
Diagnostic Laboratory Characteristics of COVID-19 Patients Infected by Fomites: COVID-19 Outbreak in a South Korean Public Administrative Facility


Abstract
:1. Introduction
2. Results
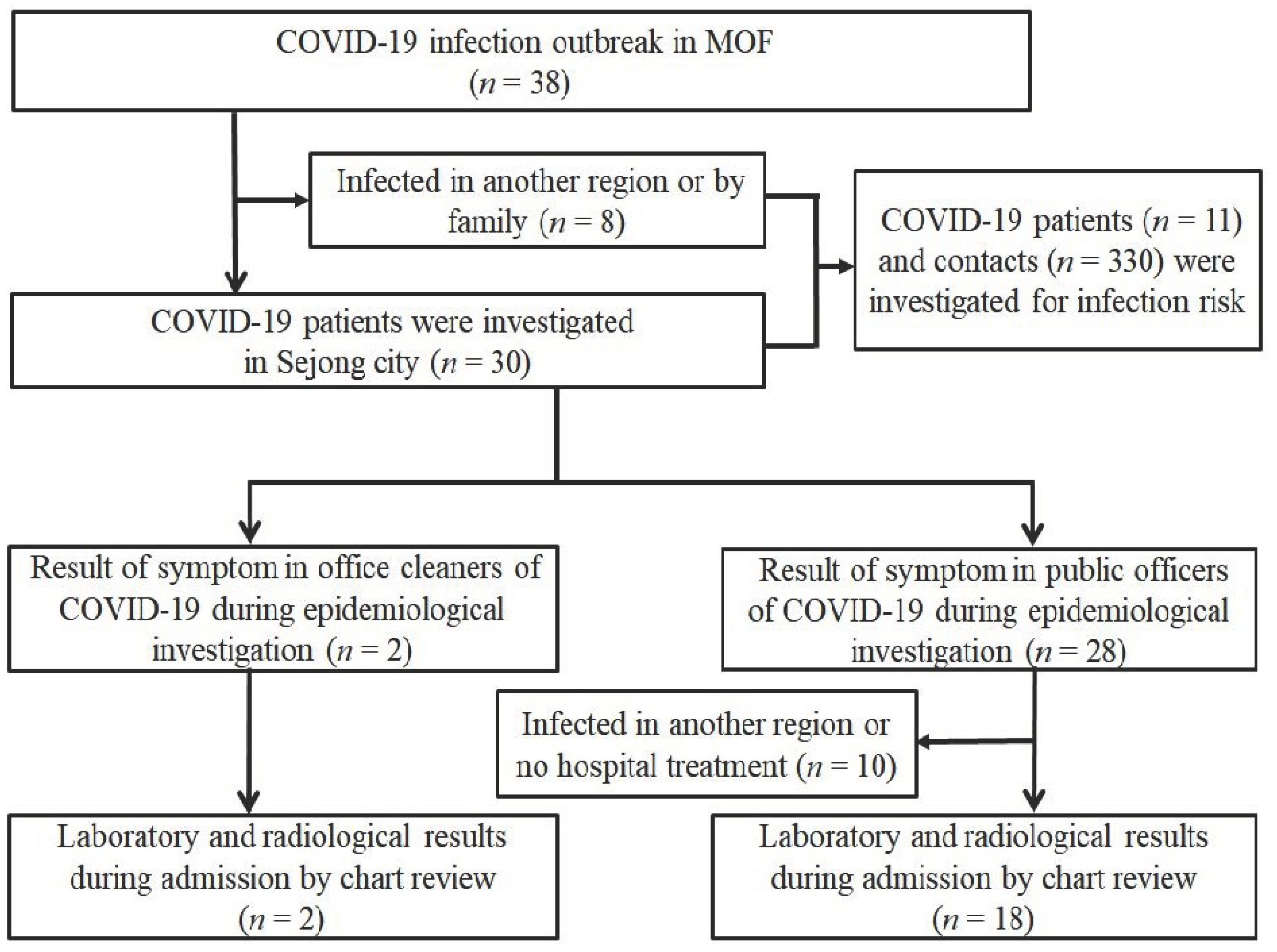
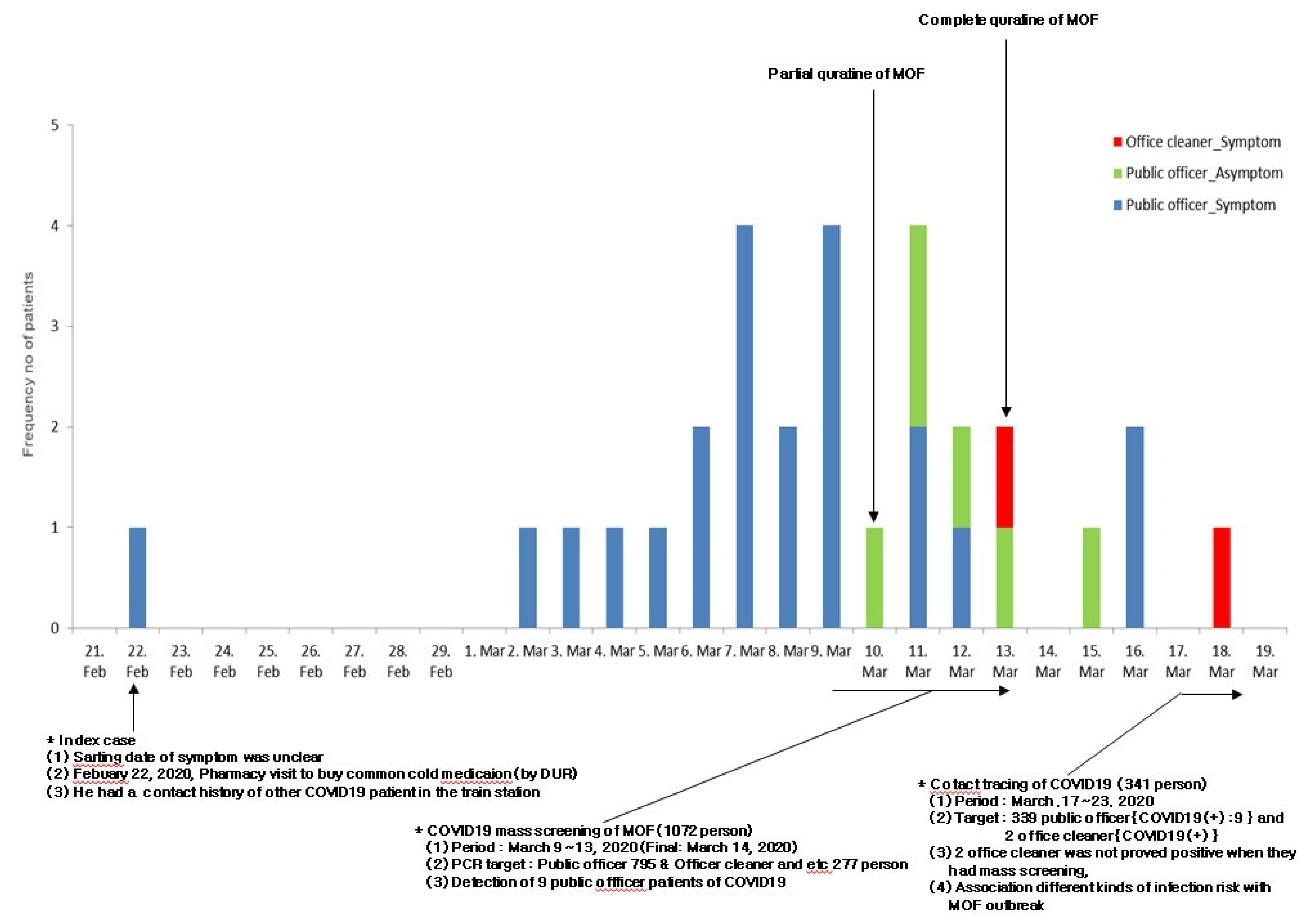
2.1. Outbreak Investigation
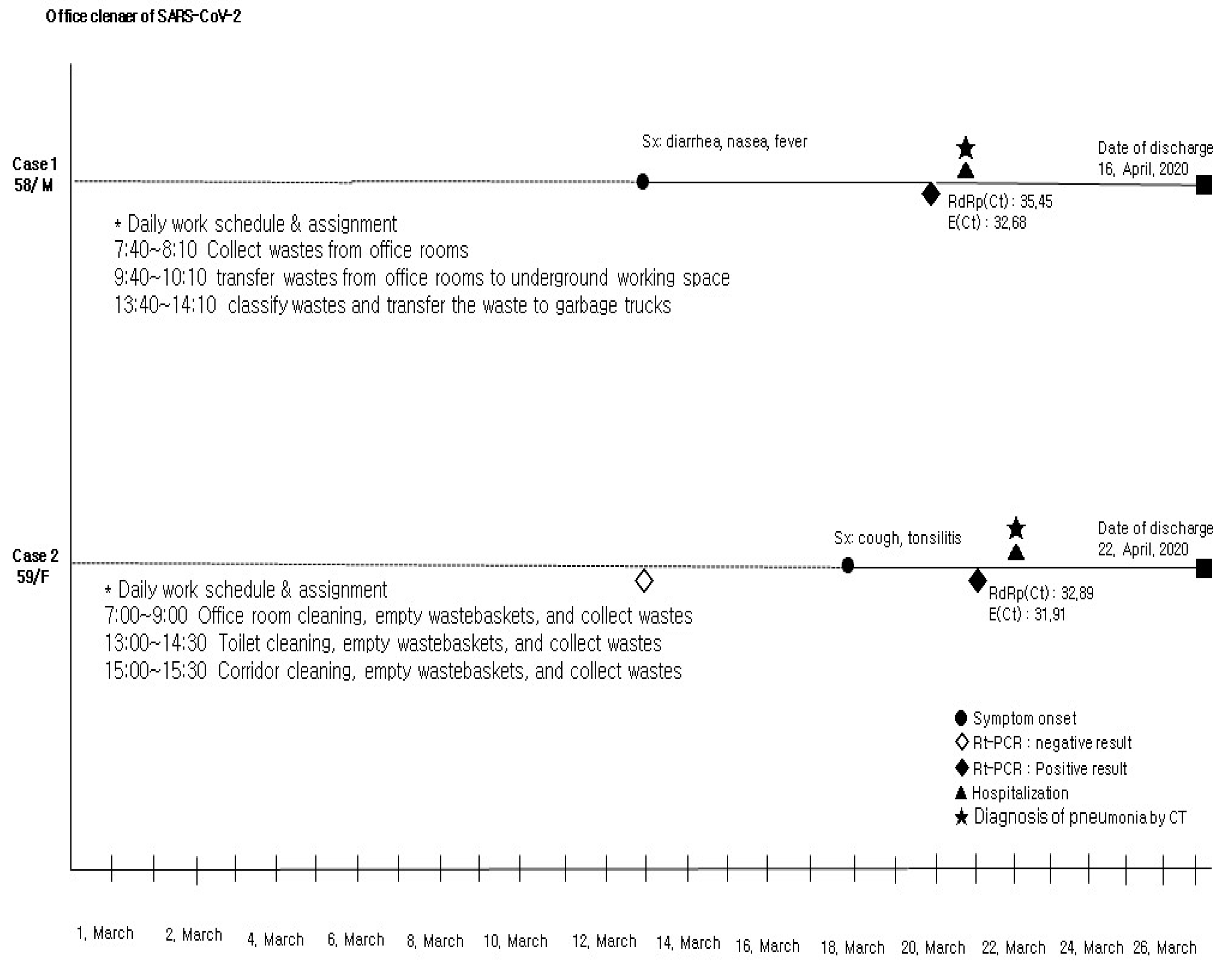
2.2. Diagnostic Laboratory Characteristics in COVID-19 Patients
2.3. Radiologic Findings and Severity of Patients with Pneumonia in the Office Cleaners
3. Discussion
4. Materials and Methods
4.1. Outbreak Investigation (Subjects)
4.2. COVID-19 Testing
4.3. Review of Diagnostic Laboratory Characteristic
4.4. Statistical Methods
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.; Lau, E.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- The Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). COVID-19 Dashboard. Available online: https://www.arcgis.com/apps/MapSeries/index.html?appid=b379f788425349168d02669285758af0 (accessed on 22 May 2022).
- Stadnytskyi, V.; Bax, C.E.; Bax, A.; Anfinrud, P. The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission. Proc. Natl. Acad. Sci. USA 2020, 117, 11875–11877. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Li, Y.; Zhang, A.L.; Wang, Y.; Molina, M.J. Identifying airborne transmission as the dominant route for the spread of COVID-19. Proc. Natl. Acad. Sci. USA 2020, 117, 14857–14863. [Google Scholar] [CrossRef]
- Mondelli, M.U.; Colaneri, M.; Seminari, E.M.; Baldanti, F.; Bruno, R. Low risk of SARS-CoV-2 transmission by fomites in real-life conditions. Lancet Infect Dis. 2021, 21, e112. [Google Scholar] [CrossRef]
- Goldman, E. Exaggerated risk of transmission of COVID-19 by fomites. Lancet Infect Dis. 2020, 20, 892–893. [Google Scholar] [CrossRef]
- Cai, J.; Sun, W.; Huang, J.; Gamber, M.; Wu, J.; He, G. Indirect Virus Transmission in Cluster of COVID-19 Cases, Wenzhou, China, 2020. Emerg Infect Dis. 2020, 26, 1343–1345. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Chen, Z.; Gong, C.; Liu, H.; Li, B.; Li, K.; Chen, X.; Xu, C.; Jing, Q.; Liu, G.; et al. Sewage as a Possible Transmission Vehicle During a Coronavirus Disease 2019 Outbreak in a Densely populated Community: Guangzhou, China, April 2020. Clin. Infect Dis. 2021, 73, e1487–e1488. [Google Scholar] [CrossRef]
