
Anti-TBE Intrathecal Synthesis as a Prediction Marker in TBE Patients

 ,
,
Abstract
:1. Introduction
2. Results
2.1. General Results
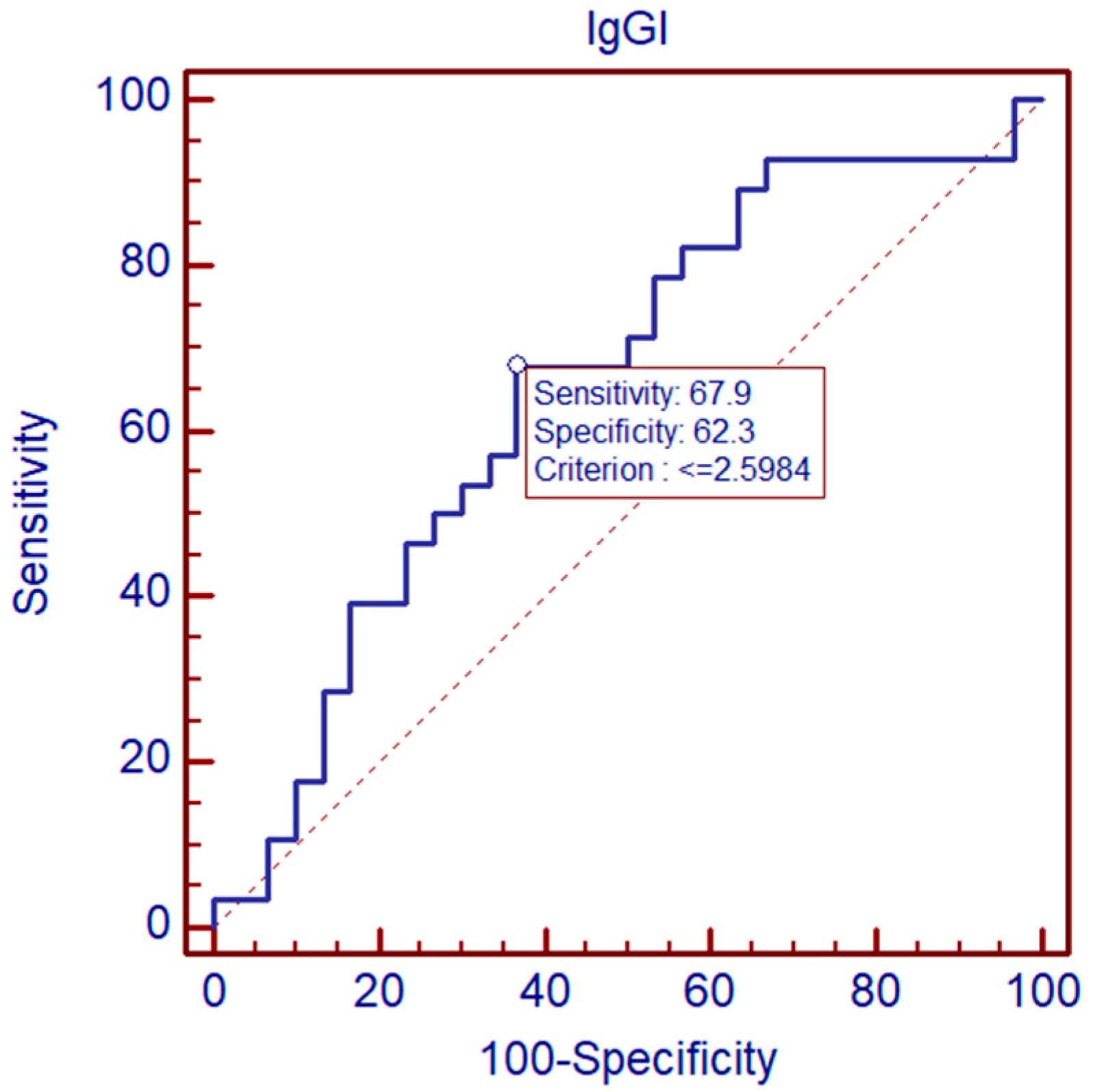
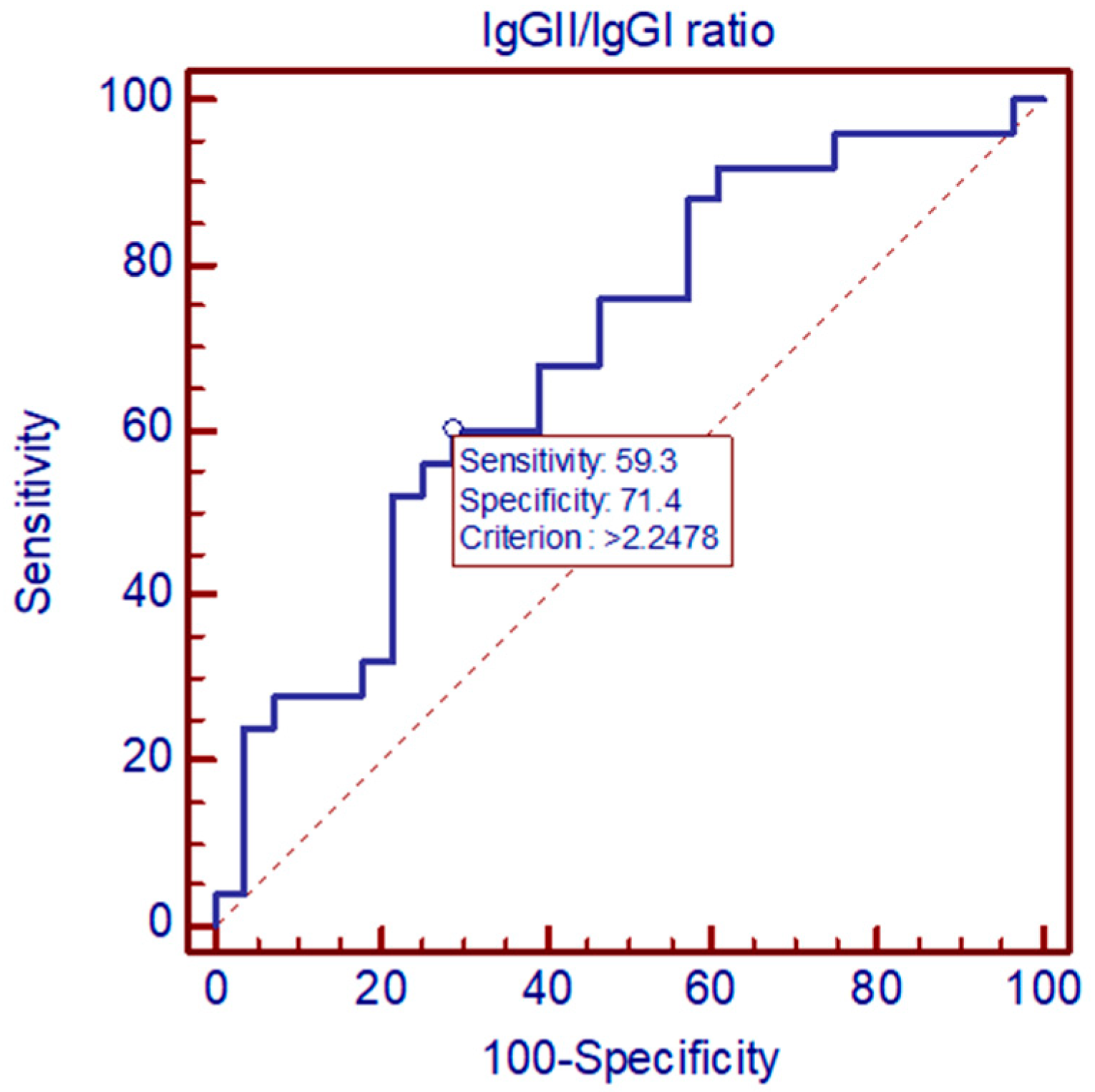
2.2. ROC Analysis
2.3. Analysis of Correlation
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bogovic, P.; Strle, F. Tick-borne encephalitis: A review of epidemiology, clinical characteristics, and management. World J. Clin. Cases 2015, 3, 430–441. [Google Scholar] [CrossRef] [PubMed]
- Epidemiological Situation of Tick-Borne Encephalitis in the European Union and European Free Trade Association Countries. Available online: http://ecdc.europa.eu/ (accessed on 22 February 2022).
- Yearly Report on Infectious Diseases Incidence. Available online: http://www.pzh.gov.pl (accessed on 22 February 2022).
