1. Introduction
The pathogenesis of colorectal cancer is marked by accumulating mutations in pathways of cell cycle, proliferation and cell death leading to uncontrolled tumor growth [
1]. However, the role of the tumor microenvironment for the progression and prognosis of colorectal cancer has recently gained increasing attention [
2]. This microenvironment also includes the intestinal microbiota and potentially non-autochthonous bacteria, which have a crucial function for colorectal carcinogenesis [
3]. In particular, a negative impact of
Fusobacterium nucleatum including increased proliferation of colorectal cancer cells [
4], the promotion of metastases [
5] and resistance to chemotherapy [
6] has been demonstrated.
Here, we report the unique case of a patient with systemic infection with Fusobacterium nucleatum that resulted in the diagnosis of rectal cancer and facilitated successful therapy.
2. Case Report
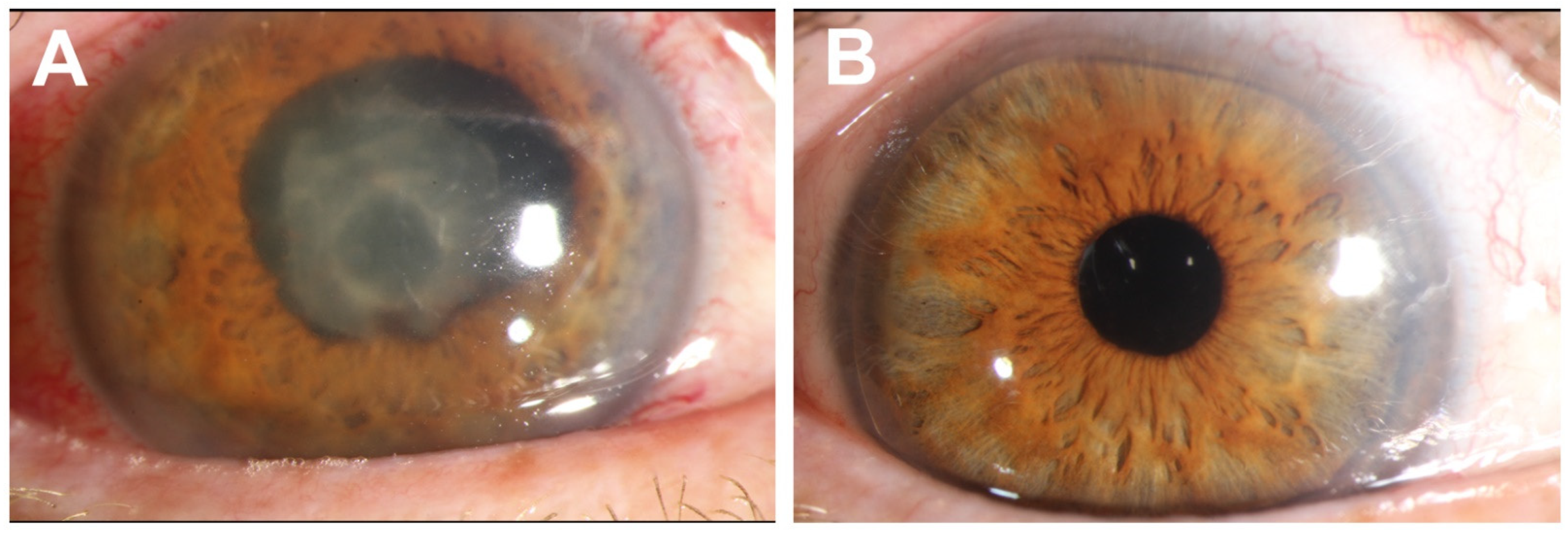
We describe the case of a 47-year-old male Caucasian patient who presented with progressive loss of vision on the right eye. He also reported abdominal discomfort over the past three weeks as well as fevers and chills during the previous 10 days.
Upon admission, the patient had a temperature of 39 °C. Clinical examination revealed a hypopyon of the right eye (
Figure 1A). Laboratory tests showed elevated leukocyte counts (20.56 G/L), abnormal liver function tests (GPT 97 U/L) and a C-reactive protein level of 172 mg/L (normal < 5 mg/L). The diagnosis of endophthalmitis was made and immediate vitrectomy was performed. Empiric antibiotic treatment with meropenem and vancomycin was initiated.