- Del Brutto, O.H.; Costa, A.F.; Mera, R.M.; Recalde, B.Y.; Bustos, J.A.; García, H.H. Late incidence of SARS-CoV-2 infection in a highly-endemic remote rural village. A prospective population-based cohort study. Pathog. Glob. Health 2020, 114, 457–462. [Google Scholar] [CrossRef]
- van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef]
- Ye, G.; Lin, H.; Chen, S.; Wang, S.; Zeng, Z.; Wang, W.; Zhang, S.; Rebmann, T.; Li, Y.; Pan, Z.; et al. Environmental contamination of SARS-CoV-2 in healthcare premises. J. Infect. 2020, 81, e1–e5. [Google Scholar] [CrossRef]
- Casini, B.; Tuvo, B.; Cristina, M.L.; Spagnolo, A.M.; Totaro, M.; Baggiani, A.; Privitera, G.P. Evaluation, of an ultraviolet C (UVC) light-emitting device for disinfection of high touch surfaces, in hospital critical areas. Int. J. Environ. Res. Public Health 2019, 16, 3572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, Z.; Qian, H.; Xu, B.; Huang, Y.; Miao, T.; Yen, H.L.; Xiao, S.; Cui, L.; Wu, X.; Shao, W.; et al. Toilets dominate environmental detection of severe acute respiratory syndrome coronavirus 2 in a hospital. Sci. Total Environ. 2021, 753, 141710. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Ni, W.; Wang, Z.; Ma, G.; Pan, B.; Dong, L.; Gao, R.; Jiang, F. The distribution of SARS-CoV-2 contamination on the environmental surfaces during incubation period of COVID-19 patients. Ecotoxicol. Environ. Saf. 2021, 208, 111438. [Google Scholar] [CrossRef] [PubMed]
- Chia, P.Y.; Coleman, K.K.; Tan, Y.K.; Ong, S.; Gum, M.; Lau, S.K.; Lim, X.F.; Lim, A.S.; Sutjipto, S.; Lee, P.H.; et al. Detection of air and surface contamination by SARS-CoV-2 in hospital rooms of infected patients. Nat. Commun. 2020, 11, 2800. [Google Scholar] [CrossRef] [PubMed]
- Ryu, B.H.; Cho, Y.; Cho, O.H.; Hong, S.I.; Kim, S.; Lee, S. Environmental contamination of SARS-CoV-2 during the COVID-19 outbreak in South Korea. Am. J. Infect. Control. 2020, 48, 875–879. [Google Scholar] [CrossRef]
- Kim, U.J.; Lee, S.Y.; Lee, J.Y.; Lee, A.; Kim, S.E.; Choi, O.J.; Lee, J.S.; Kee, S.J.; Jang, H.C. Air and Environmental Contamination Caused by COVID-19 Patients: A Multi-Center Study. J. Korean Med. Sci. 2020, 35, e332. [Google Scholar] [CrossRef]
