
Functional Autoreactive Anti-β2 Adrenergic Antibodies May Contribute to Insulin Resistance Profile in Patients with Chronic Chagas Disease

 ,
, 
Abstract
:
1. Introduction
2. Results
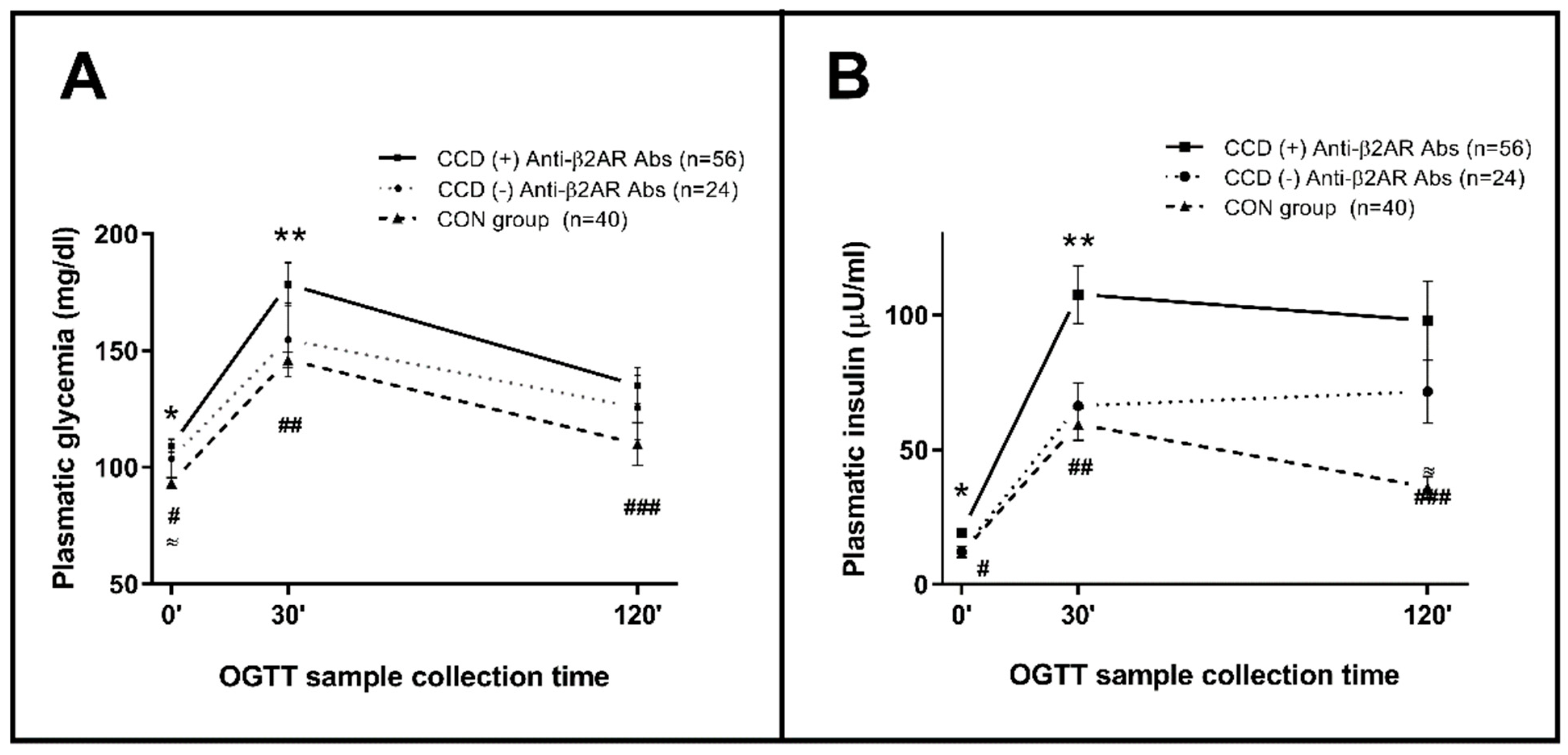
2.1. CCD Association with Increased Prevalence of Dysglycemia and Insulin Resistance
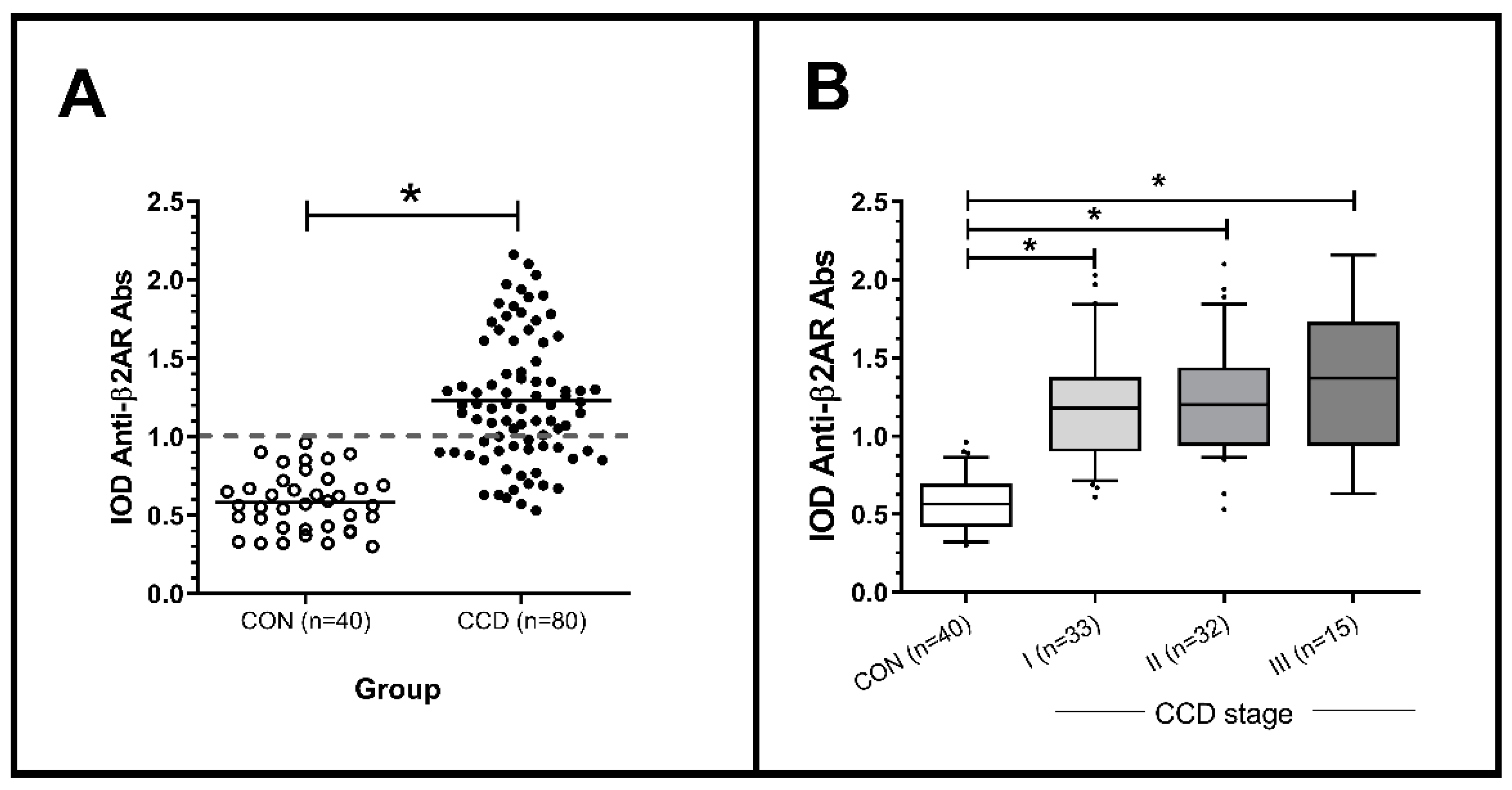
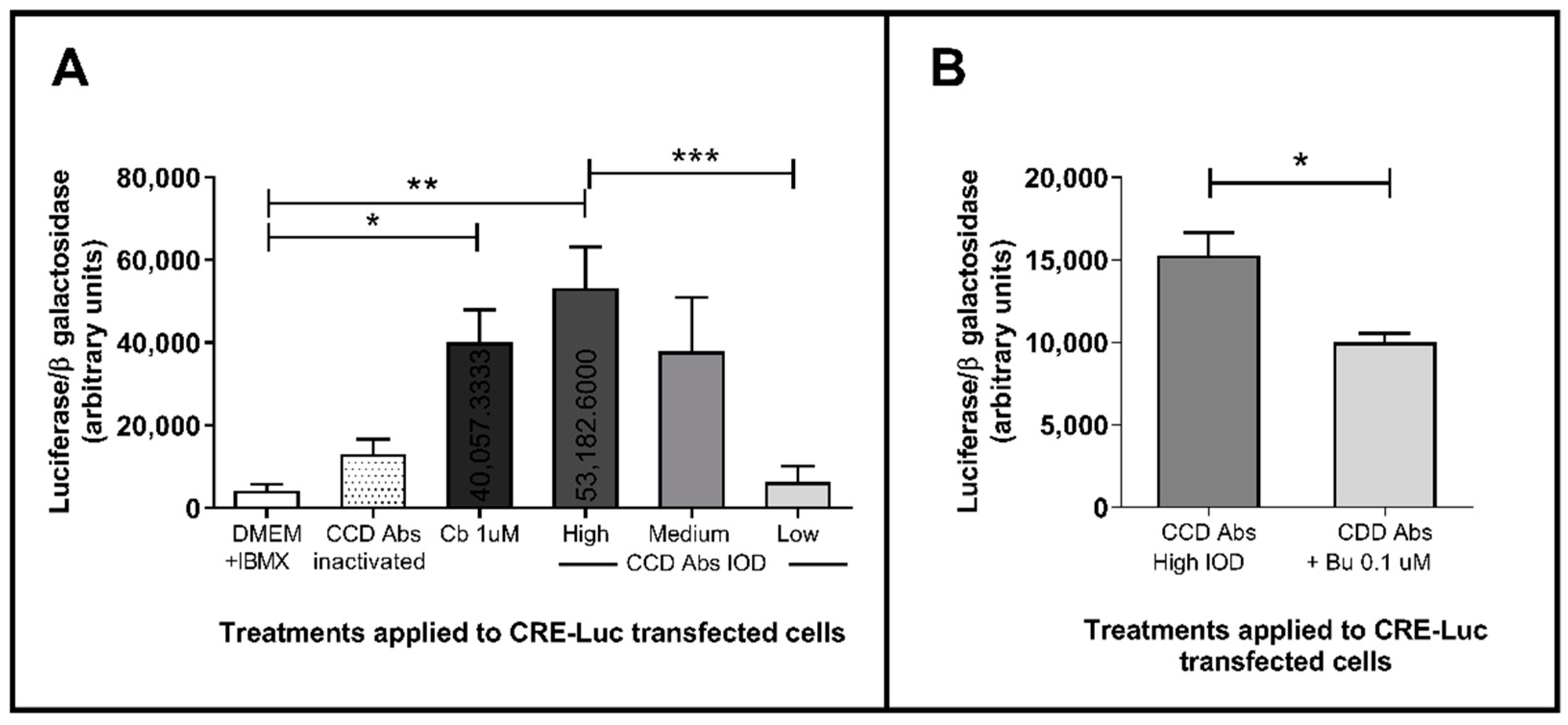
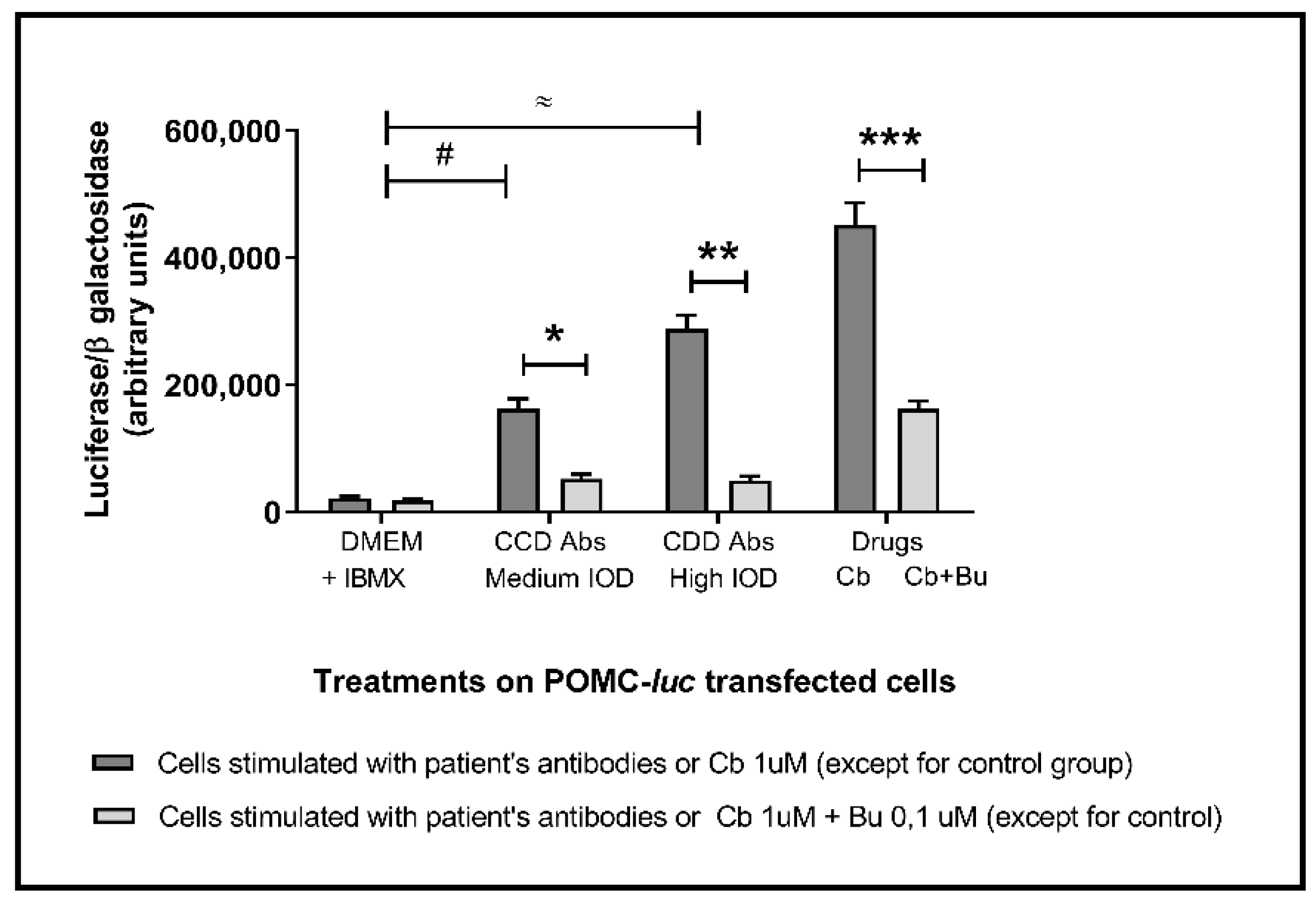
2.2. Anti-β2AR Antibodies Reactivity in Patient Sera and Functional Bioassay
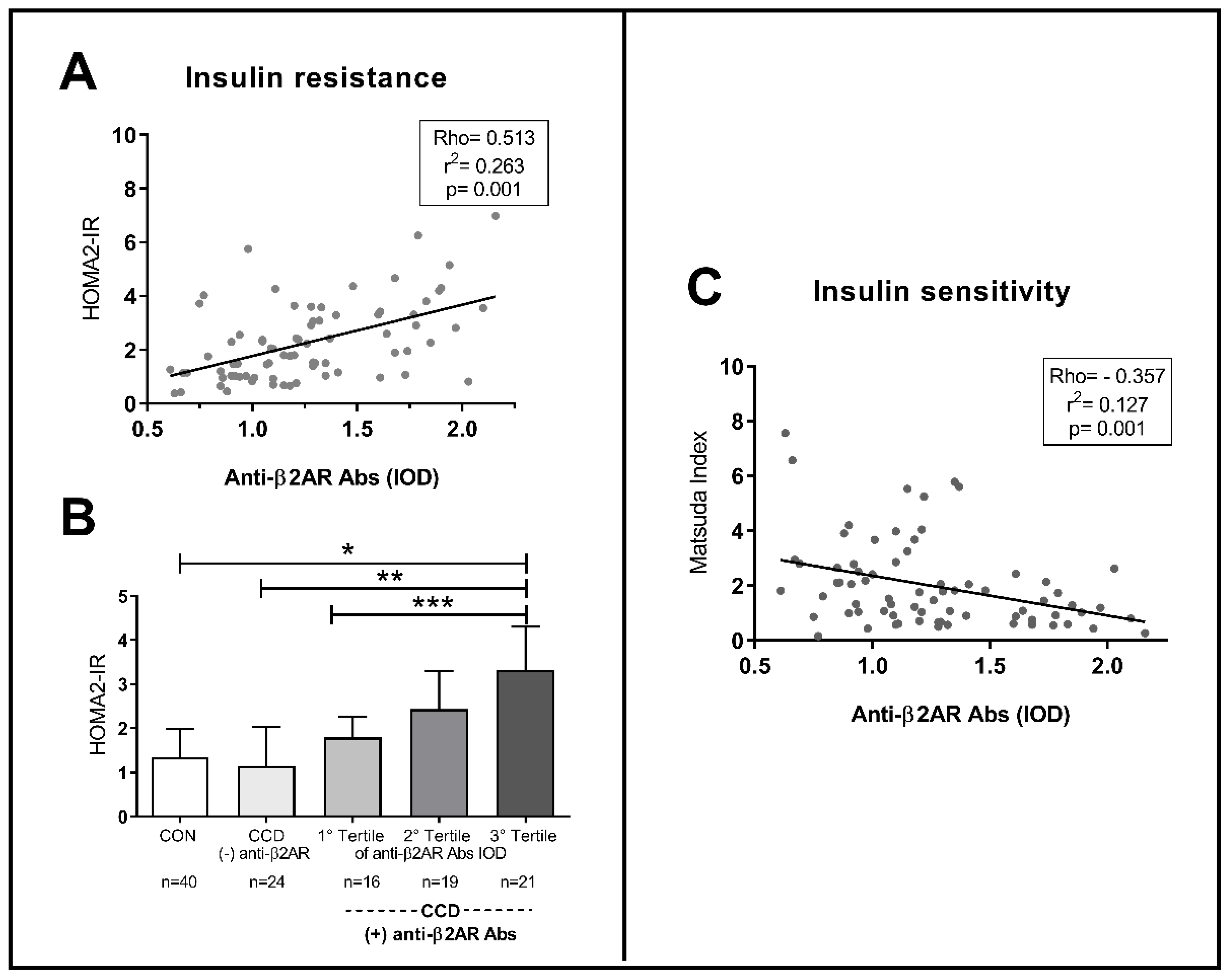
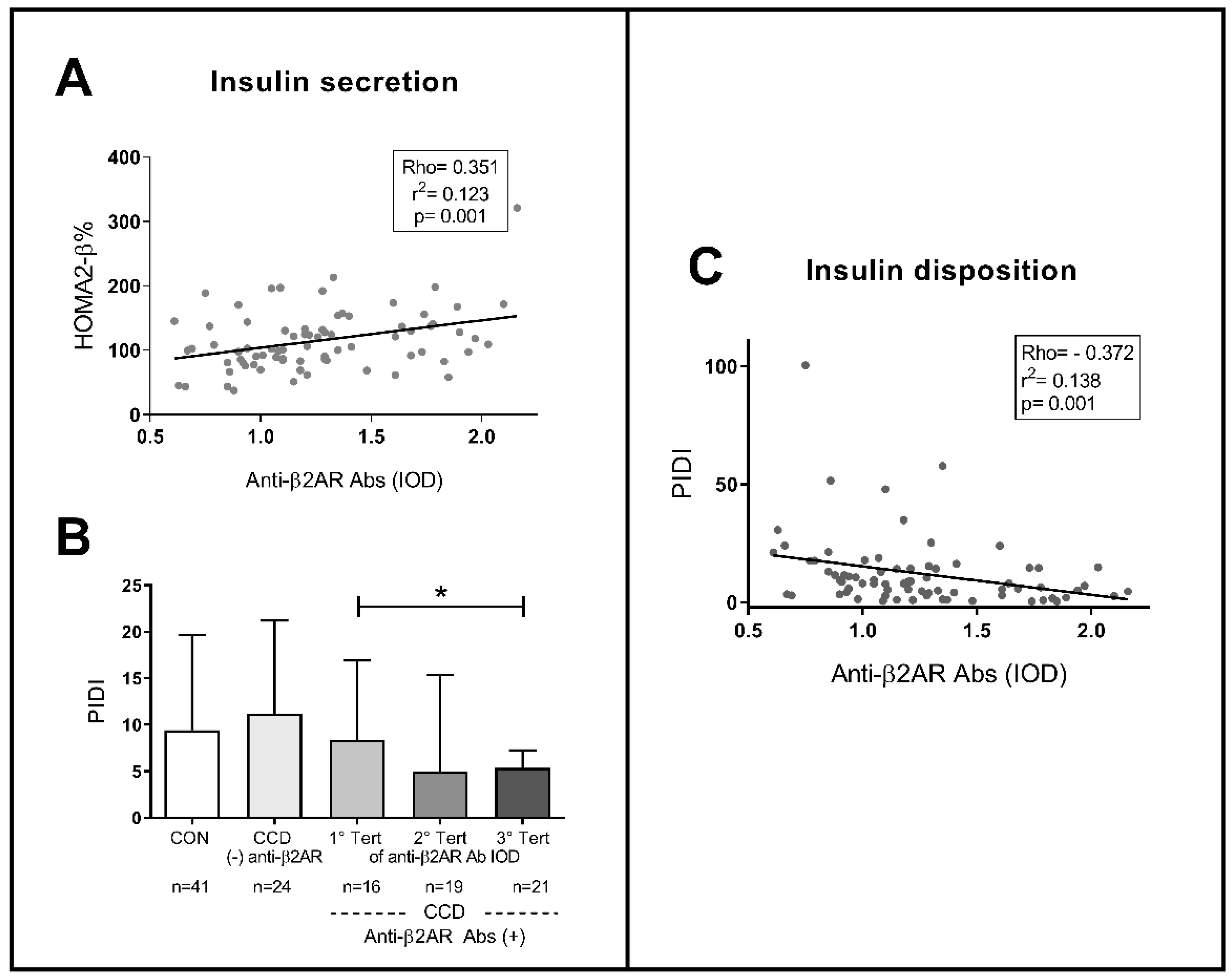
2.3. Anti-B2AR Antibodies in CCD Patients: Correlation with an Insulin Resistance Profile
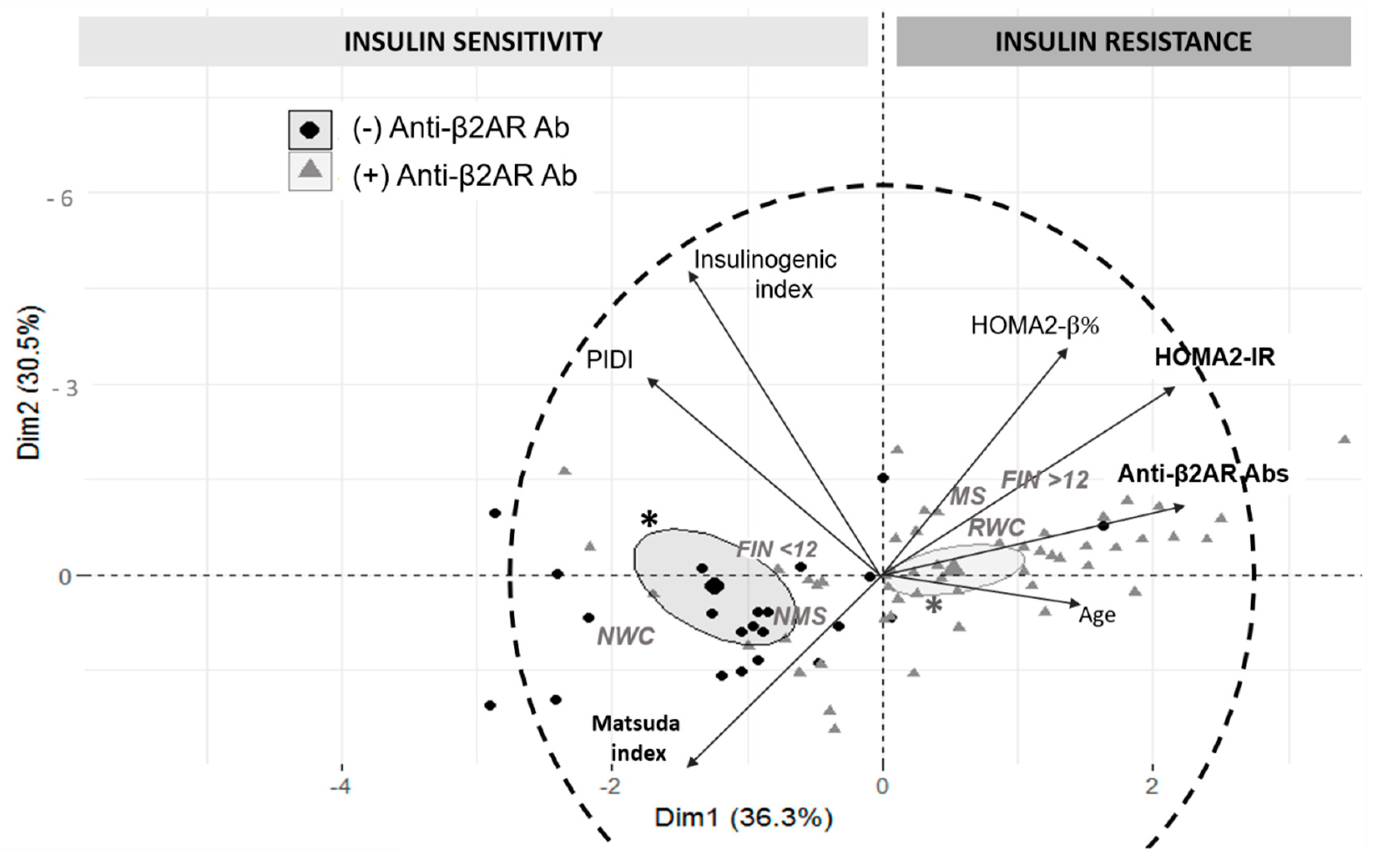
2.3.1. Multivariate Exploration and Logistic Regression Analysis
2.3.2. Logistic Regression Analysis
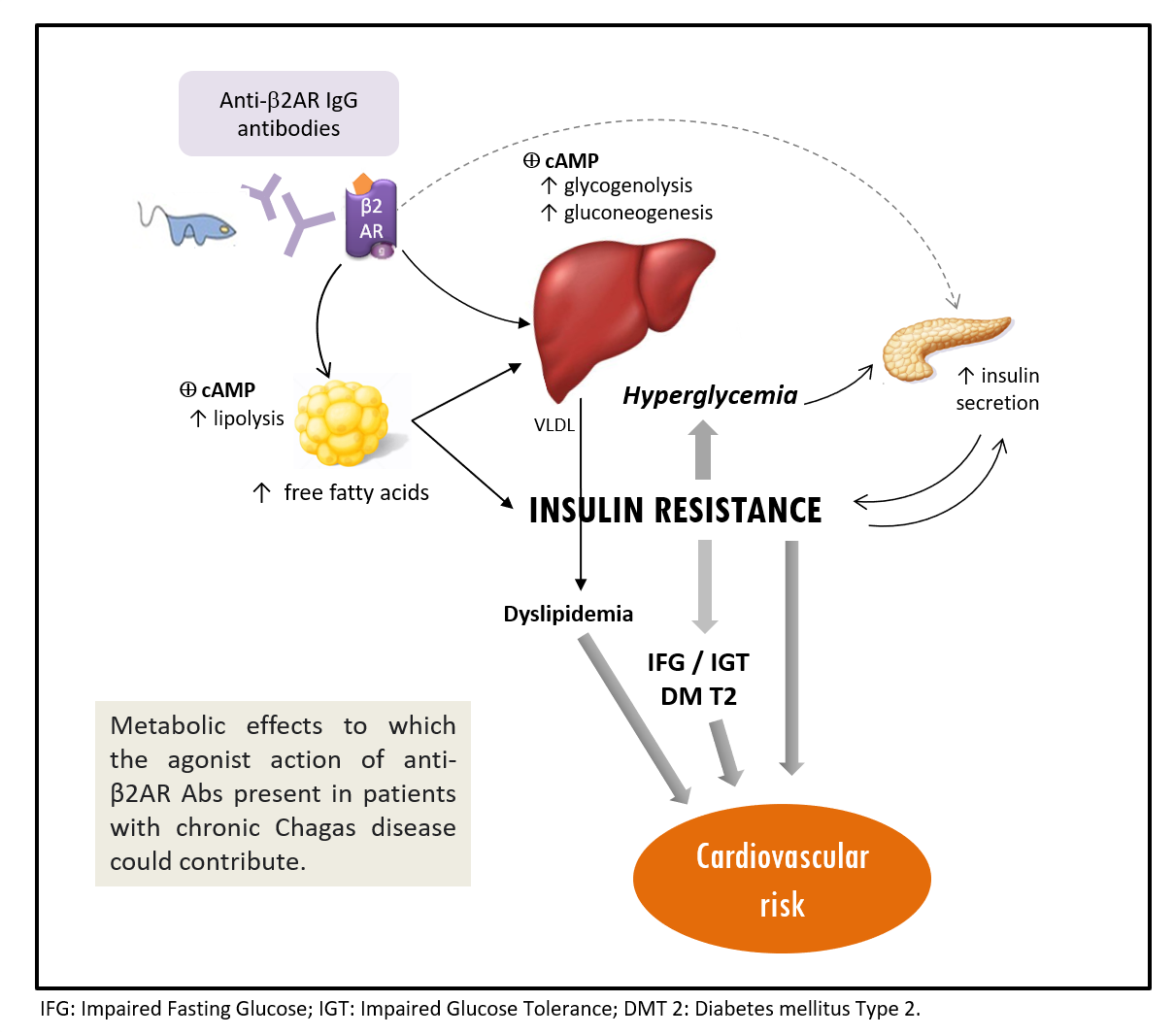
3. Discussion
4. Materials and Methods
4.1. Study Population and Subject Evaluation
- age ≥70 years;
- previously known diabetes mellitus, high hypertriglyceridemia levels (≥300 mg/dL), or other endocrinopathies;
- current treatment with drugs with known effects on carbohydrates metabolism (i.e., corticosteroids, thiazides, atypical antipsychotics, normo/hypoglycemic agents) and/or β adrenergic agonists/antagonists;
- pregnancy or immediate puerperium;
- chronic ethylism or relatively recent (≤2 years) abandonment of the habit.
- acute T. cruzi infection or chronic Chagas disease with advanced cardiac impact (i.e., severe arrhythmias, severe heart failure, evidence of acute decompensation);
- prior or present treatment with anti-T. cruzi compounds or immunosuppressive drugs;
- other relevant systemic complaints (i.e., autoimmune, oncological, or hematological diseases);
- psychiatric diseases or any other condition that might impair the patients’ capacity to give informed consent.
4.2. H26Q Peptide Synthesis and Assessment of Anti-β2AR Antibodies
4.3. Specific Anti-β2AR Antibodies Purification
4.4. Functional Bioassay
4.4.1. Cells and Culture Conditions
4.4.2. Transfections and Reporter Assays
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pan American Health Organization, World Health Organization. Guidelines for the Diagnosis and Treatment of Chagas Disease; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Morrot, A.; Villar, S.R.; González, F.B.; Pérez, A.R. Evasion and Immuno-Endocrine Regulation in Parasite Infection: Two Sides of the Same Coin in Chagas Disease? Front. Microbiol. 2016, 7, 704. [Google Scholar] [CrossRef] [PubMed]
