



Clinical Spectrum and Outcomes of Cryptogenic Klebsiella pneumoniae Liver Abscess in the Americas: A Scoping Review

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
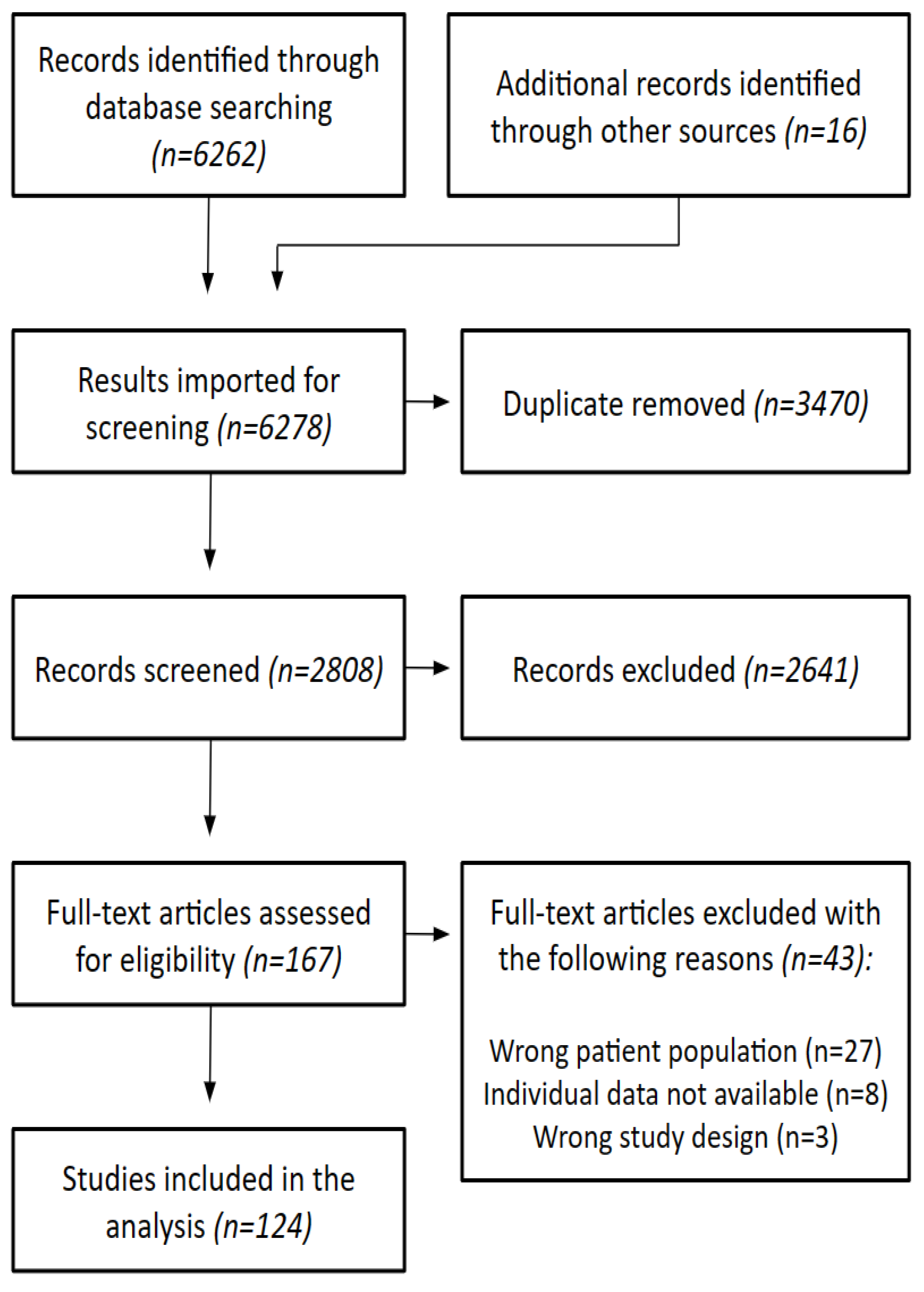
2.1. Study Eligibility and Search Strategy
2.2. Study Selection and Data Extraction
2.3. Data Synthesis and Statistical Analysis
2.4. Study Definitions
3. Results
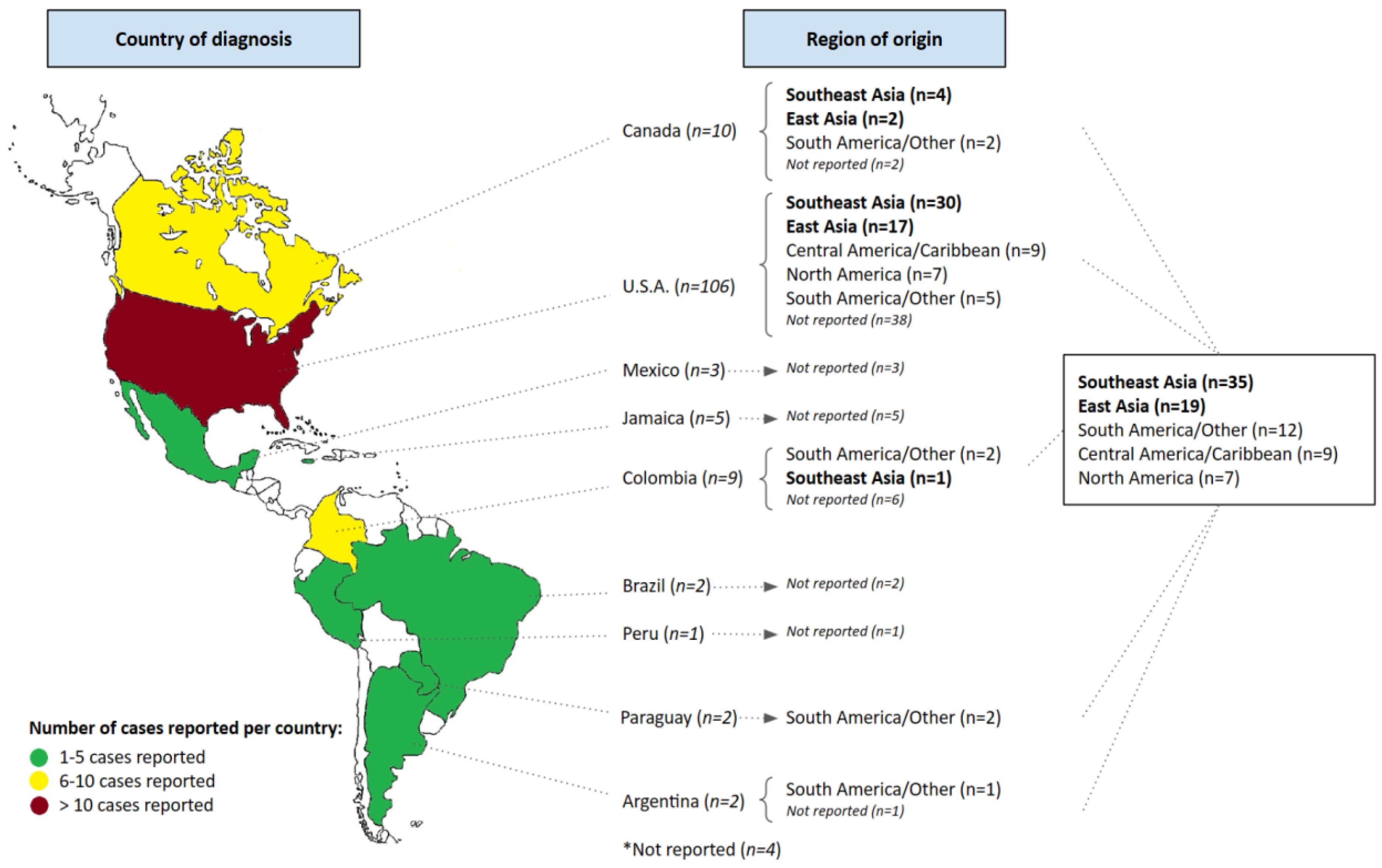
3.1. Study Characteristics
3.2. Population Characteristics
3.3. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Detailed Search Strategy
Appendix B. Articles Included in the Analysis
| Goldman | 1978 | Hepatic abscess and osteomyelitis from Klebsiella pneumoniae |
| Talcott | 1984 | A Vietnamese woman with chills and fever |
| Ridker | 1990 | False positive mononucleosis screening test results associated with Klebsiella hepatic abscess |
| Barton | 1991 | Diabetes mellitus and Klebsiella pneumoniae liver abscess in adults |
| Martinez | 1991 | Septic endophthalmitis associated with bacteremia and liver abscess caused by Klebsiella pneumoniae |
| Saccente | 1999 | Klebsiella pneumoniae Liver Abscess, Endophthalmitis, and Meningitis in a Man with Newly Recognized Diabetes Mellitus |
| Dharmarajan | 2000 | Pyogenic Liver Abscess: A Geriatric Problem |
| Harris | 2000 | Bacterial subretinal abscess: A case report and review of the literature |
| Roeder | 2001 | 29-Year-Old Man with Fever, Malaise, and Abdominal Pain |
| Solarte | 2001 | Endoftalmitis y septicemia por Klebsiella pneumoniae |
| Kim | 2003 | Klebsiella liver abscess |
| Lewis | 2004 | Klebsiella pneumoniae primary liver abscess in a newly diagnosed diabetic |
| Fang | 2005 | Liver abscess caused by magA+ Klebsiella pneumoniae in North America |
| Harris | 2005 | Two cases of Klebsiella pneumoniae primary liver abscess; an emerging clinical entity among diabetics |
| Lederman | 2005 | Pyogenic liver abscess with a focus on Klebsiella pneumoniae as a primary pathogen: An emerging disease with unique clinical characteristics |
| Pearl | 2005 | Hepatic abscesses |
| Golia | 2006 | Pyogenic liver abscess: Klebsiella as an emerging pathogen |
| Braiteh | 2007 | Cryptogenic invasive Klebsiella pneumoniae liver abscess syndrome |
| Connell | 2007 | Klebsiella pneumoniae endophthalmitis with associated hepatic abscess |
| Keynan | 2007 | Pyogenic liver abscess caused by hypermucoviscous Klebsiella pneumoniae |
| Nadasy | 2007 | Invasive Klebsiella pneumoniae syndrome in North America |
| Victor | 2007 | Endophthalmitis complicating Klebsiella pneumoniae liver abscess: An infrequently recognized complication |
| Dodson | 2009 | Klebsiella pneumoniae Endophthalmitis Secondary to Liver Abscess Presenting as Acute Iridocyclitis |
| Doud | 2009 | A k(2)A-positive Klebsiella pneumoniae causes liver and brain abscess in a Saint Kitt’s man |
| Frazee | 2009 | Invasive Infection with Hypermucoviscous Klebsiella pneumoniae: Multiple Cases Presenting to a Single Emergency Department in the United States |
| Segretin | 2009 | Comunicación Breve Endoftalmitis endógena por Klebsiella pneumoniae |
| Sharma | 2009 | Endogenous Klebsiella endophthalmitis in a Vietnamese immigrant |
