
Human Astrovirus in Symptomatic and Asymptomatic Children: A Cross-Sectional Study on Hospitalized and Outpatients from Rural Communities of South Africa between 2017–2021


Abstract
:1. Introduction
2. Results
2.1. Study Characteristics, Clinical Features of Children and Astrovirus Prevalence
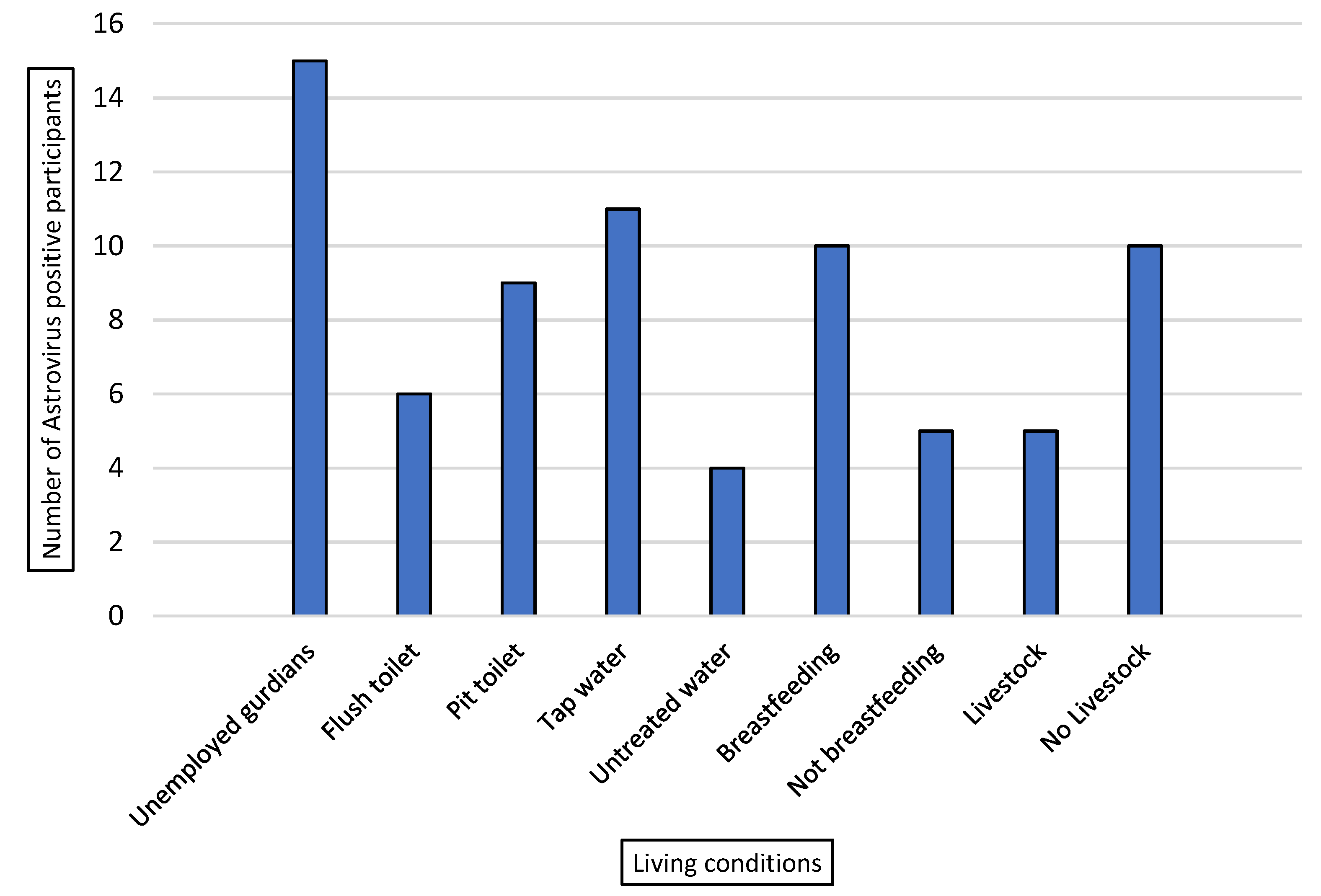
2.2. Living Conditions of Study Participants and Astrovirus Positive Cases
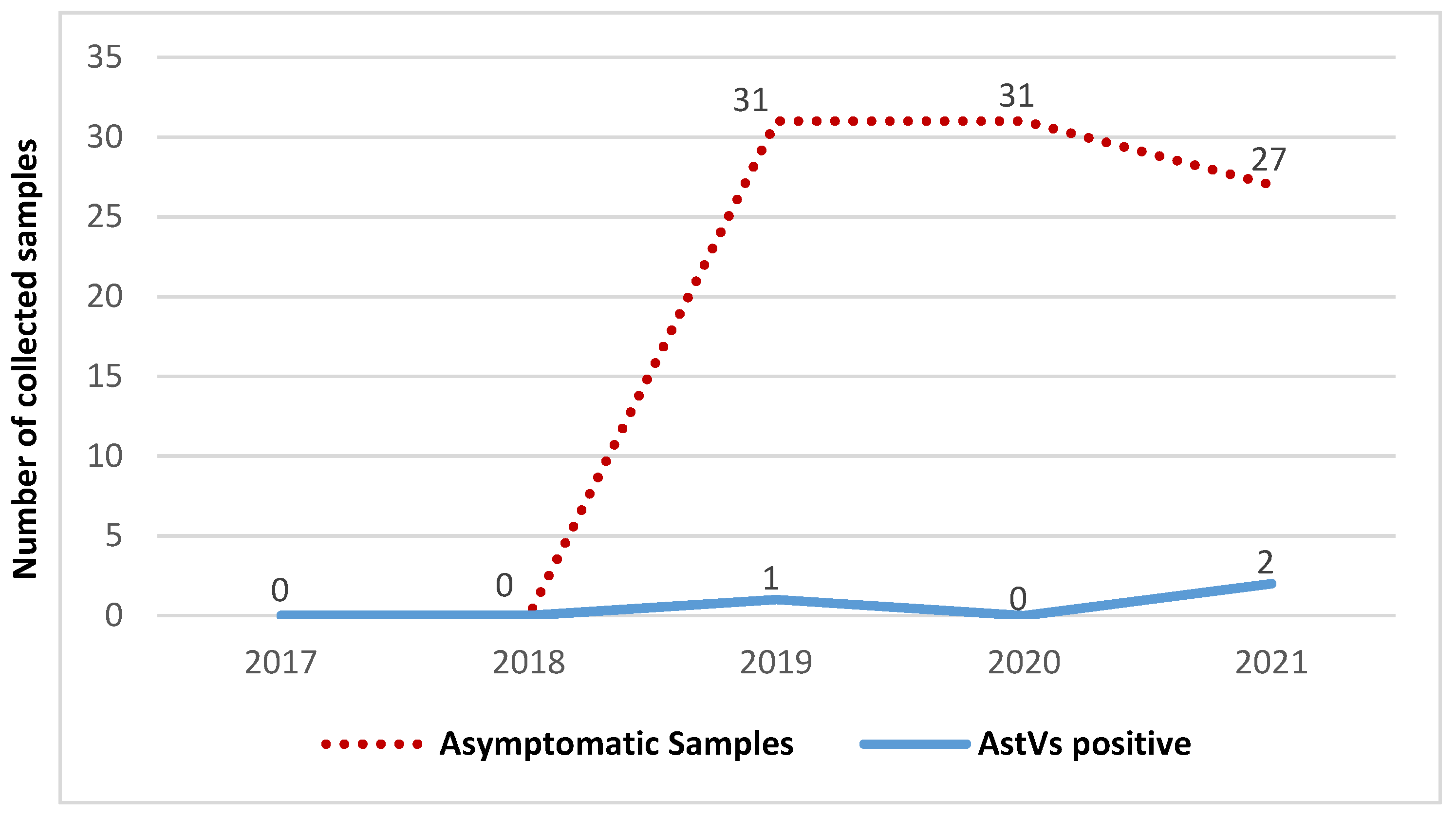
2.3. Comparison of Astrovirus Prevalence in Symptomatic and Asymptomatic Children
2.4. Comparison of Astrovirus Prevalence in Hospitalized and Outpatient Children
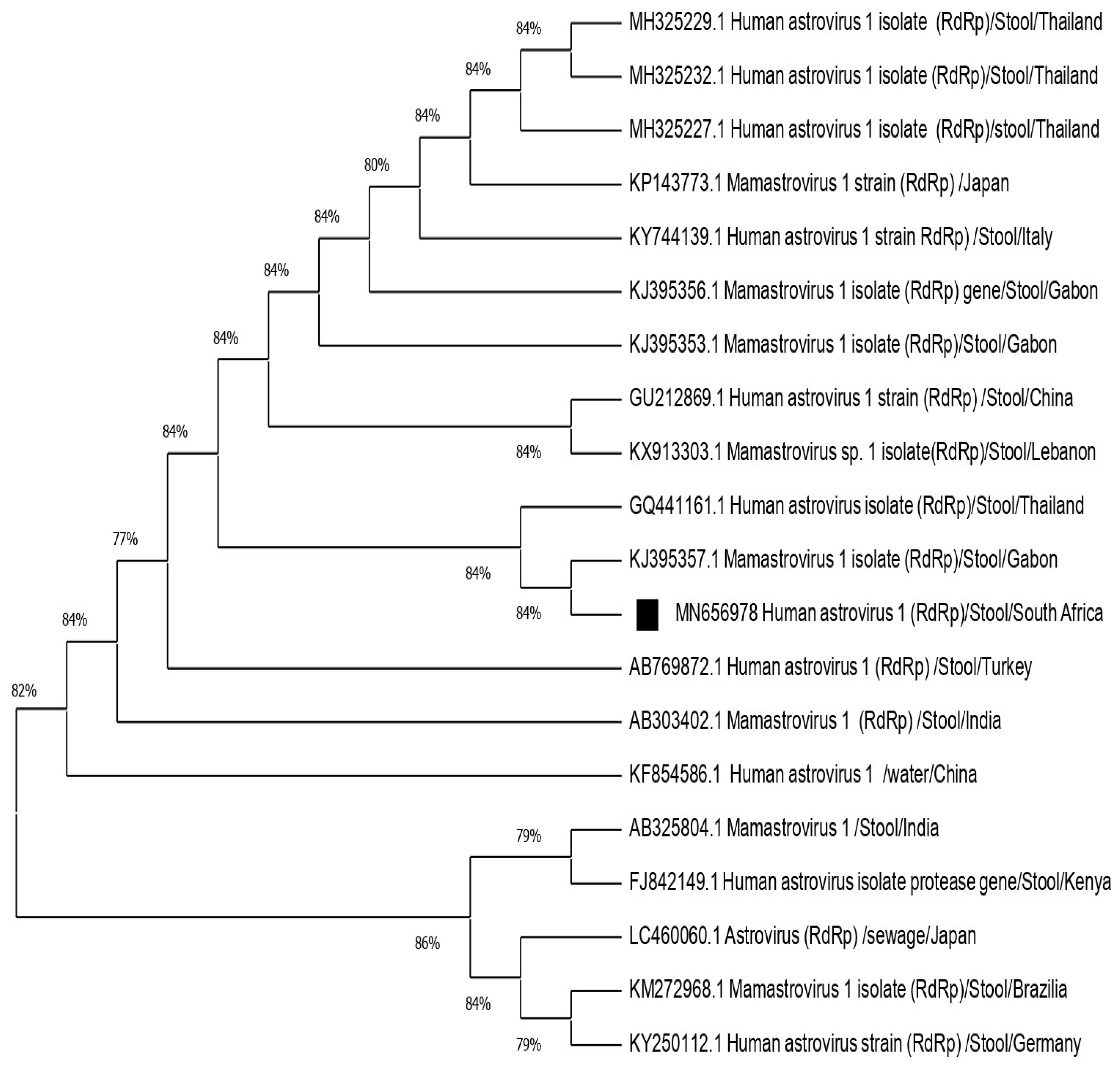
2.5. Genotyping and Phylogenetic Analysis
3. Discussion
4. Materials and Methods
4.1. Ethics
4.2. Study Population and Sample Collection
4.3. Sample Processing
4.3.1. RNA Extraction
4.3.2. Real-Time PCR for Astrovirus Detection
4.3.3. Astrovirus RT-PCR Amplification
4.3.4. Genotyping and Phylogenetic Analysis of Astrovirus
4.3.5. Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Troeger, C.; Blacker, B.F.; Khalil, I.A.; Rao, P.C.; Cao, S.; Zimsen, S.R.; Albertson, S.B.; Stanaway, J.D.; Deshpande, A.; Abebe, Z.; et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: A systematic analysis for the global burden of disease study 2016. Lancet Infect. Dis. 2018, 18, 1211–1228. [Google Scholar] [CrossRef] [Green Version]
- Vu, D.L.; Bosch, A.; Pintó, R.M.; Guix, S. Epidemiology of classic and novel human astrovirus: Gastroenteritis and beyond. Viruses 2017, 9, 33. [Google Scholar] [CrossRef]
- Bosch, A.; Pintó, R.M.; Guix, S. Human astroviruses. Clin. Microbiol. Rev. 2014, 27, 1048–1074. [Google Scholar] [CrossRef] [Green Version]
- Jeong, H.S.; Jeong, A.; Cheon, D.S. Epidemiology of astrovirus infection in children. Korean J. Pediatrics 2012, 55, 77. [Google Scholar] [CrossRef] [PubMed]
- Moser, L.; Schultz-Cherry, S. Astroviruses. Encycl. Virol. 2008, 3, 204. [Google Scholar]
- Appleton, H.; Higgins, P.G. Viruses and gastroenteritis in infants. Lancet 1975, 1, 1297. [Google Scholar] [CrossRef]
