
Characterization of Bacterial Differences Induced by Cleft-Palate-Related Spatial Heterogeneity

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
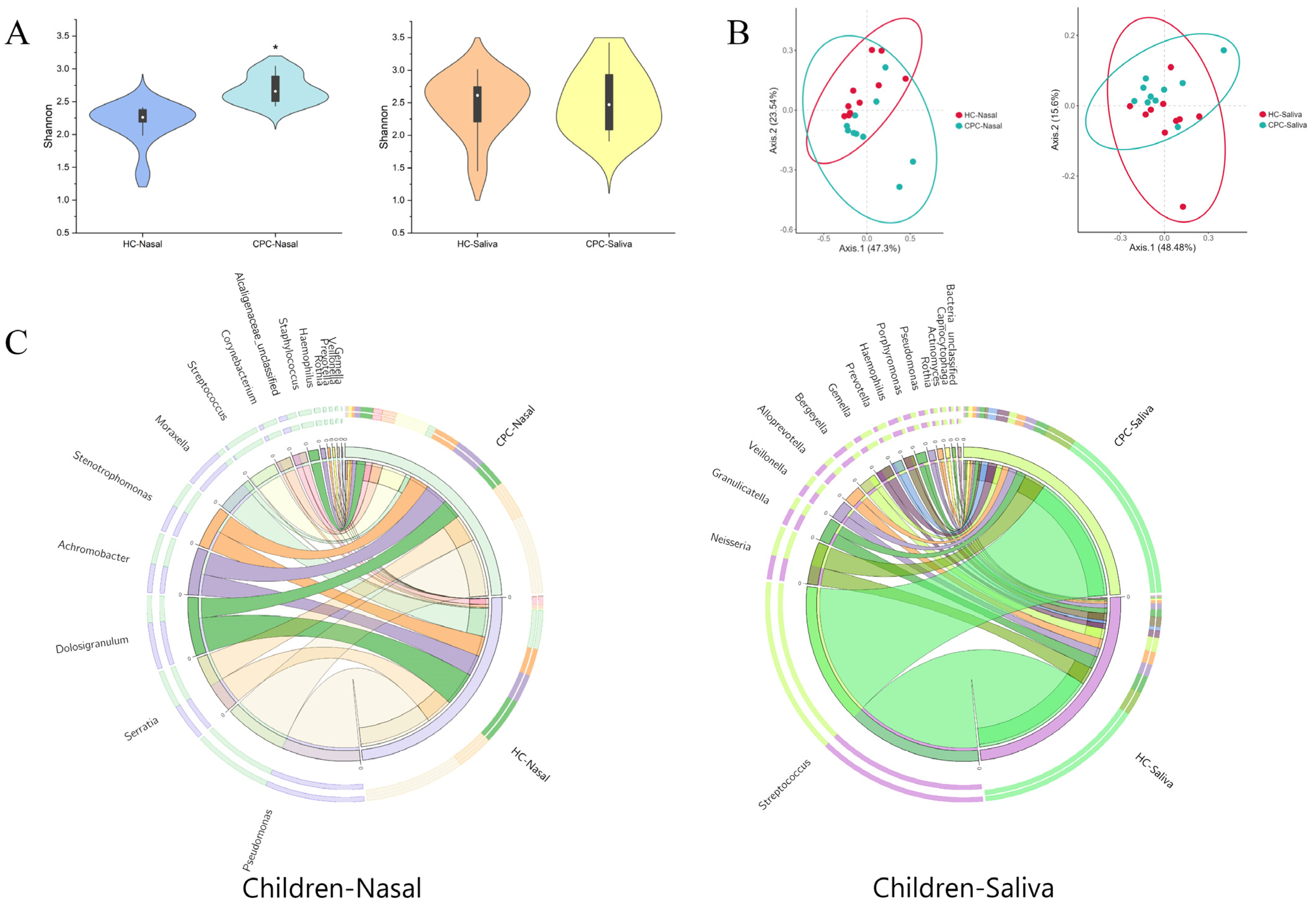
2.1. Differences in Oral and Nasal Bacterial Communities between Healthy and CP Children
2.1.1. Effect of CP on Nasal Bacteria in Children Was Greater than That of Oral Bacteria
2.1.2. Cleft Palate Changed the Composition of Oral and Nasal Flora in Children
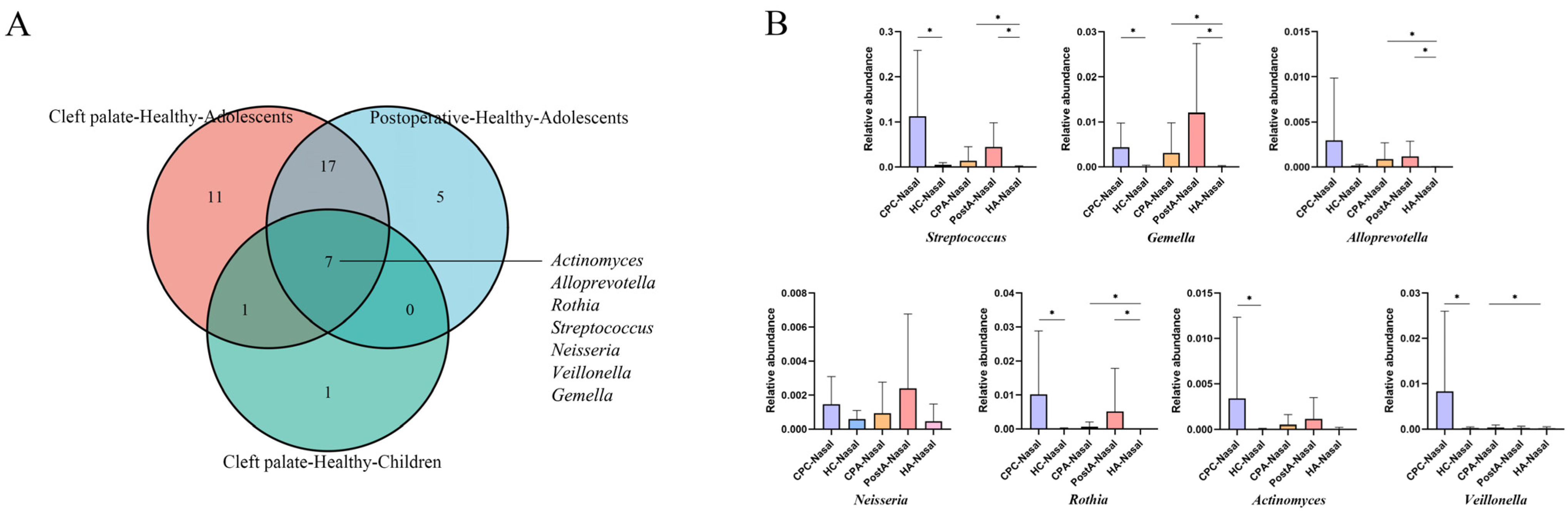
2.2. Differences in Oral and Nasal Bacterial Communities between Healthy, CP, and Postoperative Adolescents
2.2.1. The Bacteria of Postoperative Adolescents Were Similar to CP Adolescents
2.2.2. Taxonomic Composition of Nasal and Oral Bacterial Communities in CP, Postoperative, and Healthy Adolescents
2.3. Oral–Nasal Bacterial Translocation in CP Patients
3. Discussion
4. Materials and Methods
4.1. Study Design and Procedures
4.2. Sample Collection
4.3. DNA Extraction and 16S rRNA Gene Amplicon Sequencing
4.4. Bioinformatics Analysis and Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shkoukani, M.A.; Chen, M.; Angela, V. Cleft lip—A comprehensive review. Front. Pediatrics 2013, 1, 53. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Yoshioka, E.; Saijo, Y.; Miyamoto, T.; Azuma, H.; Tanahashi, Y.; Ito, Y.; Kobayashi, S.; Minatoya, M.; Bamai, Y.A.; et al. Lower respiratory tract infections and orofacial clefts: A prospective cohort study from the Japan Environment and Children’s Study. J. Epidemiol. 2022, 32, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Fauroux, B.; Hascoët, J.-M.; Jarreau, P.-H.; Magny, J.-F.; Rozé, J.-C.; Saliba, E.; Schwarzinger, M. Risk factors for bronchiolitis hospitalization in infants: A French nationwide retrospective cohort study over four consecutive seasons (2009–2013). PLoS ONE 2020, 15, e0229766. [Google Scholar] [CrossRef]
- Durhan, M.A.; Topcuoglu, N.; Kulekci, G.; Ozgentas, E.; Tanboga, I. Microbial profile and dental caries in cleft lip and palate babies between 0 and 3 years old. Cleft Palate-Craniofacial J. 2018, 56, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Ahluwalia, M.; Brailsford, S.R.; Tarelli, E.; Gilbert, S.C.; Clark, D.T.; Barnard, K.; Beighton, D. Dental caries, oral hygiene, and oral clearance in children with craniofacial disorders. J. Dent. Res. 2004, 83, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Kirchberg, A.; Treide, A.; Hemprich, A. Investigation of caries prevalence in children with cleft lip, alveolus, and palate. J. Cranio-Maxillofac. Surg. 2004, 32, 216–219. [Google Scholar] [CrossRef]
