
Detection of Anti-Echinococcus granulosus Antibodies in Humans: An Update from Pakistan

 , , and
, , and 
Abstract
:1. Introduction
2. Results
3. Discussion
4. Material and Methods
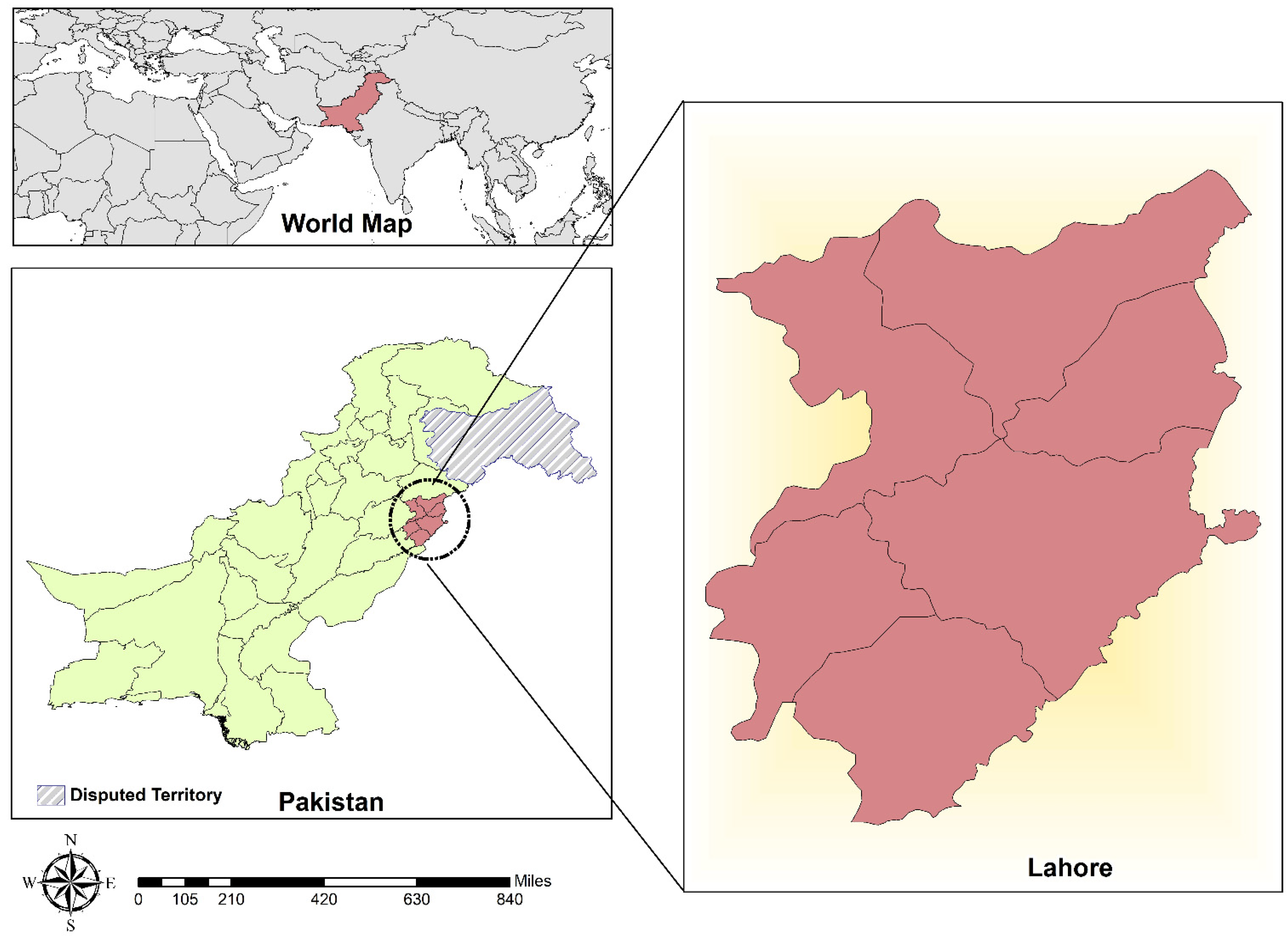
4.1. Study Area
4.2. Methods
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Borhani, M.; Fathi, S.; Darabi, E.; Jalousian, F.; Simsek, S.; Ahmed, H.; Kesik, H.K.; Hosseini, S.H.; Romig, T.; Harandi, M.F. Echinococcoses in Iran, Turkey, and Pakistan: Old Diseases in the New Millennium. Clin. Microbiol. Rev. 2021, 34, e00290-20. [Google Scholar] [CrossRef]
- Thompson, R. Biology and systematics of Echinococcus. Adv. Parasitol. 2017, 95, 65–109. [Google Scholar]
- Craig, P.; Mastin, A.; van Kesteren, F.; Boufana, B. Echinococcus granulosus: Epidemiology and state-of-the-art of diagnostics in animals. Vet. Parasitol. 2015, 213, 132–148. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Zhang, Z.; Wu, W.; Shi, B.; Li, J.; Zhou, X.; Wen, H.; McManus, D.P. Epidemiology and control of echinococcosis in central Asia, with particular reference to the People’s Republic of China. Acta Trop. 2015, 141, 235–243. [Google Scholar] [CrossRef] [PubMed]
- McManus, D.; Smyth, J. Hydatidosis: Changing concepts in epidemiology and speciation. Parasitol. Today 1986, 2, 163–168. [Google Scholar] [CrossRef]
- Grubor, N.M.; Jovanova-Nesic, K.D.; Shoenfeld, Y. Liver cystic echinococcosis and human host immune and autoimmune follow-up: A review. World J. Hepatol. 2017, 9, 1176. [Google Scholar] [CrossRef] [PubMed]
- Anvari, D.; Rezaei, F.; Ashouri, A.; Rezaei, S.; Majidiani, H.; Pagheh, A.S.; Rezaei, F.; Shariatzadeh, S.A.; Fotovati, A.; Siyadatpanah, A. Current situation and future prospects of Echinococcus granulosus vaccine candidates: A systematic review. Transbound. Emerg. Dis. 2021, 68, 1080–1096. [Google Scholar] [CrossRef]
- Andrabi, A.; Tak, H.; Lone, B.A.; Para, B.A. Seroprevalence of human cystic echinococcosis in South Kashmir, India. Parasite Epidemiol. Control 2020, 11, e00172. [Google Scholar] [CrossRef] [PubMed]
- Bitrus, D.; Weka, R.P.; Yakubu, R.A.; Ogo, I.N.; Ikeh, E.I. Echinococcus granulosus Antibodies in Dogs and Breeder practices promoting spread of infection in Plateau State, Nigeria. Ann. Med. Lab. Sci. 2021, 1, 9–17. [Google Scholar]
- Alvi, M.A.; Ohiolei, J.A.; Li, L.; Saqib, M.; Hussain, M.H.; Tayyab, M.H.; Ghafoor, M.; Qamar, W.; Faridi, N.Y.; Alvi, A.A. In-House Developed ELISA Indicates High Prevalence of Anti-Echinococcus granulosus IgG in Sheep Population—An Update from Pakistan. Pathogens 2020, 9, 905. [Google Scholar] [CrossRef]
- Tamarozzi, F.; Sako, Y.; Ito, A.; Piccoli, L.; Grisolia, A.; Itoh, S.; Gatti, S.; Meroni, V.; Genco, F.; Brunetti, E. Recombinant AgB8/1 ELISA test vs. commercially available IgG ELISA test in the diagnosis of cystic echinococcosis. Parasite Immunol. 2013, 35, 433–440. [Google Scholar] [CrossRef]