- Del Brutto, O.H.; Costa, A.F.; Mera, R.M.; Andrade-Molina, D.; Recalde, B.Y.; García, H.H.; Fernández-Cadena, J.C. SARS-CoV-2 RNA in Swabbed Samples from Latrines and Flushing Toilets: A Case-Control Study in a Rural Latin American Setting. Am. J. Trop. Med. Hyg. 2021, 104, 1045–1047. [Google Scholar] [CrossRef]
- Liu, J.; Liu, J.; He, Z.; Yang, Z.; Yuan, J.; Wu, H.; Zhu, P.; Fu, X.; Lin, Y.; Zhang, Y.; et al. Duration of SARS-CoV-2 positive in quarantine room environments: A perspective analysis. Int. J. Infect. Dis. 2021, 105, 68–74. [Google Scholar] [CrossRef]
- Hu, X.; Xing, Y.; Ni, W.; Zhang, F.; Lu, S.; Wang, Z.; Gao, R.; Jiang, F. Environmental contamination by SARS-CoV-2 of an imported case during incubation period. Sci. Total Environ. 2020, 742, 140620. [Google Scholar] [CrossRef]
- Luo, L.; Liu, D.; Zhang, H.; Li, Z.; Zhen, R.; Zhang, X.; Xie, H.; Song, W.; Liu, J.; Huang, Q.; et al. Air and surface contamination in non-health care settings among 641 environmental specimens of 39 COVID-19 cases. PLoS Negl. Trop. Dis. 2020, 14, e0008570. [Google Scholar] [CrossRef]
- Montagna, M.T.; De Giglio, O.; Calia, C.; Pousis, C.; Apollonio, F.; Campanale, C.; Diella, G.; Lopuzzo, M.; Marzella, A.; Triggiano, F.; et al. First Detection of Severe Acute Respiratory Syndrome Coronavirus 2 on the Surfaces of Tourist-Recreational Facilities in Italy. Int. J. Environ. Res. Public Health 2021, 18, 3252. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.U.; Kim, M.J.; Ra, S.H.; Lee, J.; Bae, S.; Jung, J.; Kim, S.H. Clinical characteristics of asymptomatic and symptomatic patients with mild COVID-19. Clin. Microbiol. Infect. 2020, 26, 948.e1–948.e3. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.Y.; Chen, T.J.; Hwang, S.J. Analysis of Imported Cases of COVID-19 in Taiwan: A Nationwide Study. Int. J. Environ. Res. Public Health 2020, 17, 3311. [Google Scholar] [CrossRef]
- Othman, B.A.; Maulud, S.Q.; Jalal, P.J.; Abdulkareem, S.M.; Ahmed, J.Q.; Dhawan, M.; Choudhary, O.P. Olfactory dysfunction as a post-infectious symptom of SARS-CoV-2 infection. Ann. Med. Surg. 2022, 75, 103352. [Google Scholar] [CrossRef]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro. Surveill. 2020, 25, 2000045. [Google Scholar] [CrossRef] [Green Version]
