
Lessons from SARS-CoV-2 Pandemics: How Restrictive Measures Impacted the Trend of Respiratory Infections in Neonates and Infants up to Three Months of Age
 , ,
, ,  , , , , , , , , and
, , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, J.D.; Rhinehart, E.; Jackson, M.; Chiarello, L.; Health Care Infection Control Practices Advisory Committee. 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Health Care Settings. Am. J. Infect. Control 2007, 35, S65–S164. [Google Scholar] [PubMed]
- Haapanen, M.; Renko, M.; Artama, M.; Kuitunen, I. The impact of the lockdown and the re-opening of schools and day cares on the epidemiology of SARS-CoV-2 and other respiratory infections in children-A nationwide register study in Finland. EClinicalMedicine 2021, 34, 100807. [Google Scholar] [CrossRef] [PubMed]
- Angoulvant, F.; Ouldali, N.; Yang, D.D.; Filser, M.; Gajdos, V.; Rybak, A.; Guedj, R.; Soussan-Banini, V.; Basmaci, R.; Lefevre-Utile, A.; et al. Coronavirus Disease 2019 Pandemic: Impact Caused by School Closure and National Lockdown on Pediatric Visits and Admissions for Viral and Nonviral Infections-a Time Series Analysis. Clin. Infect. Dis. 2021, 72, 319–322. [Google Scholar] [CrossRef] [PubMed]
- Raucci, U.; Musolino, A.M.; Di Lallo, D.; Piga, S.; Barbieri, M.A.; Pisani, M.; Rossi, F.P.; Reale, A.; Ciofi Degli Atti, M.L.; Villani, A.; et al. Impact of the COVID-19 pandemic on the Emergency Department of a tertiary children’s hospital. Ital. J. Pediatr. 2021, 47, 21. [Google Scholar] [CrossRef]
- Ferro, V.; Boccuzzi, E.; Battaglia, M.; Rossi, F.P.; Olita, C.; Giglioni, E.; Concato, C.; Piccioni, L.; Perrotta, D.; Reale, A.; et al. The Role of Viral Coinfection in Bronchiolitis Treated with High-Flow Nasal Cannula at Pediatric Emergency Department during 2 Consecutive Seasons: An Observational Study. Pediatr. Infect. Dis. J. 2020, 39, 102–107. [Google Scholar] [CrossRef]
- Van Brusselen, D.; De Troeyer, K.; Ter Haar, E.; Vander Auwera, A.; Poschet, K.; Van Nuijs, S.; Bael, A.; Stobbelaar, K.; Verhulst, S.; Van Herendael, B.; et al. Bronchiolitis in COVID-19 times: A nearly absent disease? Eur. J. Pediatr. 2021, 30, 1969–1973. [Google Scholar] [CrossRef]
- Ferrero, F.; Ossorio, M.F. Is there a place for bronchiolitis in the COVID-19 era? Lack of hospitalizations due to common respiratory viruses during the 2020 winter. Pediatr. Pulmonol. 2021, 56, 2372–2373. [Google Scholar] [CrossRef]
- Wilder, J.L.; Parsons, C.R.; Growdon, A.S.; Toomey, S.L.; Mansbach, J.M. Pediatric Hospitalizations During the COVID-19 Pandemic. Pediatrics 2020, 146, e2020005983. [Google Scholar] [CrossRef]
- Rambaud, J.; Dauger, S.; Morin, L.; Bergounioux, J.; Leger, P.L.; Carbajal, R.; Renolleau, S.; Guedj, R. Bronchiolitis Admissions to Intensive Care During COVID. Pediatrics 2021, 147, e2021050103. [Google Scholar] [CrossRef]
