
Pandemic Portraits—An Intersectional Analysis of the Experiences of People with Disabilities and Caregivers during COVID-19 in Bangladesh and Liberia

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Approach
2.2. Co-Researcher Selection and Study Sites
3. Data Collection
4. Analysis
5. Results
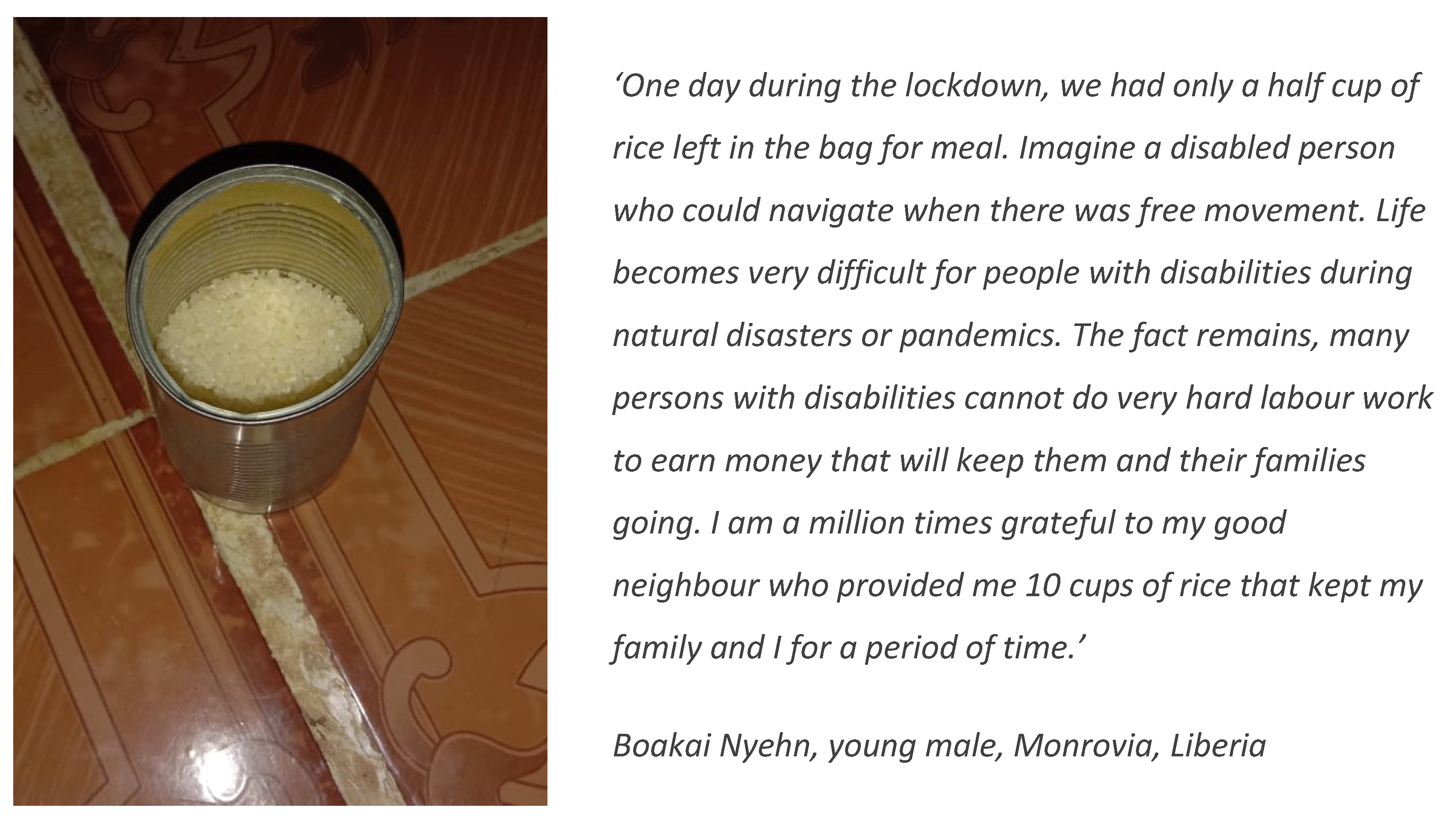
5.1. Impact on Livelihoods
‘We have been in a financial crisis since last year due to the COVID-19 epidemic. Living in a lower middle income family, we cannot share our problems with others. We have faced trouble to afford my son’s regular medicine for