E.M.; Bado, P.; Ouedraogo, T.C.; Djigma, F.W.; et al. Molecular characterization of high-risk human papillomavirus (HR-HPV) in women in Lomé, Togo. BMC Infect. Dis. 2021, 21, 278. [Google Scholar]
- Nyasenu, Y.T.; Gbeasor-Komlanvi, F.A.; Ehlan, A.; Issa, S.A.-R.; Dossim, S.; Kolou, M.; Yambiyo, B.M.; Prince-David, M.; Salou, M.; Ekouevi, D.K.; et al. Prevalence and distribution of Human Papillomavirus (HPV) genotypes among HIV infected women in Lomé, Togo. PLoS ONE 2019, 14, e0212516. [Google Scholar]
- Katundu, K.; Bateman, A.C.; Pfaendler, K.S.; Mwanahamuntu, M.H.; Kapambwe, S.; Vermund, S.H.; Sahasrabuddhe, V.V.; Msadabwe, S.C.; Stringer, J.S.A.; Parham, G.P.; et al. The Effect of Cryotherapy on Human Papillomavirus Clearance among HIV-positive Women in Lusaka, Zambia. J. Low Genit. Tract. Dis. 2015, 19, 301–306. [Google Scholar] [CrossRef] [Green Version]
- Mandishora, R.S.D.; Rounge, T.B.; Fitzpatrick, M.; Christiansen, I.K.; Ambur, O.H.; Lagström, S.; Stray-Pedersen, B.; Tommasino, M.; Palefsky, J.; Chirenje, Z.M. Self-collected and clinician-collected anal swabs show modest agreement for HPV genotyping. PLoS ONE 2021, 16, e0250426. [Google Scholar]
- Kuguyo, O.; Mandishora, R.S.D.; Thomford, N.E.; Makunike-Mutasa, R.; Nhachi, C.F.B.; Matimba, A.; Dandara, C. High-risk HPV genotypes in Zimbabwean women with cervical cancer: Comparative analyses between HIV-negative and HIV-positive women. PLoS ONE 2021, 16, e0257324. [Google Scholar]
- Fitzpatrick, M.B.; Mandishora, R.S.D.; Katzenstein, D.A.; McCarty, K.; Weber, J.; Sahoo, M.K.; Manasa, J.; Chirenje, Z.M.; Pinsky, B.A. hrHPV prevalence and type distribution in rural Zimbabwe: A community-based self-collection study using near-point-of-care GeneXpert HPV testing. Int. J. Infect. Dis. 2019, 82, 21. [Google Scholar] [CrossRef] [Green Version]
- Mudini, W.M.C.; Palefsky, J.M.M.; Hale, M.J.M.C.; Chirenje, M.Z.M.; Makunike-Mutasa, R.M.C.; Mutisi, F.H.; Murahwa, A.H.; Mario, A. Human Papillomavirus Genotypes in Invasive Cervical Carcinoma in HIV Seropositive and Seronegative Women in Zimbabwe. J. Acquir. Immune Defic. Syndr. 2018, 79, e1–e6. [Google Scholar] [CrossRef]
- Kelly, H.; Weiss, H.A.; Benavente, Y.; de Sanjose, S.; Mayaud, P.; ART and HPV Review Group. Association of antiretroviral therapy with high-risk human papillomavirus, cervical intraepithelial neoplasia, and invasive cervical cancer in women living with HIV: A systematic review and meta-analysis. Lancet HIV 2018, 5, e45–e58. [Google Scholar] [PubMed] [Green Version]
- Segondy, M.; Kelly, H.; Magooa, M.P.; Djigma, F.; Ngou, J.; Gilham, C.; Omar, T.; Goumbri-Lompo, O.; Michelow, P.; Doutre, S.; et al. Performance of careHPV for detecting high-grade cervical intraepithelial neoplasia among women living with HIV-1 in Burkina Faso and South Africa: HARP study. Br. J. Cancer 2016, 115, 425–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mbatha, J.N.; Taylor, M.; Kleppa, E.; Lillebo, K.; Galapaththi-Arachchige, H.N.; Singh, D.; Kjetland, E.F.; Baay, M.F.D.; Mkhize-Kwitshana, Z.L. High-risk human papillomavirus types in HIV-infected and HIV-uninfected young women in KwaZulu-Natal, South Africa: Implications for vaccination. Infect. Dis. 2017, 49, 601–608. [Google Scholar]