- Johnson, J.A.; Parra, G.I.; Levenson, E.A.; Green, K.Y. A large outbreak of acute gastroenteritis in Shippensburg, Pennsylvania, 1972 revisited: Evidence for common source exposure to a recombinant GII. Pg/GII. 3 noroviruses. Epidemiol. Infect. 2017, 145, 1591–1596. [Google Scholar] [CrossRef] [Green Version]
- Barbosa, G.; Caetano, A.; Dábilla, N.; Franco, F.; Silva-Sales, M.; Fiaccadori, F.; Souza, M. Classical human astroviruses in symptomatic and asymptomatic children of Goiás, Brazil: Positivity rates, viral loads, and molecular characterization. J. Med. Virol. 2020, 92, 1053–1058. [Google Scholar] [CrossRef]
- Méndez-Toss, M.; Griffin, D.D.; Calva, J.; Contreras, J.F.; Puerto, F.I.; Mota, F.; Guiscafré, H.; Cedillo, R.; Munoz, O.; Herrera, I.; et al. Prevalence and genetic diversity of human astroviruses in Mexican children with symptomatic and asymptomatic infections. J. Clin. Microbiol. 2004, 42, 151–157. [Google Scholar] [CrossRef] [Green Version]
- Rossouw, E.; Brauer, M.; Meyer, P.; du Plessis, N.M.; Avenant, T.; Mans, J. Virus etiology, diversity and clinical characteristics in south african children hospitalised with gastroenteritis. Viruses 2021, 13, 215. [Google Scholar] [CrossRef] [PubMed]
- Nadan, S.; Taylor, M.B.; Groome, M.J.; Cohen, C.; Madhi, S.A.; Page, N.A. Epidemiology of human astroviruses among children younger than 5 years: Prospective hospital-based sentinel surveillance in South Africa, 2009–2014. J. Med. Virol. 2019, 91, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Nadan, S.; Taylor, M.B.; Page, N.A. Circulation of classic and recombinant human astroviruses detected in South Africa: 2009 to 2014. J. Clin. Virol. 2021, 135, 104719. [Google Scholar] [CrossRef]
- Mulondo, G.; Khumela, R.; Kabue, J.P.; Traore, A.N.; Potgieter, N. Molecular characterization of norovirus strains isolated from older children and adults in impoverished communities of Vhembe District, South Africa. Adv. Virol. 2020, 2020, 8436951. [Google Scholar] [CrossRef] [PubMed]
- Kabue, J.P.; Meader, E.; Hunter, P.R.; Potgieter, N. Norovirus prevalence and estimated viral load in symptomatic and asymptomatic children from rural communities of Vhembe district, South Africa. J. Clin. Virol. 2016, 84, 12–18. [Google Scholar] [CrossRef] [Green Version]
