
Risk Factors for the Development of Post-Infectious Bronchiolitis Obliterans in Children: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Publication Bias
2.6. Data Analysis
3. Results
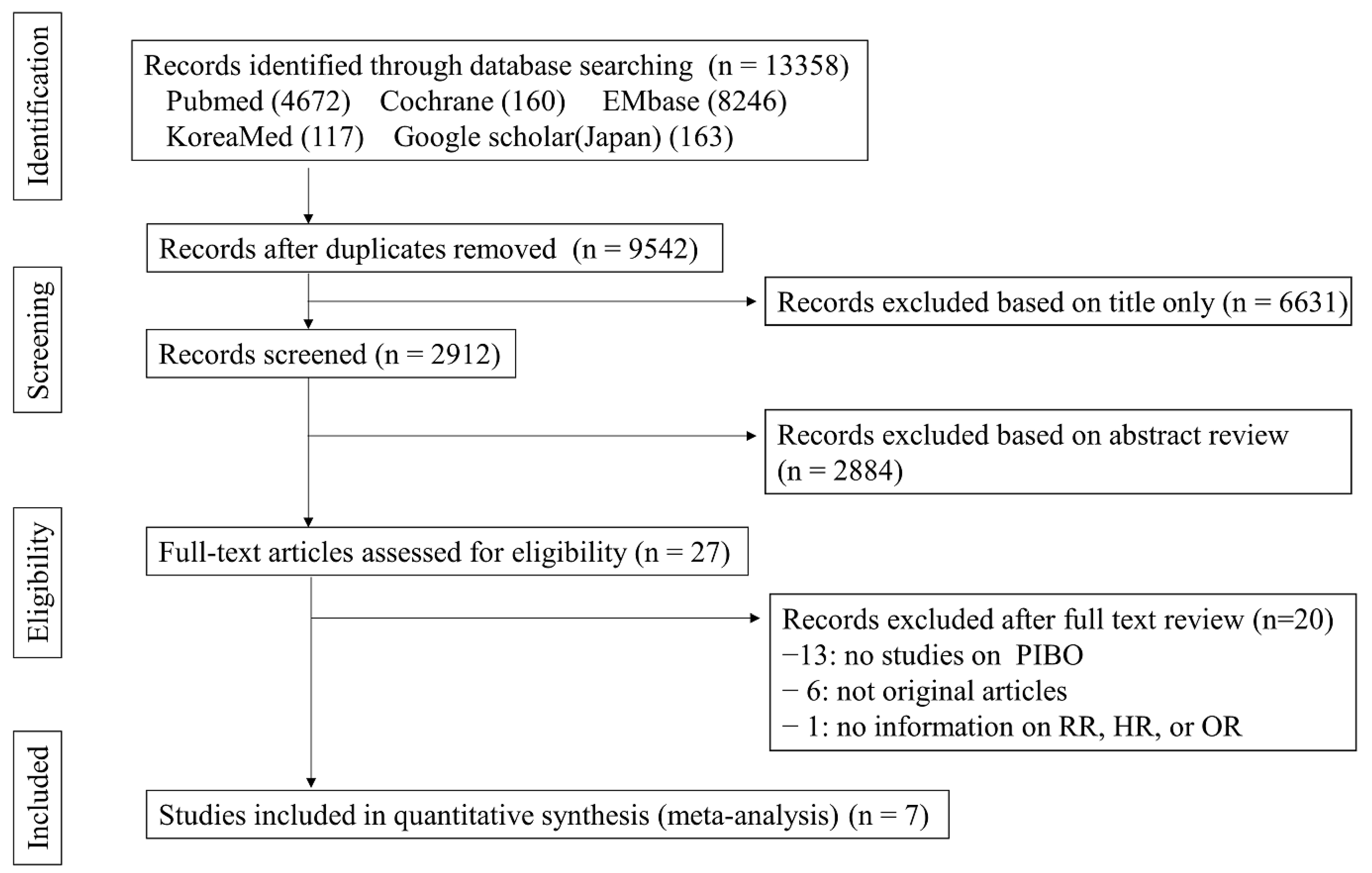
3.1. Study Selection and Characteristics
3.2. Study Quality
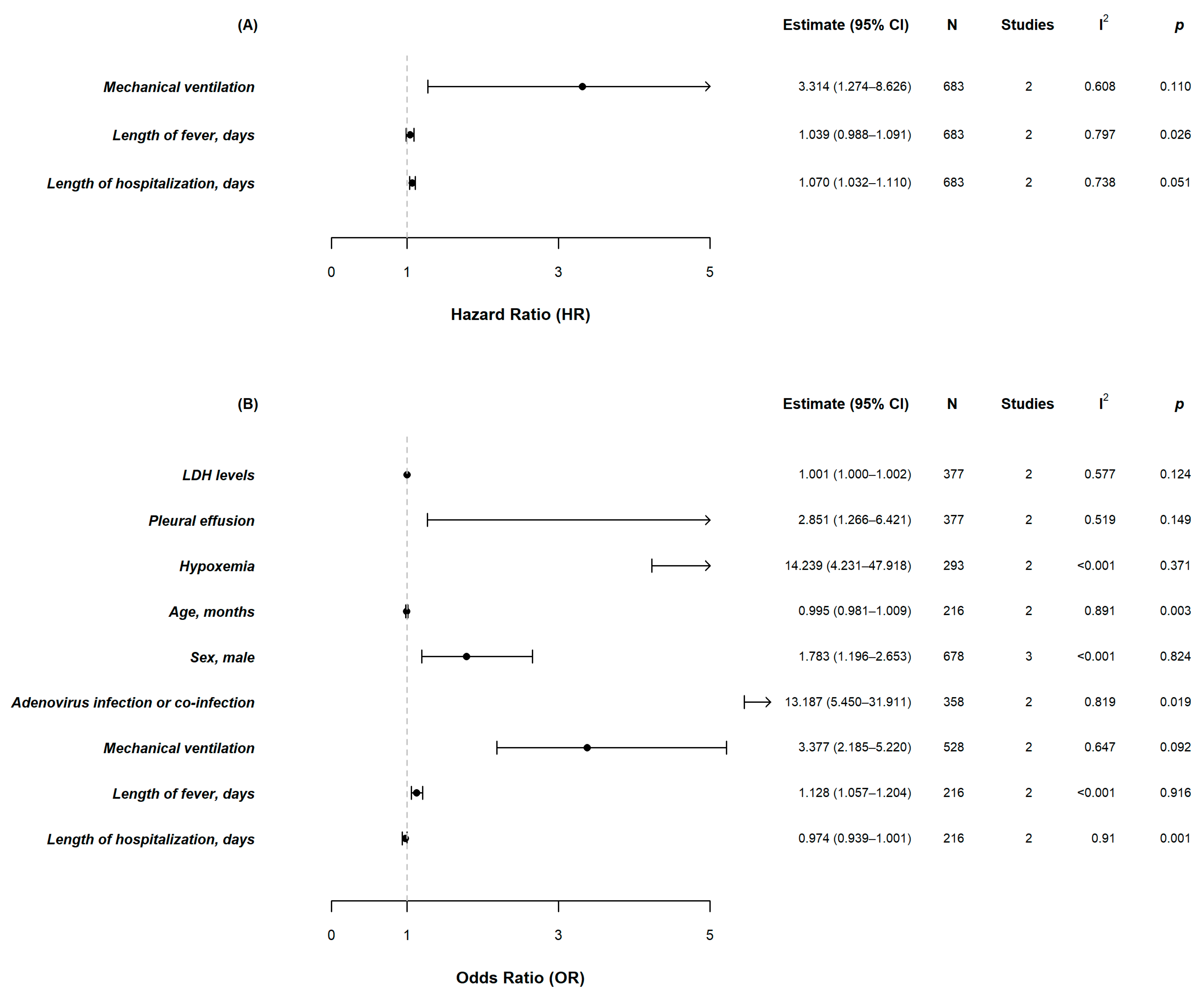
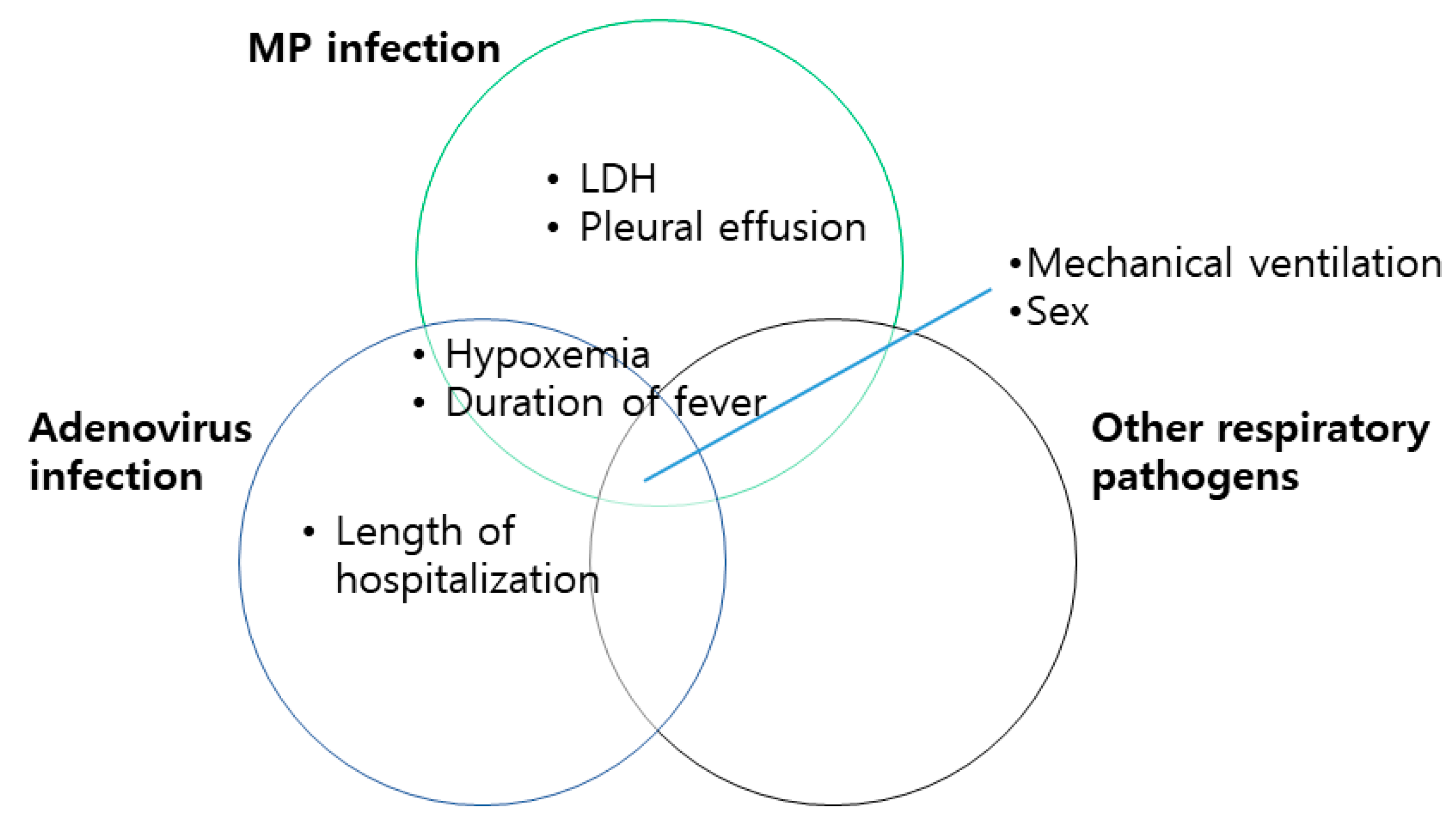
3.3. Risk Factors for the Development of PIBO
4. Discussions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Flanagan, F.; Casey, A.; Reyes-Mugica, M.; Kurland, G. Post-infectious bronchiolitis obliterans in children. Paediatr. Respir. Rev. 2022, 42, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Colom, A.J.; Teper, A.M. Post-infectious bronchiolitis obliterans. Pediatr. Pulmonol. 2019, 54, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Castleman, W.L. Bronchiolitis obliterans and pneumonia induced in young dogs by experimental adenovirus infection. Am. J. Pathol. 1985, 119, 495–504. [Google Scholar] [PubMed]
- Saraya, T.; Kurai, D.; Nakagaki, K.; Sasaki, Y.; Niwa, S.; Tsukagoshi, H.; Nunokawa, H.; Ohkuma, K.; Tsujimoto, N.; Hirao, S.; et al. Novel aspects on the pathogenesis of Mycoplasma pneumoniae pneumonia and therapeutic implications. Front. Microbiol. 2014, 5, 410. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [Green Version]
- Song, P.; Zhang, Y.; Yu, J.; Zha, M.; Zhu, Y.; Rahimi, K.; Rudan, I. Global Prevalence of Hypertension in Children: A Systematic Review and Meta-analysis. JAMA Pediatr. 2019, 173, 1154–1163. [Google Scholar] [CrossRef]
- Sterne, J.A.; Sutton, A.J.; Ioannidis, J.P.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rucker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [Green Version]
- Lee, E.; Young Lee, Y. Risk factors for the development of post-infectious bronchiolitis obliterans after Mycoplasma pneumoniae pneumonia in the era of increasing macrolide resistance. Respir. Med. 2020, 175, 106209. [Google Scholar] [CrossRef]