- Rassi, A.; Marin-Neto, J.A. Chagas disease. Lancet 2010, 375, 1388–1402. [Google Scholar] [CrossRef]
- Tarleton, R.L. Parasite persistence in the aetiology of Chagas disease. Int. J. Parasitol. 2001, 31, 550–554. [Google Scholar] [CrossRef]
- Gironès, N.; Cuervo, H.; Fresno, M. Trypanosoma cruzi-Induced Molecular Mimicry and Chagas’ Disease. Curr. Top. Microbiol. Immunol. 2005, 296, 89–123. [Google Scholar] [CrossRef] [PubMed]
- Elies, R.; Ferrari, I.; Wallukat, G.; Lebesgue, D.; Chiale, P.; Elizari, M.; Rosenbaum, M.; Hoebeke, J.; Levin, M.J. Structural and functional analysis of the B cell epitopes recognized by anti-receptor autoantibodies in patients with Chagas’ disease. J. Immunol. 1996, 157, 4203–4211. [Google Scholar]
- Rosenbaum, M.B.; Chiale, P.A.; Schejtman, D.; Levin, M.; Elizari, M.V. Antibodies to Beta-Adrenergic Receptors Disclosing Agonist-Like Properties in Idiopathic Dilated Cardiomyopathy and Chagas’ Heart Disease. J. Cardiovasc. Electrophysiol. 1994, 5, 367–375. [Google Scholar] [CrossRef]
- Sterin-Borda, L.; Perez Leiros, C.; Wald, M.; Cremaschi, G.; Borda, E. Antibodies to β1 and β2 adrenoreceptors in Chagas’ disease. Clin. Exp. Immunol. 1988, 74, 349–354. [Google Scholar]
- Dhiman, M.; Zago, M.P.; Nunez, S.; Amoroso, A.; Rementeria, H.; Dousset, P.; Burgos, F.N.; Garg, N.J. Cardiac-Oxidized Antigens Are Targets of Immune Recognition by Antibodies and Potential Molecular Determinants in Chagas Disease Pathogenesis. PLoS ONE 2012, 7, e28449. [Google Scholar] [CrossRef] [Green Version]
- Gìronés, N.; Rodriguez, C.I.; Carrasco-Marín, E.; Hernáez, R.F.; De Rego, J.L.; Fresno, M. Dominant T- and B-cell epitopes in an autoantigen linked to Chagas’ disease. J. Clin. Investig. 2001, 107, 985–993. [Google Scholar] [CrossRef]
- A Hawkins, G.; Weiss, S.T.; Bleecker, E.R. Clinical consequences ofADRβ2polymorphisms. Pharmacogenomics 2008, 9, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Brunton, L.L.; Hilal-Dandan, R.; Knollmann, B.C. (Eds.) Goodman & Gilman’s the Pharmacological Basis of Therapeutics; McGraw-Hill Education: New York, NY, USA, 2018; p. 7. [Google Scholar]
