
Efficacy of Fosfomycin-Containing Regimens for Treatment of Bacteremia Due to Pan-Drug Resistant Acinetobacter baumannii in Critically Ill Patients: A Case Series Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Patients and Methods
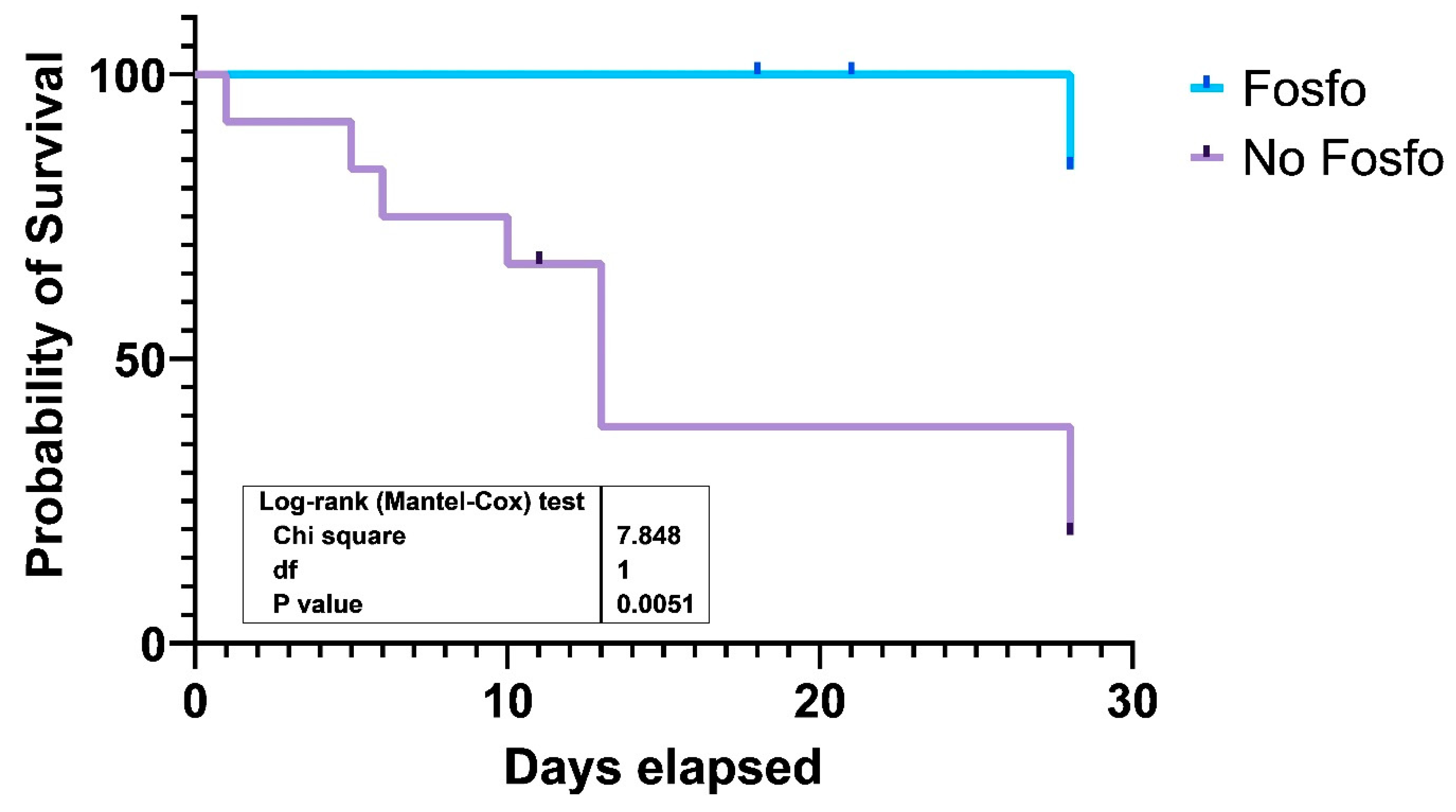
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nowak, J.; Zander, E.; Stefanik, D.; Higgins, P.G.; Roca, I.; Vila, J.; McConnell, M.J.; Cisneros, J.M.; Seifert, H.; MagicBullet Working Group WP4. High incidence of pandrug-resistant Acinetobacter baumannii isolates collected from patients with ventilator-associated pneumonia in Greece, Italy and Spain as part of the MagicBullet clinical trial. J. Antimicrob. Chemother. 2017, 72, 3277–3282. [Google Scholar] [CrossRef] [PubMed]
- Polemis, M.; Mandilara, G.; Pappa, O.; Argyropoulou, A.; Perivolioti, E.; Koudoumnakis, N.; Pournaras, S.; Vasilakopoulou, A.; Vourli, S.; Katsifa, H.; et al. COVID-19 and Antimicrobial Resistance: Data from the Greek Electronic System for the Surveillance of Antimicrobial Resistance—WHONET-Greece (January 2018–March 2021). Life 2021, 11, 996. [Google Scholar] [CrossRef] [PubMed]
- Karakonstantis, S.; Kritsotakis, E.I.; Gikas, A. Pandrug-resistant Gram-negative bacteria: A systematic review of current epidemiology, prognosis and treatment options. J. Antimicrob. Chemother. 2020, 75, 271–282. [Google Scholar] [CrossRef] [PubMed]
- Karakonstantis, S.; Kritsotakis, E.I.; Gikas, A. Treatment options for K. pneumoniae, P. aeruginosa and A. baumannii co-resistant to carbapenems, aminoglycosides, polymyxins and tigecycline: An approach based on the mechanisms of resistance to carbapenems. Infection 2020, 48, 835–851. [Google Scholar] [CrossRef]
- Karakonstantis, S.; Gikas, A.; Astrinaki, E.; Kritsotakis, E.I. Excess mortality due to pandrug-resistant Acinetobacter baumannii infections in hospitalized patients. J. Hosp. Infect. 2020, 106, 447–453. [Google Scholar] [CrossRef]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 13.0. 2023. Available online: http://www.eucast.org (accessed on 10 January 2023).
- Chuang, Y.C.; Cheng, C.Y.; Sheng, W.H.; Sun, H.Y.; Wang, J.T.; Chen, Y.C.; Chang, S.C. Effectiveness of tigecycline-based versus colistin- based therapy for treatment of pneumonia caused by multidrug-resistant Acinetobacter baumannii in a critical setting: A matched cohort analysis. BMC Infect. Dis. 2014, 14, 102. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.; Chuang, Y.C.; Sun, H.Y.; Sheng, W.H.; Yang, C.J.; Liao, C.H.; Hsueh, P.R.; Yang, J.L.; Shen, N.J.; Wang, J.T.; et al. Excess Mortality Associated with Colistin-Tigecycline Compared with Colistin-Carbapenem Combination Therapy for Extensively Drug-Resistant Acinetobacter baumannii Bacteremia: A Multicenter Prospective Observational Study. Crit. Care Med. 2015, 43, 1194–1204. [Google Scholar] [CrossRef]