- Huang, K.; Liu, J.; Lv, W.; Chu, Y.; Li, B.; Wu, P.; Shuai, J. Analysis of Risk Factors of Bronchiolitis Obliterans in Children with Mycoplasma pneumoniae Bronchiolitis. Comput. Math. Methods Med. 2022, 2022, 9371406. [Google Scholar] [CrossRef]
- Murtagh, P.; Giubergia, V.; Viale, D.; Bauer, G.; Pena, H.G. Lower respiratory infections by adenovirus in children. Clinical features and risk factors for bronchiolitis obliterans and mortality. Pediatr. Pulmonol. 2009, 44, 450–456. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.Q.; Li, X.; Jiang, W.H.; Yin, G.Q.; Lei, A.H.; Xiao, Q.; Huang, J.J.; Xie, Z.W.; Deng, L. Hypoxemia is an independent predictor of bronchiolitis obliterans following respiratory adenoviral infection in children. Springerplus 2016, 5, 1622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, X.; Ma, Y.; Gao, Y.; You, H. Epidemiology of Adenovirus Pneumonia and Risk Factors for Bronchiolitis Obliterans in Children During an Outbreak in Jilin, China. Front. Pediatr. 2021, 9, 722885. [Google Scholar] [CrossRef]
- Zhong, L.; Lin, J.; Dai, J. Risk factors for the development of bronchiolitis obliterans in children with severe adenovirus pneumonia: A retrospective study with dose-response analysis. J. Med. Virol. 2020, 92, 3093–3099. [Google Scholar] [CrossRef] [PubMed]
- Colom, A.J.; Teper, A.M.; Vollmer, W.M.; Diette, G.B. Risk factors for the development of bronchiolitis obliterans in children with bronchiolitis. Thorax 2006, 61, 503–506. [Google Scholar] [CrossRef] [Green Version]
- He, J.; Liu, M.; Ye, Z.; Tan, T.; Liu, X.; You, X.; Zeng, Y.; Wu, Y. Insights into the pathogenesis of Mycoplasma pneumoniae. Mol. Med. Rep. 2016, 14, 4030–4036. [Google Scholar] [CrossRef] [Green Version]
- Poddighe, D. Extra-pulmonary diseases related to Mycoplasma pneumoniae in children: Recent insights into the pathogenesis. Curr. Opin. Rheumatol. 2018, 30, 380–387. [Google Scholar] [CrossRef]
