
Campylobacteriosis, Shigellosis and Salmonellosis in Hospitalized Children with Acute Inflammatory Diarrhea in Georgia

 and
and
Abstract
:1. Introduction
2. Results
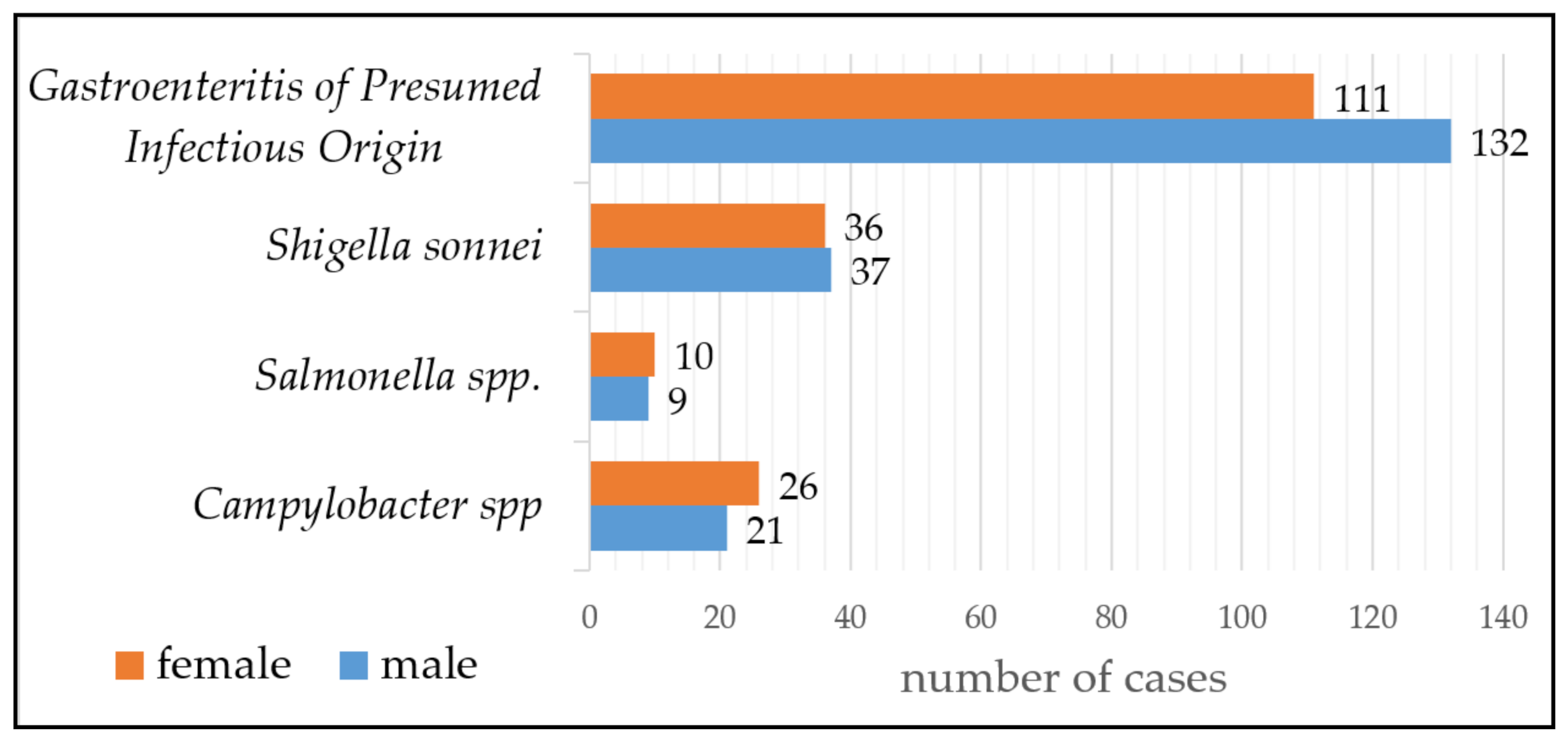
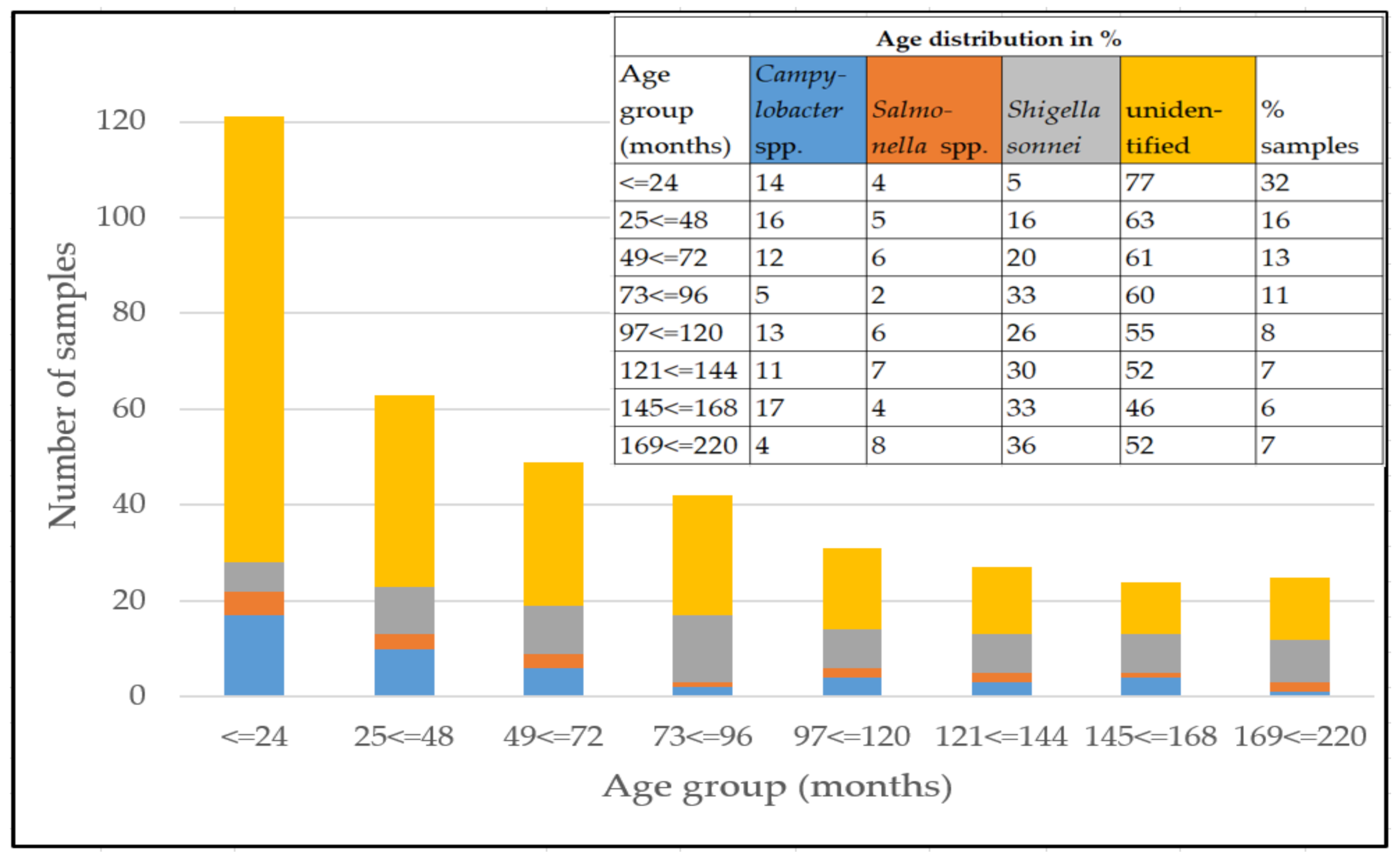
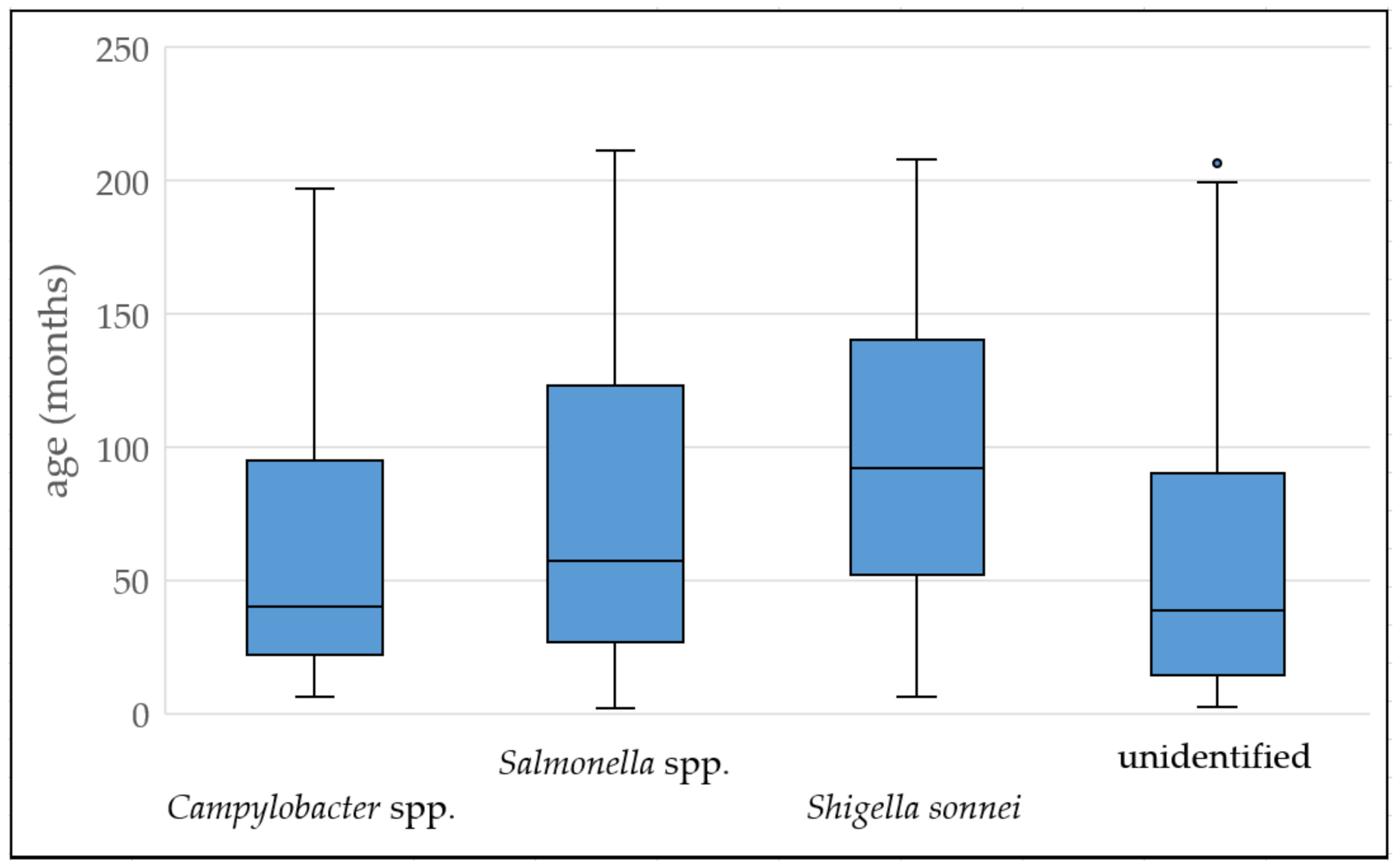
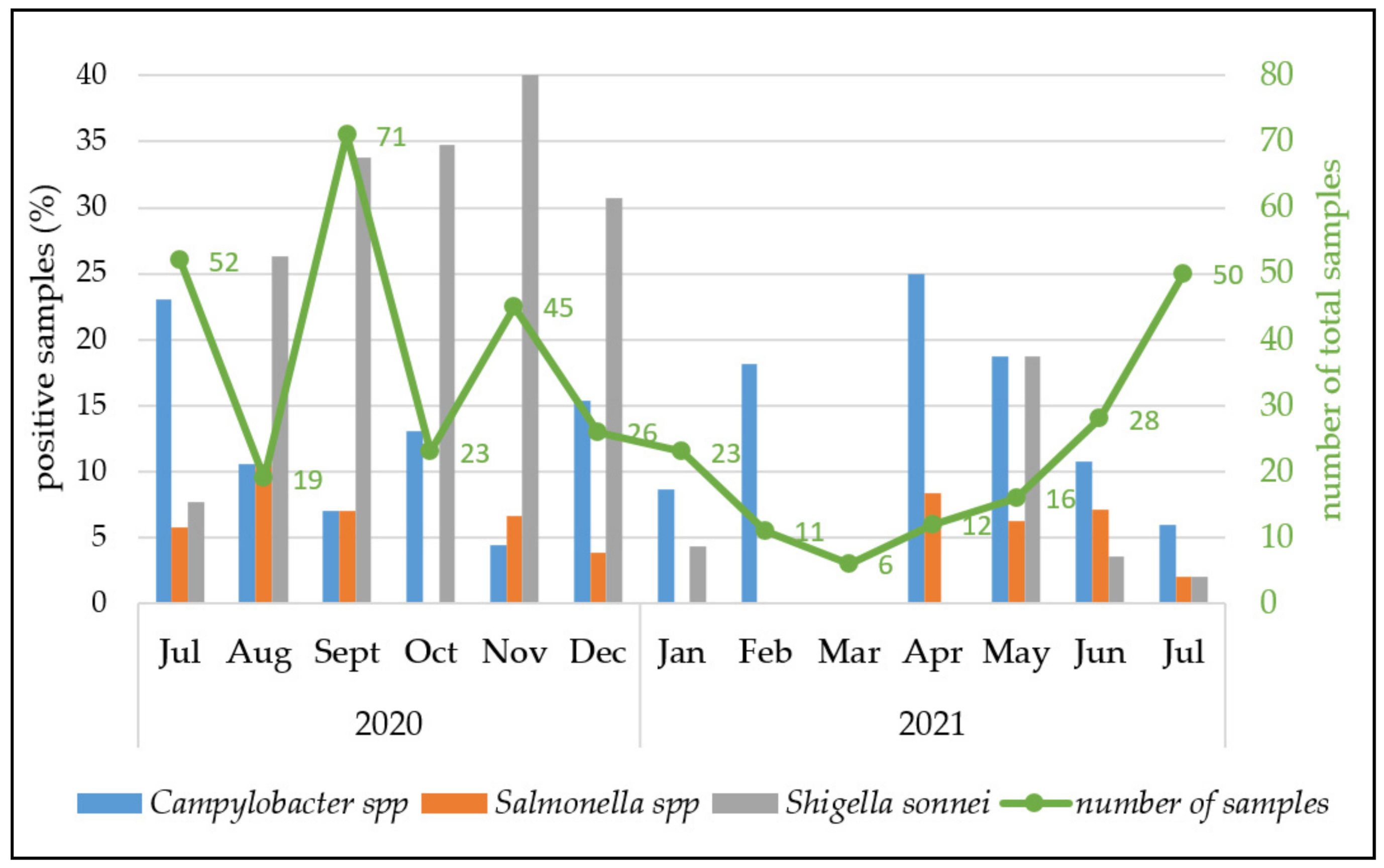
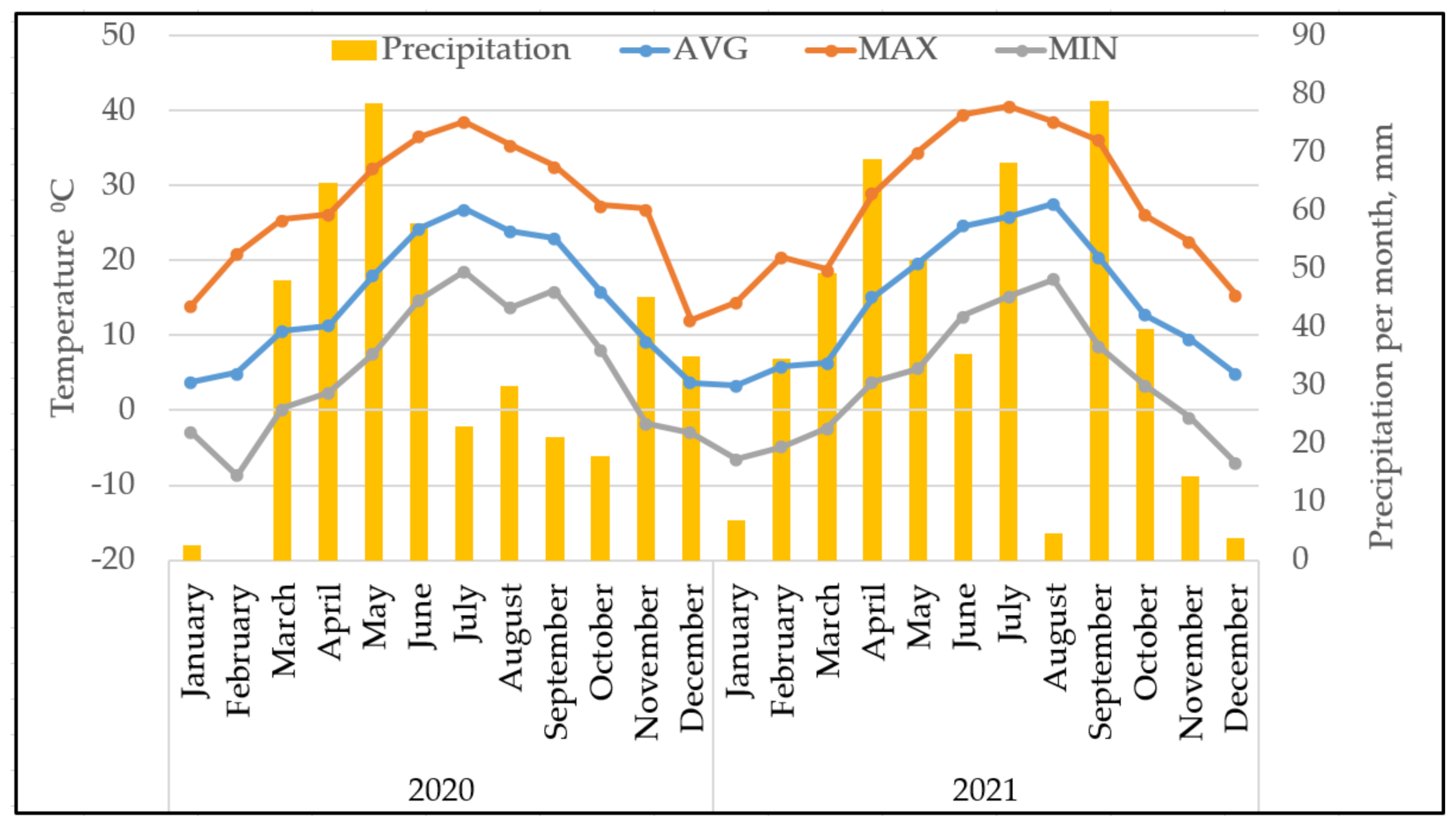
2.1. Prevalences of the Three Analysed Diarrhea-Causing Bacteria, Age Distribution of the Patients and Seasonality