| Rivero | 2010 | K2 Serotype Klebsiella pneumoniae causing a Liver Abscess Associated with Infective Endocarditis |
| Nazir | 2010 | Pyogenic liver abscess |
| Pepin | 2010 | Klebsiella pneumoniae bacteraemia in a region of Canada |
| Fierer | 2011 | Recurring Klebsiella pneumoniae Pyogenic Liver Abscess in a Resident of San Diego, California, Due to a K1 Strain Carrying the Virulence Plasmid |
| Pope | 2011 | Klebsiella pneumoniae liver abscess: An emerging problem in North America |
| Kashani | 2011 | Bilateral Klebsiella pneumoniae (K1 serotype) endogenous endophthalmitis as the presenting sign of disseminated infection |
| Pomakova | 2012 | Clinical and phenotypic differences between classic and hypervirulent Klebsiella pneumoniae: An emerging and under-recognized pathogenic variant |
| Vila | 2011 | Appearance of Klebsiella pneumoniae liver abscess syndrome in Argentina: Case report and review of molecular mechanisms of pathogenesis |
| Vu-Holbrook | 2012 | Overcoming the Rigors of Klebsiella pneumoniae |
| Abate | 2012 | Clinical and bacteriological characteristics of Klebsiella pneumoniae causing liver abscess with less frequently observed multi-locus sequences type, ST163, from Singapore and Missouri, US |
| Lai | 2012 | Multifocal Pneumonia Caused by Klebsiella pneumoniae Liver Abscess Syndrome |
| Persichino | 2012 | Klebsiella pneumoniae necrotizing fasciitis in a Latin American male |
| Carrillo-Esper | 2013 | Síndrome de absceso hepático secundario a Klebsiella pneumoniae hipermucoviscosa. Una entidad emergente |
| Carrillo-Esper | 2013 | Síndrome de absceso hepático secundario a Klebsiella pneumoniae hipermucoviscosa con involucro pulmonar |
| Cordero-Chen | 2013 | Absceso hepático asociado a absceso pulmonar y endoftalmitis |
| Kashani | 2013 | The emergence of Klebsiella pneumoniae endogenous endophthalmitis in the USA: basic and clinical advances |
| Lodhi | 2013 | Pyogenic liver abscesses: Manifestations and management of an evolving pathogen |
| Patel | 2013 | Pyogenic Liver Abscess, Bacteremia, and Meningitis with Hypermucoviscous Klebsiella pneumoniae: An Unusual Case Report in a Human T-Cell Lymphotropic Virus Positive Patient of Caribbean origin in the United States |
| Rios | 2013 | Genotyping Klebsiella pneumoniae isolated from hepatic abscesses in three patients from Bogota, Colombia |
| Sachdev | 2013 | Klebsiella pneumoniae K1 Liver Abscess and Septic Endophthalmitis in a U.S. Resident |
| Buppajarntham | 2014 | Tumor-like pyogenic liver abscess caused by Klebsiella pneumoniae in diabetes |
| Coutinho | 2014 | Community-acquired invasive liver abscess syndrome caused by a K1 serotype Klebsiella pneumoniae isolate in Brazil: A case report of hypervirulent ST23 |
| Kwon | 2014 | A Case of Klebsiella Liver Abscesses |
| Patel | 2014 | Hypervirulent Klebsiella pneumoniae |
| Saha | 2014 | Cryptogenic liver abscess in a diabetic patient |
| Neto | 2014 | Abscesso hepático por Klebsiella pneumoniae e suas complicações sistêmicas / Liver abscess by Klebsiella pneumoniae and its systemic complication |
| Sridhar | 2014 | Endophthalmitis caused by Klebsiella species |
| Williams | 2014 | Occult pyogenic liver abscess in an adolescent with type 2 diabetes |