- Pan, Y.; Zhang, D.; Yang, P.; Poon, L.; Wang, Q. Viral load of SARS-CoV-2 in clinical samples. Lancet Infect. Dis. 2020, 20, 411–412. [Google Scholar] [CrossRef]
- Kampf, G.; Lemmen, S.; Suchomel, M. Ct values and infectivity of SARS-CoV-2 on surfaces. Lancet Infect. Dis. 2021, 21, e141. [Google Scholar] [CrossRef]
- Sung, H.K.; Kim, J.Y.; Heo, J.; Seo, H.; Jang, Y.S.; Kim, H.; Koh, B.R.; Jo, N.; Oh, H.S.; Baek, Y.M.; et al. Clinical Course and Outcomes of 3,060 Patients with Coronavirus Disease 2019 in Korea, January-May 2020. J. Korean Med. Sci. 2020, 35, e280. [Google Scholar] [CrossRef]
- Fang, X.; Li, S.; Yu, H.; Wang, P.; Zhang, Y.; Chen, Z.; Li, Y.; Cheng, L.; Li, W.; Jia, H.; et al. Epidemiological, comorbidity factors with severity and prognosis of COVID-19: A systematic review and meta-analysis. Aging 2020, 12, 12493–12503. [Google Scholar] [CrossRef] [PubMed]
- Levin, A.T.; Hanage, W.P.; Owusu-Boaitey, N.; Cochran, K.B.; Walsh, S.P.; Meyerowitz-Katz, G. Assessing the age specificity of infection fatality rates for COVID-19: Systematic review, meta-analysis, and public policy implications. Eur. J. Epidemiol. 2020, 12, 1123–1138. [Google Scholar] [CrossRef] [PubMed]
- Nazaroff, W.W.; Weschler, C.J. Cleaning products and air fresheners: Exposure to primary and secondary air pollutants. Atmos. Environ. 2004, 38, 2841–2865. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| COVID-19 (+): n (%) | COVID-19 (−): n (%) | p-Value ** | OR | 95% CI | |||
|---|---|---|---|---|---|---|---|
| Yes | No | Yes | No | ||||
| Demographics | |||||||
| Age, median (range) † | 45 (26–59) | 41 (20–58) | 0.383 | ||||
| Male | 7 (63.6) | 4 (36.4) | 239 (72.4) | 91 (27.6) | 0.507 | 0.67 | 0.191–2.330 |
| Contact risk factor by COVID-19 (+) | |||||||
| Contact interval < 2 m | 5 (45.5) | 6 (54.5) | 202 (61.2) | 128 (38.8) | 0.352 | 0.53 | 0.158–1.766 |
| No mask | 7 (63.6) | 4 (36.4) | 180 (54.5) | 150 (45.5) | 0.551 | 1.46 | 0.419–5.077 |
| Same office room | 4 (36.4) | 7 (63.6) | 140 (42.4) | 190 (57.6) | 0.766 | 0.78 | 0.223–2.701 |
| Physical contact (ex. Handshake, etc.) | 1 (9.1) | 10 (90.9) | 10 (3.0) | 320 (97.0) | 0.307 | 3.20 | 0.373–27.467 |