- Saraya, T.; Nakata, K.; Nakagaki, K.; Motoi, N.; Iihara, K.; Fujioka, Y.; Oka, T.; Kurai, D.; Wada, H.; Ishii, H.; et al. Identification of a mechanism for lung inflammation caused by Mycoplasma pneumoniae using a novel mouse model. Results Immunol. 2011, 1, 76–87. [Google Scholar] [CrossRef] [Green Version]
- Han, H.Y.; Park, K.C.; Yang, E.A.; Lee, K.Y. Macrolide-Resistant and Macrolide-Sensitive Mycoplasma pneumoniae Pneumonia in Children Treated Using Early Corticosteroids. J. Clin. Med. 2021, 10, 1309. [Google Scholar] [CrossRef]
- Zhu, Z.; Zhang, T.; Guo, W.; Ling, Y.; Tian, J.; Xu, Y. Clinical characteristics of refractory mycoplasma pneumoniae pneumonia in children treated with glucocorticoid pulse therapy. BMC Infect. Dis. 2021, 21, 126. [Google Scholar] [CrossRef]
- Caiazzo, E.; Rezig, A.O.M.; Bruzzese, D.; Ialenti, A.; Cicala, C.; Cleland, J.G.F.; Guzik, T.J.; Maffia, P.; Pellicori, P. Systemic administration of glucocorticoids, cardiovascular complications and mortality in patients hospitalised with COVID-19, SARS, MERS or influenza: A systematic review and meta-analysis of randomised trials. Pharmacol. Res. 2022, 176, 106053. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Choi, I. Clinical Usefulness of Serum Lactate Dehydrogenase Levels in Mycoplasma pneumoniae Pneumonia in Children. Indian J. Pediatr. 2022, 89, 1003–1009. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Lee, E.; Song, E.S.; Lee, Y.Y. Clinical Significance of Pleural Effusion in Mycoplasma pneumoniae Pneumonia in Children. Pathogens 2021, 10, 1075. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Jung, S.; Kim, M.; Park, S.; Yang, H.J.; Lee, E. Global Trends in the Proportion of Macrolide-Resistant Mycoplasma pneumoniae Infections: A Systematic Review and Meta-analysis. JAMA Netw. Open 2022, 5, e2220949. [Google Scholar] [CrossRef]