| Perez | 2015 | ID Challenges in the ICU: Klebsiella liver abscess syndrome in the abscess of native hepatobiliary disease |
| Persichino | 2015 | Eight cases of invasive Klebsiella pneumoniae infection from a public teaching medical institution in the USA |
| Sierra Saldívar | 2015 | Absceso hepático a Klebsiella pneumoniae/KLEBSIELLA PNEUMONIAE hepatic abscess |
| Davies | 2016 | Concurrent Endophthalmitis and Orbital Cellulitis from Metastatic Klebsiella pneumoniae Liver Abscess |
| Bhattacharya | 2016 | Klebsiella pneumoniae Hepatic Abscess in a Woman from China |
| Dsouza | 2016 | Abscess, abscess everywhere! A case of metastatic klebsiella infection |
| Fazili | 2016 | Klebsiella pneumoniae Liver Abscess an Emerging Disease |
| Jaramillo-Aristizabal | 2016 | Endoftalmitis endógena asociada a absceso hepático por Klebsiella pneumoniae. Descripción de tres casos y revisión de la literatura |
| Gao | 2016 | A Case of the Unseen: Klebsiella pneumoniae Pyogenic Liver Abscess with Pneumonia and Septic Endophthalmitis in A Non-Asian Us Resident |
| Gupta | 2016 | “Air-raising”: An air-fluid level in the right subphrenic region |
| Woll | 2016 | Klebsiella pneumoniae liver abscess syndrome: Case presentation to a college student health clinic |
| Kazanji | 2016 | A case of hypermucoviscous Klebsiella pneumoniae liver abscess syndrome in an Iraqi male |
| Villegas | 2016 | Caso de absceso hepático bacteriano drenado a pleura y cavidad abdominal |
| Wells | 2016 | Klebsiella pneumoniae Liver Abscess and Metastatic Endophthalmitis |
| Williams | 2016 | Klebsiella Liver Abscess |
| Yucuma-Gutierrez | 2016 | Absceso hepático por Klebsiella pneumoniae asociado con bacteriemia y meningitis. Reporte de un caso |
| Al-Khazraji | 2016 | Invasive liver abscess syndrome in North America |
| Kamal | 2017 | Klebsiella pneumoniae Liver Abscess: A Case Report and Review of Literature |
| Sink | 2017 | Disparate Domains: Cryptogenic Invasive Klebsiella pneumoniae Liver Abscess Syndrome |
| Lo | 2017 | A sticky situation: Hypermucoviscous Klebsiella pneumoniae causing alternative pyogenic abscess |
| Oikonomou | 2017 | Klebsiella Pneumoniae Liver Abscess: A Case Series of Six Asian Patients |
| Ramos-Rossy | 2017 | An unexpected cause of sepsis: Always keep searching |
| Schifeling | 2017 | A new super-villain strikes under the cover of DKA |
| Iradukunda | 2018 | Unexpected source of fever: Liver abscess on point-of-care ultrasound |
| Maheswaranathan | 2018 | Identification and Management of the Hypervirulent Invasive Klebsiella pneumoniae Syndrome: A Unique and Distinct Clinical Entity |
| Alvarez Escalante | 2018 | Síndrome de invasión por Klebsiella multisensible. Reporte de un caso y revisión de la literatura/Invasion syndrome by multi-drug resistant Klebsiella. Case report and literature review |
| Peermohamed | 2018 | Hypervirulent (hypermucoviscous) Klebsiella pneumoniae causing pyogenic liver abscess |
| Chan | 2018 | Hypermucoviscous Klebsiella pneumoniae liver abscess requiring liver resection |
| Gupta | 2018 | Novel complication of an emerging disease: Invasive Klebsiella pneumoniae liver abscess syndrome as a cause of acute respiratory distress syndrome |
| Schmiedecke | 2018 | First Report of Cryptogenic Klebsiella pneumoniae Liver Abscess in Pregnancy |