| Night or special duty | 0 (0) | 11 (100.0) | 55 (16.7) | 275 (83.3) | 0.223 | ||
| Meeting of meal or coffee | 2 (18.2) | 9 (81.8) | 49 (14.8) | 281 (85.2) | 0.672 | 1.27 | 0.267–6.076 |
| Conference or conversation | 3 (27.3) | 8 (72.7) | 59 (17.9) | 271 (82.1) | 0.428 | 1.72 | 0.444–6.687 |
| Same place of smoking | 0 (0) | 11 (100) | 3 (0.9) | 327 (99.1) | 1.000 | ||
| Sharing of fomites and toilet | 3 (27.3) | 8 (72.7) | 5 (1.5) | 325 (98.5) | 0.001 | 24.38 | 4.951–120.010 |
| Sharing of elevator | 1 (9.1) | 10 (90.9) | 6 (1.8) | 324 (98.2) | 0.207 | 5.4 | 0.593–49.154 |
| Meeting rooftop or corridor | 1 (9.1) | 10 (90.9) | 5 (1.5) | 325 (98.5) | 0.180 | 6.5 | 0.694–60.895 |
| Sharing car | 0 (0) | 11 (100) | 8 (2.4) | 322 (97.6) | 1.000 | 0.97 | 0.948–0.986 |
| Contact time (minute): median (range) ** | 25.5 (1–50) | 15 (0.05–180) | 0.642 | ||||
| Office Cleaner: n = 2 (%) | Public Officer: n = 28 (%) | p-Value * | OR | 95% CI | |||
|---|---|---|---|---|---|---|---|
| Yes | No | Yes | No | ||||
| Demographics (N = 30) | |||||||
| Age, median (range) ** | 58.5 (58–59) | 45.5 (26–57) | 0.845 | ||||
| Male | 1 (50.0) | 1 (50.0) | 22 (78.6) | 6 (21.4) | 0.418 | 0.27 | 0.015–5.032 |
| Symptoms (N = 30) | |||||||
| Fever | 1 (50.0) | 1 (50.0) | 9 (32.1) | 19 (67.9) | 1.000 | 2.11 | 0.118–37.72 |
| Cough | 2 (100) | 0 (0) | 13 (46.4) | 15 (53.6) | 0.483 | ||
| Sputum | 1 (50.0) | 1 (50.0) | 4 (14.3) | 24 (85.7) | 0.310 | 6.00 | 0.309–116.61 |
| Chill | 0 (0) | 2 (100) | 4 (14.3) | 24 (85.7) | 1.000 | ||
| Rhinorrhea | 0 (0) | 2 (100) | 5 (17.9) | 23 (82.1) | 1.000 | ||
| Tonsilitis | 1 (50.0) | 1 (50.0) | 8 (28.6) | 20 (71.4) | 0.517 | 2.50 | 0.139–45.01 |
| Headache | 0 (0) | 2 (100.0) | 6 (21.4) | 22 (78.6) | 1.000 | ||
| Body ache | 1 (50.0) | 1 (50.0) | 9 (32.1) | 19 (67.9) | 1.000 | 2.11 | 0.118–37.722 |
| Arthralgia | 0 (0) | 2 (100) | 2 (7.1) | 26 (92.9) | 1.000 | ||
| Dyspnea | 0 (0) | 2 (100) | 0 (0) | 28 (100) | |||
| Chest discomfort | 0 (0) | 2 (100) | 0 (0) | 28 (100) | |||
| Fatigue | 0 (0) | 2 (100) | 1 (3.6) | 27 (96.4) | 1.000 | ||
| General weakness | 0 (0) | 2 (100) | 0 (0) | 28 (100) | |||
| Olfactory sense loss | 1 (50.0) | 1 (50.0) | 1 (3.6) | 27 (96.4) | 0.131 | 27.0 | 0.887–821.79 |