- Mbulawa, Z.Z.A.; van Schalkwyk, C.; Hu, N.-C.; Meiring, T.L.; Barnabas, S.; Dabee, S.; Jaspan, H.; Kriek, J.-M.; Jaumdally, S.Z.; Muller, E.; et al. High human papillomavirus (HPV) prevalence in South African adolescents and young women encourages expanded HPV vaccination campaigns. PLoS ONE 2018, 13, e0190166. [Google Scholar] [CrossRef] [PubMed]
- Firnhaber, C.; Van Le, H.; Pettifor, A.; Schulze, D.; Michelow, P.; Sanne, I.M.; Lewis, D.A.; Williamson, A.-L.; Allan, B.; Williams, S.; et al. Association between cervical dysplasia and human papillomavirus in HIV seropositive women from Johannesburg South Africa. Cancer Causes Control 2010, 21, 433–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adler, D.H.; Wallace, M.; Bennie, T.; Mrubata, M.; Abar, B.; Meiring, T.L.; Williamson, A.L.; Bekker, L.G. Cervical Dysplasia and High-Risk Human Papillomavirus Infections among HIV-Infected and HIV-Uninfected Adolescent Females in South Africa. Infect. Dis. Obstet. Gynecol. 2014, 2014, 498048. [Google Scholar] [CrossRef] [Green Version]
- Taku, O.; Mbulawa, Z.Z.A.; Phohlo, K.; Garcia-Jardon, M.; Businge, C.B.; Williamson, A.L. Distribution of Human Papillomavirus (HPV) Genotypes in HIV-Negative and HIV-Positive Women with Cervical Intraepithelial Lesions in the Eastern Cape Province, South Africa. Viruses 2021, 13, 280. [Google Scholar] [CrossRef]
- McDonald, A.C.; Tergas, A.I.; Kuhn, L.; Denny, L.; Wright, T.C. Distribution of Human Papillomavirus Genotypes among HIV-Positive and HIV-Negative Women in Cape Town, South Africa. Front. Oncol. 2014, 4, 48. [Google Scholar] [CrossRef] [Green Version]
- Muller, E.E.; Chirwa, T.F.; Lewis, D.A. Human papillomavirus infection in heterosexual South African men attending sexual health services: Associations between HPV and HIV serostatus. Sex. Transm. Infect. 2010, 86, 175. [Google Scholar] [CrossRef]
- Moodley, J.R.; Hoffman, M.; Carrara, H.; Allan, B.R.; Cooper, D.D.; Rosenberg, L.; E Denny, L.; Shapiro, S.; Williamson, A.-L. HIV and pre-neoplastic and neoplastic lesions of the cervix in South Africa: A case-control study. BMC Cancer 2006, 6, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Kelly, H.A. The epidemiology of Human Papillomavirus (HPV) Infection and Epigenetic Factors Associated with the Development of Cervical Cancer Precursor Lesions in Women Living with HIV in Africa. Ph.D. Thesis, London School of Hygiene & Tropical Medicine, London, UK, 2017. [Google Scholar] [CrossRef]
- Chikandiwa, A.; Faust, H.; Chersich, M.F.; Mayaud, P.; Dillner, J.; Delany-Moretlwe, S. Human Papillomavirus Seroprevalence and Seroconversion among Men Living with HIV: Cohort Study in South Africa. J. Acquir. Immune Defic. Syndr. 2020, 84, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Lamoril, J.; Bogard, M.; Ameziane, N.; Deybach, J.C.; Bouizegarène, P. Biologie moléculaire et microbiologie clinique en 2007. Immuno Anal. Biol. Spec. 2007, 22, 73–94. [Google Scholar]