- Harandi, M.; Moazezi, S.; Saba, M.; Grimm, F.; Kamyabi, H.; Sheikhzadeh, F.; Sharifi, I.; Deplazes, P. Sonographical and serological survey of human cystic echinococcosis and analysis of risk factors associated with seroconversion in rural communities of Kerman, Iran. Zoonoses Public Health 2011, 58, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Lembo, T.; Craig, P.S.; Miles, M.A.; Hampson, K.R.; Meslin, F.-X. 1 2 Zoonoses Prevention, Control, and Elimination in Dogs. In Dogs, Zoonoses and Public Health; CABI: Oxford, UK, 2013; pp. 205–258. [Google Scholar]
- McManus, D.P.; Gray, D.J.; Zhang, W.; Yang, Y. Diagnosis, treatment, and management of echinococcosis. BMJ 2012, 344, e3866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Himsawi, N.; Hijjawi, N.; Al-Radaideh, A.; Al-Tamimi, M. Seroprevalence of cystic echinococcosis in a high-risk area (Al-Mafraq Governorate) in Jordan, using indirect hemagglutination test. Parasite Epidemiol. Control 2019, 5, e00104. [Google Scholar] [CrossRef] [PubMed]
- Shafiei, R.; Teshnizi, S.H.; Kalantar, K.; Gholami, M.; Mirzaee, G.; Mirzaee, F. The seroprevalence of human cystic echinococcosis in Iran: A systematic review and meta-analysis study. J. Parasitol. Res. 2016, 2016, 1425147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, A.; Ahmed, H.; Budke, C.M. Echinococcosis in Pakistan: A call for research. Lancet Infect. Dis. 2019, 19, 581. [Google Scholar] [CrossRef] [Green Version]
- Khan, A.; Ahmed, H.; Khan, H.; Saleem, S.; Simsek, S.; Brunetti, E.; Afzal, M.S.; Manciulli, T.; Budke, C.M. Cystic echinococcosis in Pakistan: A review of reported cases, diagnosis, and management. Acta Trop. 2020, 212, 105709. [Google Scholar] [CrossRef]
- Khan, A.; Ahmed, H.; Amjad, S.; Afzal, M.S.; Haider, W.; Simsek, S.; Khawaja, M.R.; Khan, D.H.; Naz, S.; Durrance-Bagale, A. Community Based Assessment of Behavior and Awareness of Risk Factors of Cystic Echinococcosis in Major Cities of Pakistan: A One Health Perspective. Front. Public Health 2021, 9, 648900. [Google Scholar] [CrossRef] [PubMed]
- Moro, P.; Schantz, P.M. Echinococcosis: A review. Int. J. Infect. Dis. 2009, 13, 125–133. [Google Scholar] [CrossRef] [Green Version]
- Karthik, L.; Kumar, G.; Keswani, T.; Bhattacharyya, A.; Chandar, S.S.; Bhaskara Rao, K. Protease inhibitors from marine actinobacteria as a potential source for antimalarial compound. PLoS ONE 2014, 9, e90972. [Google Scholar] [CrossRef] [Green Version]
- Basinger, S.C.; Khan, A.; Ahmed, H.; Afzal, M.S.; Simsek, S.; Budke, C.M. Estimation of the monetary burden of treated human cystic echinococcosis in Pakistan. Acta Trop. 2021, 222, 106026. [Google Scholar] [CrossRef] [PubMed]