| Bradley | 2019 | Metastatic Klebsiella pneumoniae Invasive Liver Abscess Syndrome in Denver, Colorado |
| Likhtshteyn | 2019 | Sneaky abscess-ion: A pyogenic liver abscess masquerading as the flu |
| McCarty | 2019 | A Rare Case of Klebsiella pneumoniae Liver Abscess with Subsequent Invasive Disease: 2377 |
| Merza | 2019 | Pleural Effusion Caused by Klebsiella Pyogenic Liver Abscess |
| Naseer | 2019 | Liver Abscess Complicated by Invasive Klebsiella Syndrome Resulting in Endophthalmitis |
| Nnaoma | 2019 | Pyogenic liver abscess in b-thalassemia: A case report |
| Criales Doria | 2019 | Liver Abscess Metastatic Syndrome Caused by Hypermucoviscous Klebsiella pneumoniae in a Canadian Patient of Vietnamese Origin |
| Pillsbury | 2019 | Sticky Business: A syndrome of mucoid bacterial spread |
| Schmiedecke | 2019 | Perinatal Pyogenic Liver Abscess: A Rare Entity and First Reported Case of Klebsiella pneumoniae |
| Ue | 2019 | A 53-Year-Old Haitian Male Presenting with a Liver Abscess |
| Young | 2019 | Invasive Liver Abscess Syndrome as a Consequence of Klebsiella Pneumoniae Urinary Tract Infection in A Nondiabetic American Caucasian Male: A Case Report |
| Echeverria | 2020 | Conservative Management of Klebsiella pneumoniae Liver Abscesses Mimicking Malignancy in Asian Man |
| Menjivar | 2020 | Klebsiella pneumoniae Liver Abscess: KLA, It’s Never Okay |
| Fan | 2020 | Concomitant Pyogenic Liver and Intraocular Abscesses in Klebsiella Endogenous Endophthalmitis: Case Report and Review of Literature |
| Raudales | 2020 | Klebsiella pneumoniae Primary Invasive Liver Abscess |
| Ahmad | 2020 | Think Outside the Box: Not All Vomiting Is Gastroenteritis |
| Torres | 2020 | Attack of the Klebsiella: A Case of Invasive Liver Abscess Syndrome with Multi-Organ Dissemination |
| Van | 2020 | A Case of Hypermucoviscous Klebsiella pneumoniae Pyogenic Liver Abscess |
| Walkty | 2020 | An 82-Year-Old Male with a Liver Abscess |
| Xie | 2020 | Klebsiella pneumoniae liver abscess associated with chronic ketamine abuse |
| Abdelrahman | 2021 | Encysted empyema: An uncommon complication of pyogenic liver abscess |
| Amoateng | 2021 | A Rare Case of Recurrent Klebsiella pneumoniae Liver Abscess |
| Arn | 2021 | Complicated Course of a Primary Klebsiella pneumoniae Liver Abscess Requiring Exploratory Laparotomy and Partial Hepatic Lobectomy |
| Brown | 2021 | Pyogenic Liver Abscess Presenting as Obstructive Jaundice from Klebsiella pneumoniae in Texas |
| Chaudhry | 2021 | Negative pressure pulmonary oedema due to rigors and chills associated with liver abscess |
| Eisenmenger | 2021 | ‘String Test’ for Hypermucoviscous Klebsiella pneumoniae |
| Ejikeme | 2021 | Hepatosplenic Abscess from Klebsiella pneumoniae in Poorly Controlled Diabetic |
| Ghobrial | 2021 | The great mimicker: An unusual presentation of Klebsiella pneumoniae in a middle-aged man |
| Limpattanachart | 2021 | Invasive Klebsiella pneumoniae Liver Abscess Syndrome Presenting as Right Calf Skin Abscess |
| Mohanty | 2021 | A Sticky Case of A Pyogenic Liver Abscess—Klebsiella pneumoniae |
| Morales-Morales | 2021 | Invasive liver abscess syndrome with septic pulmonary embolisms |