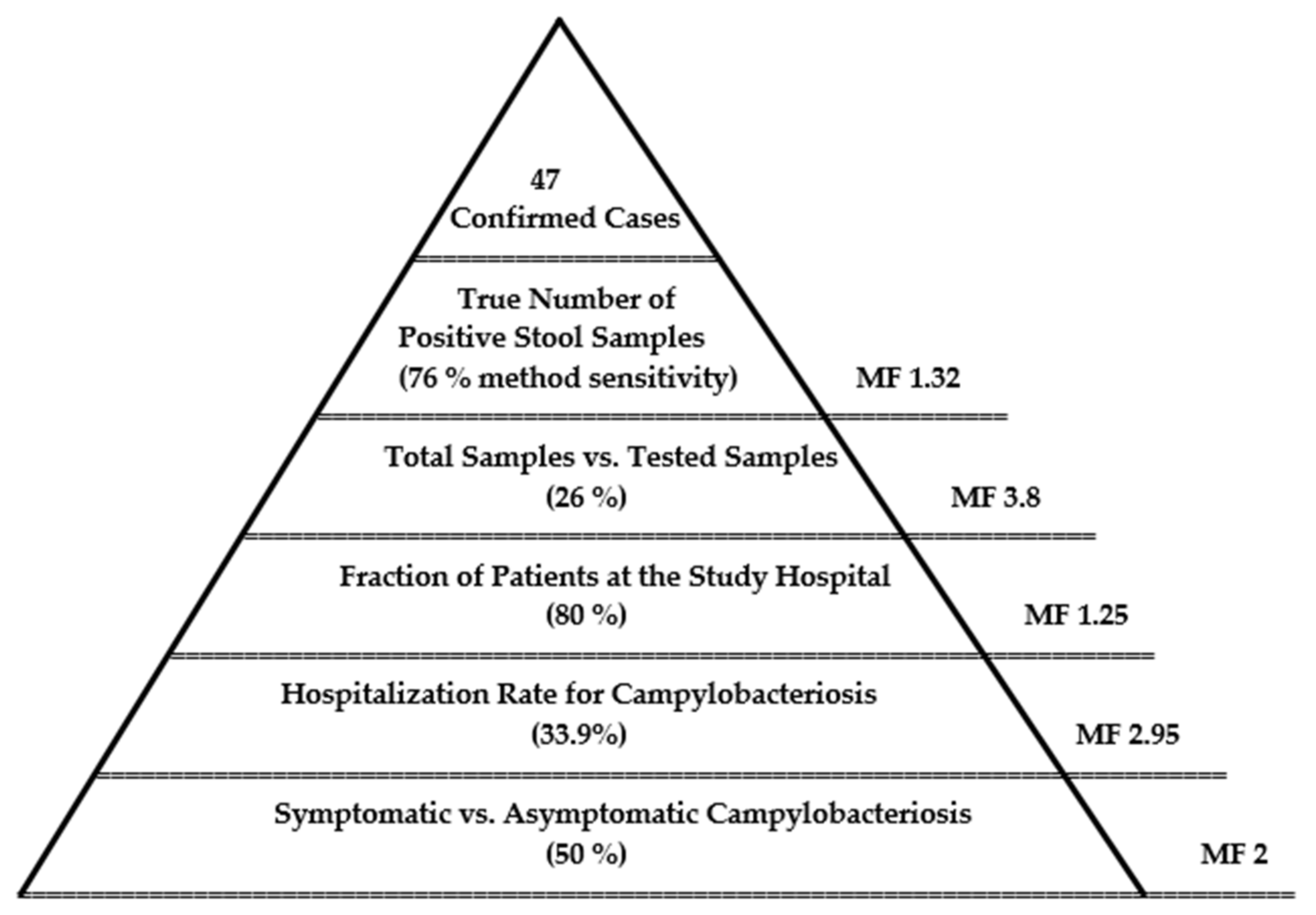
2.2. Estimated Burden of Campylobacteriosis
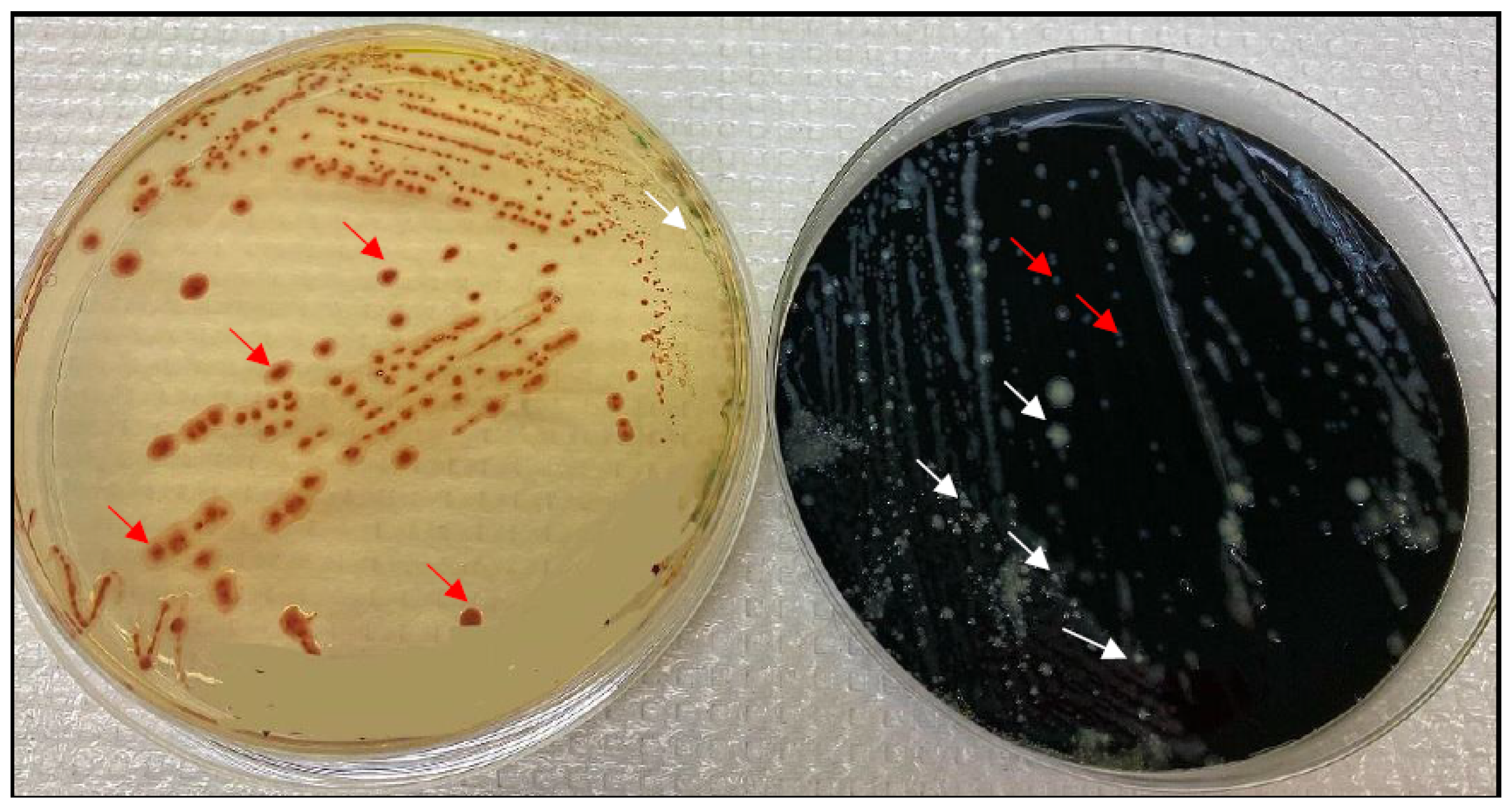
2.3. mCCDA vs. CHROMagar
3. Discussion
4. Materials and Methods
4.1. Sample Collection and Transport
4.2. Detection and Phenotypic Identification of Pathogen Species
4.3. Confirmation of Campylobacter Species Differentiation by Real-Time PCR Analysis
4.4. Data Analysis
4.5. Morbidity Surveillance Pyramid