- Friedrich, F.; Ongaratto, R.; Scotta, M.C.; Veras, T.N.; Stein, R.T.; Lumertz, M.S.; Jones, M.H.; Comaru, T.; Pinto, L.A. Early Impact of social distancing in response to COVID-19 on hospitalizations for acute bronchiolitis in infants in Brazil. Clin. Infect. Dis. 2021, 72, 2071–2075. [Google Scholar] [CrossRef]
- Groves, H.E.; Piché-Renaud, P.P.; Peci, A.; Farrar, D.S.; Buckrell, S.; Bancej, C.; Sevenhuysen, C.; Campigotto, A.; Gubbay, J.B.; Morris, S.K. The impact of the COVID-19 pandemic on influenza, respiratory syncytial virus, and other seasonal respiratory virus circulation in Canada: A population-based study. Lancet Reg. Health Am. 2021, 1, 100015. [Google Scholar] [PubMed]
- Paroni, L.; D’Apice, C.; Ussai, S.; Armocida, B.; Formenti, B.; Min, L.; Missoni, E. The Traffic Light Approach: Indicators and Algorithms to Identify Covid-19 Epidemic Risk Across Italian Regions. Front. Public Health 2021, 9, 650243. [Google Scholar] [CrossRef] [PubMed]
- Rotulo, G.A.; Percivale, B.; Molteni, M.; Naim, A.; Brisca, G.; Piccotti, E.; Castagnola, E. The impact of COVID-19 lockdown on infectious diseases epidemiology: The experience of a tertiary Italian Pediatric Emergency Department. Am. J. Emerg. Med. 2021, 43, 115–117. [Google Scholar] [CrossRef] [PubMed]
- Stera, G.; Pierantoni, L.; Masetti, R.; Leardini, D.; Biagi, C.; Buonsenso, D.; Pession, A.; Lanari, M. Impact of SARS-CoV-2 Pandemic on Bronchiolitis Hospitalizations: The Experience of an Italian Tertiary Center. Children 2021, 8, 556. [Google Scholar] [CrossRef]
- Curatola, A.; Lazzareschi, I.; Bersani, G.; Covino, M.; Gatto, A.; Chiaretti, A. Impact of COVID-19 outbreak in acute bronchiolitis: Lesson from a tertiary Italian Emergency Department. Pediatr. Pulmonol. 2021, 56, 2484–2488. [Google Scholar] [CrossRef]
- Vittucci, A.C.; Piccioni, L.; Coltella, L.; Ciarlitto, C.; Antilici, L.; Bozzola, E.; Midulla, F.; Palma, P.; Perno, C.F.; Villani, A. The Disappearance of Respiratory Viruses in Children during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health. 2021, 18, 9550. [Google Scholar] [CrossRef]
- Ujiie, M.; Tsuzuki, S.; Nakamoto, T.; Iwamoto, N. Resurgence of Respiratory Syncytial Virus Infections during COVID-19 Pandemic, Tokyo, Japan. Emerg. Infect. Dis. 2021, 27, 2969–2970. [Google Scholar] [CrossRef]
- Lambert, L.; Sagfors, A.M.; Openshaw, P.J.; Culley, F.J. Immunity to RSV in Early-Life. Front. Immunol. 2014, 5, 466. [Google Scholar] [CrossRef]
- Foley, D.A.; Yeoh, D.K.; Minney-Smith, C.A.; Martin, A.C.; Mace, A.O.; Sikazwe, C.T.; Le, H.; Levy, A.; Moore, H.C.; Blyth, C.C. The Interseasonal Resurgence of Respiratory Syncytial Virus in Australian Children Following the Reduction of Coronavirus Disease 2019-Related Public Health Measures. Clin. Infect. Dis. 2021, 73, e2829–e2830. [Google Scholar] [CrossRef]
- Hussain, F.; Kotecha, S.; Edwards, M.O. RSV bronchiolitis season 2021 has arrived, so be prepared! Arch. Dis. Child. 2021, 106, e51. [Google Scholar] [CrossRef]