his special needs. I joined as a Nursing Officer in Dhaka Medical College last year but still I did not get any salary from there. Now I cannot go to work due to the lockdown.’(Bithi Akter, 30-year-old female caregiver of son with cerebral palsy, Bangladesh)
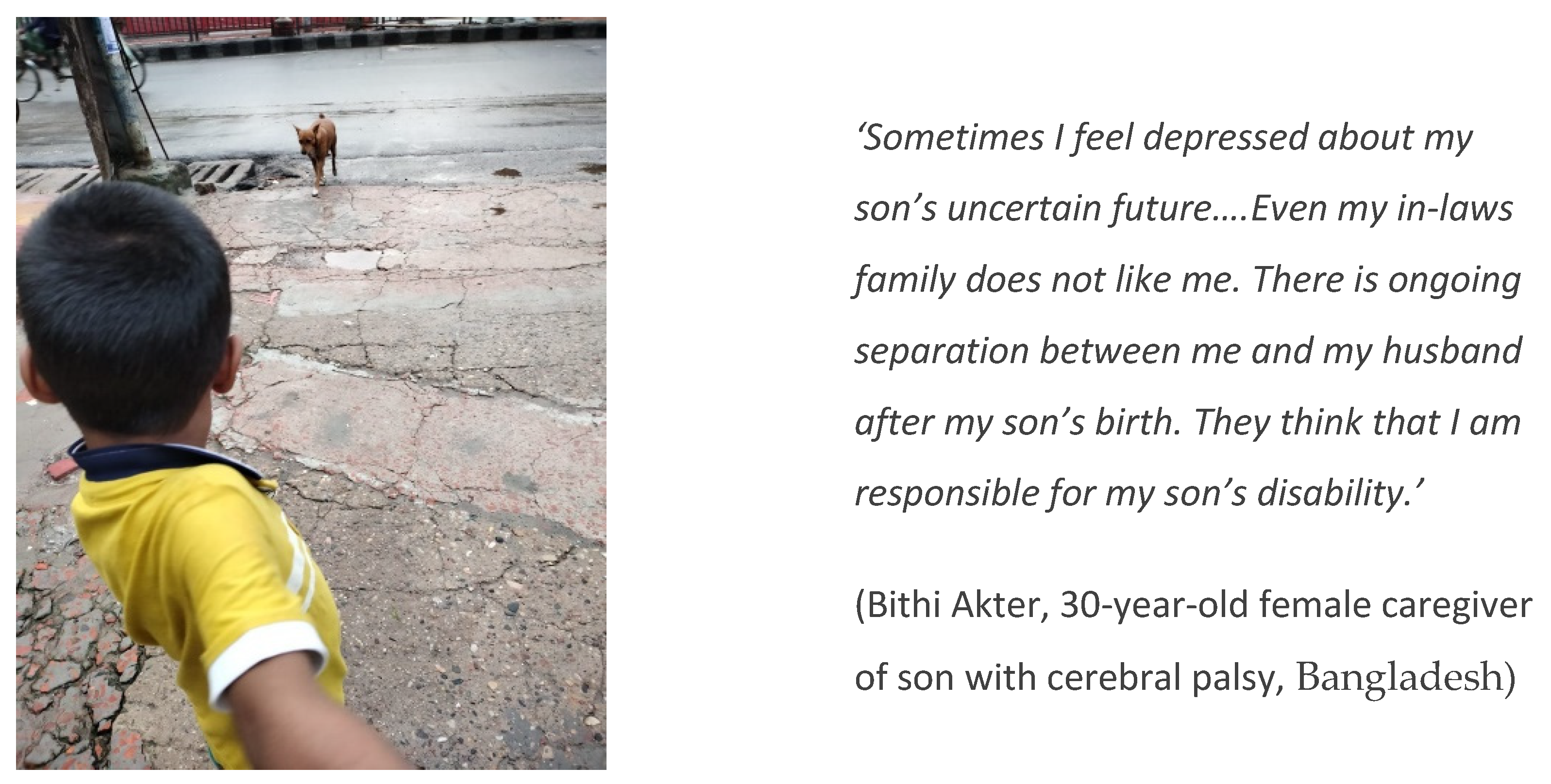
