

Do We Have Enough Evidence to Specifically Recommend Transoral Robotic Surgery in HPV−Driven Oropharyngeal Cancer? A Systematic Review
 , , , , , ,
, , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Data Source and Study Searching
2.3. Study Quality Assessment
2.4. Data Extraction and Analyses
3. Results
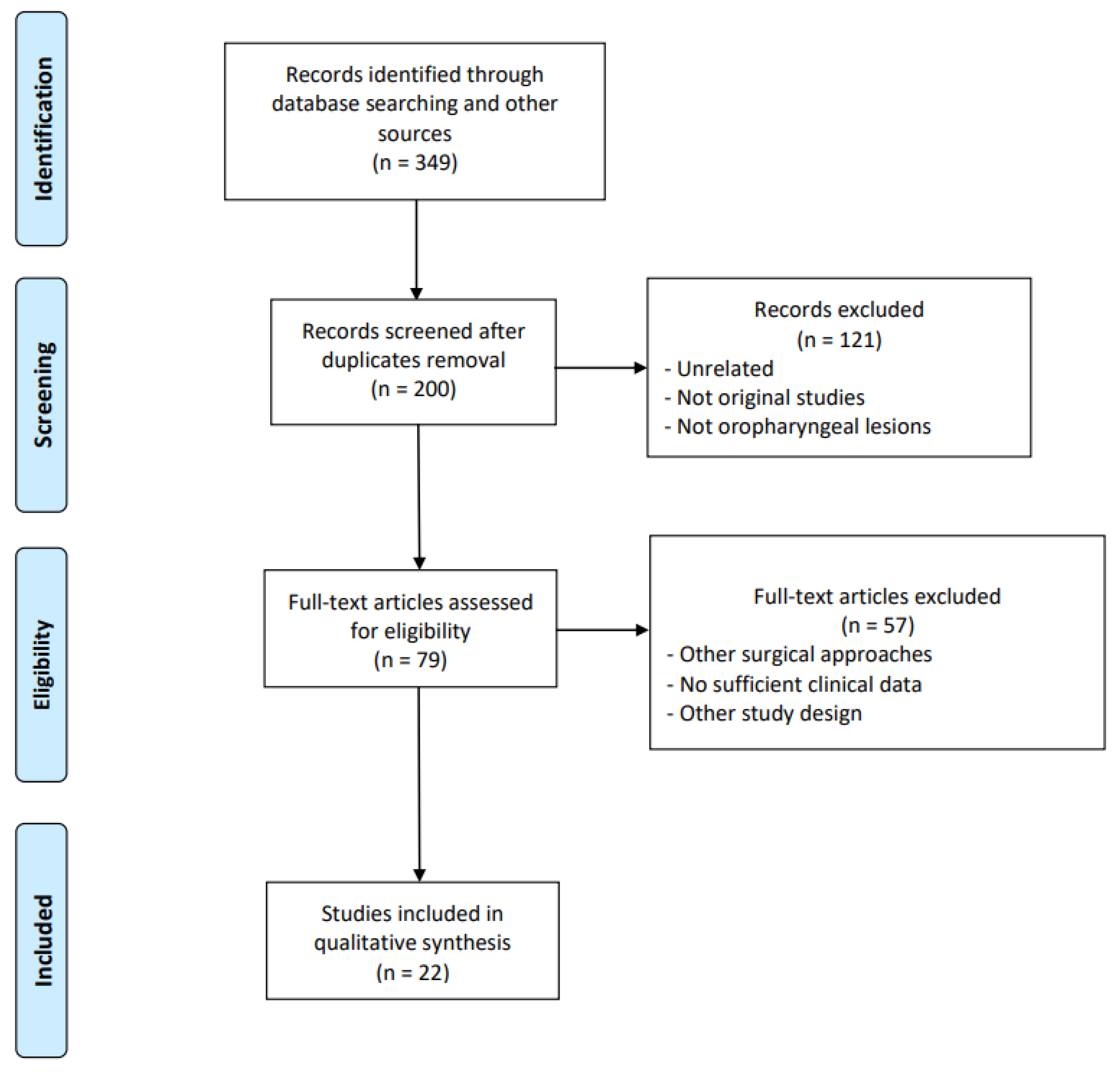
3.1. Search Results and Patients’ Characteristics
3.2. Methodological Quality of Included Studies
3.3. Oncologic Outcomes and Relation to HPV Status
4. Discussion
4.1. The issue of Detection Method
4.2. Clinical Meaning of HPV−Driven Carcinogenesis
4.3. Impact of TORS on Long-Term Morbidity in Survivors
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- D’Souza, G.; Kreimer, A.R.; Viscidi, R.; Pawlita, M.; Fakhry, C.; Koch, W.M.; Westra, W.H.; Gillison, M.L. Case-control study of human papillomavirus and oropharyngeal cancer. N. Engl. J. Med. 2007, 356, 1944–1956. [Google Scholar] [CrossRef] [Green Version]
- Dayyani, F.; Etzel, C.J.; Liu, M.; Ho, C.H.; Lippman, S.M.; Tsao, A.S. Meta-analysis of the impact of human papillomavirus (HPV) on cancer risk and overall survival in head and neck squamous cell carcinomas (HNSCC). Head Neck Oncol. 2010, 2, 15. [Google Scholar] [CrossRef] [Green Version]
- Termine, N.; Panzarella, V.; Falaschini, S.; Russo, A.; Matranga, D.; Lo Muzio, L.; Campisi, G. HPV in oral squamous cell carcinoma vs. head and neck squamous cell carcinoma biopsies: A meta-analysis (1988-2007). Ann. Oncol. 2008, 19, 1681–1690. [Google Scholar] [CrossRef]
- Adelstein, D.J.; Ridge, J.A.; Gillison, M.L.; Chaturvedi, A.K.; D’Souza, G.; Gravitt, P.E.; Westra, W.; Psyrri, A.; Kast, W.M.; Koutsky, L.A.; et al. Head and neck squamous cell cancer and the human papillomavirus: Summary of a National Cancer Institute State of the Science Meeting, 9–10 November 2008, Washington, D.C. Head Neck 2009, 31, 1393–1422. [Google Scholar] [CrossRef]
- Chaturvedi, A.K.; Engels, E.A.; Pfeiffer, R.M.; Hernandez, B.Y.; Xiao, W.; Kim, E.; Jiang, B.; Goodman, M.T.; Sibug-Saber, M.; Cozen, W.; et al. Human papillomavirus and rising oropharyngeal cancer incidence in the United States. J. Clin. Oncol. 2011, 29, 4294–4301. [Google Scholar] [CrossRef]
- Licitra, L.; Perrone, F.; Bossi, P.; Suardi, S.; Mariani, L.; Artusi, R.; Oggionni, M.; Rossini, C.; Cantù, G.; Squadrelli, M.; et al. High-risk human papillomavirus affects prognosis in patients with surgically treated oropharyngeal squamous cell carcinoma. J. Clin. Oncol. 2006, 24, 5630–5636. [Google Scholar] [CrossRef] [Green Version]
- Fakhry, C.; Westra, W.H.; Li, S.; Cmelak, A.; Ridge, J.A.; Pinto, H.; Forastiere, A.; Gillison, M.L. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J. Natl. Cancer Instig. 2008, 100, 261–269. [Google Scholar] [CrossRef] [Green Version]
- Sturgis, E.M.; Cinciripini, P.M. Trends in head and neck cancer incidence in relation to smoking prevalence: An emerging epidemic of human papillomavirus-associated cancers? Cancer 2007, 110, 1429–1435. [Google Scholar] [CrossRef]
- Bussu, F.; Sali, M.; Gallus, R.; Petrone, G.; Zannoni, G.F.; Autorino, R.; Dinapoli, N.; Santangelo, R.; Vellone, V.G.; Graziani, C.; et al. Human papillomavirus (HPV) infection in squamous cell carcinomas arising from the oropharynx: Detection of HPV DNA and p16 immunohistochemistry as diagnostic and prognostic indicators--a pilot study. Int. J. Radiat. Oncol. Biol. Phys. 2014, 89, 1115–1120. [Google Scholar] [CrossRef]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef]