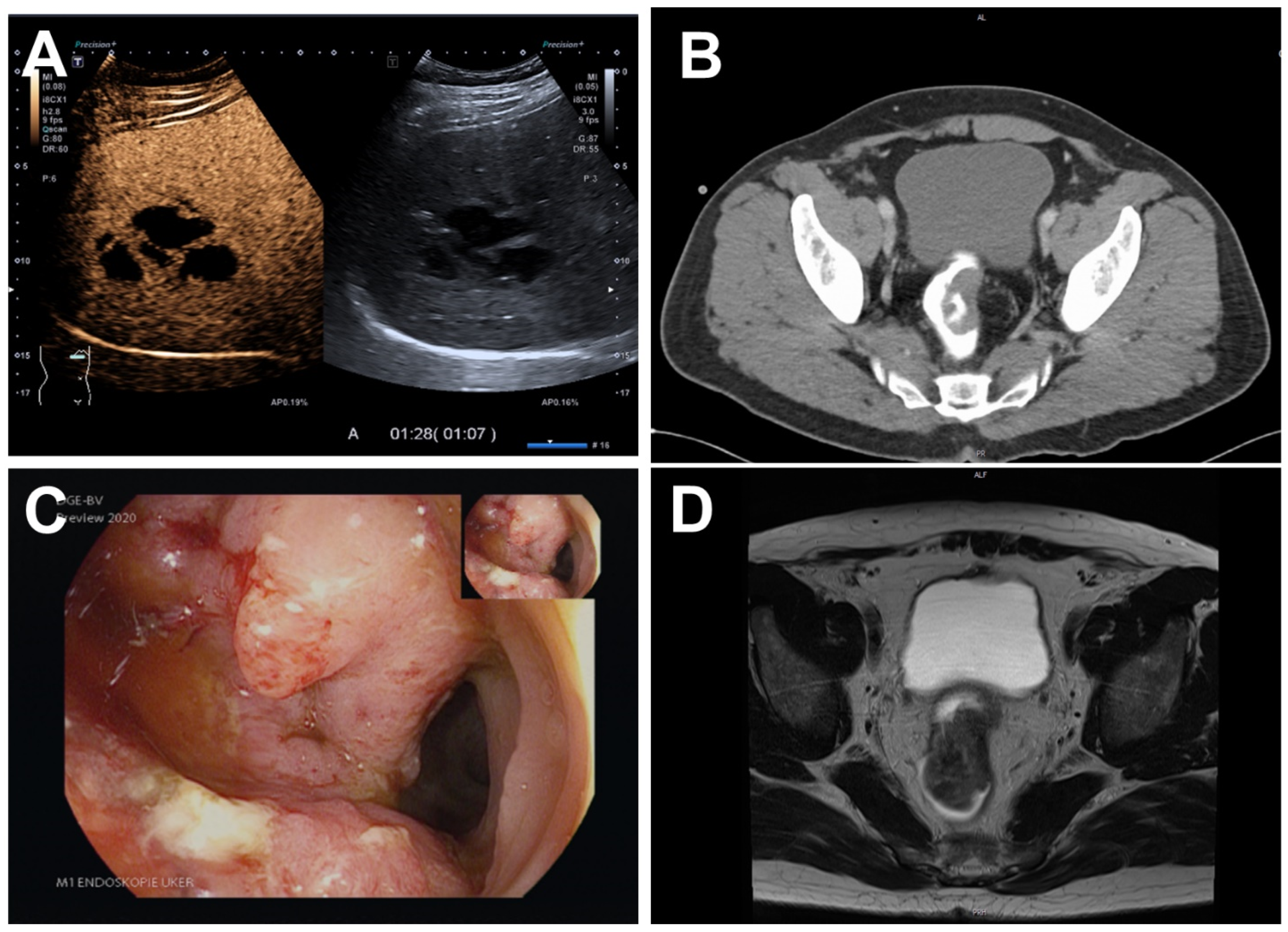
Upon referral to diagnostic ultrasound, B-mode sonography and contrast-enhanced ultrasound (
Figure 2A) identified an abscess in the right liver lobe. A 10 French pigtail drainage catheter was placed.