- Dos Santos, V.M.; Cunha, S.F.D.C.D.; Teixeira, V.D.P.A.; Monteiro, J.P.; Dos Santos, J.A.M.; Dos Santos, T.A.M.; Dos Santos, L.A.M.; Da Cunha, D.F. Freqüência de diabetes mellitus e hiperglicemia em mulheres chagásicas e não-chagásicas. Rev. Soc. Bras. Med. Trop. 1999, 32, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Geraix, J.; Ardisson, L.P.; Marcondes-Machado, J.; Pereira, P.C.M. Clinical and nutritional profile of individuals with chagas disease. Braz. J. Infect. Dis. 2007, 11, 411–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarro, E.C.; Abreu, M.M.D.; Tavares, F.C.; Corrente, J.E.; Arruda, C.M.D.; Pereira, P.C.M. Indeterminate form of Chagas’ disease and metabolic syndrome: A dangerous combination. Am. J. Med. Med. Sci. 2013, 3, 68–73. [Google Scholar]
- Combs, T.P.; Mukherjee, S.; De Almeida, C.J.G.; Jelicks, L.A.; Schubert, W.; Lin, Y.; Jayabalan, D.S.; Zhao, D.; Braunstein, V.L.; Landskroner-Eiger, S.; et al. The Adipocyte as an Important Target Cell for Trypanosoma cruzi Infection. J. Biol. Chem. 2005, 280, 24085–24094. [Google Scholar] [CrossRef] [Green Version]
- Nagajyothi, F.; Desruisseaux, M.S.; Thiruvur, N.; Weiss, L.M.; Braunstein, V.L.; Albanese, C.; Teixeira, M.M.; De Almeida, C.J.; Lisanti, M.P.; Scherer, P.E.; et al. Trypanosoma cruzi Infection of Cultured Adipocytes Results in an Inflammatory Phenotype. Obesity 2008, 16, 1992–1997. [Google Scholar] [CrossRef] [Green Version]
- Blalock, J.E. The syntax of immune-neuroendocrine communication. Immunol. Today 1994, 15, 504–511. [Google Scholar] [CrossRef]
- Savino, W.; Guaraldi, F. Endocrine Immunology of Chagas Disease. Front. Horm. Res. 2017, 48, 160–175. [Google Scholar] [CrossRef]
- Chiale, P.A.; Rosenbaum, M.B.; Elizari, M.V.; Hjalmarson, Å.; Magnusson, Y.; Wallukat, G.; Hoebeke, J. High prevalence of antibodies against beta1- and beta2-adrenoceptors in patients with primary electrical cardiac abnormalities. J. Am. Coll. Cardiol. 1995, 26, 864–869. [Google Scholar] [CrossRef] [Green Version]
- Jahns, R.; Boivin, V.; Krapf, T.; Wallukat, G.; Boege, F.; Lohse, M.J. Modulation of beta1-adrenoceptor activity by domain-specific antibodies and heart failure–associated autoantibodies. J. Am. Coll. Cardiol. 2000, 36, 1280–1287. [Google Scholar] [CrossRef] [Green Version]
- Lebesgue, D.; Wallukat, G.; Mijares, A.; Granier, C.; Argibay, J.; Hoebeke, J. An agonist-like monoclonal antibody against the human β2-adrenoceptor. Eur. J. Pharmacol. 1998, 348, 123–133. [Google Scholar] [CrossRef]
- Tabák, A.G.; Herder, C.; Rathmann, W.; Brunner, E.J.; Kivimäki, M. Prediabetes: A high-risk state for diabetes development. Lancet 2012, 379, 2279–2290. [Google Scholar] [CrossRef] [Green Version]