- Lassen, P.; Eriksen, J.G.; Hamilton-Dutoit, S.; Tramm, T.; Alsner, J.; Overgaard, J. Effect of HPV−associated p16INK4A expression on response to radiotherapy and survival in squamous cell carcinoma of the head and neck. J. Clin. Oncol. 2009, 27, 1992–1998. [Google Scholar] [CrossRef] [Green Version]
- Albers, A.; Abe, K.; Hunt, J.; Wang, J.; Lopez-Albaitero, A.; Schaefer, C.; Gooding, W.; Whiteside, T.L.; Ferrone, S.; DeLeo, A.; et al. Antitumor activity of human papillomavirus type 16 E7-specific T cells against virally infected squamous cell carcinoma of the head and neck. Cancer Res. 2005, 65, 11146–11155. [Google Scholar] [CrossRef] [Green Version]
- Hong, A.M.; Dobbins, T.A.; Lee, C.S.; Yeo, R.; Yeoh, K.W. Human papillomavirus predicts outcome in oropharyngeal cancer in patients treated primarily with surgery or radiation therapy. Br. J. Cancer 2010, 103, 1510–1517. [Google Scholar] [CrossRef]
- Boscolo-Rizzo, P.; Stellin, M.; Fuson, R.; Marchiori, C.; Gava, A.; Da Mosto, M.C. Long-term quality of life after treatment for locally advanced oropharyngeal carcinoma: Surgery and postoperative radiotherapy versus concurrent chemoradiation. Oral Oncol. 2009, 45, 953–957. [Google Scholar] [CrossRef]
- Mortensen, H.R.; Jensen, K.; Aksglaede, K.; Behrens, M.; Grau, C. Late dysphagia after IMRT for head and neck cancer and correlation with dose-volume parameters. Radiother. Oncol. 2013, 107, 288–294. [Google Scholar] [CrossRef]
- Naik, M.; Ward, M.C.; Bledsoe, T.J.; Kumar, A.M.; Rybicki, L.A.; Saxton, J.P.; Burkey, B.B.; Greskovich, J.F.; Adelstein, D.J.; Koyfman, S.A. It is not just IMRT: Human papillomavirus related oropharynx squamous cell carcinoma is associated with better swallowing outcomes after definitive chemoradiotherapy. Oral Oncol. 2015, 51, 800–804. [Google Scholar] [CrossRef]
- O’Sullivan, B.; Huang, S.H.; Siu, L.L.; Waldron, J.; Zhao, H.; Perez-Ordonez, B.; Weinreb, I.; Kim, J.; Ringash, J.; Bayley, A. Deintensification candidate subgroups in human papillomavirus-related oropharyngeal cancer according to minimal risk of distant metastasis. J. Clin. Oncol. 2013, 31, 543–550. [Google Scholar] [CrossRef]
- O’Sullivan, B.; Huang, S.H.; Perez-Ordonez, B.; Massey, C.; Siu, L.L.; Weinreb, I.; Hope, A.; Kim, J.; Bayley, A.J.; Cummings, B.; et al. Outcomes of HPV−related oropharyngeal cancer patients treated by radiotherapy alone using altered fractionation. Radiother. Oncol. 2012, 103, 49–56. [Google Scholar] [CrossRef]
- Van Abel, K.M.; Quick, M.H.; Graner, D.E.; Lohse, C.M.; Price, D.L.; Price, K.A.R.; Ma, D.J.; Moore, E.J. Outcomes following TORS for HPV−positive oropharyngeal carcinoma: PEGs, tracheostomies, and beyond. Am. J. Otolaryngol. 2019, 40, 729–734. [Google Scholar] [CrossRef]
- Masterson, L.; Moualed, D.; Liu, Z.W.; Howard, J.E.; Dwivedi, R.C.; Tysome, J.R.; Benson, R.; Sterling, J.C.; Sudhoff, H.; Jani, P.; et al. De-escalation treatment protocols for human papillomavirus-associated oropharyngeal squamous cell carcinoma: A systematic review and meta-analysis of current clinical trials. Eur. J. Cancer 2014, 50, 2636–2648. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Head and Neck Cancer (Version 1.2020). Available online: http://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf (accessed on 21 March 2020).