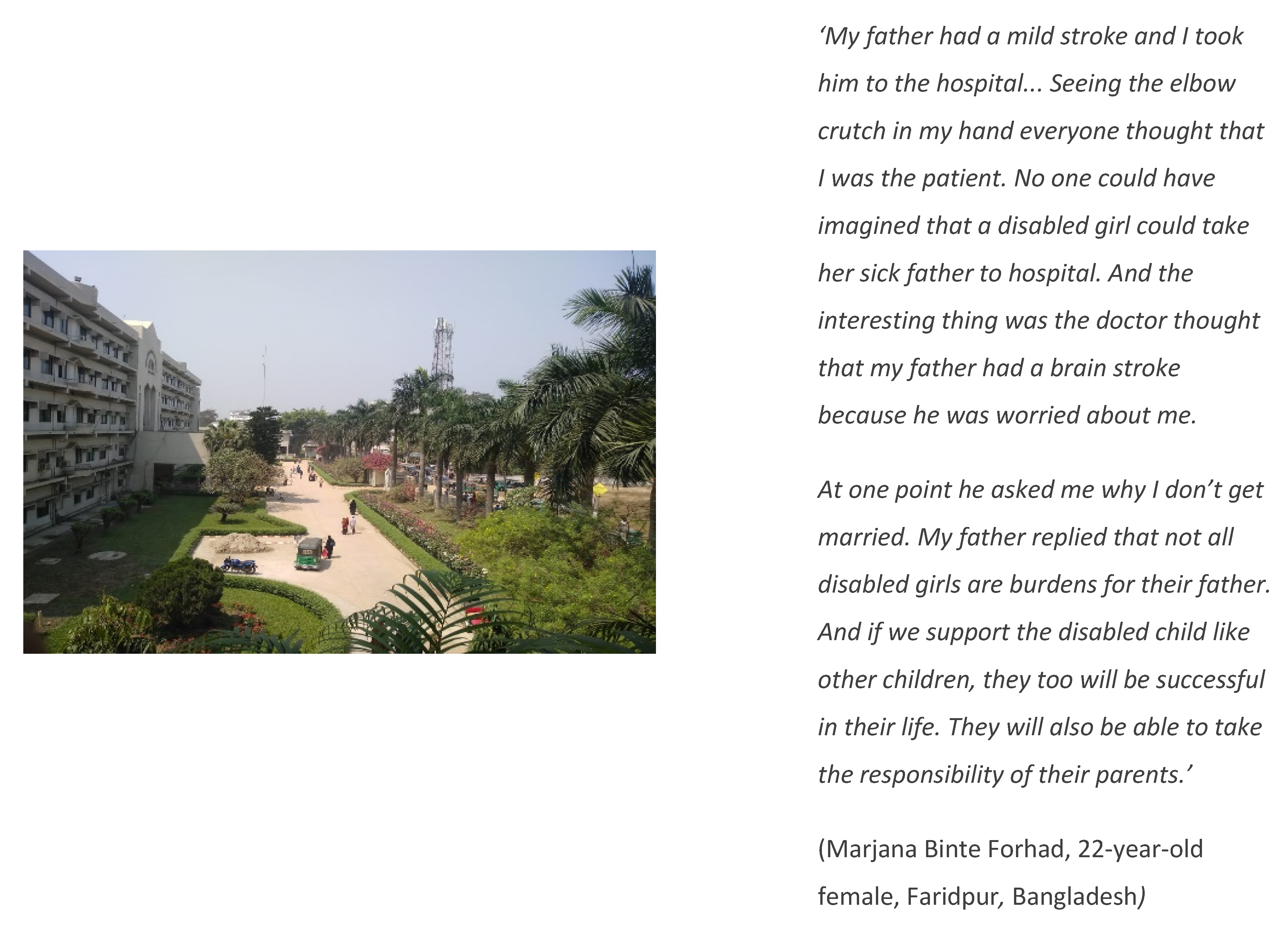
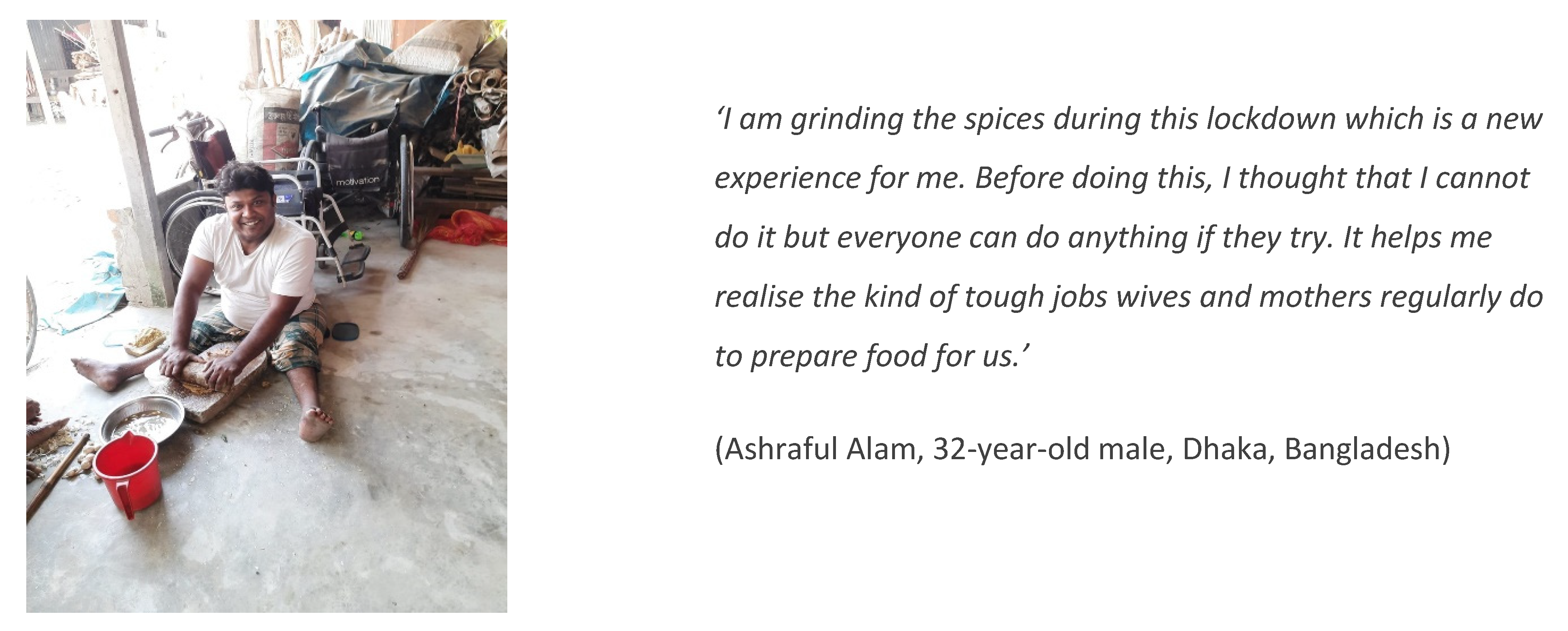
5.2. Gendered Impacts
‘Munni wants to get married... We feel that she does not have a clear idea about what marriage is… I am her elder sister-in-law. I have taken care of her for around 8/9 years. However, we don’t