- Antonarakis, G.S.; Palaska, P.K.; Herzog, G. Caries prevalence in non-syndromic patients with cleft lip and/or palate: A meta-analysis. Caries Res. 2013, 47, 406–413. [Google Scholar] [CrossRef]
- Sundell, A.L.; Ullbro, C.; Marcusson, A.; Twetman, S. Comparing caries risk profiles between 5- and 10- year-old children with cleft lip and/or palate and non-cleft controls. BMC Oral Health 2015, 15, 85. [Google Scholar] [CrossRef]
- Perdikogianni, H.; Papaioannou, W.; Nakou, M.; Oulis, C.; Papagiannoulis, L. Periodontal and microbiological parameters in children and adolescents with cleft lip and/or palate. Int. J. Paediatr. Dent. 2009, 19, 455–467. [Google Scholar] [CrossRef]
- Costa, B.; De Oliveira Lima, J.E.; Gomide, M.R.; Da Silva Rosa, O.P. Clinical and microbiological evaluation of the periodontal status of children with unilateral complete cleft lip and palate. Cleft Palate-Craniofacial J. 2003, 40, 585–589. [Google Scholar] [CrossRef]
- Zhang, M.; Wang, R.; Liao, Y.; Buijs, M.J.; Li, J. Profiling of oral and nasal microbiome in children with cleft palate. Cleft Palate-Craniofacial J. 2016, 53, 332–338. [Google Scholar] [CrossRef]
- Machorowska-Pieniążek, A.; Mertas, A.; Skucha-Nowak, M.; Tanasiewicz, M.; Morawiec, T. A comparative study of oral microbiota in infants with complete cleft lip and palate or cleft soft palate. BioMed Res. Int. 2017, 2017, 1460243. [Google Scholar] [CrossRef] [PubMed]
- Farronato, G.; Cannalire, P.; Martinelli, G.; Tubertini, I.; Giannini, L.; Galbiati, G.; Maspero, C. Cleft lip and/or palate: Review. Minerva Stomatol. 2014, 63, 111–126. [Google Scholar] [PubMed]
- Haange, S.-B.; Jehmlich, N.; Krügel, U.; Hintschich, C.; Wehrmann, D.; Hankir, M.; Seyfried, F.; Froment, J.; Hübschmann, T.; Müller, S.; et al. Gastric bypass surgery in a rat model alters the community structure and functional composition of the intestinal microbiota independently of weight loss. Microbiome 2020, 8, 13. [Google Scholar] [CrossRef] [PubMed]
- Roode, G.; Bütow, K.-W.; Naidoo, S. Preoperative evaluation of micro-organisms in non-operated cleft in soft palate: Impact on use of antibiotics. Br. J. Oral Maxillofac. Surg. 2017, 55, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Shaal, R.; Anil, M. The spectrum of intraoral bacteria seen in patients with cleft palates in an African setting. Microbiologyopen 2018, 8, e00679. [Google Scholar]
- Sundell, A.L.; Ullbro, C.; Dahlén, G.; Marcusson, A.; Twetman, S. Salivary microbial profiles in 5-year old children with oral clefts: A comparative study. Eur. Arch. Paediatr. Dent. 2018, 19, 57–60. [Google Scholar] [CrossRef]