- Mirghani, H.; Amen, F.; Blanchard, P.; Moreau, F.; Guigay, J.; Hartl, D.M.; Lacau St Guily, J. Treatment de-escalation in HPV−positive oropharyngeal carcinoma: Ongoing trials, critical issues and perspectives. Int. J. Cancer 2015, 136, 1494–1503. [Google Scholar] [CrossRef]
- De Virgilio, A.; Kim, S.H.; Magnuson, J.S.; Holsinger, C.; Remacle, M.; Lawson, G.; Wang, C.C.; Mercante, G.; Malvezzi, L.; Iocca, O.; et al. Anatomical-based classification for transoral lateral oropharyngectomy. Oral Oncol. 2019, 99, 104450. [Google Scholar] [CrossRef]
- De Virgilio, A.; Park, Y.M.; Kim, W.S.; Baek, S.J.; Kim, S.H. How to optimize laryngeal and hypopharyngeal exposure in transoral robotic surgery. Auris Nasus Larynx 2013, 40, 312–319. [Google Scholar] [CrossRef]
- Mercante, G.; Masiello, A.; Sperduti, I.; Cristalli, G.; Pellini, R.; Spriano, G. Quality of life and functional evaluation in patients with tongue base tumors treated exclusively with transoral robotic surgery: A 1-year follow-up study. J. Craniomaxillofac. Surg. 2015, 43, 1561–1566. [Google Scholar] [CrossRef]
- Mercante, G.; Ruscito, P.; Pellini, R.; Cristalli, G.; Spriano, G. Transoral robotic surgery (TORS) for tongue base tumours. Acta Otorhinolaryngol. Ital. 2013, 33, 230–235. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Methods for the Development of NICE Public Health Guidance; National Institute for Health and Care Excellence (NICE): London, UK, 2012.
- Smith, R.V.; Schiff, B.A.; Garg, M.; Haigentz, M. The impact of transoral robotic surgery on the overall treatment of oropharyngeal cancer patients. Laryngoscope 2015, 125 (Suppl. 10), S1–S15. [Google Scholar] [CrossRef]
- Moore, E.J.; Van Abel, K.M.; Price, D.L.; Lohse, C.M.; Olsen, K.D.; Jackson, R.S.; Martin, E.J. Transoral robotic surgery for oropharyngeal carcinoma: Surgical margins and oncologic outcomes. Head Neck 2018, 40, 747–755. [Google Scholar] [CrossRef]
- Nichols, A.C.; Theurer, J.; Prisman, E.; Read, N.; Berthelet, E.; Tran, E.; Fung, K.; de Almeida, J.R.; Bayley, A.; Goldstein, D.P.; et al. Radiotherapy versus transoral robotic surgery and neck dissection for oropharyngeal squamous cell carcinoma (ORATOR): An open-label, phase 2, randomised trial. Lancet Oncol. 2019, 20, 1349–1359. [Google Scholar] [CrossRef]
- Cohen, M.A.; Weinstein, G.S.; O’Malley, B.W., Jr.; Feldman, M.; Quon, H. Transoral robotic surgery and human papillomavirus status: Oncologic results. Head Neck 2011, 33, 573–580. [Google Scholar] [CrossRef]
- Blanco, R.G.; Fakhry, C.; Ha, P.K.; Ryniak, K.; Messing, B.; Califano, J.A.; Saunders, J.R. Transoral robotic surgery experience in 44 cases. J. Laparoendosc. Adv. Surg. Tech. A 2013, 23, 900–907. [Google Scholar] [CrossRef]
- Cannon, R.B.; Houlton, J.J.; Patel, S.; Raju, S.; Noble, A.; Futran, N.D.; Parvathaneni, U.; Méndez, E. Patterns of cervical node positivity, regional failure rates, and fistula rates for HPV+ oropharyngeal squamous cell carcinoma treated with transoral robotic surgery (TORS). Oral Oncol. 2018, 86, 296–300. [Google Scholar] [CrossRef]
- Dabas, S.; Gupta, K.; Sharma, A.K.; Shukla, H.; Ranjan, R.; Sharma, D.K. Oncological outcome following initiation of treatment for stage III and IV HPV negative oropharyngeal cancers with transoral robotic surgery (TORS). Eur. J. Surg. Oncol. 2019, 45, 2137–2142. [Google Scholar] [CrossRef]
- Dhanireddy, B.; Burnett, N.P.; Sanampudi, S.; Wooten, C.E.; Slezak, J.; Shelton, B.; Shelton, L.; Shearer, A.; Arnold, S.; Kudrimoti, M.; et al. Outcomes in surgically resectable oropharynx cancer treated with transoral robotic surgery versus definitive chemoradiation. Am. J. Otolaryngol. 2019, 40, 673–677. [Google Scholar] [CrossRef]
- Meccariello, G.; Montevecchi, F.; D’Agostino, G.; Iannella, G.; Calpona, S.; Parisi, E.; Costantini, M.; Cammaroto, G.; Gobbi, R.; Firinu, E.; et al. Trans-oral robotic surgery for the management of oropharyngeal carcinomas: A 9-year institutional experience. Acta Otorhinolaryngol. Ital. 2019, 39, 75–83. [Google Scholar] [CrossRef] [Green Version]