want to let her get married to someone. She cannot understand anything properly… Is it possible? We do not want to ruin her life.’(Fatema Rahman Sumi, 32-year-old female caregiver of sister-in-law with psychosocial disability, Bangladesh)
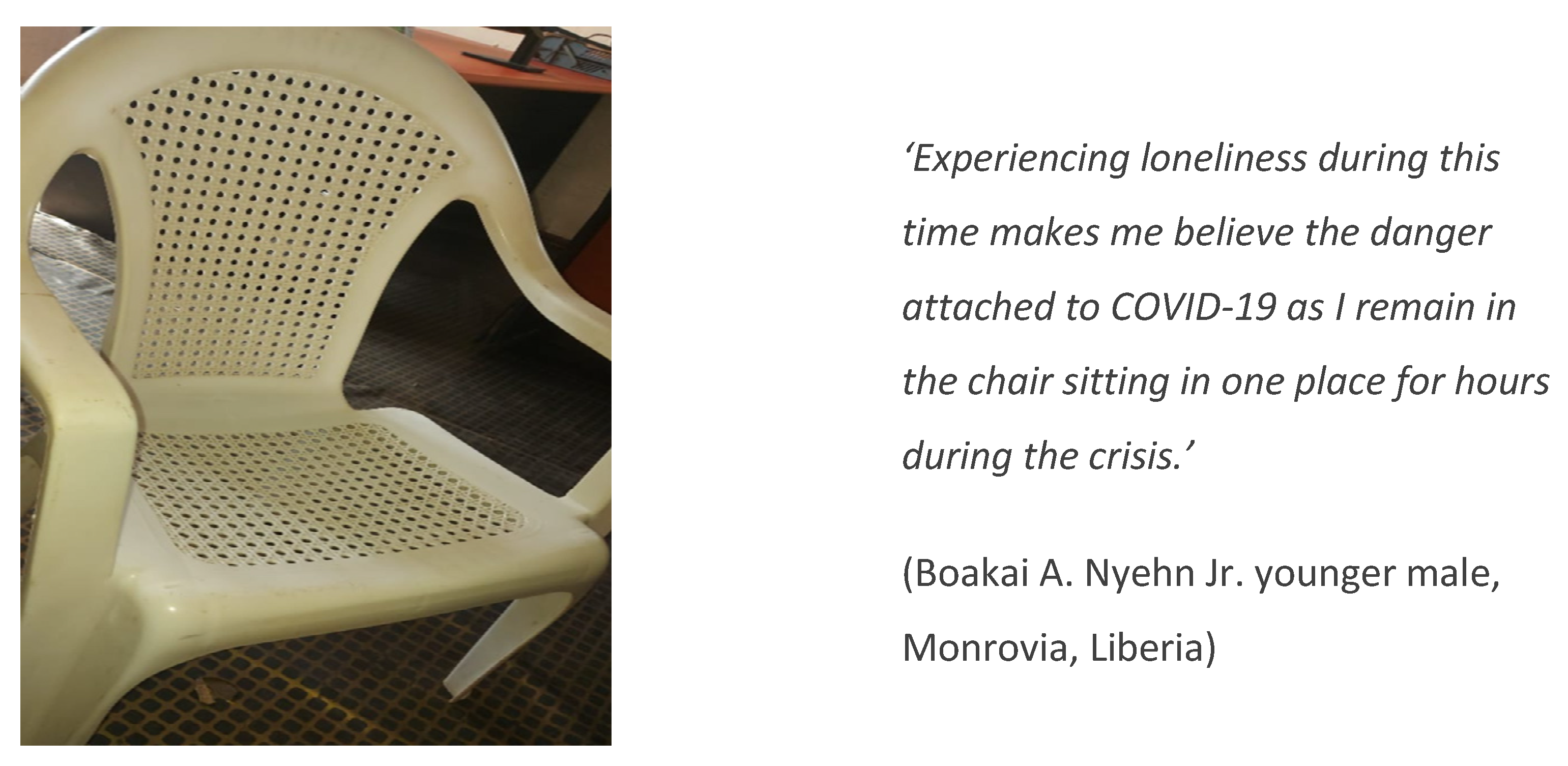