- Gimeno-Gracia, M.; Antela, A. New horizons in the pharmaceutical care of HIV patients on long-term antiretroviral treatment. Farm. Hosp. Órgano Ofical Expresión Científica Soc. Española Farm. Hosp. 2021, 45, 287–288. [Google Scholar]
- de Mattos, A.T.; de Freitas, L.B.; Lima, B.M.C.; Miranda, A.E.; Spano, L.C. Diversity and uncommon HPV types in HIV seropositive and seronegative women attending an STI clinic. Braz. J. Microbiol. 2011, 42, 786–793. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, S.A.; Mullen, P.D.; Lopez, D.M.; Savas, L.S.; Fernandez, M.E. Factors associated with adolescent HPV vaccination in the US: A systematic review of reviews and multilevel framework to inform intervention development. Prev. Med. 2019, 131, 105968. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; MacLeod, M.A.; Abramovits, W. GARDASIL 9 (Human Papillomavirus 9-Valent Vaccine, Recombinant). Skinmed 2016, 14, 33–37. [Google Scholar] [PubMed]
- Sosso, S.M.; Tchouaket, M.C.T.; Fokam, J.; Simo, R.K.; Torimiro, J.; Tiga, A.; Lobe, E.E.; Ambada, G.; Nange, A.; Semengue, E.N.J.; et al. Human immunodeficiency virus is a driven factor of human papilloma virus among women: Evidence from a cross-sectional analysis in Yaoundé, Cameroon. Virol. J. 2020, 17, 69. [Google Scholar] [CrossRef] [PubMed]
- Clifford, G.M.; Tully, S.; Franceschi, S. Carcinogenicity of Human Papillomavirus (HPV) Types in HIV-Positive Women: A Meta-Analysis from HPV Infection to Cervical Cancer. Clin. Infect. Dis. 2017, 64, 1228–1235. [Google Scholar] [CrossRef]
- Black, E.; Richmond, R. Prevention of Cervical Cancer in Sub-Saharan Africa: The Advantages and Challenges of HPV Vaccination. Vaccines 2018, 6, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eakin, C.; Ekollo, R.; Nembulefack, D.; Halle-Ekane, G.; Tangui, G.; Brady, R.; Bhattarai, B.; Orock, G.E.; Greenspan, D. Cervical Cancer Screening Beliefs and Prevalence of LSIL/HSIL Among a University-Based Population in Cameroon. J. Low Genit. Tract. Dis. 2018, 22, 274–279. [Google Scholar] [CrossRef] [PubMed]
- da Silva, L.; Miranda, A.; Batalha, R.; Ferreira, L. High-risk human papillomavirus and cervical lesions among women living with HIV/AIDS in Brazilian Amazon, Brazil. Braz. J. Infect. Dis. 2015, 19, 557–562. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Molecular Genotyping Technique/(Targeted Genotypes) | Sample Size | Number with HR-HPV+ | Risk Factors Associated with HR-HPV Positivity | |
|---|---|---|---|---|---|
| 1 | Banura et al., 2008 [3] | Test HPV Linear Array de Roche/(17-HPV) | 1275 | 762 | HIV infection, employment in the service sector, multiple sexual partners |
| 2 | Mbulawa et al., 2018 [27] | Genotyping Roche Linear Array HPV/(37-HPV) | 291 | 194 | STI; multiple sexual partners |
| 3 | De Vuyst et al., 2011 [31] | PCR-HPV by in-line reverse hybridization (14-HPV) | 274 | 235 | Multiple sexual partners and age |
| 4 | Safaeian et al., 2008 [32] | Test Roche-PCR line blot/(13-HPV) | 1079 | 264 | Age; HIV infection; single women, two or more partners in the past year. |
| 5 | Kumakech et al., 2016 [33] | Genotyping test HPV, CLART® HPV2/(35-HPV) | 401 | 70 | - |
| 6 | Veldhuijzen et al., 2011 [34] | Genotyping test HPV Linear Array/(37-HPV) | 800 | 487 | Hormonal contraceptives and age |