| Ochi | 2021 | Hypervirulent klebsiella pneumonia causing disseminated infection in immunocompetent host |
| Pentecost | 2021 | Pyogenic liver abscess and endogenous endophthalmitis secondary to Klebsiella pneumoniae |
| Sulaiman | 2021 | A rare case of klebsiella liver abscess |
| Vongsavath | 2021 | Klebsiella pneumonia Liver Abscess in a Previously Healthy Thai Male |
| Zegarra Piérola | 2021 | Absceso hepático, bacteriemia y meningoencefalitis por Klebsiella pneumoniae hipervirulenta en el curso de infección por SARS-CoV2. Reporte de caso |
| Fernández-Vega González | 2022 | Klebsiella pneumoniae endogenous endophthalmitis secondary to liver abscess syndrome |
| Doshi | 2022 | Disseminated hypervirulent Klebsiella pneumoniae causing endophthalmitis, and lung and liver abscesses |
References
- Prokesch, B.C.; TeKippe, M.; Kim, J.; Raj, P.; TeKippe, E.M.; Greenberg, D.E. Primary osteomyelitis caused by hypervirulent Klebsiella pneumoniae. Lancet Infect. Dis. 2016, 16, e190–e195. [Google Scholar] [CrossRef]
- Chen, D.; Zhang, Y.; Wu, J.; Li, J.; Chen, H.; Zhang, X.; Hu, X.; Chen, F.; Yu, R. Analysis of hypervirulent Klebsiella pneumoniae and classic Klebsiella pneumoniae infections in a Chinese hospital. J. Appl. Microbiol. 2022, 132, 3883–3890. [Google Scholar] [CrossRef] [PubMed]
- Russo, T.A.; Marr, C.M. Hypervirulent Klebsiella pneumoniae. Clin. Microbiol. Rev. 2019, 32, e00001-19. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-R.; Lee, J.H.; Park, K.S.; Jeon, J.H.; Kim, Y.B.; Cha, C.-J.; Jeong, B.C.; Lee, S.H. Antimicrobial Resistance of Hypervirulent Klebsiella pneumoniae: Epidemiology, Hypervirulence-Associated Determinants, and Resistance Mechanisms. Front. Cell Infect. Microbiol. 2017, 7, 483. [Google Scholar] [CrossRef]
- Melot, B.; Brisse, S.; Breurec, S.; Passet, V.; Malpote, E.; Lamaury, I.; Thiery, G.; Hoen, B. Community-acquired meningitis caused by a CG86 hypervirulent Klebsiella pneumoniae strain: First case report in the Caribbean. BMC Infect. Dis. 2016, 16, 736. [Google Scholar] [CrossRef]
- Rossi, B.; Gasperini, M.L.; Leflon-Guibout, V.; Gioanni, A.; de Lastours, V.; Rossi, G.; Dokmak, S.; Ronot, M.; Roux, O.; Nicolas-Chanoine, M.-H.; et al. HypervirulentKlebsiella pneumoniae in Cryptogenic Liver Abscesses, Paris, France. Emerg Infect. Dis. 2018, 24, 221–229. [Google Scholar] [CrossRef]
- Liu, Y.-C. Klebsiella pneumoniae Liver Abscess Associated With Septic Endophthalmitis. Arch. Int. Med. 1976, 146, 1913. [Google Scholar] [CrossRef]
- Wang, J.; Yan, Y.; Xue, X.; Wang, K.; Shen, D. Comparison of pyogenic liver abscesses caused by hypermucoviscous Klebsiella pneumoniae and non-Klebsiella pneumoniae pathogens in Beijing: A retrospective analysis. J. Int. Med. Res. 2013, 41, 1088–1097. [Google Scholar] [CrossRef]
- Ontanilla, G.; Herrera, J.M.; Alcívar, J.M.; Martín-Gutiérrez, G.; Márquez, C.; Márquez, J.L. Liver abscess due to Klebsiella pneumoniae and its relation to colon lesions. Rev. Esp. Enferm. Dig. Organo Of. Soc. Esp. Patol. Dig. 2015, 107, 51–52. [Google Scholar]
- Choby, J.E.; Howard-Anderson, J.; Weiss, D.S. Hypervirulent Klebsiella pneumoniae—Clinical and molecular perspectives. J. Int. Med. 2019, 287, 283–300. [Google Scholar] [CrossRef] [PubMed]