| Nasal obstruction | 0 (0) | 2 (100) | 4 (14.3) | 24 (85.7) | 1.000 | ||
| Taste sense loss | 1 (50.0) | 1 (50.0) | 1 (3.6) | 27 (96.4) | 0.131 | 27.0 | 0.887–821.79 |
| Diarrhea | 1 (50.0) | 1 (50.0) | 3 (10.7) | 25 (89.3) | 0.253 | 8.33 | 0.407–170.66 |
| Hoarse voice | 0 (0) | 2 (100) | 1 (3.6) | 27 (96.4) | 1.000 | ||
| Laboratory Index (Unit) | Office Cleaner: n = 2 (%) | Public Officer: n = 18 (%) | p-Value ** | ||
|---|---|---|---|---|---|
| Number of Abnormal Patient(s) * | (Median, Range) | Number of Abnormal Patient(s) * | (Median, Range) | ||
| Upper respiratory PCR (N = 25) * | |||||
| RdRp(Ct) value | 1/2 (50%) | (34.17, 32.89–35.45) | 23 (100%) * | (24.99, 17.60–33.60) | 0.035 |
| E(Ct) value | 2/2 (100%) | (32.30, 31.91–32.68) | 23 (100%) * | (24.74, 17.20–33.00) | 0.045 |
| Complete blood count (N = 20) | |||||
| White blood cell (k/µL) | 0/2 (0%) | (5.95, 4.60–7.30) | 2/18 (11.1%) | (5.50, 3.57–9.37) | 0.705 |
| Neutrophil (%) | 2/2 (100%) | (80.10, 77.30–82.90) | 3/18 (16.7%) | (57.95, 43.60–80.0) | 0.044 |
| Neutrophil count (/µL) | 0/2 (0%) | (4.75, 3.50–6.00) | 1/10 (10.0%) | (3.66, 1.68–6.38) | 0.451 |
| Lymphocyte (%) | 2/2 (100%) | (14.85, 14.30–15.40) | 3/18 (16.7%) | (30.70, 13.0–42.0) | 0.078 |
| Lymphocyte count (/µL) | 1/2 (50%) | (0.85, 0.70–1.00) | 3/10 (30.0%) | (1.62, 0.90–3.09) | 0.086 |
| Eosinophil (%) | 0/2 (0%) | (0.40, 0.3–0.5) | 0/18 (0%) | (1.15, 0–3.70) | 0.114 |
| Eosinophil count (/µL) | 0/2 (0%) | (0) | 0/10 (0%) | (0.07, 0–0.20) | 0.079 |
| Basophil (%) | 0/2 (0%) | (0.15, 0.10–0.20) | 1/18 (5.6%) | (0.4, 0–2.20) | 0.338 |
| Basophil count (/µL) | 0/2 (0%) | (0) | 0/10 (0%) | (0.02, 0–0.10) | 0.118 |
| Monocyte (%) | 1/2 (50%) | (4.50, 2.10–6.90) | 2/18 (11.1%) | (7.0, 5.0–13.0) | 0.183 |
| Monocyte count (/µL) | 1/2 (50%) | (0.25, 0.20–0.30) | 0/10 (0%) | (0.46, 0.30–0.68) | 0.051 |
| Serum chemistry (N = 20) | |||||
| Glucose, fasting (mg/dL) | 2/2 (100%) | (163.50, 163–164) | 5/18 (27.8%) | (102.50, 86–188) | 0.044 |
| Blood urea nitrogen (mg/dL) | 0/2 (0%) | (11.1, 10.70–11.50) | 1/18 (5.6%) | (13.10, 7.60–17.50) | 0.378 |
| Serum creatinine (mg/dL) | 2/2 (100%) | (0.67, 0.58–0.75) | 9/18 (50.0%) | (0.88, 0.43–1.24) | 0.207 |