- Zajkowska, J.; Czupryna, P.; Pancewicz, S.; Adamczyk-Przychodzeń, A.; Kondrusik, M.; Grygorczuk, S.; Moniuszko, A. Fatal outcome of tick-borne encephalitis—A case series. Neurol. Neurochir. Pol. 2011, 45, 402–406. [Google Scholar] [CrossRef]
- Shamier, M.C.; Bogers, S.; Yusuf, E.; van Splunter, M.; Ten Berge, J.C.E.M.; Titulaer, M.; van Kampen, J.J.A.; GeurtsvanKessel, C.H. The role of antibody indexes in clinical virology. Clin. Microbiol. Infect. 2021, 27, 1207–1211. [Google Scholar] [CrossRef] [PubMed]
- Czupryna, P.; Grygorczuk, S.; Krawczuk, K.; Pancewicz, S.; Zajkowska, J.; Dunaj, J.; Matosek, A.; Kondrusik, M.; Moniuszko-Malinowska, A. Sequelae of tick-borne encephalitis in retrospective analysis of 1072 patients. Epidemiol. Infect. 2018, 146, 1663–1670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radzisauskienė, D.; Urbonienė, J.; Kaubrys, G.; Andruskevičius, S.; Jatuzis, D.; Matulytė, E.; Žvirblytė-Skrebutienė, K. The epidemiology, clinical presentation, and predictors of severe Tick-borne encephalitis in Lithuania, a highly endemic country: A retrospective study of 1040 patients. PLoS ONE 2020, 15, e0241587. [Google Scholar] [CrossRef] [PubMed]
- Dussaix, E.; Cerqueti, P.M.; Pontet, F.; Bloch-Michel, E. New approaches to the detection of locally produced antiviral antibodies in the aqueous of patients with endogenous uveitis. Ophthalmologica 1987, 194, 145e9. [Google Scholar] [CrossRef] [PubMed]
- De Groot-Mijnes, J.D.; Rothova, A.; Van Loon, A.M.; Schuller, M.; Ten Dam-Van Loon, N.H.; De Boer, J.H.; Schuuan, R.; Weersink, A.J. Polymerase chain reaction and Goldmann- Witmer coefficient analysis are complimentary for the diagnosis of infectious uveitis. Am. J. Ophthalmol. 2006, 141, 313.e8. [Google Scholar] [CrossRef] [PubMed]
- Quentin, C.D.; Reiber, H. Fuchs heterochromic cyclitis: Rubella virus antibodies and genome in aqueous humor. Am. J. Ophthalmol. 2004, 138, 46.e54. [Google Scholar] [CrossRef] [PubMed]
- Mygland, A.; Ljøstad, U.; Fingerle, V.; Rupprecht, T.; Schmutzhard, E.; Steiner, I. European Federation of Neurological Societies. EFNS guidelines on the diagnosis and management of European Lyme neuroborreliosis. Eur. J. Neurol. 2010, 17, 8–16.e1-4. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Commission Implementing Decision (2012/506/EU) of 8 August 2012 Amending Deision 2002/253/EC laying Down Case Definitions for Reporting Communicable Diseases to the Community Network under Decision No 2119/98/EC of the European Parliament and of the Council. Official Journal of the European Union. Publications Office of the European Union: Luxembourg, 27 September 2012. Available online: http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2012:262:0001:0057:EN:PDF (accessed on 22 February 2022).



{kind=link}
{kind=link}
| IgGI | IgGII | IgGII/IgGI | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Median | Min | Max | p | Median | Min | Max | p | Median | Min | Max | p | |
| Overall | 2.571 | 0.4343 | 12.502 | 4.035 | 0.9752 | 59.679 | 1.997 | 0.1466 | 11.297 | |||
| sex | ||||||||||||
| Male | 2.596 | 0.4343 | 12.502 | 0.59 | 3.770 | 1.0405 | 59.679 | 0.39 | 1.997 | 0.1466 | 11.297 | 0.87 |
| Female | 2.058 | 0.8051 | 11.701 | 4.894 | 0.9752 | 25.629 | 1.722 | 0.3657 | 7.666 | |||
| Clinical form | ||||||||||||
| Meningitis | 2.015 | 0.4343 | 12.502 | 0.19 | 3.775 | 0.9752 | 59.679 | 0.86 | 2.017 | 0.3657 | 11.297 | 0.41 |
| Meningoencephalitis | 3.342 | 0.9125 | 7.736 | 4.663 | 1.0405 | 32.016 | 1.997 | 0.1466 | 7.798 | |||