- Brody, R.M.; Shimunov, D.; Cohen, R.B.; Lin, A.; Lukens, J.N.; Hartner, L.; Aggarwal, C.; Duvvuri, U.; Montone, K.T.; Jalaly, J.B.; et al. A benchmark for oncologic outcomes and model for lethal recurrence risk after transoral robotic resection of HPV−related oropharyngeal cancers. Oral Oncol. 2022, 127, 105798. [Google Scholar] [CrossRef]
- Carey, R.M.; Brody, R.M.; Shimunov, D.; Shinn, J.R.; Mady, L.J.; Rajasekaran, K.; Cannady, S.B.; Lin, A.; Lukens, J.N.; Bauml, J.M.; et al. Locoregional Recurrence in p16-Positive Oropharyngeal Squamous Cell Carcinoma After TORS. Laryngoscope 2021, 131, E2865–E2873. [Google Scholar] [CrossRef]
- Gershowitz, J.; Chao, H.H.; Doucette, A.; Lukens, J.N.; Swisher-McClure, S.; Weinstein, G.S.; O’Malley, B.W., Jr.; Chalian, A.A.; Rassekh, C.H.; Newman, J.G.; et al. Risk of post-operative, pre-radiotherapy contralateral neck recurrence in patients treated with surgery followed by adjuvant radiotherapy for human papilloma virus-associated tonsil cancer. Br. J. Radiol. 2019, 92, 20190466. [Google Scholar] [CrossRef]
- Holcomb, A.J.; Herberg, M.; Strohl, M.; Ochoa, E.; Feng, A.L.; Abt, N.B.; Mokhtari, T.E.; Suresh, K.; McHugh, C.I.; Parikh, A.S.; et al. Impact of surgical margins on local control in patients undergoing single-modality transoral robotic surgery for HPV−related oropharyngeal squamous cell carcinoma. Head Neck 2021, 43, 2434–2444. [Google Scholar] [CrossRef]
- Nichols, D.S.; Zhao, J.; Boyce, B.J.; Amdur, R.; Mendenhall, W.M.; Danan, D.; Hitchcock, K.; Ning, K.; Keyes, K.; Lee, J.H.; et al. HPV/p16-positive oropharyngeal cancer treated with transoral robotic surgery: The roles of margins, extra-nodal extension and adjuvant treatment. Am. J. Otolaryngol. 2021, 42, 102793. [Google Scholar] [CrossRef]
- O’Hara, J.; Warner, L.; Fox, H.; Hamilton, D.; Meikle, D.; Counter, P.; Robson, A.; Goranova, R.; Iqbal, S.; Kelly, C.; et al. Primary transoral robotic surgery +/- adjuvant therapy for oropharyngeal squamous cell carcinoma-A large observational single-centre series from the United Kingdom. Clin. Otolaryngol. 2021, 46, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- Parhar, H.S.; Shimunov, D.; Brody, R.M.; Cannady, S.B.; Newman, J.G.; O’Malley, B.W., Jr.; Chalian, A.A.; Rassekh, C.H.; Weinstein, G.S.; Rajasekaran, K. Revisiting the Recommendation for Contralateral Tonsillectomy in HPV−Associated Tonsillar Carcinoma. Otolaryngol. Head Neck Surg. 2021, 164, 1222–1229. [Google Scholar] [CrossRef] [PubMed]
- Parhar, H.S.; Weinstein, G.S.; O’Malley, B.W., Jr.; Shimunov, D.; Rassekh, C.H.; Chalian, A.A.; Newman, J.G.; Basu, D.; Cannady, S.B.; Rajasekaran, K.; et al. Oncologic outcomes of transoral robotic surgery for HPV−negative oropharyngeal carcinomas. Head Neck 2021, 43, 2923–2934. [Google Scholar] [CrossRef] [PubMed]
- Philips, R.; Sagheer, H.; Barsouk, A.; Swendseid, B.; Johnson, J.; Bar Ad, V.; Luginbuhl, A.; Curry, J.; Cognetti, D. Trends in Adjuvant Therapy After Surgery for Oropharyngeal Squamous Cell Carcinoma. Laryngoscope 2022, 132, 806–812. [Google Scholar] [CrossRef]
- Sahovaler, A.; Lee, J.J.W.; Xu, W.; Su, S.; Hosni, A.; Bayley, A.; Goldstein, D.P.; de Almeida, J.R. Contralateral nodal failures in oropharyngeal cancers after TORS and unilateral neck management: A retrospective study. J. Otolaryngol. Head Neck Surg. 2021, 50, 71. [Google Scholar] [CrossRef]
- Sun, L.; Shimunov, D.; Tan, E.X.; Swisher-Mcclure, S.; Lin, A.; Lukens, J.N.; Basu, D.; Chalian, A.A.; Cannady, S.B.; Newman, J.G.; et al. Survival and toxicity in patients with human papilloma virus-associated oropharyngeal squamous cell cancer receiving trimodality therapy including transoral robotic surgery. Head Neck 2021, 43, 3053–3061. [Google Scholar] [CrossRef]