- Milani, G.P.; Bollati, V.; Ruggiero, L.; Bosis, S.; Pinzani, R.M.; Lunghi, G.; Rota, F.; Dioni, L.; Luganini, A.; Agostoni, C.; et al. Bronchiolitis and SARS-CoV-2. Arch. Dis. Child. 2021, 106, 999–1001. [Google Scholar] [CrossRef] [PubMed]
- Heinonen, S.; Helve, O.; Andersson, S.; Janér, C.; Süvari, L.; Kaskinen, A. Nasal expression of SARS-CoV-2 entry receptors in newborns. Arch. Dis. Child. Fetal Neonatal Ed. 2021, 107, 95–97. [Google Scholar] [CrossRef]
- De Rose, D.U.; Piersigilli, F.; Ronchetti, M.P.; Santisi, A.; Bersani, I.; Dotta, A.; Danhaive, O.; Auriti, C.; Study Group of Neonatal Infectious Diseases of the Italian Society of Neonatology (SIN). Novel Coronavirus disease (COVID-19) in newborns and infants: What we know so far. Ital. J. Pediatr. 2020, 46, 56. [Google Scholar] [CrossRef] [PubMed]
- Bollani, L.; Baraldi, E.; Chirico, G.; Dotta, A.; Lanari, M.; Del Vecchio, A.; Manzoni, P.; Boldrini, A.; Paolillo, P.; Di Fabio, S.; et al. Revised recommendations concerning palivizumab prophylaxis for respiratory syncytial virus (RSV). Ital. J. Pediatr. 2015, 41, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Camporesi, A.; Morello, R.; Ferro, V.; Pierantoni, L.; Rocca, A.; Lanari, M.; Trobia, G.L.; Sciacca, T.; Bellinvia, A.G.; De Ferrari, A.; et al. Epidemiology, Microbiology and Severity of Bronchiolitis in the First Post-Lockdown Cold Season in Three Different Geographical Areas in Italy: A prospective, observational study. Children 2022, 9, 491. [Google Scholar] [CrossRef] [PubMed]
- Piret, J.; Boivin, G. Viral Interference between Respiratory Viruses. Emerg. Infect. Dis. 2022, 28, 273–281. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
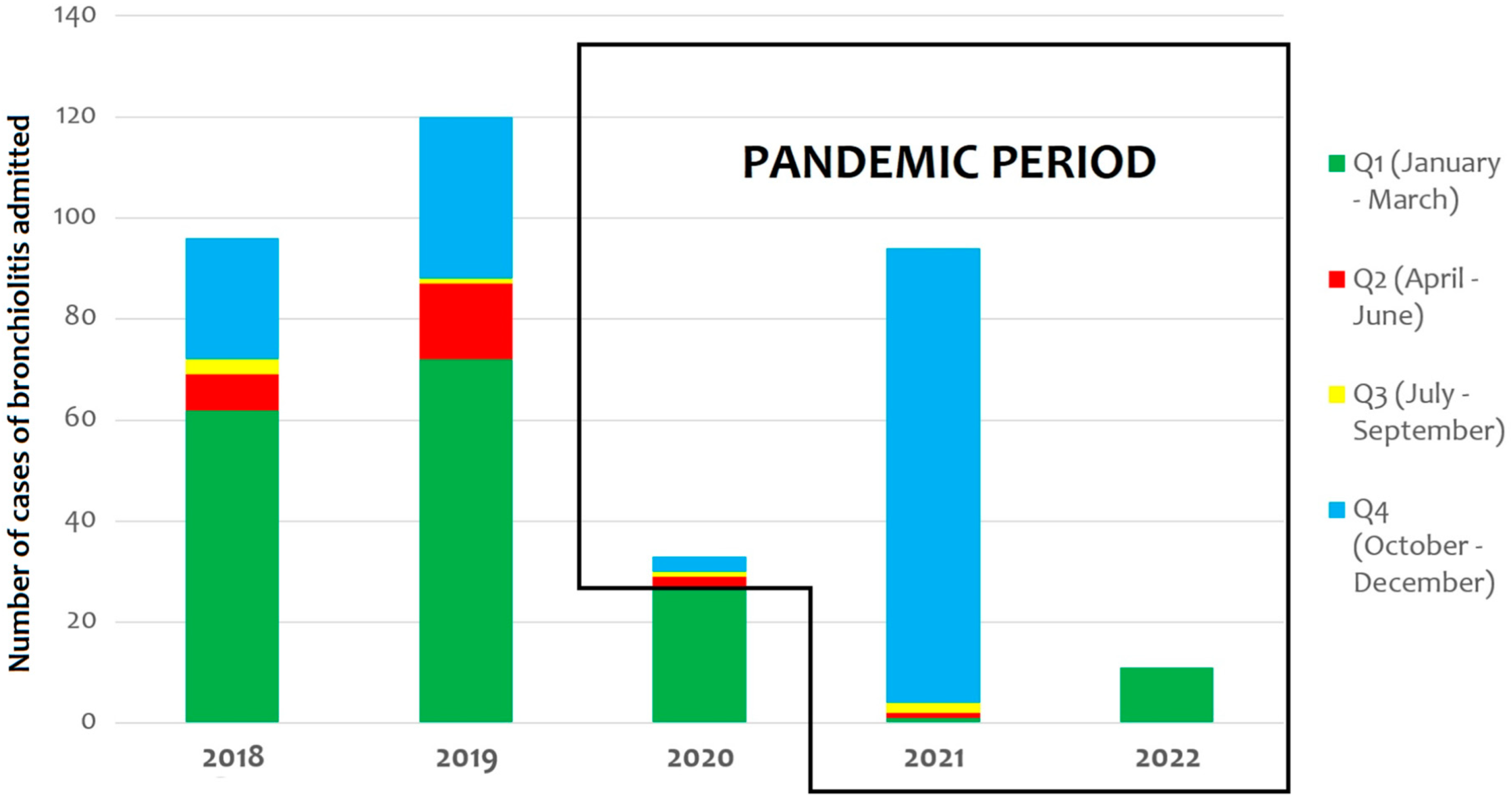
| 2018 | 2019 | 2020 | 2021 | 2022 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| RSV | 51 | RSV | 63 | RSV | 24 | RSV | 1 | RSV | 6 | |
| Rhinovirus | 5 | Rhinovirus | 6 | Rhinovirus | 1 | Rhinovirus | 2 | |||
| Influenza | 1 | Influenza | 1 | Coronavirus * | 2 | SARS-CoV-2 | 2 | |||
| Bocavirus | 1 | Bordetella pert. | 1 | Metapneumov. | 1 | |||||
| Not identified | 4 | Not identified | 1 | |||||||
| Q1 | Total | 62 | Total | 72 | Total | 27 | Total | 1 | Total | 11 |
| RSV | 2 | RSV | 2 | RSV | 1 | Rhinovirus | 1 | |||
| Rhinovirus | 3 | Rhinovirus | 8 | Not identified | 1 | |||||
| Parainfluenza | 1 | Parainfluenza | 2 | |||||||
| Adenovirus | 1 | Adenovirus | 1 | |||||||
| Not identified | 2 | |||||||||
| Q2 | Total | 7 | Total | 15 | Total | 2 | Total | 1 | ||
| Rhinovirus | 2 | Coronavirus ** | 1 | Rhinovirus | 1 | Rhinovirus | 2 | |||
| Not identified | 1 | |||||||||
| Q3 | Total | 3 | Total | 1 | Total | 1 | Total | 2 | ||
| RSV | 13 | RSV | 15 | Rhinovirus | 3 | RSV | 74 | |||
| Rhinovirus | 7 | Rhinovirus | 12 | Rhinovirus | 7 | |||||
| Parainfluenza | 2 | Parainfluenza | 2 | Parainfluenza | 3 | |||||
| Coronavirus *** | 1 | Adenovirus | 1 | Bocavirus | 1 | |||||
| Not identified | 1 | Not identified | 2 | Metapneumov. | 5 | |||||