| Proteins, total (g/dL) | 0/2 (0%) | (7.45, 7.30–7.60) | 4/18 (22.3%) | (7.60, 6.30–8.20) | 0.705 |
| Albumin (g/dL) | 1/2 (50%) | (3.70, 3.40–4.00) | 2/18 (11.1%) | (4.20, 3.70–4.70) | 0.049 |
| Serum bilirubin, total (mg/dL) | 0/2 (0%) | (0.49, 0.28–0.69) | 0/18 (0%) | (0.48, 0.28–1.03) | 0.801 |
| Alkaline phosphatase (IU/L) | 0/2 (0%) | (62.50, 54–71) | 8/18 (44.4%) | (72.50, 40–261) | 0.801 |
| Aspartate aminotransferase (IU/L) | 0/2 (0%) | (17, 14–20) | 5/18 (27.8%) | (23.50, 9–49) | 0.207 |
| Alanine aminotransferase (IU/L) | 0/2 (0%) | (16.50, 14–19) | 5/18 (27.8%) | (29.5, 11–78) | 0.115 |
| Lactate dehydrogenase (mg/dL) | 2/2 (100%) | (510, 466–554) | 3/18 (16.7%) | (360, 223–513) | 0.044 |
| Creatine kinase (IU/L) | 0/2 (0%) | (80.50, 76–85) | 3/18 (16.7%) | (96, 39–364) | 0.412 |
| Cholesterol (mg/dL) | 1/2 (50%) | (191, 151–231) | 2/18 (11.1%) | (186, 105–224) | 0.705 |
| Office Cleaner: n = 2 (%) | Public Officer: n = 16 (%) | p-Value * | OR | 95% CI | |||
|---|---|---|---|---|---|---|---|
| Yes | No | Yes | No | ||||
| Radiological finding of X-ray (N = 18) | |||||||
| Pneumonia | 0 (0) | 2 (100) | 3 (18.8) | 13 (81.3) | 1.000 | ||
| Ground glass opacity | 2 (100.0) | 0 (0) | 3 (18.8) | 13 (81.3) | 0.065 | ||
| Consolidation | 0 | 2 (100) | 0 | 16 (100) | |||
| Diffuse pattern | 1 (50.0) | 1 (50.0) | 0 | 16 (100) | 0.111 | ||
| Atelectasis | 1 (50.0) | 1 (50.0) | 1 (6.3) | 15 (93.8) | 0.216 | 15.0 | 0.485–464.20 |
| Emphysema | 0 (0) | 2 (100) | 0 | 16 (100) | |||
| Nodule | 1 (50.0) | 1 (50.0) | 1 (6.3) | 15 (93.8) | 0.216 | 15.0 | 0.485–464.20 |
| Calcification | 0 (0) | 2 (100) | 0 | 16 (100) | |||
| Pleural effusion | 0 (0) | 2 (100) | 0 | 16 (100) | |||
| Invasion lesion of X-ray (N = 18) | |||||||
| Right upper lobe | 0 (0) | 2 (100) | 2 (12.5) | 14 (87.5) | 1.000 | ||
| Right middle lobe | 1 (50.0) | 1 (50.0) | 1 (6.3) | 15 (93.8) | 0.216 | 15.0 | 0.485–464.20 |
| Right lower lobe | 1 (50.0) | 1 (50.0) | 3 (18.8) | 13 (81.3) | 0.405 | 4.33 | 0.207–90.85 |
| Left upper lobe | 0 (0) | 2 (100) | 2 (12.5) | 14 (87.5) | 1.000 | ||
| Left lower lobe | 2 (100) | 0 (0) | 4 (25.0) | 12 (75.0) | 0.098 | ||
| Both lobe | 2 (100) | 0 (0) | 2 (12.5) | 14 (87.5) | 0.039 | ||