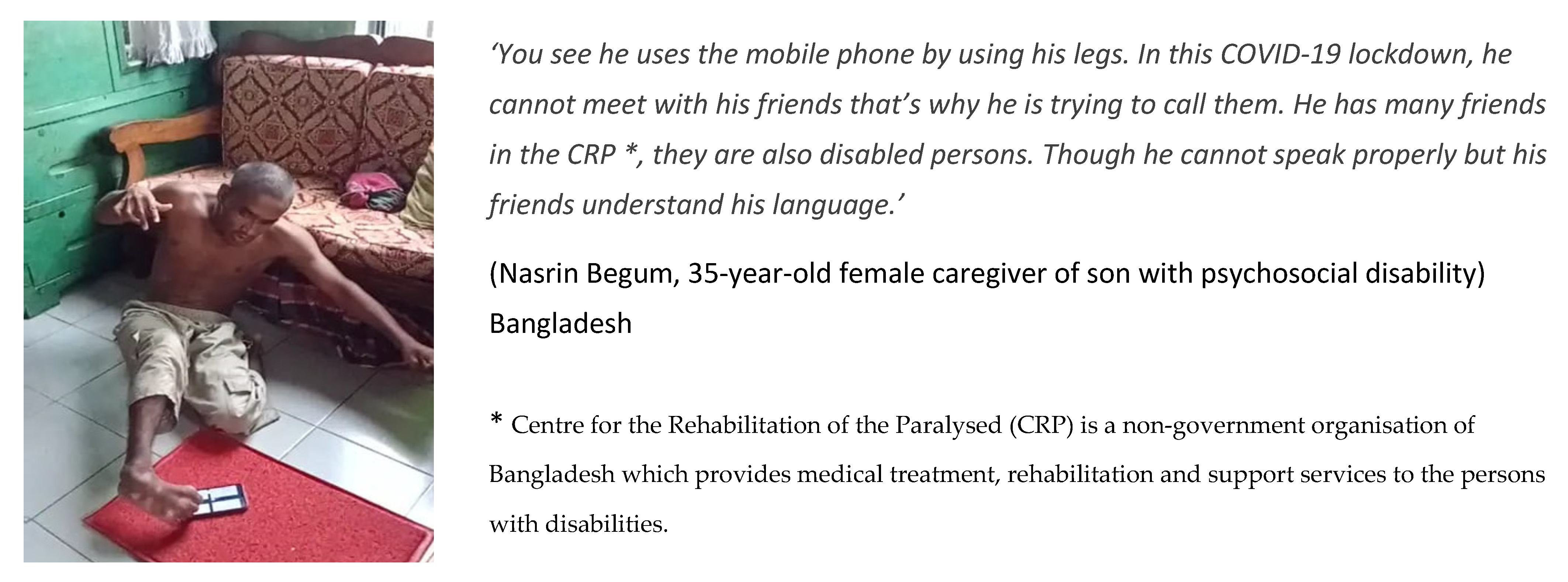
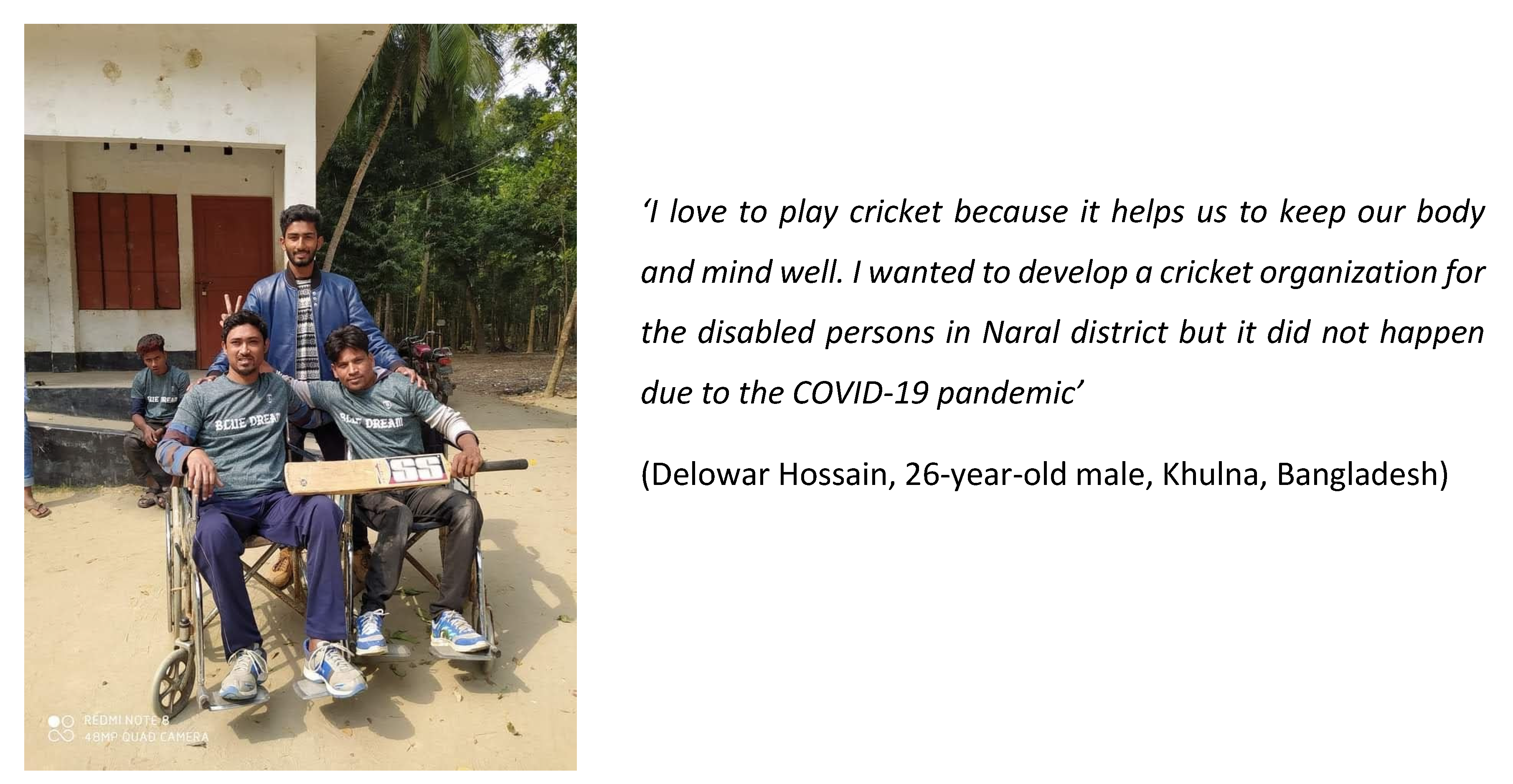
5.3. Social Connection
‘We are experiencing loneliness during the current coronavirus pandemic. Now we cannot meet with relatives, neighbours or friends to talk about our feelings. Though we are now having a good time with family