- Yang, T.; Mei, H.; Wang, J.; Cai, Y. Therapeutic Drug Monitoring of Tigecycline in 67 Infected Patients and a Population Pharmacokinetics/Microbiological Evaluation of A. baumannii Study. Front. Microbiol. 2021, 12, 678165. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Montrucchio, G.; Corcione, S.; Lupia, T.; Shbaklo, N.; Olivieri, C.; Poggioli, M.; Pagni, A.; Colombo, D.; Roasio, A.; Bosso, S.; et al. The Burden of Carbapenem-Resistant Acinetobacter baumannii in ICU COVID-19 Patients: A Regional Experience. J. Clin. Med. 2022, 11, 5208. [Google Scholar] [CrossRef] [PubMed]
- Ballouz, T.; Aridi, J.; Afif, C.; Irani, J.; Lakis, C.; Nasreddine, R.; Azar, E. Risk Factors, Clinical Presentation, and Outcome of Acinetobacter baumannii Bacteremia. Front. Cell. Infect. Microbiol. 2017, 7, 156. [Google Scholar] [CrossRef] [PubMed]
- Dezza, F.C.; Arcari, G.; Alessi, F.; Valeri, S.; Curtolo, A.; Sacco, F.; Ceccarelli, G.; Raponi, G.; Alessandri, F.; Mastroianni, C.M.; et al. Clinical Impact of COVID-19 on Multi-Drug-Resistant Gram-Negative Bacilli Bloodstream Infections in an Intensive Care Unit Setting: Two Pandemics Compared. Antibiotics 2022, 11, 926. [Google Scholar] [CrossRef]
- Doi, Y. Treatment Options for Carbapenem-resistant Gram-negative Bacterial Infections. Clin. Infect. Dis. 2019, 69 (Suppl. S7), S565–S575. [Google Scholar] [CrossRef] [PubMed]
- Poulikakos, P.; Tansarli, G.S.; Falagas, M.E. Combination antibiotic treatment versus monotherapy for multidrug-resistant, extensively drug-resistant, and pandrug-resistant Acinetobacter infections: A systematic review. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 1675–1685. [Google Scholar] [CrossRef]
- Karakonstantis, S.; Ioannou, P.; Samonis, G.; Kofteridis, D.P. Systematic Review of Antimicrobial Combination Options for Pandrug-Resistant Acinetobacter baumannii. Antibiotics 2021, 10, 1344. [Google Scholar] [CrossRef]
- Dizbay, M.; Tozlu, D.K.; Cirak, M.Y.; Isik, Y.; Ozdemir, K.; Arman, D. In vitro synergistic activity of tigecycline and colistin against XDR-Acinetobacter baumannii. J. Antibiot. 2010, 63, 51–53. [Google Scholar] [CrossRef]
- Karakonstantis, S.; Ioannou, P.; Kofteridis, D.D. In search for a synergistic combination against pandrug-resistant A. baumannii; methodological considerations. Infection 2022, 50, 569–581. [Google Scholar] [CrossRef]
- Falagas, M.E.; Vouloumanou, E.K.; Samonis, G.; Vardakas, K.Z. Fosfomycin. Clin. Microbiol. Rev. 2016, 29, 321–347. [Google Scholar] [CrossRef]