- Gelaw, A.; Pietsch, C.; Liebert, U.G. Genetic diversity of human adenovirus and human astrovirus in children with acute gastroenteritis in Northwest Ethiopia. Arch. Virol. 2019, 164, 2993. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.A.M.; de Souza Oliveira, D.; de Carvalho, T.C.N.; Portal, T.M.; Justino, M.C.A.; da Silva, L.D.; Resque, H.R.; Gabbay, Y.B. Astrovirus infection in hospitalized children: Molecular, clinical and epidemiological features. J. Clin. Virol. 2017, 94, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Arowolo, K.O.; Ayolabi, C.I.; Adeleye, I.A.; Lapinski, B.; Santos, J.S.; Raboni, S.M. Molecular epidemiology of astrovirus in children with gastroenteritis in southwestern Nigeria. Arch. Virol. 2020, 165, 2461–2469. [Google Scholar] [CrossRef] [PubMed]
- Olortegui, M.P.; Rouhani, S.; Yori, P.P.; Salas, M.S.; Trigoso, D.R.; Mondal, D.; Bodhidatta, L.; Platts-Mills, J.; Samie, A.; Kabir, F.; et al. Astrovirus infection and diarrhea in 8 countries. Pediatrics 2018, 141, 20171326. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, S.; Hassan, E.; Baldridge, M.T. Experimental methods to study the pathogenesis of human enteric RNA viruses. Viruses 2021, 13, 975. [Google Scholar] [CrossRef]
- Bishop, R.F.; Kirkwood, C.D. Enteric Viruses, Reference Module in Biomedical Sciences; Elsevier: Amsterdam, The Netherlands, 2014; ISBN 9780128012383. [Google Scholar] [CrossRef]
- Makimaa, H.; Ingle, H.; Baldridge, M.T. Enteric viral co-infections: Pathogenesis and perspective. Viruses 2020, 12, 904. [Google Scholar] [CrossRef]
- Naficy, A.B.; Rao, M.R.; Holmes, J.L.; Abu-Elyazeed, R.; Savarino, S.J.; Wierzba, T.F.; Frenck, R.W.; Monroe, S.S.; Glass, R.I.; Clemens, J.D. Astrovirus diarrhea in Egyptian children. J. Infect. Dis. 2000, 182, 685–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moser, L.A.; Schultz-Cherry, S. Suppression of astrovirus replication by an ERK1/2 inhibitor. J. Virol. 