| 7 | Bouassa et al., 2019 [35] | Detection kit Anyplex II HPV28 (28-HPV) | 253 | 56 | Multiple sexual partners |
| 8 | Firnhaber et al., 2010 [36] | Roche Linear Array HPV/(37-HPV) | 1010 | 528 | - |
| 9 | Ferré et al., 2019 [37] | Detection kit Anyplex II HPV-28/(28-HPV) | 207 | 107 | - |
| 10 | Kuassi-Kpede et al., 2021 [38] | RT-PCR multiplex, Sacace Biotechnologies (14-HPV) | 240 | 207 | - |
| 11 | Nyasenu et al., 2019 [39] | Kit PCR Mix and Phire Hot Start II/(36-HPV) | 221 | 52 | HIV infection, age |
| 12 | Katundu et al., 2016 [40] | Linear Array genotyping assay (Roche)/(37-HPV) | 101 | 89 | - |
| 13 | Mandishora et al., 2021 [41] | Next generation sequencing | 300 | 97 | HIV infection |
| 14 | Fitzpatrick et al., 2019 [42] | Detection kit Anyplex II HPV HR/(14-HPV) | 643 | 111 | - |
| 15 | Mudini et al., 2019 [43] | MY09/MY11 PCR and hybridisation typing/(37-HPV) | 107 | 104 | - |
| 16 | Kelly et al., 2018 [44] | Genotyping INNO-LiPA HPV Extra/(37-HPV) | 604 | 809 | - |
| 17 | Segondy et al., 2016 [45] | Genotyping test INNO-LiPA HPV Extra (28-HPV) | 1052 | 422 | HIV infection, marriage, alcohol, age, tobacco |
| 18 | Mbatha et al., 2016 [46] | Roche Linear Array HPV genotyping test/(18-HPV) | 1223 | 482 | - |
| 19 | Mbulawa et al., 2018 [47] | Genotyping test Roche Linear Array/(37-HPV) | 459 | 371 | - |
| 20 | Chikandiwa et al., 2019 [29] | Roche Linear Array (RLA, Roche Diagnostics)/(37-HPV) | 304 | 104 | - |
| 21 | Kuguyo et al., 2021 [41] | Detection kit Anyplex ™ II HPV HR/(14-HPV) | 258 | 382 | - |
| 22 | Adler et al., 2014 [49] | Test HPV Linear Array de Roche/(13-HPV) | 85 | 64 | - |
| 23 | Taku et al., 2021 [50] | Direct flow HPV kit/(36-HPV) | 193 | 300 | HIV infection |
| 24 | McDonald et al., 2014 [51] | Hybrid capture DNA test 2 (HC2)/(13-HPV) | 9421 | 1994 | - |
| 25 | Muller et al., 2016 [52] | Roche HPV Linear Array (37-HPV) | 200 | 107 | - |
| 26 | Moodley et al., 2006 [53] | Test Digene Hybrid Capture 2 (HC2) (13-HPV) | 109 | 38 | - |
| 27 | Kelly et al., 2017 [54] | Test INNO-LiPA HPV/(37-HPV) | 1238 | 467 | HIV infection |
| 28 | Chikandiwa et al., 2017 [55] | PCR system GeneAmp 9700 de Roche/(37-HPV) | 304 | 133 | HIV infection, multiple sexual partners, condoms |
| Total | 22,652 | 9036 |
| Author and Year | Country | HPV 16 | HPV 18 | HPV 31 | HPV 33 | HPV 35 | HPV 39 | HPV 45 | HPV 51 | HPV 52 | HPV 56 | HPV 58 | HPV 59 | HPV 61 | HPV 62 | HPV 66 | HPV 68 | Total | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Banura et al., 2008 [3] | Ouganda | 93 | 105 | 54 | 83 | 42 | 34 | 21 | 92 | 105 | 65 | 20 | 19 | - | - | - | 29 | 762 |
| 2 | Mbulawa et al., 2022 [27] | South Africa | 43 | 27 | 25 | - | - | - | - | 31 | - | - | 39 | - | - | - | 29 | - | 194 |
| 3 | De Vuyst et al., 2011 [31] | Kenya and South Africa | 118 | 37 | 3 | 6 | 17 | 2 | 33 | 1 | - | 5 | 7 | 1 | - | - | - | 5 | 235 |
| 4 | Safaeian et al., 2011 [32] | Ouganda | 32 | 18 | 10 | 17 | 13 | 18 | 23 | 37 | 22 | 20 | 14 | 22 | - | - | - | 18 | 264 |
| 5 | Kumakech et al., 2016 [33] | Ouganda | 0 | 4 | 7 | 1 | 5 | 5 | 2 | 13 | 19 | - | - | - | - | - | 14 | - | 70 |