- Gray, G.C.; McCarthy, T.; Lebeck, M.G.; Schnurr, D.P.; Russell, K.L.; Kajon, A.E.; Landry, M.L.; Leland, D.S.; Storch, G.A.; Ginocchio, C.C.; et al. Genotype prevalence and risk factors for severe clinical adenovirus infection, United States 2004–2006. Clin. Infect. Dis. 2007, 45, 1120–1131. [Google Scholar] [CrossRef] [Green Version]
- Crenshaw, B.J.; Jones, L.B.; Bell, C.R.; Kumar, S.; Matthews, Q.L. Perspective on Adenoviruses: Epidemiology, Pathogenicity, and Gene Therapy. Biomedicines 2019, 7, 61. [Google Scholar] [CrossRef] [Green Version]
- Rouse, B.T.; Sehrawat, S. Immunity and immunopathology to viruses: What decides the outcome? Nat. Rev. Immunol. 2010, 10, 514–526. [Google Scholar] [CrossRef]
- Liu, D.; Liu, J.; Zhang, L.; Chen, Y.; Zhang, Q. Risk Factors for Post-infectious Bronchiolitis Obliterans in Children: A Systematic Review and Meta-Analysis. Front. Pediatr. 2022, 10, 881908. [Google Scholar] [CrossRef]
- Jerkic, S.P.; Brinkmann, F.; Calder, A.; Casey, A.; Dishop, M.; Griese, M.; Kurland, G.; Niemitz, M.; Nyilas, S.; Schramm, D.; et al. Postinfectious Bronchiolitis Obliterans in Children: Diagnostic Workup and Therapeutic Options: A Workshop Report. Can. Respir. J. 2020, 2020, 5852827. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Risk Factors | Study (Year) | Variables | OR | Lower 95% CI | Upper 95% CI | p Value | Tau2 | I2 | Q Statistic | Degree of Freedom (Q) | p Value (Q) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Respiratory virus co-infection | |||||||||||
| Lee E et al. (2020) [9] | multivariate | 4.069 | 1.224 | 13.523 | |||||||
| Summary statistics | 4.069 | 1.224 | 13.527 | 0.022 | |||||||
| Co-infections with RSV | |||||||||||
| Murtagh P et al. (2009) [11] | univariate | 4.100 | 1.500 | 10.600 | |||||||
| Summary statistics | 4.100 | 1.500 | 11.207 | 0.006 | |||||||
| LDH | |||||||||||
| Lee E et al. (2020) [9] | multivariate | 1.001 | 1.000 | 1.003 | |||||||
| Huang K et al. (2012) [10] | multivariate | 1.005 | 1.000 | 1.009 | |||||||
| Summary statistics | 1.001 | 1.000 | 1.002 | 0.021 | 0.002 | 0.577 | 2.361 | 1.000 | 0.124 | ||