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Report of an Expert Consultation. The Global View of Campylobacteriosis. 2013. Available online: https://apps.who.int/iris/handle/10665/80751 (accessed on 24 January 2022).
- Heymann, D.L. Control of Communicable Diseases Manual, 20th ed.; American Public Health Association, Alpha Press: Washington, DC, USA, 2014; ISBN 978-0-87553-018-5. [Google Scholar]
- Peterson, M.C. Clinical aspects of Campylobacter jejuni infections in adults. Western J. Med. 1994, 161, 148–152. [Google Scholar] [PubMed]
- Acheson, D.; Allos, B.M. Campylobacter jejuni Infections: Update on Emerging Issues and Trends. Clin. Infect. Dis. 2001, 32, 1201–1206. [Google Scholar] [CrossRef] [PubMed]
- Blaser, M.J.; Wells, J.G.; Feldman, R.A.; Pollard, R.A.; Allen, J.R. Campylobacter Enteritis in the United States. Ann. Intern. Med. 1983, 98, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Moffatt, C.R.M.; Kennedy, K.J.; O’Neill, B.; Selvey, L.; Kirk, M.D. Bacteraemia, antimicrobial susceptibility and treatment among Campylobacter-associated hospitalisations in the Australian Capital Territory: A review. BMC Infect. Dis. 2021, 21, 1–12. [Google Scholar] [CrossRef]
- Patrick, M.E.; Henao, O.L.; Robinson, T.; Geissler, A.L.; Cronquist, A.; Hanna, S.; Hurd, S.; Medalla, F.; Pruckler, J.; Mahon, B.E. Features of illnesses caused by five species ofCampylobacter, Foodborne Diseases Active Surveillance Network (FoodNet)—2010–2015. Epidemiol. Infect. 2017, 146, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Laughlin, M.E.; Chatham-Stephens, K.; Geissler, A.L. Campylobacteriosis. In CDC Yellow Book 2020: Health Information for International Travel; Brunette, G.W., Nemhauser, J.B., Eds.; Center for Disease Control and Prevention (CDC): New York, NY, USA; Oxford University Press: Oxford, UK, 2019. Available online: https://wwwnc.cdc.gov/travel/yellowbook/2020/travel-related-infectious-diseases/campylobacteriosis (accessed on 24 January 2022).