| Course | ||||||||||||
| Monophasic | 3.343 | 0.9152 | 12.502 | 0.001 | 3.871 | 1.1153 | 59.679 | 0.83 | 1.363 | 0.1466 | 8.055 | 0.04 |
| Biphasic | 2.068 | 0.4343 | 12.502 | 4.585 | 0.9752 | 59.679 | 2.154 | 0.3657 | 8.055 | |||
| Coinfection with B. burgdorferi | ||||||||||||
| No | 2.068 | 0.4343 | 12.502 | 0.12 | 4.585 | 0.9752 | 59.679 | 0.25 | 2.154 | 0.3657 | 8.055 | 0.02 |
| Yes | 3.11 | 1.283 | 8.352 | 3.627 | 1.115 | 14.491 | 0.792 | 0.147 | 11.297 | |||
| Treatment with dexamethasone | ||||||||||||
| No | 2.596 | 0.4343 | 12.502 | 0.53 | 4.432 | 0.9752 | 59.679 | 0.46 | 2.01 | 0.3657 | 11.297 | 0.88 |
| Yes | 2.015 | 0.9125 | 8.3 | 3.514 | 1.1153 | 32.016 | 1.997 | 0.1466 | 7.798 | |||
| Age | ||||||||||||
| <60 | 2.545 | 0.4343 | 12.502 | 0.52 | 4.103 | 0.9752 | 59.679 | 0.63 | 2.069 | 0.3657 | 11.297 | 0.31 |
| >60 | 2.774 | 1.091 | 7.606 | 3.968 | 1.041 | 14.935 | 0.863 | 0.147 | 5.591 | |||
| Sequalae | ||||||||||||
| No | 3.05 | 0.81 | 12.5 | 0.04 | 3.87 | 0.98 | 59.68 | 0.85 | 1.27 | 0.15 | 8.05 | 0.02 |
| Yes | 1.88 | 0.43 | 11.7 | 4.43 | 1.68 | 32.02 | 3.0 | 0.37 | 11.3 | |||
| n = 66 | ||
|---|---|---|
| Symptom | Number of Patients | % |
| Symptoms at admission | ||
| fever | 63 | 95% |
| fatigue | 25 | 38% |
| headache | 66 | 100% |
| nausea | 33 | 50% |
| paresthesia | 3 | 5% |
| meningeal signs | 53 | 80% |
| cerebellar syndrome | 18 | 27% |
| paresthesia | 7 | 11% |
| tremor | 7 | 11% |
| paresis | 4 | 6% |
| Persistent sequelae (after 1 month) | ||
| headache | 20 | 30% |
| fatigue | 7 | 11% |
| cerebellar syndrome | 2 | 3% |
| tremor | 2 | 3% |
| paresthesia | 3 | 5% |
| concentration disorders | 3 | 5% |
| Parameter | First Examination | Second Examination | ||||
|---|---|---|---|---|---|---|
| Median | Min | Max | Median | Min | Max | |
| CSF | ||||||
| pleocytosis (1/µL) | 93 | 20 | 491 | 17.5 | 2 | 116 |
| protein concentration (mg/dL) | 67 | 38 | 136 | 47 | 21 | 175 |
| albumin concentration [mg/dL] | 47.07 | 23.38 | 423 | 29.63 | 4.01 | 106.56 |
| TBE IgM [U/mL] | 77.9 | 5.9 | 2194.7 | 147.25 | 0.4 | 310.7 |
| TBE IgG [U/mL] | 620.2 | 47.3 | 8500 | 1786.4 | 51.2 | 9194.4 |
| Serum | ||||||
| CRP [mg/L] | 4.18 | 0 | 67.53 | 0.44 | 0 | 36.17 |
| WBC [10³/µL] | 9.88 | 4.83 | 16.02 | 5.85 | 3.9 | 12 |
| PLT [10³/µL] | 220 | 120 | 675 | 229 | 80.6 | 976 |
| ALT [U/L] | 17 | 5 | 80 | 20 | 1 | 137 |
| AST [U/L] | 17 | 8 | 92 | 19 | 12 | 89 |
| TBE IgM [U/mL] | 134.2 | 26.4 | 1382.3 | 127.1 | 2.86 | 2622.2 |
| TBE IgG [U/mL] | 712.55 | 113.9 | 8500 | 1900.9 | 89.7 | 7838.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siemieniako-Werszko, A.; Czupryna, P.; Moniuszko-Malinowska, A.; Dunaj-Małyszko, J.; Pancewicz, S.; Grygorczuk, S.; Zajkowska, J. Anti-TBE Intrathecal Synthesis as a Prediction Marker in TBE Patients. Pathogens 2022, 11, 416. https://doi.org/10.3390/pathogens11040416
Siemieniako-Werszko A, Czupryna P, Moniuszko-Malinowska A, Dunaj-Małyszko J, Pancewicz S, Grygorczuk S, Zajkowska J. Anti-TBE Intrathecal Synthesis as a Prediction Marker in TBE Patients. Pathogens. 2022; 11(4):416. https://doi.org/10.3390/pathogens11040416
Chicago/Turabian StyleSiemieniako-Werszko, Agnieszka, Piotr Czupryna, Anna Moniuszko-Malinowska, Justyna Dunaj-Małyszko, Sławomir Pancewicz, Sambor Grygorczuk, and Joanna Zajkowska. 2022. "Anti-TBE Intrathecal Synthesis as a Prediction Marker in TBE Patients" Pathogens 11, no. 4: 416. https://doi.org/10.3390/pathogens11040416