| Poor response to treatment | |||||||||||
| Lee E et al. (2020) [9] | multivariate | 41.760 | 2.792 | 624.543 | |||||||
| Summary statistics | 41.760 | 2.792 | 624.574 | 0.007 | |||||||
| Duration of moist rale | |||||||||||
| Huang K et al. (2012) [10] | multivariate | 1.203 | 1.066 | 1.358 | |||||||
| Summary statistics | 1.203 | 1.066 | 1.358 | 0.003 | |||||||
| Hypoxemia | |||||||||||
| Huang K et al. (2012) [10] | multivariate | 7.442 | 1.148 | 48.225 | |||||||
| Yu X et al. (2021) [13] | univariate | 22.846 | 4.633 | 112.666 | |||||||
| Summary statistics | 14.239 | 4.231 | 47.918 | <0.001 | 0.000 | 0.000 | 0.800 | 1.000 | 0.371 | ||
| Pleural effusion | |||||||||||
| Lee E et al. (2020) [9] | multivariate | 1.272 | 0.325 | 4.969 | |||||||
| Huang K et al. (2012) [10] | multivariate | 4.437 | 1.616 | 12.181 | |||||||
| Summary statistics | 2.851 | 1.266 | 6.421 | 0.011 | 0.637 | 0.519 | 2.081 | 1.000 | 0.149 | ||
| Adenovirus infection or adenovirus co-infection | |||||||||||
| Lee E et al. (2020) [9] | multivariate | 5.607 | 1.801 | 17.454 | |||||||
| Colom AJ et al. (2006) [15] | multivariate | 49.000 | 12.000 | 199.000 | |||||||
| Summary statistics | 13.187 | 5.450 | 31.911 | <0.001 | 1.387 | 0.819 | 5.522 | 1.000 | 0.019 | ||
| Mechanical ventilation | |||||||||||
| Colom AJ et al. (2006) [15] | multivariate | 11.000 | 2.600 | 45.000 | |||||||
| Murtagh P et al. (2009) [11] | univariate | 3.000 | 1.900 | 4.600 | |||||||
| Summary statistics | 3.377 | 2.185 | 5.220 | <0.001 | 0.739 | 0.647 | 2.833 | 1.000 | 0.092 | ||
| >30 days of Hospitalization | |||||||||||
| Murtagh P et al. (2009) [11] | multivariate | 27.200 | 14.600 | 50.900 | |||||||
| Summary statistics | 27.200 | 14.600 | 50.673 | <0.001 | |||||||
| Length of hospitalization, days | |||||||||||
| Lee E et al. (2020) [9] | multivariate | 1.102 | 1.016 | 1.194 | |||||||
| Yu X et al. (2021) [13] | univariate | 0.944 | 0.906 | 0.985 | |||||||