- Shon, A.S.; Russo, T.A. Hypervirulent Klebsiella pneumoniae: The next superbug? Future Microbiol. 2012, 7, 669–671. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.; Wong, E.; Liu, C.; Wong, M.; Li, K. Clinical features and prognostic factors of Klebsiella endophthalmitis—10-year experience in an endemic region. Eye 2017, 31, 1569–1575. [Google Scholar] [CrossRef] [PubMed]
- Vila, A. Appearance of Klebsiella Pneumoniae Liver Abscess Syndrome in Argentina: Case Report and Review of Molecular Mechanisms of Pathogenesis. Open Microbiol. J. 2011, 5, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Struve, C.; Roe, C.C.; Stegger, M.; Stahlhut, S.G.; Hansen, D.S.; Engelthaler, D.M.; Andersen, P.S.; Driebe, E.M.; Keim, P.; Krogfelt, K.A. Mapping the Evolution of Hypervirulent Klebsiella pneumoniae. mBio 2015, 6, e00630-15. [Google Scholar] [CrossRef]
- Compain, F.; Babosan, A.; Brisse, S.; Genel, N.; Audo, J.; Ailloud, F.; Kassis-Chikhani, N.; Arlet, G.; Decré, D. Multiplex PCR for Detection of Seven Virulence Factors and K1/K2 Capsular Serotypes of Klebsiella pneumoniae. J. Clin. Microbiol. 2014, 52, 4377–4380. [Google Scholar] [CrossRef] [PubMed]
- Dai, P.; Hu, D. The making of hypervirulent Klebsiella pneumoniae. J. Clin. Lab. Anal. 2022, 36, e24743. [Google Scholar] [CrossRef]
- Walker, K.A.; Miller, V.L. The intersection of capsule gene expression, hypermucoviscosity and hypervirulence in Klebsiella pneumoniae. Curr. Opin. Microbiol. 2020, 54, 95–102. [Google Scholar] [CrossRef]
- de Campos, T.A.; Gonçalves, L.F.; Magalhães, K.G.; de Paulo Martins, V.; Pappas Júnior, G.J.; Peirano, G.; Pitout, J.D.; Gonçalves, G.B.; Furlan, J.P.R.; Stehling, E.G.; et al. A Fatal Bacteremia Caused by Hypermucousviscous KPC-2 Producing Extensively Drug-Resistant K64-ST11 Klebsiella pneumoniae in Brazil. Front. Med. 2018, 5, 265. [Google Scholar] [CrossRef]
- Cubero, M.; Marti, S.; Domínguez, M.Á.; González-Díaz, A.; Berbel, D.; Ardanuy, C. Hypervirulent Klebsiella pneumoniae serotype K1 clinical isolates form robust biofilms at the air-liquid interface. PLoS ONE 2019, 14, e0222628. [Google Scholar] [CrossRef]
- Fang, C.-T.; Lai, S.-Y.; Yi, W.-C.; Hsueh, P.-R.; Liu, K.-L.; Chang, S.-C. Klebsiella pneumoniae Genotype K1: An Emerging Pathogen That Causes Septic Ocular or Central Nervous System Complications from Pyogenic Liver Abscess. Clin. Infect. Dis. 2007, 45, 284–293. [Google Scholar] [CrossRef] [PubMed]
- Siu, L.K.; Yeh, K.-M.; Lin, J.-C.; Fung, C.-P.; Chang, F.-Y. Klebsiella pneumoniae liver abscess: A new invasive syndrome. Lancet Infect. Dis. 2012, 12, 881–887. [Google Scholar] [CrossRef] [PubMed]
- Fazili, T.; Sharngoe, C.; Endy, T.; Kiska, D.; Javaid, W.; Polhemus, M. Klebsiella pneumoniae Liver Abscess: An Emerging Disease. Am. J. Med. Sci. 2016, 351, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological quality of case series studies. JBI Database Syst. Rev. Implem. Rep. 2019, 18, 1. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Int. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, R.K.; Burns, B. Systemic Inflammatory Response Syndrome. StatPearls [Internet]. January 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK547669/ (accessed on 16 January 2022).