| Q4 | Total | 24 | Total | 32 | Total | 3 | Total | 90 | ||
| Total | 96 | 120 | 33 | 94 | 11 | |||||
| Period | Date | Measure |
|---|---|---|
| Pre-pandemic period | Before February 2020 | No restrictive measures for Italian citizens |
| 22 February 2020 | Quarantine from 11 municipalities in Northern Italy (the “Red Zones”) | |
| 8 March 2020 | Expansion of the quarantine to all of Lombardy and 14 northern provinces | |
| 9 March 2020 | Order of national lockdown in the whole country | |
| Pandemic period | 3 June 2020 | End of national lockdown |
| 7 October 2020 | New imposition of the use of protective masks outdoors | |
| 25 October 2020 | New restrictions with a “traffic light” color code (red, orange, and yellow zones), imposing the online schooling for 75% of secondary schools and university students, the closing of gyms, swimming pools, theaters, and cinemas, as well as the closing of bars and restaurants before 6 p.m. based on the number of infections | |
| 28 June 2021 | Slowdown of restrictive measures, with the introduction of the “Green Pass” for vaccinated or recovered subjects or those with a proof of a negative test taken within the last 48 h; no requirement to wear masks outdoors | |
| 1 September 2021 | Full reopening of secondary schools and universities for in-person teaching | |
| 8 October 2021 | Full reopening of theaters, cinemas, and concert halls | |
| 6 December 2021 | Introduction of a two-tiered Green Pass system, named the “Super Green Pass” to access events, venues, and services and to travel on all local and long-distance public transport | |
| 7 January 2022 | Introduction of the vaccination obligation for people aged 50 or over, with a penalty for non-compliant persons |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Rose, D.U.; Caoci, S.; Auriti, C.; Maddaloni, C.; Capolupo, I.; Salvatori, G.; Brusco, C.; Coltella, L.; Concato, C.; Russo, C.; et al. Lessons from SARS-CoV-2 Pandemics: How Restrictive Measures Impacted the Trend of Respiratory Infections in Neonates and Infants up to Three Months of Age. Pathogens 2022, 11, 1086. https://doi.org/10.3390/pathogens11101086
De Rose DU, Caoci S, Auriti C, Maddaloni C, Capolupo I, Salvatori G, Brusco C, Coltella L, Concato C, Russo C, et al. Lessons from SARS-CoV-2 Pandemics: How Restrictive Measures Impacted the Trend of Respiratory Infections in Neonates and Infants up to Three Months of Age. Pathogens. 2022; 11(10):1086. https://doi.org/10.3390/pathogens11101086
Chicago/Turabian StyleDe Rose, Domenico Umberto, Stefano Caoci, Cinzia Auriti, Chiara Maddaloni, Irma Capolupo, Guglielmo Salvatori, Carla Brusco, Luana Coltella, Carlo Concato, Cristina Russo, and et al. 2022. "Lessons from SARS-CoV-2 Pandemics: How Restrictive Measures Impacted the Trend of Respiratory Infections in Neonates and Infants up to Three Months of Age" Pathogens 11, no. 10: 1086. https://doi.org/10.3390/pathogens11101086