| 6 | Veldhuijzen et al., 2011 [34] | Rwanda | 29 | 20 | 39 | 34 | 32 | 40 | 37 | 48 | 50 | 34 | 60 | 28 | - | - | - | 36 | 487 |
| 7 | Bouassa et al., 2019 [35] | Tchad | 5 | 4 | 6 | 1 | 6 | 3 | 5 | - | 5 | 6 | 7 | - | - | 4 | 4 | - | 56 |
| 8 | Ferré et al., 2019 [36] | Togo | 27 | - | 26 | - | 31 | - | - | - | - | - | - | 23 | - | - | - | - | 107 |
| 9 | Kuassi-Kpede et al., 2021 [37] | Togo | 3 | 18 | 24 | 3 | 22 | 7 | 10 | 25 | 24 | 29 | 12 | 7 | - | - | 12 | 11 | 207 |
| 10 | Nyasenu et al., 2019 [38] | Togo | 3 | 20 | - | - | - | - | - | - | - | - | - | - | - | 11 | - | 18 | 52 |
| 11 | Katundu et al., 2016 [39] | Zambia | 24 | 24 | - | - | - | - | 3 | 18 | - | - | 20 | - | - | - | - | - | 89 |
| 12 | Mandishora et al., 2021 [40] | Zimbabwe | 20 | 7 | - | - | - | 7 | 10 | - | 18 | - | 14 | - | - | 9 | 5 | 7 | 97 |
| 13 | Kuguyo et al., 2021 [41] | Zimbabwe | 123 | 65 | 17 | 25 | 68 | 10 | 14 | 11 | 9 | 6 | 23 | 3 | - | - | 1 | 7 | 382 |
| 14 | Fitzpatrick et al., 2019 [42] | Zimbabwe | 12 | 12 | 5 | 6 | 12 | 2 | 10 | 6 | 12 | 6 | 10 | 4 | - | - | 3 | 11 | 111 |
| 15 | Mudini et al., 2019 [43] | Zimbabwe | 59 | 20 | - | 7 | - | - | 4 | - | - | 9 | 5 | - | - | - | - | - | 104 |
| 16 | Kelly et al., 2018 [44] | South Africa | 115 | 89 | 61 | 48 | 99 | 48 | 47 | 146 | 58 | 54 | 11 | - | - | - | 33 | 809 | |
| 17 | Segondy et al., 2016 [45] | Burkina Faso and South Africa | 41 | 33 | 49 | 16 | 36 | 21 | 20 | 23 | 83 | 25 | 22 | 3 | - | - | 27 | 23 | 422 |
| 18 | Mbatha et al., 2016 [46] | South Africa | 99 | 56 | - | 47 | 50 | 15 | 34 | 58 | 32 | 42 | 15 | 31 | - | - | - | 3 | 482 |
| 19 | Mbulawa et al., 2018 [47] | South Africa | 133 | 44 | - | - | 67 | - | 44 | - | 37 | - | 46 | - | - | - | - | - | 371 |
| 20 | Chikandiwa et al., 2019 [29] | South Africa | 18 | 9 | 4 | 4 | 4 | 2 | 15 | 8 | 5 | 5 | 10 | 12 | - | - | - | 8 | 104 |
| 21 | Firnhaber et al., 2010 [48] | South Africa | 208 | - | - | 71 | - | - | - | - | - | 112 | - | 56 | - | - | 81 | - | 528 |
| 22 | Adler et al., 2014 [49] | South Africa | 10 | 7 | 1 | 1 | 6 | 2 | 9 | 6 | 6 | 2 | 2 | 2 | - | - | - | 10 | 64 |
| 23 | Taku et al., 2021 [50] | South Africa | 40 | 17 | 22 | 25 | 44 | 12 | 29 | 13 | 26 | 16 | 32 | - | - | - | 16 | 8 | 300 |
| 24 | McDonald et al., 2014 [51] | South Africa | 247 | 179 | 129 | 132 | 279 | 100 | 194 | 157 | 174 | 112 | 126 | 68 | - | - | - | 97 | 1994 |
| 25 | Muller et al., 2016 [52] | South Africa | 48 | 7 | 5 | - | 3 | - | 10 | 34 | - | - | - | - | - | - | - | - | 107 |
| 26 | Moodley et al., 2009 [53] | South Africa | 6 | 5 | - | - | 2 | 3 | 5 | - | - | - | 2 | - | 8 | - | 7 | - | 38 |
| 27 | Kelly et al., 2017 [54] | Burkina Faso and South Africa | 51 | 42 | 47 | 19 | 62 | 43 | 26 | - | 121 | - | 27 | 6 | - | - | - | 23 | 467 |
| 28 | Chikandiwa et al., 2017 [55] | South Africa | 19 | 10 | 3 | 6 | 15 | 6 | 12 | 13 | 8 | 7 | 10 | 13 | - | - | - | 11 | 133 |
| Total n (%) | 1626 18% | 879 9.7% | 537 5.9% | 552 6.1% | 915 10.1% | 380 4.2% | 617 6.8% | 594 6.6% | 902 9.9% | 559 6.2% | 577 6.4% | 309 3.4% | 8 0.1% | 24 0.3% | 199 2.2% | 358 3.9% | 9036 100% | ||