| Summary statistics | 0.974 | 0.939 | 1.011 | 0.163 | 0.104 | 0.910 | 11.098 | 1.000 | 0.001 | ||
| Multifocal pneumonia | |||||||||||
| Murtagh P et al. (2009) [11] | multivariate | 26.600 | 5.300 | 132.000 | |||||||
| Summary statistics | 26.600 | 5.300 | 133.498 | <0.001 | |||||||
| Hypercapnia | |||||||||||
| Murtagh P et al. (2009) [11] | multivariate | 5.600 | 3.500 | 9.000 | |||||||
| Summary statistics | 5.600 | 3.500 | 8.960 | <0.001 | |||||||
| Persistent wheezing | |||||||||||
| Yu X et al. (2021) [13] | multivariate | 181.776 | 3.385 | 9761.543 | |||||||
| Summary statistics | 181.776 | 3.385 | 9760.737 | 0.011 | |||||||
| Respiratory failure | |||||||||||
| Yu X et al. (2021) [13] | multivariate | 51.288 | 1.858 | 1415.441 | |||||||
| Summary statistics | 51.288 | 1.858 | 1415.661 | 0.020 | |||||||
| Length of fever, days | |||||||||||
| Lee E et al. (2020) [9] | multivariate | 1.133 | 1.024 | 1.255 | |||||||
| Yu X et al. (2021) [13] | univariate | 1.125 | 1.033 | 1.226 | |||||||
| Summary statistics | 1.128 | 1.057 | 1.204 | 0.000 | 0.000 | 0.000 | 0.011 | 1.000 | 0.916 | ||
| Dyspnea | |||||||||||
| Yu X et al. (2021) [13] | univariate | 10.625 | 2.702 | 41.779 | |||||||
| Summary statistics | 10.625 | 2.702 | 41.779 | 0.001 | |||||||
| Age (mo) | |||||||||||
| Lee E et al. (2020) [9] | multivariate | 0.990 | 0.976 | 1.003 | |||||||
| Yu X et al. (2021) [13] | univariate | 1.097 | 1.028 | 1.170 | |||||||
| Summary statistics | 0.995 | 0.981 | 1.009 | 0.452 | 0.069 | 0.891 | 9.148 | 1.000 | 0.003 | ||
| Sex, male | |||||||||||
| Lee E et al. (2020) [9] | multivariate | 1.570 | 0.569 | 4.329 | |||||||
| Colom AJ et al. (2006) [15] | multivariate | 1.250 | 0.385 | 5.000 | |||||||
| Murtagh P et al. (2009) [11] | univariate | 1.901 | 1.200 | 3.003 | |||||||
| Summary statistics | 1.783 | 1.196 | 2.653 | 0.005 | 0.000 | 0.000 | 0.387 | 2.000 | 0.824 | ||
| Adenovirus 7 h serotype | |||||||||||
| Murtagh P et al. (2009) [11] | univariate | 1.900 | 1.000 | 3.900 | |||||||