- Swisher-McClure, S.; Lukens, J.N.; Aggarwal, C.; Ahn, P.; Basu, D.; Bauml, J.M.; Brody, R.; Chalian, A.; Cohen, R.B.; Fotouhi-Ghiam, A.; et al. A Phase 2 Trial of Alternative Volumes of Oropharyngeal Irradiation for De-intensification (AVOID): Omission of the Resected Primary Tumor Bed After Transoral Robotic Surgery for Human Papilloma Virus-Related Squamous Cell Carcinoma of the Oropharynx. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 725–732. [Google Scholar] [CrossRef]
- Yver, C.M.; Shimunov, D.; Weinstein, G.S.; Rajasekaran, K.; Cannady, S.B.; Lukens, J.N.; Lin, A.; Swisher-McClure, S.; Cohen, R.B.; Aggarwal, C.; et al. Oncologic and survival outcomes for resectable locally-advanced HPV−related oropharyngeal cancer treated with transoral robotic surgery. Oral Oncol. 2021, 118, 105307. [Google Scholar] [CrossRef]
- Bussu, F.; Ragin, C.; Boscolo-Rizzo, P.; Rizzo, D.; Gallus, R.; Delogu, G.; Morbini, P.; Tommasino, M. HPV as a marker for molecular characterization in head and neck oncology: Looking for a standardization of clinical use and of detection method(s) in clinical practice. Head Neck 2019, 41, 1104–1111. [Google Scholar] [CrossRef]
- El-Naggar, A.K.; Westra, W.H. p16 expression as a surrogate marker for HPV−related oropharyngeal carcinoma: A guide for interpretative relevance and consistency. Head Neck 2012, 34, 459–461. [Google Scholar] [CrossRef]
- Bussu, F.; Sali, M.; Gallus, R.; Vellone, V.G.; Zannoni, G.F.; Autorino, R.; Dinapoli, N.; Santangelo, R.; Martucci, R.; Graziani, C.; et al. HPV infection in squamous cell carcinomas arising from different mucosal sites of the head and neck region. Is p16 immunohistochemistry a reliable surrogate marker? Br. J. Cancer 2013, 108, 1157–1162. [Google Scholar] [CrossRef] [PubMed]
- Nauta, I.H.; Rietbergen, M.M.; van Bokhoven, A.; Bloemena, E.; Lissenberg-Witte, B.I.; Heideman, D.A.M.; de Jong, R.J.B.; Brakenhoff, R.H.; Leemans, C.R. Evaluation of the eighth TNM classification on p16-positive oropharyngeal squamous cell carcinomas in the Netherlands and the importance of additional HPV DNA testing. Ann. Oncol. 2018, 29, 1273–1279. [Google Scholar] [CrossRef] [PubMed]
- Mariz, B.A.L.A.; Kowalski, L.P.; William, W.N., Jr.; de Castro, G., Jr.; Chaves, A.L.F.; Santos, M.; de Oliveira, T.B.; Araújo, A.L.D.; Normando, A.G.C.; Ribeiro, A.C.P.; et al. Global prevalence of human papillomavirus-driven oropharyngeal squamous cell carcinoma following the ASCO guidelines: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2020, 156, 103116. [Google Scholar] [CrossRef] [PubMed]
- Anantharaman, D.; Abedi-Ardekani, B.; Beachler, D.C.; Gheit, T.; Olshan, A.F.; Wisniewski, K.; Wunsch-Filho, V.; Toporcov, T.N.; Tajara, E.H.; Levi, J.E.; et al. Geographic heterogeneity in the prevalence of human papillomavirus in head and neck cancer. Int. J. Cancer 2017, 140, 1968–1975. [Google Scholar] [CrossRef] [Green Version]
- Carlander, A.; Jakobsen, K.; Bendtsen, S.; Garset-Zamani, M.; Lynggaard, C.; Jensen, J.; Grønhøj, C.; Buchwald, C. A Contemporary Systematic Review on Repartition of HPV−Positivity in Oropharyngeal Cancer Worldwide. Viruses 2021, 9, 1326. [Google Scholar] [CrossRef]
- Stein, A.P.; Saha, S.; Kraninger, J.L.; Swick, A.D.; Yu, M.; Lambertg, P.F.; Kimple, R. Prevalence of Human Papillomavirus in Oropharyngeal Cancer: A Systematic Review. Cancer J. 2015, 21, 138–146. [Google Scholar] [CrossRef] [Green Version]
- Castellsagué, X.; Mena, M.; Alemany, L. Epidemiology of HPV−Positive Tumors in Europe and in the World. Recent Results Cancer Res. 2017, 6, 27–35. [Google Scholar]
- Bussu, F.; Muresu, N.; Crescio, C.; Gallus, R.; Rizzo, D.; Cossu, A.; Sechi, I.; Fedeli, M.; Cossu, A.; Delogu, G.; et al. Low Prevalence of HPV Related Oropharyngeal Carcinogenesis in Northern Sardinia. Cancers 2022, 14, 4205. [Google Scholar] [CrossRef]
- Prigge, E.S.; Arbyn, M.; von Knebel Doeberitz, M.; Reuschenbach, M. Diagnostic accuracy of p16(INK4a) immunohistochemistry in oropharyngeal squamous cell carcinomas: A systematic review and meta-analysis. Int. J. Cancer 2017, 140, 1186–1198. [Google Scholar] [CrossRef] [Green Version]