2008, 82, 7475–7482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, D.K.; Matson, D.O.; Jiang, X.; Berke, T.; Monroe, S.S.; Carter, M.J.; Willcocks, M.M.; Pickering, L.K. Molecular epidemiology of childhood astrovirus infection in child care centers. J. Infect. Dis. 1999, 180, 514–517. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, R.G.; Marmot, M. (Eds.) Social Determinants of Health: The Solid Facts; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Dongdem, J.T.; Damanka, S.; Asmah, R. Molecular isolation of human norovirus and astrovirus in tap water by RT-PCR. Int. Res. J. Biochem. Bioinform. 2011, 1, 131–138. [Google Scholar]
- Arowolo, K.O.; Ayolabi, C.I.; Lapinski, B.; Santos, J.S.; Raboni, S.M. Epidemiology of enteric viruses in children with gastroenteritis in Ogun State, Nigeria. J. Med. Virol. 2019, 91, 1022–1029. [Google Scholar] [CrossRef]
- Kumthip, K.; Khamrin, P.; Ushijima, H.; Maneekarn, N. Molecular epidemiology of classic, MLB and VA astroviruses isolated from <5 year-old children with gastroenteritis in Thailand, 2011. Infect. Genet. Evol. 2018, 65, 373–379. [Google Scholar] [CrossRef]
- Lekana-Douki, S.E.; Kombila-Koumavor, C.; Nkoghe, D.; Drosten, C.; Drexler, J.F.; Leroy, E.M. Molecular epidemiology of enteric viruses and genotyping of rotavirus A, adenovirus and astrovirus among children under 5 years old in Gabon. Int. J. Infect. Dis. 2015, 34, 90–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfaardt, M.; Kiulia, N.M.; Mwenda, J.M.; Taylor, M.B. Evidence of a recombinant wild-type human astrovirus strain from a Kenyan child with gastroenteritis. J. Clin. Microbiol. 2011, 49, 728–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medici, M.C.; Tummolo, F.; Albonetti, V.; Abelli, L.A.; Chezzi, C.; Calderaro, A. Molecular detection and epidemiology of astrovirus, bocavirus, and sapovirus in Italian children admitted to hospital with acute gastroenteritis, 2008. J. Med. Virol. 