| Summary statistics | 1.900 | 1.000 | 3.610 | 0.050 | |||||||
| Exposure to ETS at present | |||||||||||
| Colom AJ et al. (2006) [15] | univariate | 1.400 | 0.400 | 4.500 | |||||||
| Summary statistics | 1.400 | 0.400 | 4.900 | 0.599 | |||||||
| Dyspnea | |||||||||||
| Zhong L et al. (2020) [14] | multivariate | 3.922 | 1.060 | 14.511 | |||||||
| Summary statistics | 3.922 | 1.060 | 14.511 | 0.041 | |||||||
| Length of fever, days | |||||||||||
| Wu PQ et al. (2016) [12] | multivariate | 1.000 | 0.942 | 1.062 | |||||||
| Zhong L et al. (2020) [14] | multivariate | 1.129 | 1.033 | 1.234 | |||||||
| Summary statistics | 1.039 | 0.988 | 1.091 | 0.135 | 0.077 | 0.797 | 4.932 | 1.000 | 0.026 | ||
| Length of hospitalization, days | |||||||||||
| Wu PQ et al. (2016) [12] | multivariate | 1.044 | 0.999 | 1.091 | |||||||
| Zhong L et al. (2020) [14] | univariate | 1.129 | 1.058 | 1.205 | |||||||
| Summary statistics | 1.070 | 1.032 | 1.110 | 0.000 | 0.048 | 0.738 | 3.821 | 1.000 | 0.051 | ||
| Hypoxemia | |||||||||||
| Wu PQ et al. (2016) [12] | multivariate | 5.046 | 1.170 | 21.762 | |||||||
| Summary statistics | 5.046 | 1.170 | 21.762 | 0.030 | |||||||
| Length of mechanical ventilation | |||||||||||
| Zhong L et al. (2020) [14] | univariate | 1.103 | 1.013 | 1.201 | |||||||
| Summary statistics | 1.103 | 1.013 | 1.201 | 0.024 | |||||||
| Mechanical ventilation | |||||||||||
| Wu PQ et al. (2016) [12] | multivariate | 1.438 | 0.354 | 5.841 | |||||||
| Zhong L et al. (2020) [14] | multivariate | 6.861 | 1.854 | 25.390 | |||||||
| Summary statistics | 3.314 | 1.274 | 8.626 | 0.014 | 0.862 | 0.608 | 2.551 | 1.000 | 0.110 | ||
| Study Author, Year | Country | Study Duration | Pathogens | Number | Age, Mean (SD)/Median (IQR)/Range | Risk Factors | Statistics | ||
|---|---|---|---|---|---|---|---|---|---|
| Control | PIBO | Control | PIBO | ||||||