- Sourij, H.; Saely, C.H.; Schmid, F.; Zweiker, R.; Marte, T.; Wascher, T.C.; Drexel, H. Post-challenge hyperglycaemia is strongly associated with future macrovascular events and total mortality in angiographied coronary patients. Eur. Heart J. 2010, 31, 1583–1590. [Google Scholar] [CrossRef] [Green Version]
- DeFronzo, R.A.; Abdul-Ghani, M. Assessment and Treatment of Cardiovascular Risk in Prediabetes: Impaired Glucose Tolerance and Impaired Fasting Glucose. Am. J. Cardiol. 2011, 108, 3B–24B. [Google Scholar] [CrossRef]
- Lindström, J.; Tuomilehto, J. The Diabetes Risk Score: A practical tool to predict type 2 diabetes risk. Diabetes Care 2003, 26, 725–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Festa, A.; Williams, K.; D’Agostino, R.; Wagenknecht, L.E.; Haffner, S.M. The natural course of β-cell function in nondiabetic and diabetic individuals: The Insulin Resistance Atherosclerosis Study. Diabetes 2006, 55, 1114–1120. [Google Scholar] [CrossRef] [Green Version]
- Ferrannini, E.; Nannipieri, M.; Williams, K.; Gonzales, C.; Haffner, S.M.; Stern, M.P. Mode of Onset of Type 2 Diabetes from Normal or Impaired Glucose Tolerance. Diabetes 2004, 53, 160–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fonseca, V.A. Defining and Characterizing the Progression of Type 2 Diabetes. Diabetes Care 2009, 32, S151–S156. [Google Scholar] [CrossRef] [Green Version]
- Nichols, G.A.; Hillier, T.A.; Brown, J.B. Progression from Newly Acquired Impaired Fasting Glusose to Type 2 Diabetes. Diabetes Care 2007, 30, 228–233. [Google Scholar] [CrossRef] [Green Version]
- Weyer, C.; Bogardus, C.; Mott, D.M.; Pratley, R.E. The natural history of insulin secretory dysfunction and insulin resistance in the pathogenesis of type 2 diabetes mellitus. J. Clin. Investig. 1999, 104, 787–794. [Google Scholar] [CrossRef]
- Nagajyothi, F.; Desruisseaux, M.S.; Weiss, L.M.; Chua, S.; Albanese, C.; Machado, F.S.; Esper, L.; Lisanti, M.P.; Teixeira, M.M.; Scherer, P.E.; et al. Chagas disease, adipose tissue and the metabolic syndrome. Memórias Inst. Oswaldo Cruz 2009, 104, 219–225. [Google Scholar] [CrossRef] [Green Version]
- Nagajyothi, F.; Kuliawat, R.; Kusminski, C.M.; Machado, F.S.; Desruisseaux, M.S.; Zhao, D.; Schwartz, G.J.; Huang, H.; Albanese, C.; Lisanti, M.P.; et al. Alterations in Glucose Homeostasis in a Murine Model of Chagas Disease. Am. J. Pathol. 2013, 182, 886–894. [Google Scholar] [CrossRef]