2012, 84, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Zaraket, H.; Abou-El-Hassan, H.; Kreidieh, K.; Soudani, N.; Ali, Z.; Hammadi, M.; Reslan, L.; Ghanem, S.; Hajar, F.; Inati, A.; et al. Characterization of astrovirus-associated gastroenteritis in hospitalized children under five years of age. Infect. Genet. Evol. 2017, 53, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Xu, X.; Song, J.; Wang, W.; Wang, J.; Hung, T. Molecular characterization of astrovirus infection in children with diarrhea in Beijing, 2005. J. Med. Virol. 2010, 82, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Gabbay, Y.B.; Leite, J.P.G.; Oliveira, D.S.; Nakamura, L.S.; Nunes, M.R.; Mascarenhas, J.D.A.P.; Heinemann, M.B.; Linhares, A.C. Molecular epidemiology of astrovirus type 1 in Belem, Brazil, as an agent of infantile gastroenteritis, over a period of 18 years (1982–2000): Identification of two possible new lineages. Virus Res. 2007, 129, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Dalton, R.M.; Roman, E.R.; Negredo, A.A.; Wilhelmi, I.D.; Glass, R.I.; Sanchez-Fauquier, A. Astrovirus acute gastroenteritis among children in Madrid, Spain. Pediatric Infect. Dis. J. 2002, 21, 1038–1041. [Google Scholar] [CrossRef] [PubMed]
- Silva, P.A.; Stark, K.; Mockenhaupt, F.P.; Reither, K.; Weitzel, T.; Ignatius, R.; Saad, E.; Seidu-Korkor, A.; Bienzle, U.; Schreier, E. Molecular characterization of enteric viral agents from children in northern region of Ghana. J. Med. Virol. 2008, 80, 1790–1798. [Google Scholar] [CrossRef] [PubMed]
- Pativada, M.S.; Chatterjee, D.; Mariyappa, N.S.; Rajendran, K.; Bhattacharya, M.K.; Ghosh, M.; Kobayashi, N.; Krishnan, T. Emergence of unique variants and inter-genotype recombinants of human astroviruses infecting infants, children and adults in Kolkata, India. Int. J. Mol. Epidemiol. Genet. 2011, 2, 228. [Google Scholar] [PubMed]
- Jacobsen, S.; Höhne, M.; Marques, A.M.; Beslmüller, K.; Bock, C.T.; Niendorf, S. Co-circulation of classic and novel astrovirus strains in patients with acute gastroenteritis in Germany. J. Infect. 