No pathogens grew in blood cultures and cultures of the vitreous humor. Real-time PCR of the vitreous humor was negative for Tropheryma whipplei, Staphylococcus aureus, cytomegalovirus, herpes simplex and varicella zoster virus DNA. Serologic results for galactomannan, Candida antigen, beta-D-glucan, Borrelia burgdorferi and Treponema pallidum were negative. However, PCR of the vitreous humor and the liver abscess using pan-bacterial primers were positive and Fusobacterium nucleatum was exclusively detected by sequence analysis (sequencing performed by eurofins) in both materials. Moreover, Fusobacterium nucleatum grew on Schaedler agar with vitamin K and was subsequently detected by mass spectrometry (MALDI-TOF) in cultures of the liver abscess. Since a dental focus had been ruled out a few days prior to hospital admission, these results were overall consistent with systemic Fusobacterium nucleatum infection without an obvious port of entry.
Hence, a thoracic/abdominal/pelvic CT scan revealed a tumor in the rectum (
Figure 2B) in addition to the known liver abscess in segment 6/7. Consistently, colonoscopy was suspicious for rectal cancer (
Figure 2C) and histopathological analysis confirmed a moderately differentiated intestinal-type adenocarcinoma. Staging including MRI of the pelvis characterized the carcinoma as cT3b cN0 (
Figure 2D).
The drainage of the liver abscess was stopped after four days. Antibiotic treatment included four weeks of IV meropenem followed by four weeks of an oral sequential therapy with amoxicillin/clavulanic acid. Activity against
Fusobacterium nucleatum has previously been demonstrated for both agents [
7]. Follow-up liver B-mode sonography showed consolidation of the abscess at 10 days and a complete resolution after 6 weeks. Following further ophthalmologic interventions, the patient partially regained vision (
Figure 1B). With regards to rectal cancer, he received neoadjuvant radio-chemotherapy, deep anterior rectum resection and adjuvant radiochemotherapy.
3. Discussion
Taken together, we consider the rectal cancer as the most likely source of invasive infection with
Fusobacterium nucleatum in this patient.
Fusobacterium nucleatum is an oral bacterium rarely found in healthy gut and colorectal cancer is a precondition for its colonization [
8]. Several bacterial species have previously been linked to colorectal carcinogenesis [
9] and recent studies even suggested a causal role for
Fusobacterium nucleatum [
4,
10,
11]. Although we were not able to verify the presence of
Fusobacterium nucleatum in cancer tissue from our patient, we did not find an oral–gingival or other port of entry. Notably, in contrast to vitreous humor and liver abscess material, tissue samples were obtained after several days of antibiotic treatment substantially reducing the probability of successful detection [
12].
Thus, to our knowledge, we describe the first case of undiagnosed colorectal cancer presenting primarily with systemic infection with Fusobacterium nucleatum. It shows that bacteria involved in the pathogenesis of colorectal cancer may not only play a local role, but also become invasive. This highlights the necessity to consider colorectal cancer in the differential diagnosis of systemic infection with Fusobacterium nucleatum and to include endoscopy in the diagnostic work-up, since this might expedite diagnosis and treatment and, thus, improve prognosis.
Author Contributions
S.Z.: diagnostic ultrasound/contrast-enhanced ultrasound, interventional ultrasound, diagnostic endoscopy, drafting of the manuscript; C.M.: ophthalmologic diagnosis and surgery; S.B.: histopathologic diagnosis; F.V.: diagnostic endoscopy; R.S. revised manuscript, infectious disease consultation; J.F.: infectious disease consultation; M.F.N.: supervision of diagnostic and therapeutic management; D.S.: diagnostic ultrasound/contrast-enhanced ultrasound, interventional ultrasound. All authors have read and agreed to the published version of the manuscript.