members, but we are missing our unlocked life. Now we have to rely on technology to communicate with others.’(Israt Jahan Isha, 18-year-old female, caregiver of sister with physical disability, Bangladesh)
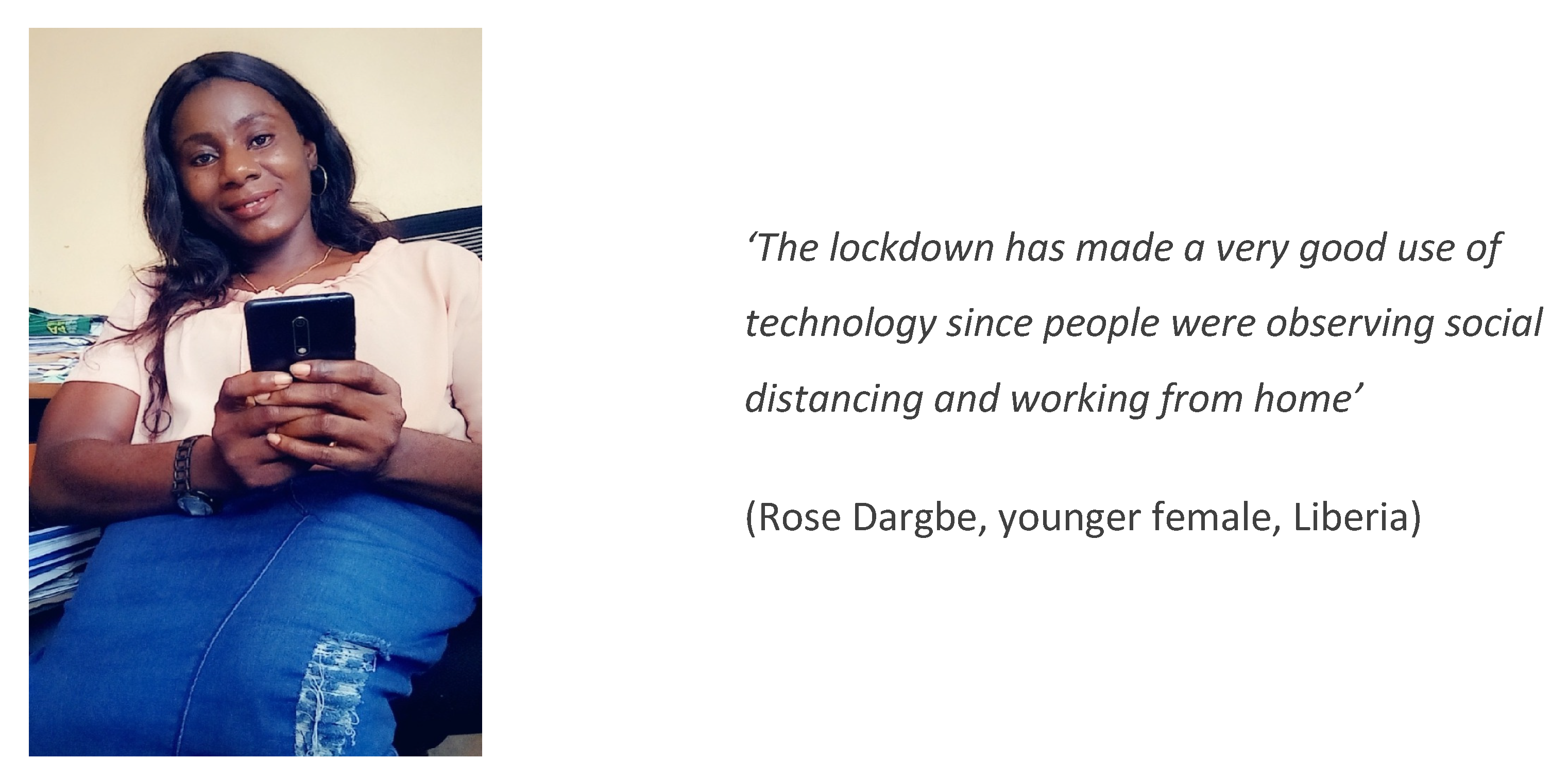
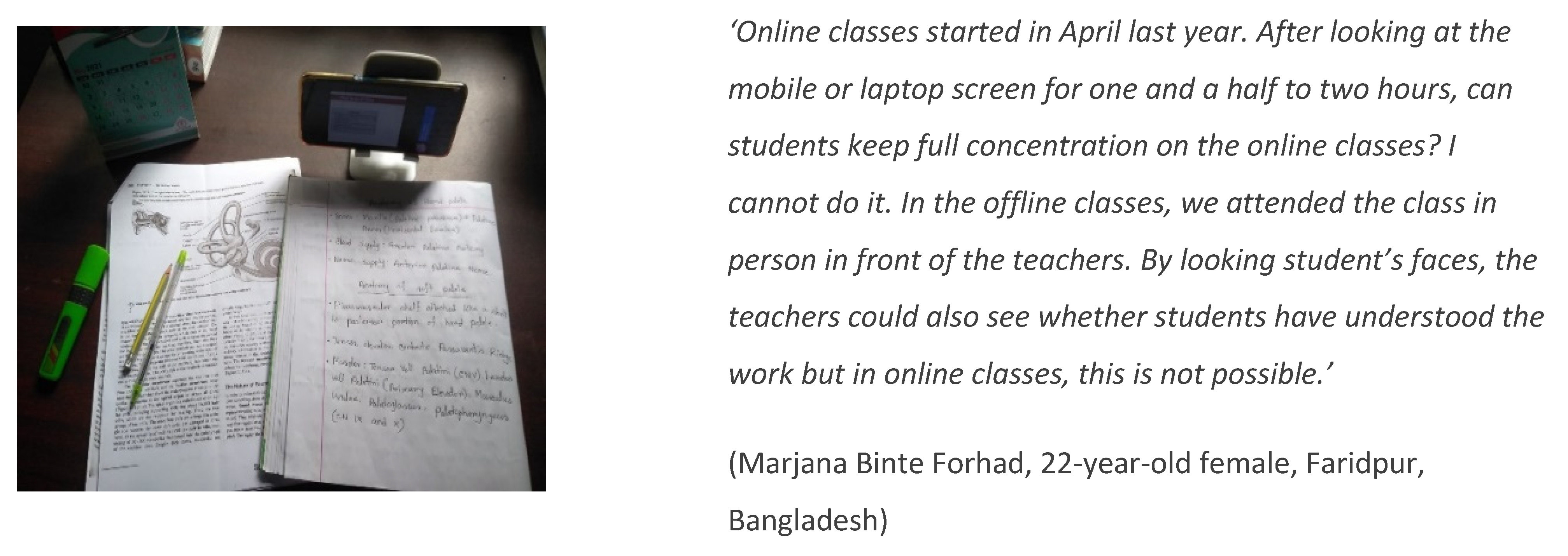