2018, 76, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C.T.; Bauer, I.K.; Antonio, M.; Adeyemi, M.; Saha, D.; Oundo, J.O.; Ochieng, J.B.; Omore, R.; Stine, O.C.; Wang, D.; et al. Prevalence of classic, MLB-clade and VA-clade Astroviruses in Kenya and The Gambia. Virol. J. 2015, 12, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vu, D.L.; Sabrià, A.; Aregall, N.; Michl, K.; Rodriguez Garrido, V.; Goterris, L.; Bosch, A.; Pintó, R.M.; Guix, S. Novel human astroviruses: Prevalence and association with common enteric viruses in undiagnosed gastroenteritis cases in Spain. Viruses 2019, 11, 585. [Google Scholar] [CrossRef] [Green Version]
- De Grazia, S.; Medici, M.C.; Pinto, P.; Moschidou, P.; Tummolo, F.; Calderaro, A.; Bonura, F.; Banyai, K.; Giammanco, G.M.; Martella, V. Genetic heterogeneity and recombination in human type 2 astroviruses. J. Clin. Microbiol. 2012, 50, 3760–3764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bull, R.A.; Tanaka, M.M.; White, P.A. Norovirus recombination. J. Gen. Virol. 2007, 88, 3347–3359. [Google Scholar] [CrossRef]
- World Health Organization. The World Health Report: 2005: Make Every Mother and Child Count; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Boom, R.C.J.A.; Sol, C.J.; Salimans, M.M.; Jansen, C.L.; Wertheim-van Dillen, P.M.; Van der Noordaa, J.P.M.E. Rapid and simple method for purification of nucleic acids. J. Clin. Microbiol. 1990, 28, 495–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noel, J.S.; Lee, T.W.; Kurtz, J.B.; Glass, R.I.; Monroe, S.S. Typing of human astroviruses from clinical isolates by enzyme immunoassay and nucleotide sequencing. J. Clin. Microbiol. 1995, 33, 797–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finkbeiner, S.R.; Le, B.M.; Holtz, L.R.; Storch, G.A.; Wang, D. Detection of newly described astrovirus MLB1 in stool samples from children. Emerg. Infect. Dis. 2009, 15, 441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Stecher, G.; Li, M.; Knyaz, C.; Tamura, K. MEGA X: Molecular evolutionary genetics analysis across computing platforms. Mol. Biol. Evol. 2018, 35, 1547–1549. [Google Scholar] [CrossRef] [PubMed]
- Saitou, N.; Nei, M. The neighbor-joining method: A new method for reconstructing phylogenetic trees. Mol. Biol. Evol. 1987, 4, 406–425. [Google Scholar] [PubMed]