Funding
We acknowledge financial support by Deutsche Forschungsgemeinschaft and Friedrich-Alexander-Universität Erlangen-Nürnberg within the funding programme “Open Access Publication Funding”.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Weitz, J.; Koch, M.; Debus, J.; Höhler, T.; Galle, P.R.; Büchler, M.W. Colorectal Cancer. Lancet Lond. Engl. 2005, 365, 153–165. [Google Scholar] [CrossRef]
- Schmitt, M.; Greten, F.R. The Inflammatory Pathogenesis of Colorectal Cancer. Nat. Rev. Immunol. 2021, 21, 653–667. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Chan, A.T.; Sun, J. Influence of the Gut Microbiome, Diet, and Environment on Risk of Colorectal Cancer. Gastroenterology 2020, 158, 322–340. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Weng, W.; Peng, J.; Hong, L.; Yang, L.; Toiyama, Y.; Gao, R.; Liu, M.; Yin, M.; Pan, C.; et al. Fusobacterium Nucleatum Increases Proliferation of Colorectal Cancer Cells and Tumor Development in Mice by Activating Toll-Like Receptor 4 Signaling to Nuclear Factor-ΚB, and Up-Regulating Expression of MicroRNA-21. Gastroenterology 2017, 152, 851–866.e24. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Fan, L.; Lin, Y.; Shen, W.; Qi, Y.; Zhang, Y.; Chen, Z.; Wang, L.; Long, Y.; Hou, T.; et al. Fusobacterium Nucleatum Promotes Colorectal Cancer Metastasis through MiR-1322/CCL20 Axis and M2 Polarization. Gut Microbes 2021, 13, 1980347. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.; Guo, F.; Yu, Y.; Sun, T.; Ma, D.; Han, J.; Qian, Y.; Kryczek, I.; Sun, D.; Nagarsheth, N.; et al. Fusobacterium Nucleatum Promotes Chemoresistance to Colorectal Cancer by Modulating Autophagy. Cell 2017, 170, 548–563.e16. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, U.; Manncke, B.; Gerbracht, K.; Werner, H. In Vitro Activity of Meropenem Compared with Imipenem, Metronidazole, Ampicillin, and Ampicillin/Sulbactam against Anaerobes. Arzneimittel-Forschung 1994, 44, 859–862. [Google Scholar] [PubMed]
- Wang, S.; Liu, Y.; Li, J.; Zhao, L.; Yan, W.; Lin, B.; Guo, X.; Wei, Y. Fusobacterium Nucleatum Acts as a Pro-Carcinogenic Bacterium in Colorectal Cancer: From Association to Causality. Front. Cell Dev. Biol. 2021, 9, 710165. [Google Scholar] [CrossRef]
- Tilg, H.; Adolph, T.E.; Gerner, R.R.; Moschen, A.R. The Intestinal Microbiota in Colorectal Cancer. Cancer Cell 2018, 33, 954–964. [Google Scholar] [CrossRef] [PubMed]
- Bullman, S.; Pedamallu, C.S.; Sicinska, E.; Clancy, T.E.; Zhang, X.; Cai, D.; Neuberg, D.; Huang, K.; Guevara, F.; Nelson, T.; et al. Analysis of Fusobacterium Persistence and Antibiotic Response in Colorectal Cancer. Science 2017, 358, 1443–1448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesa, F.; Mesa-López, M.J.; Egea-Valenzuela, J.; Benavides-Reyes, C.; Nibali, L.; Ide, M.; Mainas, G.; Rizzo, M.; Magan-Fernandez, A. A New Comorbidity in Periodontitis: Fusobacterium Nucleatum and Colorectal Cancer. Medicina 2022, 58, 546. [Google Scholar] [CrossRef] [PubMed]
- Scheer, C.; Fuchs, C.; Gründling, M.; Vollmer, M.; Bast, J.; Bohnert, J.; Zimmermann, K.; Hahnenkamp, K.; Rehberg, S.; Kuhn, S.-O. Impact of Antibiotic Administration on Blood Culture Positivity at the Beginning of Sepsis: A Prospective Clinical Cohort Study. Clin. Microbiol. Infect. 2018, 25, 326–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, {kind=link}
{kind=link}