- Onofrio, L.I.; Arocena, A.R.; Paroli, A.F.; Cabalén, M.E.; Andrada, M.C.; Cano, R.C.; Gea, S. Trypanosoma cruzi Infection Is a Potent Risk Factor for Non-alcoholic Steatohepatitis Enhancing Local and Systemic Inflammation Associated with Strong Oxidative Stress and Metabolic Disorders. PLoS Negl. Trop. Dis. 2015, 9, e0003464. [Google Scholar] [CrossRef] [Green Version]
- Pérez, A.; Silva-Barbosa, S.; Berbert, L.; Revelli, S.; Beloscar, J.; Savino, W.; Bottasso, O. Immunoneuroendocrine alterations in patients with progressive forms of chronic Chagas disease. J. Neuroimmunol. 2011, 235, 84–90. [Google Scholar] [CrossRef]
- Rodeles, L.M.; Castro, M.; Zamora, M.A.G.; Savarino, R.; Peverengo, L.M.; Prochetto, E.S.; Marcipar, I.; Arias, P.; Vicco, M.H. Increased epicardial adipose tissue thickness associated with increased metabolic risk and the presence of heart failure in patients with Chronic Chagas disease. Trans. R. Soc. Trop. Med. Hyg. 2021. [Google Scholar] [CrossRef]
- Utzschneider, K.M.; Prigeon, R.L.; Faulenbach, M.V.; Tong, J.; Carr, D.B.; Boyko, E.J.; Leonetti, D.L.; McNeely, M.J.; Fujimoto, W.Y.; Kahn, S.E. Oral Disposition Index Predicts the Development of Future Diabetes Above and Beyond Fasting and 2-h Glucose Levels. Diabetes Care 2008, 32, 335–341. [Google Scholar] [CrossRef] [Green Version]
- Boyda, H.N.; Procyshyn, R.M.; Pang, C.C.Y.; Barr, A.M. Peripheral Adrenoceptors: The Impetus Behind Glucose Dysregulation and Insulin Resistance. J. Neuroendocr. 2013, 25, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Hagström-Toft, E.; Enoksson, S.; Moberg, E.; Bolinder, J.; Arner, P. β-Adrenergic regulation of lipolysis and blood flow in human skeletal muscle in vivo. Am. J. Physiol. Metab. 1998, 275, E909–E916. [Google Scholar] [CrossRef] [PubMed]
- Langfort, J.; Ploug, T.; Ihlemann, J.; Saldo, M.; Holm, C.; Galbo, H. Expression of hormone-sensitive lipase and its regulation by adrenaline in skeletal muscle. Biochem. J. 1999, 340 Pt 2, 459–465. [Google Scholar] [CrossRef]
- Qvisth, V.; Hagström-Toft, E.; Enoksson, S.; Bolinder, J. Catecholamine Regulation of Local Lactate Production in Vivo in Skeletal Muscle and Adipose Tissue: Role of β-Adrenoreceptor Subtypes. J. Clin. Endocrinol. Metab. 2008, 93, 240–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunton, L.L.; Chabner, B.A.; Knollmann, B.C. Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 12th ed.; McGraw-Hill: New York, NY, USA, 2011. [Google Scholar]
- Isomaa, B.; Almgren, P.; Tuomi, T.; Forsén, B.; Lahti, K.; Nissén, M.; Taskinen, M.-R.; Groop, L. Cardiovascular Morbidity and Mortality Associated With the Metabolic Syndrome. Diabetes Care 2001, 24, 683–689. [Google Scholar] [CrossRef] [Green Version]