- Rosner, B.M.; Schielke, A.; Didelot, X.; Kops, F.; Breidenbach, J.; Willrich, N.; Gölz, G.; Alter, T.; Stingl, K.; Josenhans, C.; et al. A combined case-control and molecular source attribution study of human Campylobacter infections in Germany, 2011–2014. Sci. Rep. 2017, 7, 1–12. [Google Scholar] [CrossRef]
- Walter, E.J.S.; Crim, S.M.; Bruce, B.B.; Griffin, P.M. Incidence of Campylobacter-Associated Guillain-Barré Syndrome Estimated from Health Insurance Data. Foodborne Pathog. Dis. 2020, 17, 23–28. [Google Scholar] [CrossRef]
- Igwaran, A.; Okoh, A. Human campylobacteriosis: A public health concern of global importance. Heliyon 2019, 5, e02814. [Google Scholar] [CrossRef]
- Amour, C.; Gratz, J.; Mduma, E.R.; Svensen, E.; Rogawski, E.T.; McGrath, M.; Seidman, J.C.; McCormick, B.J.J.; Shrestha, P.S.; Samie, A.; et al. Epidemiology and Impact of Campylobacter Infection in Children in 8 Low-Resource Settings: Results From the MAL-ED Study. Clin. Infect. Dis. 2016, 63, 1171–1179. [Google Scholar] [CrossRef] [Green Version]
- Bian, X.; Garber, J.M.; Cooper, K.K.; Huynh, S.; Jones, J.; Mills, M.K.; Rafala, D.; Nasrin, D.; Kotloff, K.L.; Parker, C.; et al. Campylobacter Abundance in Breastfed Infants and Identification of a New Species in the Global Enterics Multicenter Study. mSphere 2020, 5, e00735-19. [Google Scholar] [CrossRef] [Green Version]
- Georgian Tourism in Figures—Structure & Industry Data of 2017. Ministry of Economy and Sustainable Development of Georgia (www.economy.ge). Georgian National Tourism Administration. Publication 2018. P.4. Available online: https://gnta.ge/wp-content/uploads/2018/07/2017-ENG.pdf (accessed on 24 January 2022).
- GEOSTAT. National Statistics Office of Georgia, 2021. Number of Population as of 1 January 2021. P.3. Available online: https://www.geostat.ge/en/single-news/2234/number-of-population-as-of-january-1-2021 (accessed on 24 January 2022).
- National Centre for Disease Control and Public Health (NCDC), Georgia. Available online: https://www.ncdc.ge (accessed on 24 January 2022).
- National Centre for Disease Control and Public Health (NCDC). Georgia. 0-15 Age Children’s Health Care Highlights Georgia in 2015 [In Georgian]. Available online: https://www.ncdc.ge/#/pages/file/a1f4f3c5-b524-4fa8-b736-9b52d607ff5b (accessed on 24 January 2022).
- National Agency of Environment (NEA). Ministry of Environmental Protection and Agriculture of Georgia. Available online: https://nea.gov.ge/En/ (accessed on 24 January 2022).
- Calva, J.J. Cohort study of intestinal infection with campylobacter in mexican children. Lancet 1988, 331, 503–506. [Google Scholar] [CrossRef]
- EMA (European Medicines Agency); EFSA (European Food Safety Authority). EMA and EFSA Joint Scientific Opinion on measures to reduce the need to use antimicrobial agents in animal husbandry in the European Union, and the resulting impacts on food safety (RONAFA). EFSA J. 2017, 15, 245. [Google Scholar] [CrossRef]
- Haagsma, J.A.; Geenen, P.L.; Ethelberg, S.; Fetsch, A.; Hansdotter, F.; Jansen, A.; Korsgaard, H.; O’Brian, S.J.; Scavia, G.; Spitznagel, H.; et al. Community incidence of pathogen-specific gastroenteritis: Reconstructing the surveillance pyramid for seven pathogens in seven European Union member states. Epidemiol. Infect. 2013, 141, 1625–1639. [Google Scholar] [CrossRef] [Green Version]
- Teramura, H.; Iwasaki, M.; Ogihara, H. Development of a Novel Chromogenic Medium for Improved Campylobacter Detection from Poultry Samples. J. Food Prot. 2015, 78, 1750–1755. [Google Scholar] [CrossRef]
- Repérant, E.; Laisney, M.; Nagard, B.; Quesne, S.; Rouxel, S.; Le Gall, F.; Chemaly, M.; Denis, M. Influence of enrichment and isolation media on the detection of Campylobacter spp. in naturally contaminated chicken samples. J. Microbiol. Methods 2016, 128, 42–47. [Google Scholar] [CrossRef]
- Sakran, W.; Hexner-Erlichman, Z.; Spiegel, R.; Batheesh, H.; Halevy, R.; Koren, A. Campylobacter gastroenteritis in children in north-eastern Israel comparison with other common pathogens. Sci. Rep. 2020, 10, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Shim, J.O.; Chang, J.Y.; Kim, A.; Shin, S. Different Age Distribution between Campylobacteriosis and Nontyphoidal Salmonellosis in Hospitalized Korean Children with Acute Inflammatory Diarrhea. J. Kor. Med. Sci. 2017, 32, 1202–1206. [Google Scholar] [CrossRef]