- Ford, S.E.; Brandwein-Gensler, M.; Carroll, W.R.; Rosenthal, E.L.; Magnuson, J.S. Transoral robotic versus open surgical approaches to oropharyngeal squamous cell carcinoma by human papillomavirus status. Otolaryngol. Head Neck Surg. 2014, 151, 606–611. [Google Scholar] [CrossRef]
- Ling, D.C.; Chapman, B.V.; Kim, J.; Choby, G.W.; Kabolizadeh, P.; Clump, D.A.; Ferris, R.L.; Kim, S.; Beriwal, S.; Heron, D.E.; et al. Oncologic outcomes and patient-reported quality of life in patients with oropharyngeal squamous cell carcinoma treated with definitive transoral robotic surgery versus definitive chemoradiation. Oral Oncol. 2016, 61, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Kass, J.I.; Giraldez, L.; Gooding, W.; Choby, G.; Kim, S.; Miles, B.; Teng, M.; Sikora, A.G.; Johnson, J.T.; Myers, E.N.; et al. Oncologic outcomes of surgically treated early-stage oropharyngeal squamous cell carcinoma. Head Neck 2016, 38, 1467–1471. [Google Scholar] [CrossRef] [PubMed]
- Gillison, M.L.; Koch, W.M.; Capone, R.B.; Spafford, M.; Westra, W.H.; Wu, L.; Zahurak, M.L.; Daniel, R.W.; Viglione, M.; Symer, D.E.; et al. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J. Natl. Cancer Instig. 2000, 92, 709–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stransky, N.; Egloff, A.M.; Tward, A.D.; Kostic, A.D.; Cibulskis, K.; Sivachenko, A.; Kryukov, G.V.; Lawrence, M.S.; Sougnez, C.; McKenna, A.; et al. The mutational landscape of head and neck squamous cell carcinoma. Science 2011, 333, 1157–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiotto, M.T.; Taniguchi, C.M.; Klopp, A.H.; Colbert, L.E.; Lin, S.H.; Wang, L.; Frederick, M.J.; Osman, A.A.; Pickering, C.R.; Frank, S.J. Biology of the Radio- and Chemo-Responsiveness in HPV Malignancies. Semin. Radiat. Oncol. 2021, 31, 274–285. [Google Scholar] [CrossRef]
- Palma, D.A.; Prisman, E.; Berthelet, E.; Tran, E.; Hamilton, S.; Wu, J.; Eskander, A.; Higgins, K.; Karam, I.; Poon, I.; et al. Assessment of Toxic Effects and Survival in Treatment Deescalation With Radiotherapy vs. Transoral Surgery for HPV−Associated Oropharyngeal Squamous Cell Carcinoma: The ORATOR2 Phase 2 Randomized Clinical Trial. JAMA Oncol. 2022, 8, 845–851. [Google Scholar] [CrossRef]
- Marur, S.; D’Souza, G.; Westra, W.H.; Forastiere, A.A. HPV−associated head and neck cancer: A virus-related cancer epidemic. Lancet Oncol. 2010, 11, 781–789. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.M.; Kim, W.S.; Byeon, H.K.; De Virgilio, A.; Lee, S.Y.; Kim, S.H. Clinical outcomes of transoral robotic surgery for head and neck tumors. Ann. Otol. Rhinol. Laryngol. 2013, 122, 73–84. [Google Scholar] [CrossRef]
- Owadally, W.; Hurt, C.; Timmins, H.; Parsons, E.; Townsend, S.; Patterson, J.; Hutcheson, K.; Powell, N.; Beasley, M.; Palaniappan, N.; et al. PATHOS: A phase II/III trial of risk-stratified, reduced intensity adjuvant treatment in patients undergoing transoral surgery for Human papillomavirus (HPV) positive oropharyngeal cancer. BMC Cancer 2015, 15, 602. [Google Scholar] [CrossRef] [Green Version]
- Hargreaves, S.; Beasley, M.; Hurt, C.; Jones, T.M.; Evans, M. Deintensification of Adjuvant Treatment After Transoral Surgery in Patients With Human Papillomavirus-Positive Oropharyngeal Cancer: The Conception of the PATHOS Study and Its Development. Front. Oncol. 2019, 9, 936. [Google Scholar] [CrossRef]


{kind=link}
| Authors | Study Design | No. of Patients Treated with TORS (Male) | Mean Age (Range) | HPV Status | HPV Detection Method | Smoking Status | Overall AJCC Tumor Stage | OS | DFS |
|---|---|---|---|---|---|---|---|---|---|