- Taskinen, M.-R.; Borén, J. New insights into the pathophysiology of dyslipidemia in type 2 diabetes. Atherosclerosis 2015, 239, 483–495. [Google Scholar] [CrossRef]
- Adiels, M.; Borén, J.; Caslake, M.J.; Stewart, P.; Soro, A.; Westerbacka, J.; Wennberg, B.; Olofsson, S.-O.; Packard, C.; Taskinen, M.-R. Overproduction of VLDL 1 Driven by Hyperglycemia Is a Dominant Feature of Diabetic Dyslipidemia. Arter. Thromb. Vasc. Biol. 2005, 25, 1697–1703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brima, W.; Eden, D.J.; Mehdi, S.F.; Bravo, M.; Wiese, M.M.; Stein, J.; Almonte, V.; Zhao, D.; Kurland, I.; Pessin, J.E.; et al. The brighter (and evolutionarily older) face of the metabolic syndrome: Evidence fromTrypanosoma cruziinfection in CD-1 mice. Diabetes/Metab. Res. Rev. 2015, 31, 346–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Storino, R. La cara oculta de la enfermedad de Chagas. AV Cardiol. 2001, 21, 39–54. [Google Scholar]
- American Diabetes Association. Introduction: Standards of Medical Care in Diabetes. Diabetes Care 2018, 41, S1–S2. [Google Scholar] [CrossRef] [Green Version]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, Without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.C.; Matthews, D.R.; Hermans, M.P. Correct Homeostasis Model Assessment (HOMA) Evaluation Uses the Computer Program. Diabetes Care 1998, 21, 2191–2192. [Google Scholar] [CrossRef]
- University of Oxford. HOMA Calculator ©; Oxford University: Oxford, UK, 2004. [Google Scholar]
- Matsuda, M.; DeFronzo, R.A. Insulin sensitivity indices obtained from oral glucose tolerance testing: Comparison with the euglycemic insulin clamp. Diabetes Care 1999, 22, 1462–1470. [Google Scholar] [CrossRef]
- Brøns, C.; Jensen, C.B.; Storgaard, H.; Hiscock, N.J.; White, A.; Appel, J.S.; Jacobsen, S.; Nilsson, E.; Larsen, C.M.; Astrup, A.; et al. Impact of short-term high-fat feeding on glucose and insulin metabolism in young healthy men. J. Physiol. 2009, 587, 2387–2397. [Google Scholar] [CrossRef]
- Dobiášová, M. Atherogenic Index of Plasma [Log(Triglycerides/HDL-Cholesterol)]: Theoretical and Practical Implications. Clin. Chem. 2004, 50, 1113–1115. [Google Scholar] [CrossRef]
- Emorine, L.J.; Marullo, S.; Delavier-Klutchko, C.; Kaveri, S.V.; Durieu-Trautmann, O.; Strosberg, A.D. Structure of the gene for human beta 2-adrenergic receptor: Expression and promoter characterization. Proc. Natl. Acad. Sci. USA 1987, 84, 6995–6999. [Google Scholar] [CrossRef] [Green Version]