- Eisenmenger, E.F.; Guajardo, E.; Finch, N.; Atmar, R.; Sargsyan, Z. “String Test” for Hypermucoviscous Klebsiella pneumoniae. Am. J. Med. 2015, 134, E520–E521. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, J.; Jiang, W. An Increasing Prominent Disease of Klebsiella pneumoniae Liver Abscess: Etiology, Diagnosis, and Treatment. Gastroenterol. Res. Pract. 2013, 2013, e258514. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.-F.; Chang, Y.-Y.; Lin, Y.-T.; Wang, F.-D.; Chan, Y.-J.; Fung, C.-P. Clinical characteristics and economic consequence of Klebsiella pneumoniae liver abscess in Taiwan. J. Microbiol. Immunol. Infect. 2015, 48, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Chuang, C.; Fan, W.-C.; Lin, Y.-T.; Wang, F.-D. The emergence of Klebsiella pneumoniae liver abscess in non-diabetic patients and the distribution of capsular types. Gut Pathog. 2016, 8, 46. [Google Scholar] [CrossRef]
- Fung, C.-P. A global emerging disease of Klebsiella pneumoniae liver abscess: Is serotype K1 an important factor for complicated endophthalmitis? Gut 2002, 50, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Chung, D.R.; Lee, H.R.; Lee, S.S.; Kim, S.W.; Chang, H.H.; Jung, S.I.; Oh, M.-D.; Ko, K.S.; Kang, C.-I.; Peck, K.R.; et al. Evidence for Clonal Dissemination of the Serotype K1 Klebsiella pneumoniae Strain Causing Invasive Liver Abscesses in Korea. J. Clin. Microbiol. 2008, 46, 4061–4063. [Google Scholar] [CrossRef]
- Zheng, B.; Xu, H.; Lv, T.; Guo, L.; Xiao, Y.; Huang, C.; Zhang, S.; Chen, Y.; Han, H.; Shen, P.; et al. Stool Samples of Acute Diarrhea Inpatients as a Reservoir of ST11 Hypervirulent KPC-2-Producing Klebsiella pneumoniae. MSystems 2020, 5, e00498-20. [Google Scholar] [CrossRef]
- Ang, M.; Jap, A.; Chee, S.P. Prognostic Factors and Outcomes in Endogenous Klebsiella pneumoniae Endophthalmitis. Am. J. Ophthalmol. 2011, 151, 338–344.e2. [Google Scholar] [CrossRef]
- Dubey, D.; Raza, F.S.; Sawhney, A.; Pandey, A. Klebsiella pneumoniae renal abscess syndrome: A rare case with metastatic involvement of lungs, eye, and brain. Case Rep. Infect. Dis. 2013, 2013, 685346. [Google Scholar] [CrossRef]
- Patel, P.K.; Russo, T.A.; Karchmer, A.W. Hypervirulent Klebsiella pneumoniae. Open Forum Infect. Dis. 2014, 1, ofu028. [Google Scholar] [CrossRef] [PubMed]
- Chung, D.R.; Lee, H.; Park, M.H.; Jung, S.I.; Chang, H.H.; Kim, Y.S.; Son, J.S.; Moon, C.; Kwon, K.T.; Ryu, S.Y.; et al. Fecal carriage of serotype K1 Klebsiella pneumoniae ST23 strains closely related to liver abscess isolates in Koreans living in Korea. Eur. J. Clin. Microbiol. Infect. Dis. 2011, 31, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Siu, L.; Lin, J.; Chen, T.-L.; Tseng, C.-P.; Yeh, K.-M.; Chang, F.-Y.; Fung, C.-P. Seroepidemiology of Klebsiella pneumoniae colonizing the intestinal tract of healthy Chinese and overseas Chinese adults in Asian countries. BMC Microbiol. 2012, 12, 13. [Google Scholar] [CrossRef]
- Jun, J.-B. Klebsiella pneumoniae liver abscess. Infect. Chemotherapy. 2018, 50, 210–218. [Google Scholar] [CrossRef]
- Martin, R.M.; Bachman, M.A. Colonization, Infection, and the Accessory Genome of Klebsiella pneumoniae. Front. Cell Infect. Microbiol. 2018, 8, 4. [Google Scholar] [CrossRef]
- Mukherjee, S.; Archuleta, S.; Pang, J. Risk Factors of Septic Metastatic Infection among Patients with Klebsiella pneumoniae Liver Abscess in Singapore: A Case–Control Study. Am. J. Trop. Med. Hyg. 2022, 106, 805–808. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Zhang, B.; Wang, Y.; Jing, S.; Ning, W.; Liu, C.; Chen, C. A wide clinical spectrum of pulmonary affection in subjects with community-acquired Klebsiella pneumoniae liver abscess (CA-KPLA). J. Infect. Chemother. 2023, 29, 48–54. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, H.; Liu, Z.; Chang, Z. The incidence of septic pulmonary embolism in patients with Klebsiella pneumoniae liver abscess: A systematic review and meta-analysis. Gastroenterol. Res. Pract. 2022, 2022, 3777122. [Google Scholar] [CrossRef]
- Hsu, C.R.; Lin, T.L.; Chen, Y.C.; Chou, H.C.; Wang, J.T. The role of Klebsiella pneumoniae RMPA in capsular polysaccharide synthesis and virulence revisited. Microbiology 2011, 157, 3446–3457. [Google Scholar] [CrossRef] [PubMed]
- Russo, T.A.; Olson, R.; Fang, C.-T.; Stoesser, N.; Miller, M.; MacDonald, U.; Hutson, A.; Barker, J.H.; La Hoz, R.M.; Johnson, J.R.; et al. Identification of biomarkers for differentiation of hypervirulent Klebsiella pneumoniae from classical K. pneumoniae. J. Clin. Microbiol. 2018, 56, e00776-18. [Google Scholar] [CrossRef] [PubMed]