- Antonello, R.M.; Principe, L.; Maraolo, A.E.; Viaggi, V.; Pol, R.; Fabbiani, M.; Montagnani, F.; Lovecchio, A.; Luzzati, R.; Di Bella, S. Fosfomycin as Partner Drug for Systemic Infection Management. A Systematic Review of its Synergistic Properties from in Vitro and in Vivo Studies. Antibiotics 2020, 9, 500. [Google Scholar] [CrossRef]
- Mohd Sazlly Lim, S.; Heffernan, A.J.; Roberts, J.A.; Sime, F.B. Semi-mechanistic PK/PD modelling of fosfomycin and sulbactam combination against carbapenem-resistant Acinetobacter baumannii. Antimicrob. Agents Chemother. 2021, 65, 321–347. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Kastoris, A.C.; Karageorgopoulos, D.; Rafailidis, P.I. Fosfomycin for the treatment of infections caused by multidrug-resistant non-fermenting Gram-negative bacilli: A systematic review of microbiological, animal and clinical studies. Int. J. Antimicrob. Agents 2009, 34, 111–120. [Google Scholar] [CrossRef]
- Aysert-Yildiz, P.; Özgen-Top, O.; Habibi, H.; Dizbay, M. Efficacy and safety of intravenous fosfomycin for the treatment of carbapenem-resistant Klebsiella pneumoniae. J. Chemother. 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Sirijatuphat, R.; Thamlikitkul, V. Preliminary Study of Colistin versus Colistin plus Fosfomycin for Treatment of Carbapenem-Resistant Acinetobacter baumannii Infections. Antimicrob. Agents Chemother. 2014, 58, 5598–5601. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Bassetti, M.; Bellelli, V.; Bianchi, L.; Cattaneo, F.M.; Mazzocchetti, S.; Paciacconi, E.; Cottini, F.; Schiattarella, A.; Tufaro, G.; et al. Efficacy of a Fosfomycin-Containing Regimen for Treatment of Severe Pneumonia Caused by Multidrug-Resistant Acinetobacter baumannii: A Prospective, Observational Study. Infect. Dis. Ther. 2021, 10, 187–200. [Google Scholar] [CrossRef]


{kind=link}
| Patient | AGE | SEX | CCI | COVID | APACHE II | Antibiotics Used | Microbiological Success | 28-day Mortality |
|---|---|---|---|---|---|---|---|---|
| 1 | 65 | F | 3 | Yes | 15 | CST, TGC | Yes | No |
| 2 | 53 | M | 1 | Yes | 24 | CST, TGC | Yes | No |
| 3 | 64 | M | 2 | No | 22 | CST, SXT, FOS | Yes | No |
| 4 | 64 | M | 4 | No | 10 | CST, FOS | Yes | No |
| 5 | 28 | F | 0 | No | 7 | CST, AMS, FOS, AMK | Yes | No |
| 6 | 76 | M | 6 | No | 8 | CST, MEM | Yes | No |
| 7 | 72 | M | 9 | No | 13 | CST, TGC, FOS | Yes | No |
| 8 | 64 | F | 6 | No | 25 | TGC, AMS, FOS AMK | Yes | No |
| 9 | 71 | F | 7 | No | 19 | CST, TGC, FOS | Yes | No |
| 10 | 36 | F | 0 | Yes | 20 | CST, MEM, FOS, SXT, GEN | Yes | No |
| 11 | 53 | M | 1 | Yes | 11 | CST, TGC, AMS, SXT, AMK | Yes | Yes |
| 12 | 60 | M | 2 | Yes | 17 | CST, MEM, TGC, AMS | No | Yes |