- Torgerson, P.R.; Devleesschauwer, B.; Praet, N.; Speybroeck, N.; Willingham, A.L.; Kasuga, F.; Rokni, M.B.; Zhou, X.N.; Fèvre, E.M.; Sripa, B.; et al. World Health Organization estimates of the global and regional disease burden of 11 foodborne parasitic diseases, 2010: A data synthesis. PLoS Med. 2015, 12, e1001920. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, H.; Ali, S.; Afzal, M.S.; Khan, A.A.; Raza, H.; Shah, Z.H.; Simsek, S. Why more research needs to be done on echinococcosis in Pakistan. Infect. Dis. Poverty 2017, 6, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Ahmed, H.; Naz, K.; Gul, S.; Ishaque, S.M.; Zaidi, S.S.A.; Afzal, M.S.; Ali, M.S.; Bokari, S.A.; Budke, C.M. Surgically confirmed cases of cystic echinococcosis from Baluchistan Province, Pakistan for the years 2011–2018. Acta Trop. 2020, 205, 105354. [Google Scholar] [CrossRef]
- Muqaddas, H.; Arshad, M.; Ahmed, H.; Mehmood, N.; Khan, A.; Simsek, S. Retrospective study of cystic echinococcosis (ce) based on hospital record from five major metropolitan cities of Pakistan. Acta Parasitol. 2019, 64, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Rasib, Q.; Khan, A.; Ahmed, H.; Nizamuddin, S.; Asif, F.; Afzal, M.; Simsek, S.; Khurshid, F.; Irum, S.; Hussain, N. Demographics of cystic echinococcosis patients treated surgically in Lahore, Pakistan: A single centre study from 2007–2018. Helminthologia 2021, 58, 162–172. [Google Scholar] [CrossRef]
- Khan, A.; Zahoor, S.; Ahmed, H.; Malik, U.; Butt, R.A.; Muzam, M.S.; Kilinc, S.G.; Noor, N.; Zahoor, S.; Afzal, M.S. A retrospective analysis on the cystic echinococcosis cases occured in Northeastern Punjab Province, Pakistan. Korean J. Parasitol. 2018, 56, 385. [Google Scholar] [CrossRef]
- Borhani, M.; Fathi, S.; Lahmar, S.; Ahmed, H.; Abdulhameed, M.F.; Harandi, M.F. Cystic echinococcosis in the Eastern Mediterranean region: Neglected and prevailing! PLoS Negl. Trop. Dis. 2020, 14, e0008114. [Google Scholar] [CrossRef]
- Ortona, E.; Riganò, R.; Margutti, P.; Notargiacomo, S.; Ioppolo, S.; Vaccari, S.; Barca, S.; Buttari, B.; Profumo, E.; Teggi, A. Native and recombinant antigens in the immunodiagnosis of human cystic echinococcosis. Parasite Immunol. 2000, 22, 553–559. [Google Scholar] [CrossRef]
- Nasrieh, M.A.; Abdel-Hafez, S.K. Echinococcus granulosus in Jordan: Assessment of various antigenic preparations for use in the serodiagnosis of surgically confirmed cases using enzyme immuno assays and the indirect haemagglutination test. Diagn. Microbiol. Infect. Dis. 2004, 48, 117–123. [Google Scholar] [CrossRef]
- van Doorn, H.R.; Hofwegen, H.; Koelewijn, R.; Gilis, H.; Wentink-Bonnema, E.; Pinelli, E.; van Genderen, P.J.; Schipper, H.G.; van Gool, T. Reliable serodiagnosis of imported cystic echinococcosis with a commercial indirect hemagglutination assay. Diagn. Microbiol. Infect. Dis. 2007, 57, 409–412. [Google Scholar] [CrossRef]
- Moosa, R.A.; Abdel-Hafez, S.K. Serodiagnosis and seroepidemiology of human unilocular hydatidosis in Jordan. Parasitol. Res. 1994, 80, 664–671. [Google Scholar] [CrossRef]