| Whole | 0 (0) | 2 (100) | 0 | 16 (100) | |||
| Radiological finding of CT (N = 17) | |||||||
| Pneumonia | 2 (100) | 0 (0) | 12 (80.0) | 3 (20.0) | 1.000 | ||
| Ground glass opacity | 2 (100.0) | 0 (0) | 11 (73.3) | 4 (26.7) | 1.000 | ||
| Consolidation | 1 (50.0) | 1 (50.0) | 5 (33.0) | 10 (66.7) | 1.000 | 2.0 | 0.102–39.079 |
| Diffuse pattern | 0 (0) | 2 (100) | 0 (0) | 15 (100) | |||
| Atelectasis | 1 (50.0) | 1 (50.0) | 1 (6.7) | 14 (93.3) | 0.228 | 14.0 | 0.451–434.41 |
| Emphysema | 0 (0) | 2 (100) | 1 (6.7) | 14 (93.3) | 1.000 | ||
| Nodule | 0 (00) | 2 (100) | 0 (0) | 15 (100) | |||
| Calcification | 0 (00) | 2 (100) | 0 (0) | 15 (100) | |||
| Pleural effusion | 0 (00) | 2 (100) | 0 (0) | 15 (100) | |||
| Invasion lesion of CT (N = 17) | |||||||
| Right upper lobe | 2 (100) | 0 (0) | 7 (46.7) | 8 (53.3) | 0.471 | ||
| Right middle lobe | 2 (100) | 0 (0) | 0 (0) | 15 (100) | 0.007 | ||
| Right lower lobe | 2 (100) | 0 (0) | 5 (33.3) | 10 (66.7) | 0.154 | ||
| Left upper lobe | 2 (100) | 0 (0) | 7 (46.7) | 8 (53.3) | 0.471 | ||
| Left lower lobe | 2 (100) | 0 (0) | 5 (33.3) | 10 (66.7) | 0.154 | ||
| Both lobe | 2 (100) | 0 (0) | 5 (33.3) | 10 (66.7) | 0.154 | ||
| Whole | 2 (100) | 0 (0) | 0 (0) | 15 (100) | 0.007 | ||
| Pneumonia severity | |||||||
| PSI risk class | |||||||
| 1 | 1 (50.0) | 8 (80) | 0.455 | ||||
| 2 | 1 (50.0) | 2 (20) | |||||
| CURB score (Zero) | 0 (0) | 2 (100) | 0 (0) | 13 (100) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, S.-M.; Jung, Y.; Seo, H. Diagnostic Laboratory Characteristics of COVID-19 Patients Infected by Fomites: COVID-19 Outbreak in a South Korean Public Administrative Facility. Pathogens 2022, 11, 700. https://doi.org/10.3390/pathogens11060700
Hwang S-M, Jung Y, Seo H. Diagnostic Laboratory Characteristics of COVID-19 Patients Infected by Fomites: COVID-19 Outbreak in a South Korean Public Administrative Facility. Pathogens. 2022; 11(6):700. https://doi.org/10.3390/pathogens11060700
Chicago/Turabian StyleHwang, Se-Min, Yoomi Jung, and Haesook Seo. 2022. "Diagnostic Laboratory Characteristics of COVID-19 Patients Infected by Fomites: COVID-19 Outbreak in a South Korean Public Administrative Facility" Pathogens 11, no. 6: 700. https://doi.org/10.3390/pathogens11060700