- Delahoy, M.J.; Wodnik, B.; McAliley, L.; Penakalapati, G.; Swarthout, J.; Freeman, M.C.; Levy, K. Pathogens transmitted in animal feces in low—And middle-income countries. Int. J. Hyg. Environ. Health 2018, 221, 661–676. [Google Scholar] [CrossRef]
- Veras, H.D.N.; Quetz, J.D.S.; Lima, I.F.N.; Rodrigues, T.S.; Havt, A.; Rey, L.C.; Mota, R.M.S.; Soares, A.M.; Singhal, M.; Weigl, B.; et al. Combination of different methods for detection of Campylobacter spp. in young children with moderate to severe diarrhea. J. Microbiol. Methods 2016, 128, 7–9. [Google Scholar] [CrossRef]
- Shawky, H.M.; Kamel, N.M.; Farghaly, E.M.; Samir, A. Isolation and molecular characterization of Campylobacter spp. in newly hatched poultry in Egypt. J. Glob. Biosci. 2015, 4, 2087–2091. [Google Scholar]
- Bolton, F.J.; Robertson, L. A selective medium for isolating Campylobacter jejuni/coli. J. Clin. Pathol. 1982, 35, 462–467. [Google Scholar] [CrossRef] [Green Version]
- Davis, L.; DiRita, V. Growth and laboratory maintenance of Campylobacter jejuni. Curr. Protoc. Microbiol. 2017, 10, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Wei, B.; Kang, M.; Jang, H.-K. Evaluation of potassium clavulanate supplementation of Bolton broth for enrichment and de-tection of Campylobacter from chicken. PLoS ONE 2018, 13, 1–13. [Google Scholar] [CrossRef]
- Sylte, M.; Inbody, M.; Johnson, T.; Looft, T.; Line, J. Evaluation of different Campylobacter jejuni isolates to colonize the intestinal tract of commercial turkey poults and selective media for enumeration. Poult. Sci. 2018, 97, 1689–1698. [Google Scholar] [CrossRef]
- Nataro, J.P.; Bopp, C.A.; Fields, P.I.; Kaper, J.B.; Strockbine, N.A.; Shigella, E. Salmonella. In Manual of Clinical Microbiology, 10th ed.; Versalovic, J., Carroll, K.C., Funke, G., Jorgensen, J.H., Landry, M.L., Warnock, D.W., Eds.; ASM Press: Washington, DC, USA, 2011; Volume 1, pp. 603–626. [Google Scholar]
- Mayr, A.M.; Lick, S.; Bauer, J.; Thärigen, D.; Busch, U.; Huber, I. Rapid Detection and Differentiation of Campylobacter jejuni, Campylobacter coli, and Campylobacter lari in Food, Using Multiplex Real-Time PCR. J. Food Prot. 2010, 73, 241–250. [Google Scholar] [CrossRef]
- Anderson, A.; Pietsch, K.; Zucker, R.; Mayr, A.; Müller-Hohe, E.; Messelhäusser, U.; Sing, A.; Busch, U.; Huber, I. Validation of a duplex real-time PCR for the detection of Salmonella spp. in different food products. Food Analyt. Methods 2011, 4, 259–267. [Google Scholar] [CrossRef]
- Gibbons, C.L.; Mangen, M.-J.J.; Plass, D.; Havelaar, A.H.; Brooke, R.J.; Kramarz, P.; Peterson, K.L.; Stuurman, A.L.; Cassini, A.; Fèvre, E.M.; et al. Measuring underreporting and under-ascertainment in infectious disease datasets: A comparison of methods. BMC Public Health 2014, 14, 147. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | |
|---|---|---|---|---|---|---|---|---|---|
| NT * salmonellosis | 76 | 42 | 51 | 24 | 43 | 60 | 102 | 99 | 100 |
| Shigellosis | 431 | 107 | 493 | 906 | 391 | 435 | 517 | 267 | 488 |
| Enterohaemorrhagic Escherichiosis | 4 | 3 | 2 | 0 | 1 | 2 | 19 | 13 | 26 |
| Campylobacteriosis | 3 | 2 | 0 | - | - | - | - | - | 2 |
| Diarrhea and Gastroenteritis of Presumed Infectious Origin | 19,305 | 18,344 | 18,081 | 19,841 | 17,596 | 10,337 | 11,963 | 10,019 | 7423 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Metreveli, M.; Bulia, S.; Shalamberidze, I.; Tevzadze, L.; Tsanava, S.; Goenaga, J.C.; Stingl, K.; Imnadze, P. Campylobacteriosis, Shigellosis and Salmonellosis in Hospitalized Children with Acute Inflammatory Diarrhea in Georgia. Pathogens 2022, 11, 232. https://doi.org/10.3390/pathogens11020232
Metreveli M, Bulia S, Shalamberidze I, Tevzadze L, Tsanava S, Goenaga JC, Stingl K, Imnadze P. Campylobacteriosis, Shigellosis and Salmonellosis in Hospitalized Children with Acute Inflammatory Diarrhea in Georgia. Pathogens. 2022; 11(2):232. https://doi.org/10.3390/pathogens11020232
Chicago/Turabian StyleMetreveli, Maia, Salome Bulia, Iamze Shalamberidze, Liana Tevzadze, Shota Tsanava, Juan Cruz Goenaga, Kerstin Stingl, and Paata Imnadze. 2022. "Campylobacteriosis, Shigellosis and Salmonellosis in Hospitalized Children with Acute Inflammatory Diarrhea in Georgia" Pathogens 11, no. 2: 232. https://doi.org/10.3390/pathogens11020232