- Sotiraki, S.; Himonas, C.; Korkoliakou, P. Hydatidosis–echinococcosis in Greece. Acta Trop. 2003, 85, 197–201. [Google Scholar] [CrossRef]
- Akalin, S.; Kutlu, S.S.; Caylak, S.D.; Onal, O.; Kaya, S.; Bozkurt, A.İ. Seroprevalence of human cystic echinococcosis and risk factors in animal breeders in rural communities in Denizli, Turkey. J. Infect. Dev. Ctries. 2014, 8, 1188–1194. [Google Scholar] [CrossRef] [Green Version]
- Vola, A.; Manciulli, T.; De Silvestri, A.; Lissandrin, R.; Mariconti, M.; Siles-Lucas, M.; Brunetti, E.; Tamarozzi, F. Diagnostic performances of commercial ELISA, Indirect Hemagglutination, and Western Blot in differentiation of hepatic echinococcal and non-echinococcal lesions: A retrospective analysis of data from a single referral centre. Am. J. Trop. Med. Hyg. 2019, 101, 1345. [Google Scholar] [CrossRef] [PubMed]
- Hadipour, M.; Nazari, M.; Sanei, B.; Ghayour, Z.; Sharafi, S.M.; Yazdani, H.; Darani, H.Y. Immunological diagnosis of human hydatid cyst using Western immunoblotting technique. J. Res. Med. Sci. Off. J. Isfahan Univ. Med. Sci. 2016, 21, 130. [Google Scholar]
- Tamarozzi, F.; Covini, I.; Mariconti, M.; Narra, R.; Tinelli, C.; De Silvestri, A.; Manzoni, F.; Casulli, A.; Ito, A.; Neumayr, A. Comparison of the diagnostic accuracy of three rapid tests for the serodiagnosis of hepatic cystic echinococcosis in humans. PLoS Negl. Trop. Dis. 2016, 10, e0004444. [Google Scholar] [CrossRef] [Green Version]
- Baraquin, A.; Zait, H.; Grenouillet, F.-E.; Moreau, E.; Hamrioui, B.; Grenouillet, F. Large-scale evaluation of a rapid diagnostic test for human cystic echinococcosis. Diagn. Microbiol. Infect. Dis. 2017, 89, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.-H.; Wang, J.-Y.; Shi, F.; Steverding, D.; Wang, X.; Yang, Y.-T.; Zhou, X.-N. Field evaluation of an immunochromatographic test for diagnosis of cystic and alveolar echinococcosis. Parasites Vectors 2018, 11, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Zahawi, H.; Hameed, O.; Abalkhail, A. The possible role of the age of the human host in determining the localization of hydatid cysts. Ann. Trop. Med. Parasitol. 1999, 93, 621–627. [Google Scholar] [CrossRef]
- Salama, A.A.; Othman, A.A.; Zayed, H.A. Cystic echinococcosis in the middle region of the Nile Delta, Egypt: Clinical and radiological characteristics. Egypt. J. Radiol. Nucl. Med. 2014, 45, 641–649. [Google Scholar] [CrossRef] [Green Version]
- Rana, I.A.; Routray, J.K.; Younas, Z.I. Spatiotemporal dynamics of development inequalities in Lahore City Region, Pakistan. Cities 2020, 96, 102418. [Google Scholar] [CrossRef]
- Bioactiva Diagnostica. Echinococcus IgG-ELISA. 2011. Available online: https://bioactiva.com/pub/media/sebwite/productdownloads//e/c/echg0130ba_2020-08-09_ka-ab_lot_077.pdf (accessed on 22 December 2021).