- Felsenstein, J. Confidence limits on phylogenies: An approach using the bootstrap. Evolution 1985, 39, 783–791. [Google Scholar] [CrossRef]
- Nei, M.; Kumar, S. Molecular Evolution and Phylogenetics; Oxford University Press: Oxford, UK, 2000. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Symptomatic Patients | Asymptomatic Patients | |||||||
|---|---|---|---|---|---|---|---|---|
| Total Symptomatic Patients Enrolled | Outpatients | Hospitalized | ||||||
| n | No. of Positive (%) | n | Astrovirus Prevalence (%) | n | Astrovirus Prevalence (%) | n | Astrovirus Prevalence (%) | |
| Detection rate | 166 | 12 (7.23) | 120 | 9 (7.5) | 46 | 3 (6.52) | 70 | 3 (4.29) |
| Gender | ||||||||
| Males | 79 | 7 (8.86) | 51 | 5 (9.80) | 28 | 2 7.14) | 32 | 2 (6.25) |
| Females | 87 | 5 (5.74) | 69 | 4 (5.80) | 18 | 1 (5.56) | 38 | 1 (2.63) |
| Age groups (months) | ||||||||
| 0–6 | 33 | 6 (18.18) | 27 | 5 (18.51) | 6 | 1 (16.67) | 19 | 1 (5.26) |
| 7–12 | 52 | 2 (3.84) | 30 | 1 (3.33) | 22 | 1 (5.55) | 11 | 0 |
| 13–24 | 50 | 2(4) | 36 | 1 (0.83) | 14 | 1 (7.14) | 26 | 1 (3.85) |
| ≥25 | 31 | 2 (6.45) | 27 | 2 (2.78) | 4 | 0 | 14 | 1 (7.14) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khumela, R.; Kabue, J.P.; Traore, A.N.; Potgieter, N. Human Astrovirus in Symptomatic and Asymptomatic Children: A Cross-Sectional Study on Hospitalized and Outpatients from Rural Communities of South Africa between 2017–2021. Pathogens 2021, 10, 1398. https://doi.org/10.3390/pathogens10111398
Khumela R, Kabue JP, Traore AN, Potgieter N. Human Astrovirus in Symptomatic and Asymptomatic Children: A Cross-Sectional Study on Hospitalized and Outpatients from Rural Communities of South Africa between 2017–2021. Pathogens. 2021; 10(11):1398. https://doi.org/10.3390/pathogens10111398
Chicago/Turabian StyleKhumela, Ronewa, Jean Pierre Kabue, Afsatou Ndama Traore, and Natasha Potgieter. 2021. "Human Astrovirus in Symptomatic and Asymptomatic Children: A Cross-Sectional Study on Hospitalized and Outpatients from Rural Communities of South Africa between 2017–2021" Pathogens 10, no. 11: 1398. https://doi.org/10.3390/pathogens10111398