| Cohen et al., 2010 [32] | P | 50 (47) | HPV− 62.8 (48.8–73.8); HPV+ 56.5 (36.8–76.5) | HPV+, n = 37; HPV−, n = 13. | HPV DNA (PCR based) | N/A | HPV−: I = 1, 7.7%; II = 2, 15.4%; III = 6, 46.2%; IV = 4, 30.8%; HPV+: I = 2, 5.4%; II = 2, 5.4%; III = 14, 37.8%; IV = 19, 51.4% | 1-year: Overall, 95.7%; HPV+, 97.2%; HPV−, 90.9%. 2-year: Overall, 80.6%; HPV+, 81%; HPV−, 80% | 1-year: Overall, 97.8%; HPV+, 97.2%; HPV−, 100%. 2-year: Overall, 92.6%; HPV+, 89.5%; HPV−, 100% |
| Blanco et al., 2013 [33] | R | 30 | 52.4 (18–80) | HPV+, n = 23; HPV−, n = 7. | N/A | N/A | NA | 2-year: Overall, 93%; HPV+, 96%; HPV−, 86% | 2-year: Overall, 87%; HPV+, 91%; HPV−, 71.4% |
| Smith et al., 2015 [29] | P | 42 (34) | 62.2 (41–88) | HPV+, n = 28; HPV−, n = 12; unknown, n = 2. | HPV DNA (PCR based) or p16 IHC | 6 (14%) never; 4 (10%) < 10 pack-years; 32 (76%) > 10 pack-years | I = 5, 12%; II = 9, 21%; III = 4, 10%; IV = 24, 57% | 5-year: 83% | N/A |
| Cannon et al., 2018 [34] | R | 88 (80) | 58.3 (36–77) | HPV+, n = 88. | p16 IHC | 30 (34%) 10+ pack-year | I = 2, 2%; II, 4, 5%; III = 13, 15%; IV = 69, 78% | 2-year: 100% | 2-year: 95% |
| Moore et al., 2018 [30] | R | 314 (280) | 58 (51–63) | HPV+, n = 286; HPV−, n = 23; unknown, n = 5. | HPV ISH or p16 IHC | 149 (47%) never; 129 (41) former; 36 (11%) current | I = 15, 5%; II = 19, 6%; III = 27, 9%; IV = 253, 81% | 1-year: 98%. 3-year: 91%. 5-year: 86% | N/A |
| Dabas et al., 2019 [35] | P | 153 (96) | 56.3 (32–87) | HPV−, n = 153. | p16 IHC | 137 (89.5%) | I = 0, 0%; II = 11, 7.2%; III = 56, 36.6%; IV = 86, 56.2% | 4-year: 91.5% | 4-year: 96.5% |
| Nichols et al., 2019 [31] | P | 34 (28) | 58.1 (52.6–64.5) | HPV+ = 30; HPV− = 4. | p16 IHC | 21 (62%) former or current | I-II = 34, 100% | 3-year: 85.3% | N/A |
| Dhanireddy et al., 2019 [36] | R | 65 (48) | 61 (41–83) | HPV+, n = 52; HPV−, n = 10; unknown, n = 3. | p16 IHC | 23 (35%) former; 22 (33.5%) current | N/A | 2-year: 82.3%. 5-year: 70.2%. | N/A |
| Gershowitz et al., 2019 [40] | R | 123 (107) | 58 (36–83) | HPV+, n = 123 (100%) | p16 IHC | 116 (94%) nonsmoker; 7 (6%) current smoker | N/A | 3-year: 94% | N/A |
| Meccariello et al., 2019 [37] | R | 60 | N/A | HPV+, n = 33; HPV−, n = 27. | p16 IHC | N/A | N/A | 5-year: Overall, 77.6%; HPV+, 88.2% | 5-year: Overall, 85.2%; HPV+, 93.6% |
| Swisher-McClure et al., 2019 [49] | P | 60 (50) | 57 (34-84) | HPV+, n = 60 (100%) | p16 IHC | 32 (53%) Never | N/A | 2-year: 100% | N/A |
| Parhar et al., 2021a [44] | R | 295 (247) | 57.9 (N/A) | HPV+, n = 295 (100%) | N/A | 134 (45.4%) Never-smoker; 63 (21.4%) <10 p/y; 98 (33.2) >10 p/y | I = 227, 77%; II = 62, 21%; III = 6, 2% | 2-year: 95.5%; 5-year: 90.1% | 2-year: 90%; 5-year: 84.7% |
| Carey et al., 2021 [39] | R | 541 (469) | 59,1 | HPV+, n = 541 (100%) | p16 IHC | 176 (33.1%) Never; 110 (20.7%) <10 p/y; 245 (46.1%) >10 p/y | N/A | 5-year: 92.2% (no adjuvant therapy), 93.5% (adjuvant radiation), 92.0% (adjuvant chemoradiation) | 5-year: 83.4% (no adjuvant therapy), 88.2% (adjuvant radiation), 85.1% (adjuvant chemoradiation) |
| Holcomb et al., 2021 [41] | R | 99 (82) | 60.9 (N/A) | HPV+, n = 99 (100%) | p16 IHC or high risk HPV DNA | 45 (45.4) Never smoker; 41 (41.4) former smoker; 12 (12.1) current smoker | I = 94, 94.9%; II = 5, 5.1% | 1-year: 97.3%; 2-year: 95.7%; 3-year: 87.8% | 1-year: 94.6%; 2-year: 83.7%; 3-year: 72.4% |
| Nichols et al., 2021 [42] | R | 48 (40) | 61.2 (40.0–79.3) | HPV+, n = 48 (100%) | N/A | 24 (50%) Non-smoker; 24 (50%) current smoker | 0 = 1, 2%; I = 43, 89.6%; II = 1, 2%; III = 3, 6.3% | 5-year: 95% | N/A |
| O’Hara et al., 2021 [43] | R | 120 (91) | 58 | HPV+, n = 107 (89%); HPV -, n = 13 (11%) | p16 IHC + HPV ISH | 92 (77%) Never; 24 (19%) Current; 4 (3%) Former | I = 100, 83%; II = 12, 10%; III = 2, 2%; IV = 6, 5% | 3-year: 85% (whole cohort); 88% (HPV+) | N/A |
| Parhar et al., 2021b [45] | R | 56 (40) | 62.0 (56.0–69.0) | HPV−, n = 56 (100%) | p16 IHC | 9 (16.1%) Never-smoker; 6 (10.7%) <10 p/y; 41 (73.2%) >10 p/y | I = 4, 7.1%; II = 1, 1.8%, III = 18, 32.1%; IV = 33, 58.9% | 3-year: 85.5% | 3-year: 73.6% |