- Rafat, C.; Messika, J.; Barnaud, G.; Dufour, N.; Magdoud, F.; Billard-Pomarès, T.; Gaudry, S.; Dreyfuss, D.; Branger, C.; Decré, D.; et al. Hypervirulent Klebsiella pneumoniae, a 5-year study in a French ICU. J. Med. Microbiol. 2018, 67, 1083–1089. [Google Scholar] [CrossRef] [PubMed]
- Tan, T.Y.; Cheng, Y.; Ong, M.; Ng, L.S. Performance characteristics and clinical predictive value of the string test for detection of hepato-virulent Klebsiella pneumoniae isolated from blood cultures. Diag. Microbiol. Infect. Dis. 2014, 78, 127–128. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.P.; Siu, L.K.; Chang, F.Y. Extended-spectrum cephalosporin compared to cefazolin for treatment of Klebsiella pneumoniae-caused liver abscess. Antimicrob. Agents Chemother. 2003, 47, 2088–2092. [Google Scholar] [CrossRef]
- Lee, S.S.; Chen, Y.C.; Tsai, H.C.; Wann, S.R.; Lin, H.H.; Huang, C.K.; Liu, Y.C. Predictors of Septic Metastatic Infection and Mortality among Patients with Klebsiella pneumoniae Liver Abscess. Clin. Infect. Dis. 2008, 47, 642–650. [Google Scholar] [CrossRef]
- Harada, S.; Doi, Y. Hypervirulent Klebsiella pneumoniae: A call for consensus definition and international collaboration. J. Clin. Microbiol. 2018, 56, e00959-18. [Google Scholar] [CrossRef]
- Goldman, J.; Kowalec, J. Hepatic Abscess and Osteomyelitis from Klebsiella pneumoniae. JAMA 1978, 240, 2660. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total [n (%)] | |
|---|---|
| Age median (range) | 52 (18–86) years |
| Gender (n = 144) | |
| Male, n (%) | 112 (77.78%) |
| Comorbidities (n = 144) | |
| Diabetes mellitus, n (%) | 58 (40.28%) |
| Hypertension, n (%) | 20 (13.89%) |
| Hyperlipidemia/Coronary artery disease, n (%) | 10 (6.94%) |
| Alcohol use, n (%) | 4 (2.77%) |
| Concomitant malignancy, n (%) | 3 (2.08%) |
| Reported Symptoms (n = 144) | |
| Fever, n (%) | 121 (84.03%) |
| Abdominal pain, n (%) | 78 (54.17%) |
| Constitutional symptoms, n (%) | 71 (49.31%) |
| Nausea/vomiting, n (%) | 48 (33.33%) |
| Vision complaints, n (%) | 28 (19.44%) |
| Diarrhea, n (%) | 19 (13.19%) |
| Headache, n (%) | 17 (11.81%) |
| Dyspnea, n (%) | 14 (9.72%) |
| Cough, n (%) | 11 (7.64%) |
| Urinary symptoms, n (%) | 11 (7.64%) |
| Jaundice, n (%) | 10 (6.25%) |
| Chest pain, n (%) | 4 (2.77%) |
| Ethnicities (n = 144) | |
| Asian, n (%) | 56 (38.89%) |
| Hispanic/Latino, n (%) | 16 (11.11%) |
| White/Caucasian, n (%) | 8 (5.56%) |
| African American, n (%) | 6 (4.17%) |
| Afro-Caribbean, n (%) | 4 (2.78%) |
| Pacific Islanders, n (%) | 3 (2.08%) |
| Asian American, n (%) | 2 (1.39%) |
| Not reported, n (%) | 49 (34.03%) |
| Bacteremia (n = 144) | 86 (59.72%) |
| Extrahepatic disease (n = 144) | |
| Lungs or pleura, n (%) * | 42 (29.17%) |
| Ocular structures, n (%) + | 33 (22.92%) |
| Other intra-abdominal abscesses, n (%) # | 16 (11.11%) |
| Brain and meninges, n (%) ˠ | 15 (10.42%) |
| Genotypic profile (n = 19) | |
| magA/wzyKpK1 gene, n (%) | 11 (57.89%) |
| rmpA gene, n (%) | 13 (69.42%) |
| iro, iuc, ybtA, clbA, and/or peg-344 genes, n (%) | 4 (21.05%) |
| Phenotypic profile (n = 32) | |
| Hypermucoviscosity, n (%) | 28 (87.50%) |
| K1 serotype, n (%) | 9 (28.13%) |
| K2 serotype, n (%) | 4 (12.50%) |
| Non K1/K2 serotype, n (%) | 2 (6.25%) |
| Siderophores, n (%) | 0 (0.00%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardenas-Alvarez, J.; Balayla, G.; Triana, A.; Diaz Lankenau, R.; Franco-Paredes, C.; Henao-Martínez, A.F.; Motoa, G. Clinical Spectrum and Outcomes of Cryptogenic Klebsiella pneumoniae Liver Abscess in the Americas: A Scoping Review. Pathogens 2023, 12, 661. https://doi.org/10.3390/pathogens12050661
Cardenas-Alvarez J, Balayla G, Triana A, Diaz Lankenau R, Franco-Paredes C, Henao-Martínez AF, Motoa G. Clinical Spectrum and Outcomes of Cryptogenic Klebsiella pneumoniae Liver Abscess in the Americas: A Scoping Review. Pathogens. 2023; 12(5):661. https://doi.org/10.3390/pathogens12050661
Chicago/Turabian StyleCardenas-Alvarez, Jorge, Galit Balayla, Abel Triana, Rodrigo Diaz Lankenau, Carlos Franco-Paredes, Andrés F. Henao-Martínez, and Gabriel Motoa. 2023. "Clinical Spectrum and Outcomes of Cryptogenic Klebsiella pneumoniae Liver Abscess in the Americas: A Scoping Review" Pathogens 12, no. 5: 661. https://doi.org/10.3390/pathogens12050661