- Funahashi, K.; Shiba, T.; Watanabe, T.; Muramoto, K.; Takeuchi, Y.; Ogawa, T.; Izumi, Y.; Sekizaki, T.; Nakagawa, I.; Moriyama, K. Functional dysbiosis within dental plaque microbiota in cleft lip and palate patients. Prog. Orthod. 2019, 20, 11. [Google Scholar] [CrossRef]
- Cocco, J.F.; Antonetti, J.W.; Burns, J.L.; Heggers, J.P.; Blackwell, S.J. Characterization of the nasal, sublingual, and oropharyngeal mucosa microbiota in cleft lip and palate individuals before and after surgical repair. Cleft Palate-Craniofacial J. 2010, 47, 151. [Google Scholar] [CrossRef]
- Takemura, H.; Yasumoto, K.; Toi, T.; Hosoyamada, A. Correlation of cleft type with incidence of perioperative respiratory complications in infants with cleft lip and palate. Pediatric Anesth. 2010, 12, 585–588. [Google Scholar] [CrossRef]
- Moore, M.D.; Lawrence, W.T.; Ptak, J.J.; Trier, W.C. Complications of primary palatoplasty: A twenty-one-year review. Cleft Palate J. 1988, 25, 156–162. [Google Scholar] [PubMed]
- Gaiser, R.A.; Halimi, A.; Alkharaan, H.; Lu, L.; Davanian, H.; Healy, K.; Hugerth, L.W.; Ateeb, Z.; Valente, R.; Moro, C.F.; et al. Enrichment of oral microbiota in early cystic precursors to invasive pancreatic cancer. Gut 2019, 68, 2186–2194. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.W.; Wang, X. Mobile microbiome: Oral bacteria in extra-oral infections and inflammation. J. Dent. Res. 2013, 92, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Zaura, E.; Keijser, B.J.F.; Huse, S.M.; Crielaard, W. Defining the healthy “core microbiome” of oral microbial communities. BMC Microbiol. 2009, 9, 259. [Google Scholar] [CrossRef] [PubMed]
- Lemon, K.P.; Klepac-Ceraj, V.; Schiffer, H.K.; Brodie, E.L.; Lynch, S.V.; Kolter, R. Comparative analyses of the bacterial microbiota of the human nostril and oropharynx. mBio 2010, 1, e00129-10. [Google Scholar] [CrossRef]
- Proctor, D.; Relman, D.A. The landscape ecology and microbiota of the human nose, mouth, and throat. Cell Host Microbe 2017, 21, 421–432. [Google Scholar] [CrossRef]
- Mony, C.; Vandenkoornhuyse, P.; Bohannan, B.J.M.; Peay, K.; A Leibold, M. A landscape of opportunities for microbial ecology research. Front. Microbiol. 2020, 11, 561427. [Google Scholar] [CrossRef]
- Charlotte, T.; Norbert, S.; Bastian, O. The microbiota inpneumonia: From protection to predisposition. Sci. Transl. Med. 2021, 13, eaba0501. [Google Scholar]
- Zhou, Y.; Gao, H.; Mihindukulasuriya, K.A.; La Rosa, P.S.; Wylie, K.M.; Vishnivetskaya, T.; Podar, M.; Warner, B.; Tarr, P.I.; Nelson, D.E.; et al. Biogeography of the ecosystems of the healthy human body. Genome Biol. 2013, 14, R1. [Google Scholar] [CrossRef]