| Philips et al., 2021 [46] | R | 342 (290) | 61 (N/A) | HPV+, n = 342 (100%) | N/A | 140 (40.9%) Never-smoker; 171 (50.0%) former-smoker; 31 (9.1%) current-smoker | N/A | 2-year: 96.1% | 2-year: 91.5% |
| Sahovaler et al., 2021 [47] | R | 32 (23) | 57.9 (37.1–74.1) | HPV+, n = 23 (71.9%); HPV−, n = 9 (28.1%) | p16 IHC | 8 (25%) Never-smoker; 17 (53%) current-smoker; 7 (22%) former-smoker | N/A | 3-year: 96%; HPV+ 95%; HPV− 100% | N/A |
| Sun et al., 2021 [48] | R | 178 (156) | 59 (53–64) | HPV+, n = 178 (100%) | p16 IHC | 79 (44.4%) Never-smoker; 42 (23.6%) <10 p/y; 57 (32%) >10 p/y | I = 106, 59.6%; II = 68, 38.2%; III = 4, 2.2% | 5-year: 93.6% | N/A |
| Yver et al., 2021 [50] | R | 628 (540) | 60 (32–89) | HPV+, n = 628 (100%) | p16 IHC | 282 (44.9%) Never-smoker; 129 (20.5%) <10 p/y; 206 (32.8%) >10 p/y; 11 81.8%) unknown | I = 492, 78.3%; II = 130, 20.7%; III = 6, 1% | 5-year: 91% | N/A |
| Brody et al., 2022 [38] | R | 634 (546) | 60 (32–89) | HPV+, n = 634 (100%) | p16 IHC | 288 (46.2) Never; 129 (20.7) <10 p/y; 206 (33.1) >10 p/y | I = 494, 77.9%; II = 133, 21%; III = 7, 1.1% | 5-year: 91.2% | N/A |
| Author, Year | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| Blanco et al., 2013 [33] | No | Yes | Yes | Yes | No | Yes | Yes | Yes |
| Brody et al., 2022 [38] | No | Yes | No | Yes | No | Yes | Yes | Yes |
| Cannon et al., 2018 [34] | No | Yes | Yes | Yes | No | No | Yes | Yes |
| Carey et al., 2021 [39] | No | Yes | Yes | Yes | No | No | Yes | Yes |
| Cohen et al., 2011 [32] | No | Yes | Yes | Yes | Yes | No | Yes | Yes |
| Dabas et al., 2019 [35] | No | Yes | Yes | Yes | Yes | No | Yes | No |
| Dhanireddy et al., 2019 [36] | No | Yes | Yes | Yes | No | No | Yes | No |
| Gershowitz et al., 2019 [40] | No | Yes | Yes | Yes | No | No | Yes | Yes |
| Holcomb et al., 2021 [41] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes |
| Meccariello et al., 2019 [37] | No | Yes | Yes | Yes | No | Yes | Yes | Yes |
| Moore et al., 2018 [30] | No | Yes | Yes | Yes | No | Yes | Yes | No |
| Nichols et al., 2019 [31] | Yes | Yes | Yes | Yes | Yes | No | Yes | No |
| Nichols et al., 2021 [42] | No | Yes | Yes | Yes | No | Yes | Yes | Yes |
| O’Hara et al., 2021 [43] | No | Yes | Yes | Yes | No | Yes | Yes | Yes |
| Parhar et al., 2021a [44] | No | Yes | Yes | Yes | No | No | Yes | Yes |
| Parhar et al., 2021b [45] | No | Yes | Yes | Yes | No | No | Yes | Yes |
| Philips et al., 2021 [46] | No | Yes | Yes | Yes | No | No | Yes | Yes |
| Sahovaler et al., 2021 [47] | No | Yes | Yes | Yes | No | No | Yes | Yes |
| Smith et al., 2015 [29] | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Sun et al., 2021 [48] | No | Yes | Yes | Yes | No | Yes | Yes | Yes |
| Swisher-McClure et al., 2019 [49] | No | Yes | Yes | Yes | Yes | No | Yes | No |
| Yver et al., 2021 [50] | No | Yes | Yes | Yes | No | No | Yes | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Virgilio, A.; Costantino, A.; Rizzo, D.; Crescio, C.; Gallus, R.; Spriano, G.; Mercante, G.; Festa, B.M.; Accorona, R.; Pignataro, L.; et al. Do We Have Enough Evidence to Specifically Recommend Transoral Robotic Surgery in HPV−Driven Oropharyngeal Cancer? A Systematic Review. Pathogens 2023, 12, 160. https://doi.org/10.3390/pathogens12020160
De Virgilio A, Costantino A, Rizzo D, Crescio C, Gallus R, Spriano G, Mercante G, Festa BM, Accorona R, Pignataro L, et al. Do We Have Enough Evidence to Specifically Recommend Transoral Robotic Surgery in HPV−Driven Oropharyngeal Cancer? A Systematic Review. Pathogens. 2023; 12(2):160. https://doi.org/10.3390/pathogens12020160
Chicago/Turabian StyleDe Virgilio, Armando, Andrea Costantino, Davide Rizzo, Claudia Crescio, Roberto Gallus, Giuseppe Spriano, Giuseppe Mercante, Bianca Maria Festa, Remo Accorona, Lorenzo Pignataro, and et al. 2023. "Do We Have Enough Evidence to Specifically Recommend Transoral Robotic Surgery in HPV−Driven Oropharyngeal Cancer? A Systematic Review" Pathogens 12, no. 2: 160. https://doi.org/10.3390/pathogens12020160