| Author Year | Sample Size | Sample Size of Cervical Vaginal Smear | Number with HR-HPV+ | Cervical Cancer | |
|---|---|---|---|---|---|
| 1 | Banura et al., 2008 [3] | 1275 | - | - | - |
| 2 | Mbulawa et al., 2018 [27] | 291 | - | - | - |
| 3 | De Vuyst et al., 2011 [31] | 274 | - | - | - |
| 4 | Safaeian et al., 2011 [32] | 1079 | - | - | - |
| 5 | Kumakech et al., 2016 [33] | 401 | - | - | - |
| 6 | Veldhuijzen et al., 2011 [34] | 800 | - | - | - |
| 7 | Bouassa et al., 2019 [35] | 253 | - | - | - |
| 8 | Ferré et al., 2019 [36] | 207 | - | - | - |
| 9 | Kuassi-Kpede et al., 2021 [37] | 240 | - | - | - |
| 10 | Nyasenu et al., 2019 [38] | 221 | - | - | |
| 11 | Katundu et al., 2016 [39] | 101 | - | - | - |
| 12 | Mandishora et al., 2021 [40] | 300 | - | - | - |
| 13 | Kuguyo et al., 2021 [41] | 258 | - | - | - |
| 14 | Fitzpatrick et al., 2019 [42] | 643 | 76 | 112 | Normal = 44 LSIL = 16 HSIL = 16 |
| 15 | Muduni et al., 2019 [43] | 107 | - | - | - |
| 16 | Kelly et al., 2018 [44] | 604 | - | - | - |
| 17 | Segondy et al., 2016 [45] | 1052 | 426 | 422 | Normal = 368 LSIL = 33 HSIL = 25 |
| 18 | Mbatha et al., 2016 [46] | 1223 | - | - | - |
| 19 | Mbulawa et al., 2018 [47] | 459 | 272 * | 371 * | 16 and 35 were the most dominant genotypes in HSIL * |
| 20 | Chikandiwa et al., 2019 [29] | 304 | - | - | - |
| 21 | Firnhaber et al., 2010 [48] | 1010 | 926 | 528 | Normal = 507 LSIL = 237 HSIL = 182 |
| 22 | Adler et al., 2014 [49] | 85 | 85 | 64 | Normal 69; LSIL 8; HSIL = 8 |
| 23 | Taku et al., 2021 [50] | 193 | 193 | 300 | Normal = 0 LSIL = 43 HSIL = 147 |
| 24 | McDonald et al., 2014 [51] | 9421 | 1848 * | 1994 * | 16 and 35 were the most dominant genotypes in HSIL * |
| 25 | Muller et al., 2016 [52] | 200 | - | - | - |
| 26 | Moodley et al., 2009 [53] | 109 | 109 | 38 | Normal = 20 LSIL = 40 HSIL = 49 |
| 27 | Kelly et al., 2017 [54] | 1238 | - | - | - |
| 28 | Chikandiwa et al., 2017 [55] | 304 | 298 | 133 | Normal = 0 LSIL = 137 (46) HSIL = 161 (87) |
| Total | 22,652 | 2113 | 1597 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tchouaket, M.C.T.; Ka’e, A.C.; Semengue, E.N.J.; Sosso, S.M.; Simo, R.K.; Yagai, B.; Nka, A.D.; Chenwi, C.A.; Abba, A.; Fainguem, N.; et al. Variability of High-Risk Human Papillomavirus and Associated Factors among Women in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. Pathogens 2023, 12, 1032. https://doi.org/10.3390/pathogens12081032
Tchouaket MCT, Ka’e AC, Semengue ENJ, Sosso SM, Simo RK, Yagai B, Nka AD, Chenwi CA, Abba A, Fainguem N, et al. Variability of High-Risk Human Papillomavirus and Associated Factors among Women in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. Pathogens. 2023; 12(8):1032. https://doi.org/10.3390/pathogens12081032
Chicago/Turabian StyleTchouaket, Michel Carlos Tommo, Aude Christelle Ka’e, Ezechiel Ngoufack Jagni Semengue, Samuel Martin Sosso, Rachel Kamgaing Simo, Bouba Yagai, Alex Durand Nka, Collins Ambe Chenwi, Aissatou Abba, Nadine Fainguem, and et al. 2023. "Variability of High-Risk Human Papillomavirus and Associated Factors among Women in Sub-Saharan Africa: A Systematic Review and Meta-Analysis" Pathogens 12, no. 8: 1032. https://doi.org/10.3390/pathogens12081032