- Teo, S.M.; Mok, D.; Pham, K.; Kusel, M.; Serralha, M.; Troy, N.; Holt, B.J.; Hales, B.J.; Walker, M.L.; Hollams, E.; et al. The infant nasopharyngeal microbiome impacts severity of lower respiratory infection and risk of asthma development. Cell Host Microbe 2015, 17, 704–715. [Google Scholar] [CrossRef]
- Gibson, M.K.; Crofts, T.S.; Dantas, G. Antibiotics and the developing infant gut microbiota and resistome. Curr. Opin. Microbiol. 2015, 27, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, Z.; Ma, X.; Du, L.; Jia, Z.; Cui, X.; Yu, L.; Yang, J.; Xiao, L.; Zhang, B.; et al. Translocation of vaginal microbiota is involved in impairment and protection of uterine health. Nat. Commun. 2021, 12, 4191. [Google Scholar] [CrossRef]
- McPherson, A.C.; Pandey, S.P.; Bender, M.J.; Meisel, M. Systemic immunoregulatory consequences of gut commensal translocation. Trends Immunol. 2021, 42, 95. [Google Scholar] [CrossRef] [PubMed]
- Tsang, T.K.; Lee, K.H.; Foxman, B.; Balmaseda, A.; Gresh, L.; Sanchez, N.; Ojeda, S.; Lopez, R.; Yang, Y.; Kuan, G.; et al. Association Between the Respiratory Microbiome and Susceptibility to Influenza Virus Infection. Clin. Infect. Dis. 2020, 71, 1195–1203. [Google Scholar] [CrossRef] [PubMed]
- Yuan, B.-C.; Yeh, Y.-T.; Lin, C.-C.; Huang, C.-H.; Liu, H.-C.; Chiang, C.-P. Clinical detection of chronic rhinosinusitis through next-generation sequencing of the oral microbiota. Microorganisms 2020, 8, 959. [Google Scholar] [CrossRef] [PubMed]
- Laufer, A.S.; Metlay, J.P.; Gent, J.F.; Fennie, K.; Kong, Y.; Pettigrew, M.M. Microbial Communities of the Upper Respiratory Tract and Otitis Media in Children. mBio 2011, 2, e00245-10. [Google Scholar] [CrossRef]
- Dao, A.M.; Goudy, S.L. Cleft palate repair, gingivoperiosteoplasty, and alveolar bone grafting. Facial Plast. Surg. Clin. 2016, 24, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Arief, E.M.; Mohamed, Z.; Idris, F.M. Study of viridans streptococci and staphylococcus species in cleft lip and palate patients before and after surgery. Cleft Palate-Craniofacial J. 2005, 42, 277–279. [Google Scholar] [CrossRef]
- Stearns, J.C.; Davidson, C.J.; McKeon, S.; Whelan, F.J.; Fontes, M.E.; Schryvers, A.B.; Bowdish, D.M.E.; Kellner, J.D.; Surette, M.G. Culture and molecular-based profiles show shifts in bacterial communities of the upper respiratory tract that occur with age. ISME J. 2015, 9, 1246–1259. [Google Scholar] [CrossRef] [PubMed]
- Lear, L.; Padfield, D.; Dowsett, T.; Jones, M.; Kay, S.; Hayward, A.; Vos, M. Bacterial colonisation dynamics of household plastics in a coastal environment. Sci. Total Environ. 2022, 838, 156199. [Google Scholar] [CrossRef]