- Rodeles, L.M.; Vicco, M.H.; Bontempi, I.A.; Siano, A.; Tonarelli, G.; Bottasso, O.A.; Arias, P.; Marcipar, I.S. Combined analysis of cross-reacting antibodies anti-β1AR and anti-B13 in advanced stages of Chagas heart disease. Trop. Med. Int. Health 2016, 21, 1545–1551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vicco, M.H.; Ferini, F.; Rodeles, L.; Cardona, P.; Bontempi, I.; Lioi, S.; Beloscar, J.; Nara, T.; Marcipar, I.; Bottasso, O.A. Assessment of Cross-reactive Host-pathogen Antibodies in Patients With Different Stages of Chronic Chagas Disease. Rev. Español. Cardiol. 2013, 66, 791–796. [Google Scholar] [CrossRef]
- Gumbiner, B.; Kelly, R.B. Two distinct intracellular pathways transport secretory and membrane glycoproteins to the surface of pituitary tumor cells. Cell 1982, 28, 51–59. [Google Scholar] [CrossRef]
- Hotelling, H. Analysis of a complex of statistical variables into principal components. J. Educ. Psychol. 1933, 24, 417–441. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CON (n = 40) | CCD (n = 80) | p | |
|---|---|---|---|
| Age (years) # | 44.6 ± 12.8 | 49.1 ± 10.1 | ns |
| Sex (F/M) | 21/19 | 47/33 | ns |
| At-risk waist circumference (%) | 95.5 ± 14.5 | 98.7 ± 12.1 | ns |
| M (% ≥94 cm) | 73.7% (n = 14) | 81.3% (n = 26) | ns |
| F (% ≥80 cm) | 66.6% (n = 14) | 89.4% (n = 42) | 0.037 * |
| BMI (kg/m2; RI) ≈ | 25.8 (23.9–28.3) | 27.7(25.1–29.2) | ns |
| Underweight (%) | 5.00 | 5.00 | ns |
| Normal (%) | 35.0 | 32.5 | ns |
| Overweight (%) | 60.0 | 62.5 | ns |
| CON (n = 40) | CCD (n = 80) | p | |
|---|---|---|---|
| FINDRISC Score (% ≥12 p) | 20.0% (n = 8) | 47.4% (n = 37) | 0.039 * |
| Dysglycemic states | |||
| IFG and/or ITG (%) | 37.5 (22.5/20) | 72.5 (62.5/31.3) | 0.001 * |
| Combined IFG and ITG (%) | 7.60 (n = 19) | 20.8 (n = 26) | 0.020 * |
| Metabolic Syndrome (%) | 35.1% (n = 14) | 66.2% (n = 53) | 0.002 * |
| Insulin resistance | |||
| HOMA2-IR ≈ | 1.28 (0.940–1.98) | 1.90 (1.05–3.30) | 0.019 ‡ |
| Matsuda index ≈ | 2.82 (1.75–3.83) | 1.49 (0.876–2.59) | <0.001 ~ |
| Insulin secretion | |||
| HOMA2-%β # | 113 ± 25.1 | 114 ± 47.7 | ns |
| Insulinogenic index ≈ | 0.508 (0.292–1.11) | 1.03 (0.476–1.74) | 0.004 ~ |
| Peripheral disposition (PIDI) ≈ | 5.13 (2.61–9.03) | 7.95 (3.56–14.8) | ns |
| Anti-β2AR Antibody Status | p | ||
|---|---|---|---|