| Lee E et al. (2020) [9] | South Korea | May 2019–February 2020 | MP | 132 | 18 | 6.1 (±3.9) y | 4.8 (±2.6) y | Respiratory virus co-infection, duration between symptom onset and admission, LDH, poor response to treatment, adenovirus co-infection, length of fever | aOR |
| Huang K et al. (2012) [10] | China | January 2018–June 2020 | MP | 195 | 32 | 5 (3–6) y | 5 (3–7) y | Duration of moist rale, LDH, hypoxemia, pleural effusion | aOR |
| Colom AJ et al. (2006) [15] | Argentina | 1991–2002 | NA | 99 | 109 | 0–3 y | 0–3 y | Adenovirus infection, mechanical ventilation | aOR |
| Murtagh P et al. (2009) [11] | Argentina | March 1998–May 2005 | Adenovirus | 203 | 117 | 11.2 (±10.6) y | 10.5 (±8.8) y | >30 days of hospitalization, multifocal pneumonia, hypercapnia | aOR |
| Wu PQ et al. (2016) [12] | China | January 2011–December 2014 | Adenovirus | 530 | 14 | 23.5 (1–144) m | 15.5 (6–72) m | Hypoxemia | HR |
| Yu X et al. (2021) [13] | China | October 2018–January 2020 | Adenovirus | 46 | 20 | 30.5 (17.0–50.8) m | 16.5 (11.0–25.3) m | Persistent wheezing, respiratory failure | aOR |
| Zhong L et al. (2020) [14] | China | January 2015–February 2019 | Adenovirus | 105 | 34 | 20.5 (±14.6) m | 15.1 (±7.2) m | Length of fever, dyspnea, invasive mechanical ventilation | HR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, E.; Park, S.; Kim, K.; Yang, H.-J. Risk Factors for the Development of Post-Infectious Bronchiolitis Obliterans in Children: A Systematic Review and Meta-Analysis. Pathogens 2022, 11, 1268. https://doi.org/10.3390/pathogens11111268
Lee E, Park S, Kim K, Yang H-J. Risk Factors for the Development of Post-Infectious Bronchiolitis Obliterans in Children: A Systematic Review and Meta-Analysis. Pathogens. 2022; 11(11):1268. https://doi.org/10.3390/pathogens11111268
Chicago/Turabian StyleLee, Eun, Suyeon Park, Kyunghoon Kim, and Hyeon-Jong Yang. 2022. "Risk Factors for the Development of Post-Infectious Bronchiolitis Obliterans in Children: A Systematic Review and Meta-Analysis" Pathogens 11, no. 11: 1268. https://doi.org/10.3390/pathogens11111268