- Sarkar, P.; Malik, S.; Laha, S.; Das, S.; Bunk, S.; Ray, J.G.; Chatterjee, R.; Saha, A. Dysbiosis of Oral Microbiota During Oral Squamous Cell Carcinoma Development. Front. Oncol. 2021, 11, 614448. [Google Scholar] [CrossRef] [PubMed]
- Roh, W.S.; Chung, K.B.; Kim, D.Y. Recent emergence of Serratia marcescens in dermatology: Retrospective observations based on clinical outpatient data. Eur. J. Dermatol. 2022, 32, 94–98. [Google Scholar] [CrossRef]
- Rueca, M.; Fontana, A.; Bartolini, B.; Piselli, P.; Mazzarelli, A.; Copetti, M.; Binda, E.; Perri, F.; Gruber, C.; Nicastri, E.; et al. Investigation of Nasal/Oropharyngeal Microbial Community of COVID-19 Patients by 16S rDNA Sequencing. Int. J. Environ. Res. Public Health 2021, 18, 2174. [Google Scholar] [CrossRef] [PubMed]
- Zhou, K.; Sun, F.; Xu, X.-L.; Hao, X.-K.; Liu, J.-Y. Prevalences and characteristics of cultivable nasal bacteria isolated from preclinical medical students. J. Int. Med. Res. 2020, 48, 0300060520961716. [Google Scholar] [CrossRef] [PubMed]
- Habibi, N.; Mustafa, A.S.; Khan, M.W. Composition of nasal bacterial community and its seasonal variation in health care workers stationed in a clinical research laboratory. PLoS ONE 2021, 16, e0260314. [Google Scholar] [CrossRef] [PubMed]
- MacKenzie, B.W.; Chang, K.; Zoing, M.; Jain, R.; Hoggard, M.; Biswas, K.; Douglas, R.G.; Taylor, M.W. Longitudinal study of the bacterial and fungal microbiota in the human sinuses reveals seasonal and annual changes in diversity. Sci. Rep. 2019, 9, 17416. [Google Scholar] [CrossRef]
- De Boeck, I.; Wittouck, S.; Wuyts, S.; Oerlemans, E.F.M.; van den Broek, M.F.L.; Vandenheuvel, D.; Vanderveken, O.; Lebeer, S. Comparing the Healthy Nose and Nasopharynx Microbiota Reveals Continuity As Well As Niche-Specificity. Front. Microbiol. 2017, 8, 2372. [Google Scholar] [CrossRef]
- Glenn, T.C. Field guide to next-generation DNA sequencers. Mol. Ecol. Resour. 2011, 11, 759–769. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, F.; Su, Z.; Li, Q.; Wang, R.; Liao, Y.; Zhang, M.; Li, J. Characterization of Bacterial Differences Induced by Cleft-Palate-Related Spatial Heterogeneity. Pathogens 2022, 11, 771. https://doi.org/10.3390/pathogens11070771
Zhou F, Su Z, Li Q, Wang R, Liao Y, Zhang M, Li J. Characterization of Bacterial Differences Induced by Cleft-Palate-Related Spatial Heterogeneity. Pathogens. 2022; 11(7):771. https://doi.org/10.3390/pathogens11070771
Chicago/Turabian StyleZhou, Fangjie, Zhifei Su, Qinyang Li, Renke Wang, Ying Liao, Min Zhang, and Jiyao Li. 2022. "Characterization of Bacterial Differences Induced by Cleft-Palate-Related Spatial Heterogeneity" Pathogens 11, no. 7: 771. https://doi.org/10.3390/pathogens11070771