| Negative (n = 24) | Positive (n = 56) | ||
| Age (years) # | 46.6 ± 10.5 | 49.7 ± 9.46 | ns |
| Sex (F/M) | 15/9 | 31/25 | ns |
| Waist circumference | |||
| M (% ≥94 cm) | 33.3% (n = 3) | 39.2% (n = 10) | ns |
| F (% ≥82 cm) | 60.0% (n = 9) | 90.3% (n = 28) | ns |
| BMI (kg/m2; RI) ≈ | 26.8 (23.4–29.5) | 28.1 (25.6–29.1) | ns |
| FINDRISC Score # | 8.30 ± 4.71 | 11.1 ± 4.97 | 0.028 ‡ |
| FINDRISC Score (% ≥12 p) | 31.8% (n = 6) | 54.0% (n = 31) | 0.025 * |
| Dysglycemic states (IFG or ITG) | 70.8% (n = 17; 54.1%/29.1%) | 78.5% (n = 44; 69.6%/39.2%) | ns |
| Combined IFG and ITG | 8.30% (n = 2) | 26.7% (n = 15) | 0.042 * |
| Metabolic syndrome | 45.8% (n = 11) | 75.0% (n = 42) | 0.014 * |
| Fasting glycemia (mg/dL) ≈ | 100 (91.5–107) | 110 (94.7–115) | 0.046 ~ |
| Fasting insulin (µU/mL) ≈ | 8.84 (6.65–15.6) | 15.5 (10.4–25.6) | 0.006 ~ |
| HOMA2-IR # | 1.61 ± 1.33 | 2.54 ± 1.41 | 0.010 ‡ |
| Matsuda index ≈ | 2.14 (1.25–2.82) | 1.22 (0.724–2.09) | 0.030 ~ |
| HOMA2-β% # | 95.1 ± 40.9 | 122 ± 48.1 | 0.021 ‡ |
| Insulinogenic index ≈ | 0.869 (0.487–1.81) | 1.20 (0.470–1.82) | ns |
| PIDI ≈ | 11.21 (5.42–21.2) | 5.91 (2.88–14.2) | 0.024 ~ |
| Retained Variables | OR (95% CI) | p |
|---|---|---|
| Age ≥ 50 years | 3.83 (1.30–11.25) | 0.014 |
| (+) Anti-β2AR Abs (IDO ≥ 1.20) | 7.01 (2.39–20.5) | 0.0004 |
| Model AUC: 0.786 | (95% CI: 0.676–0.873) | p < 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodeles, L.M.; Vicco, M.H.; Siano, Á.; Fuchs, L.A.; Peverengo, L.M.; Sanchez Puch, S.; Cymeryng, C.B.; Marcipar, I.S.; Arias, P. Functional Autoreactive Anti-β2 Adrenergic Antibodies May Contribute to Insulin Resistance Profile in Patients with Chronic Chagas Disease. Pathogens 2021, 10, 378. https://doi.org/10.3390/pathogens10030378
Rodeles LM, Vicco MH, Siano Á, Fuchs LA, Peverengo LM, Sanchez Puch S, Cymeryng CB, Marcipar IS, Arias P. Functional Autoreactive Anti-β2 Adrenergic Antibodies May Contribute to Insulin Resistance Profile in Patients with Chronic Chagas Disease. Pathogens. 2021; 10(3):378. https://doi.org/10.3390/pathogens10030378
Chicago/Turabian StyleRodeles, Luz María, Miguel Hernán Vicco, Álvaro Siano, Leonardo Andrés Fuchs, Luz María Peverengo, Silvia Sanchez Puch, Cora Beatriz Cymeryng, Iván Sergio Marcipar, and Pablo Arias. 2021. "Functional Autoreactive Anti-β2 Adrenergic Antibodies May Contribute to Insulin Resistance Profile in Patients with Chronic Chagas Disease" Pathogens 10, no. 3: 378. https://doi.org/10.3390/pathogens10030378