| 13 | 71 | F | 4 | Yes | 38 | CST, TGC, FOS, AMK, SXT | Yes | Yes |
| 14 | 59 | M | 1 | Yes | 40 | CST, AMK | No | Yes |
| 15 | 78 | M | 3 | Yes | 39 | CST, PTZ | No | Yes |
| 16 | 70 | F | 5 | Yes | 26 | MEM, GEN | No | Yes |
| 17 | 55 | F | 4 | Yes | 20 | CST, MEM | No | Yes |
| 18 | 62 | F | 2 | Yes | 28 | MEM, AMS, TGC | No | Yes |
| 19 | 55 | F | 1 | Yes | 25 | CST, TGC, AMS | Yes | Yes |
| 20 | 93 | F | 8 | Yes | 12 | CST, MEM | Yes | Yes |
| 28-day Mortality | Statistics | ||
|---|---|---|---|
| Characteristics | Survived (n = 10) | Died (n = 10) | p |
| Age years [Median (IQR)] | 64 (48–71) | 61 (55–72) | ns |
| Female Gender (%) | 5 (50) | 6 (60) | ns |
| Charlson Comorbidity Index mean ± SD | 3.8 ± 3.1 | 3.1 ± 2.2 | ns |
| APACHE II mean ± SD | 16.3 ± 6.6 | 25.6 ± 10.8 | 0.032 |
| SOFA mean ± SD | 7.1 ± 3.8 | 11.4 ± 4.3 | 0.03 |
| Septic Shock (%) | 0 | 6 (60) | 0.003 |
| COVID (%) | 3 (30) | 10 (100) | 0.001 |
| ≥3 antibiotics combination regimen (%) | 6 (60) | 5 (50) | ns |
| Colistin containing regimen (%) | 9 (90) | 8 (80) | ns |
| Tigecycline containing regimen (%) | 5 (50) | 5 (50) | ns |
| Fosfomycin containing regiment (%) | 7 (70) | 1 (10) | 0.02 |
| Aminoglycoside containing regimen (%) | 3 (30) | 4 (40) | ns |
| Carbapenem containing regimen (%) | 2 (20) | 5 (50) | ns |
| Ampicillin-Sulbactam containing regimen (%) | 2 (20) | 4 (40) | ns |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assimakopoulos, S.F.; Karamouzos, V.; Eleftheriotis, G.; Lagadinou, M.; Bartzavali, C.; Kolonitsiou, F.; Paliogianni, F.; Fligou, F.; Marangos, M. Efficacy of Fosfomycin-Containing Regimens for Treatment of Bacteremia Due to Pan-Drug Resistant Acinetobacter baumannii in Critically Ill Patients: A Case Series Study. Pathogens 2023, 12, 286. https://doi.org/10.3390/pathogens12020286
Assimakopoulos SF, Karamouzos V, Eleftheriotis G, Lagadinou M, Bartzavali C, Kolonitsiou F, Paliogianni F, Fligou F, Marangos M. Efficacy of Fosfomycin-Containing Regimens for Treatment of Bacteremia Due to Pan-Drug Resistant Acinetobacter baumannii in Critically Ill Patients: A Case Series Study. Pathogens. 2023; 12(2):286. https://doi.org/10.3390/pathogens12020286
Chicago/Turabian StyleAssimakopoulos, Stelios F., Vassilis Karamouzos, Gerasimos Eleftheriotis, Maria Lagadinou, Christina Bartzavali, Fevronia Kolonitsiou, Fotini Paliogianni, Fotini Fligou, and Markos Marangos. 2023. "Efficacy of Fosfomycin-Containing Regimens for Treatment of Bacteremia Due to Pan-Drug Resistant Acinetobacter baumannii in Critically Ill Patients: A Case Series Study" Pathogens 12, no. 2: 286. https://doi.org/10.3390/pathogens12020286