- ELI.H.A Range: Indirect Hameagglutination (I.H.A)- Hydatidosis (Echinococcosis). 2019. Available online: https://www.elitechgroup.com/product/eli-h-a-echinococcus (accessed on 22 December 2021).



{kind=link}
{kind=link}
| Variables | Total | IHA | ELISA | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Positive | Negative | Prevalence (%) | Positive | Negative | Elevated | Prevalence (%) | |||
| Gender | M | 41 | 9 | 22 | 21.9 | 1 | 9 | 0 | 2.43 |
| F | 52 | 7 | 25 | 13.5 | 3 | 16 | 1 | 5.76 | |
| Age | ≤3 | 3 | 2 | 1 | 66.6 | 0 | 0 | 0 | 0 |
| 4–23 | 9 | 2 | 4 | 22.2 | 1 | 2 | 0 | 11.11 | |
| 24–43 | 24 | 3 | 7 | 12.5 | 2 | 11 | 1 | 8.33 | |
| 44–63 | 28 | 2 | 19 | 7.18 | 1 | 6 | 0 | 3.57 | |
| >64 | 15 | 1 | 8 | 6.66 | 0 | 6 | 0 | 0 | |
| Not available | 14 | 6 | 8 | 42.8 | 0 | 0 | 0 | 0 | |
| Year | 2018 | 54 | 11 | 14 | 20.3 | 4 | 24 | 1 | 7.40 |
| 2019 | 18 | 4 | 13 | 22.2 | 0 | 1 | 0 | 0 | |
| 2020 | 20 | 1 | 19 | 5.00 | 0 | 0 | 0 | 0 | |
| 2021 | 1 | 1 | 0 | 100 | 0 | 0 | 0 | 0 | |
| Variable | Category | ELISA, n (%) | IHA, n (%) | Chi-Square | p-Value | ||
|---|---|---|---|---|---|---|---|
| Age (y) | ≤3 | 0 (0%) | 0 | 2 (100%) | 100 | 1.58 | 0.811 |
| 4–23 | 1 (33.3%) | 33.3 | 2 (66.7%) | 66.7 | |||
| 24–43 | 2 (40.0%) | 40.0 | 3 (60.0%) | 60.0 | |||
| 44–63 | 1 (33.3%) | 33.3 | 2 (66.7%) | 66.7 | |||
| >64 | 0 (0%) | 0 | 1 (100%) | 100 | |||
| Not available | 0 (0%) | 0 | 6 (100%) | 100 | |||
| Gender | F | 3 (30.0%) | 30.0 | 7 | 70.0 | 1.25 | 0.264 |
| M | 1 (10.0%) | 10.0 | 9 | 90.0 | |||
| Year | 2018 | 4 (26.7%) | 26.7 | 11 (73.3%) | 73.3 | 1.66 | 0.435 |
| 2019 | 0 (0%) | 0 | 4 (100%) | 100 | |||
| 2020 | 0 (0%) | 0 | 1 (100%) | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, H.; Ahmed, H.; Afzal, M.S.; Awan, U.A.; Khurram, M.; Simsek, S.; Cao, J. Detection of Anti-Echinococcus granulosus Antibodies in Humans: An Update from Pakistan. Pathogens 2022, 11, 29. https://doi.org/10.3390/pathogens11010029
Khan H, Ahmed H, Afzal MS, Awan UA, Khurram M, Simsek S, Cao J. Detection of Anti-Echinococcus granulosus Antibodies in Humans: An Update from Pakistan. Pathogens. 2022; 11(1):29. https://doi.org/10.3390/pathogens11010029
Chicago/Turabian StyleKhan, Huma, Haroon Ahmed, Muhammad Sohail Afzal, Usman Ayub Awan, Muhammad Khurram, Sami Simsek, and Jianping Cao. 2022. "Detection of Anti-Echinococcus granulosus Antibodies in Humans: An Update from Pakistan" Pathogens 11, no. 1: 29. https://doi.org/10.3390/pathogens11010029