5.4. Adaptability and Technology
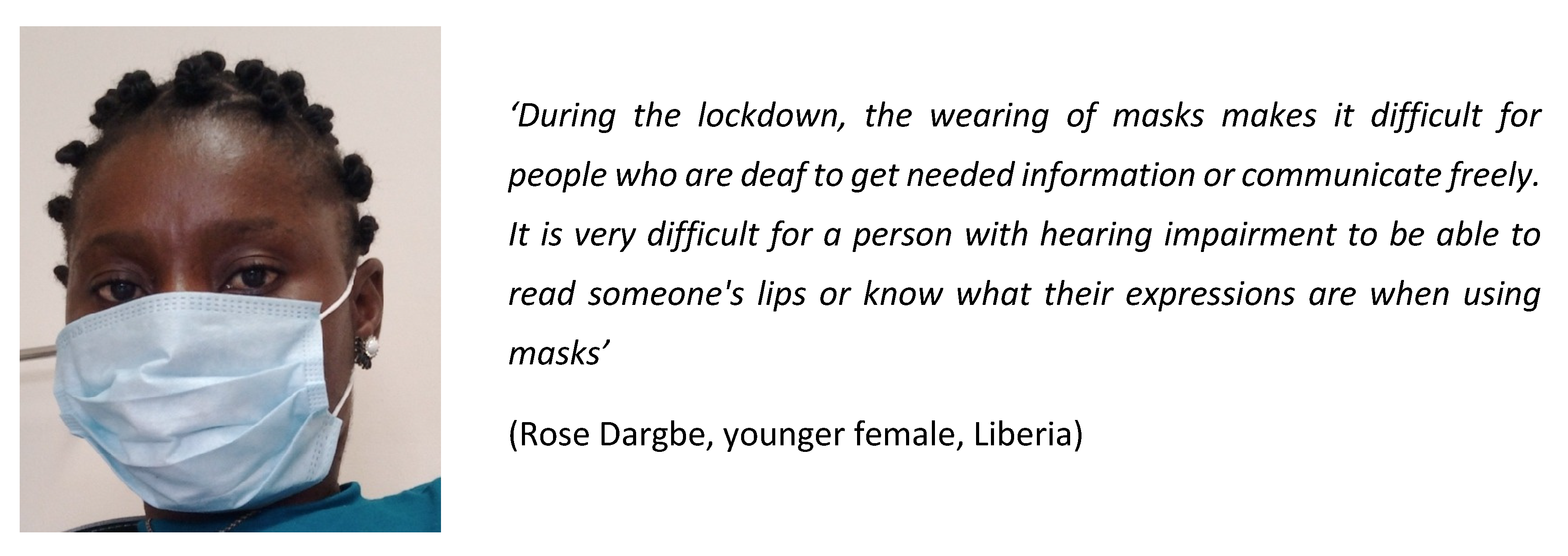
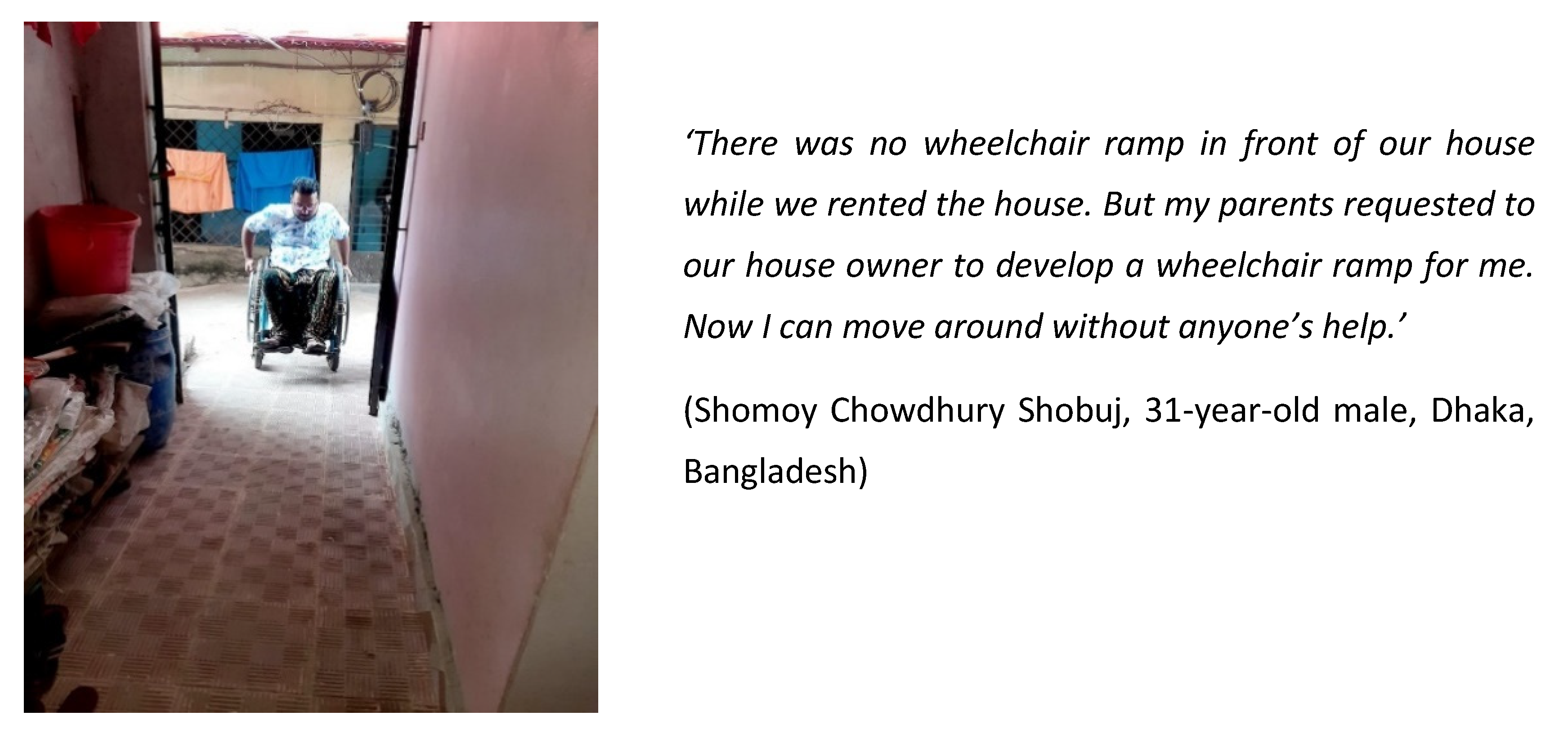
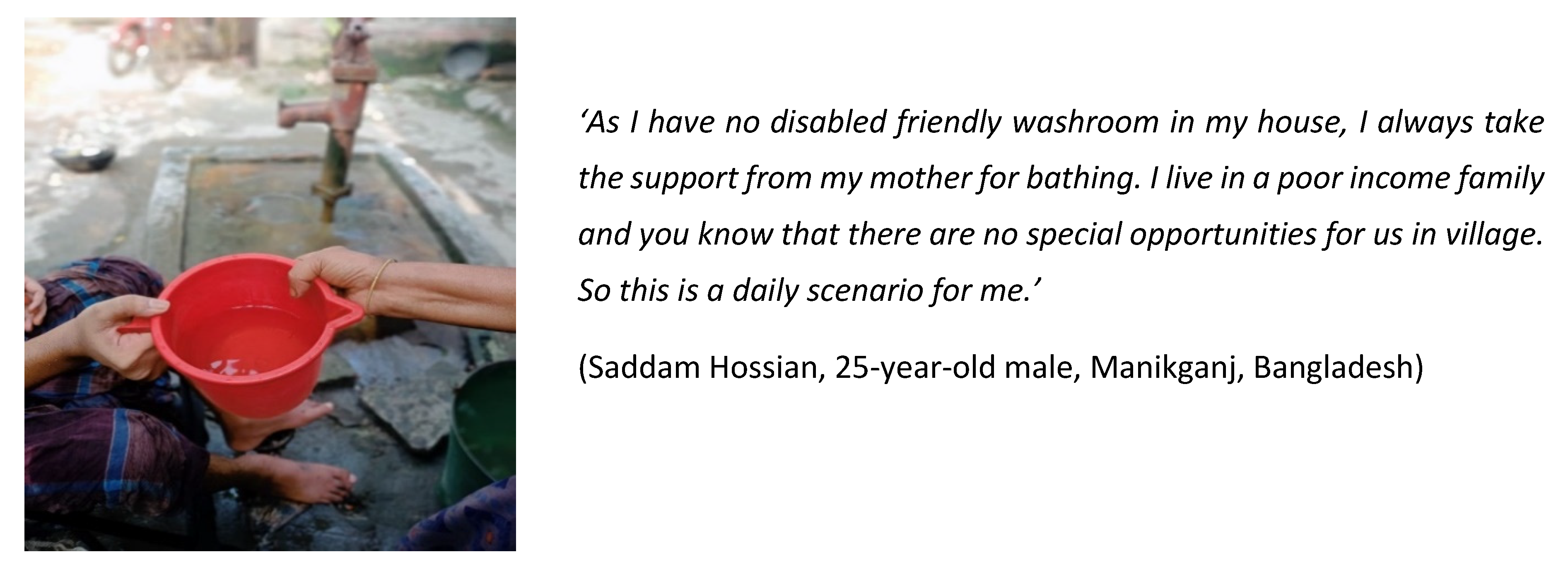
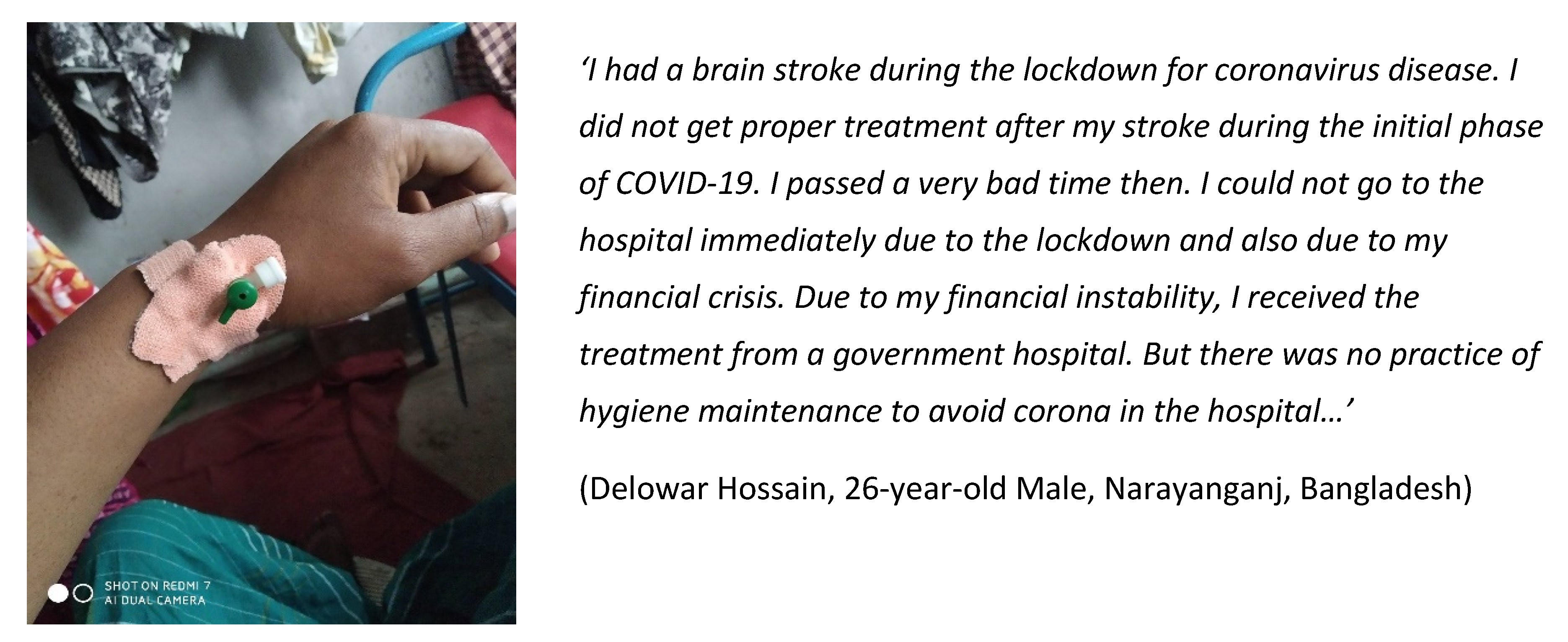
5.5. Accessibility and Awareness
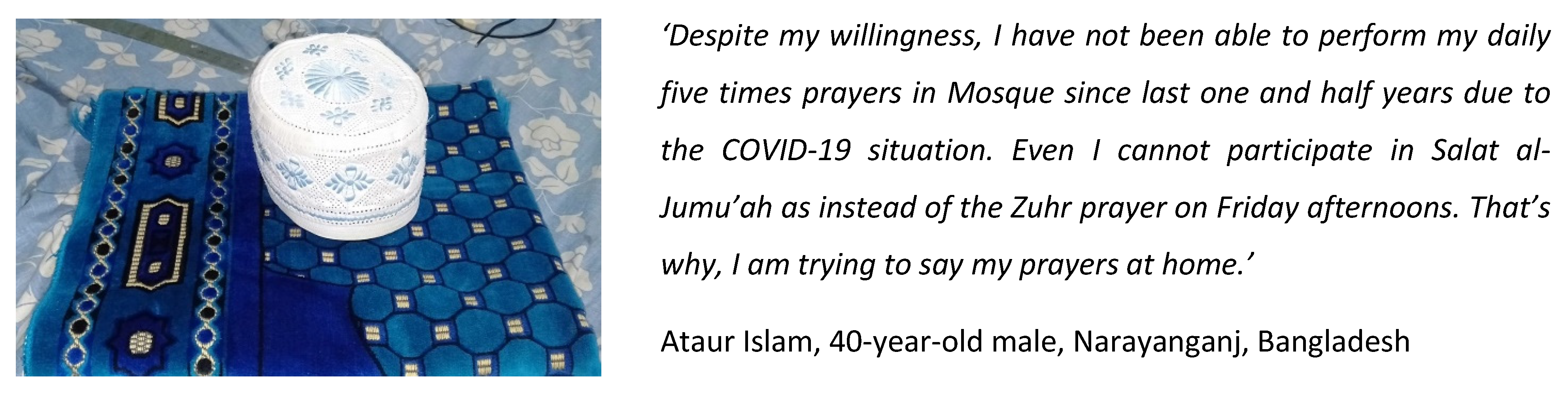
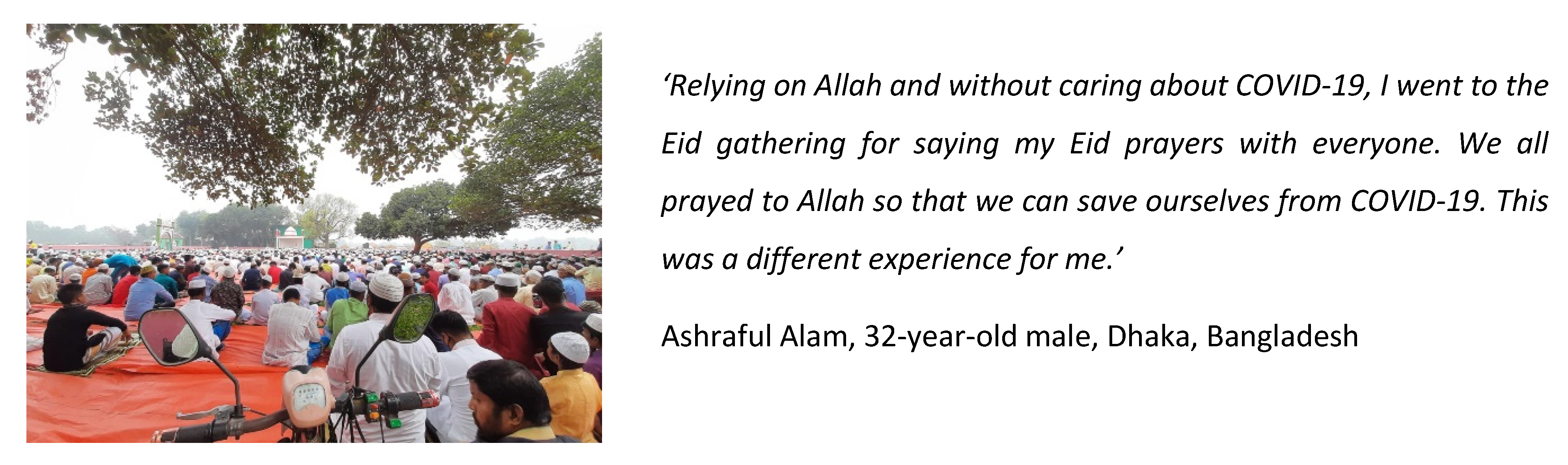
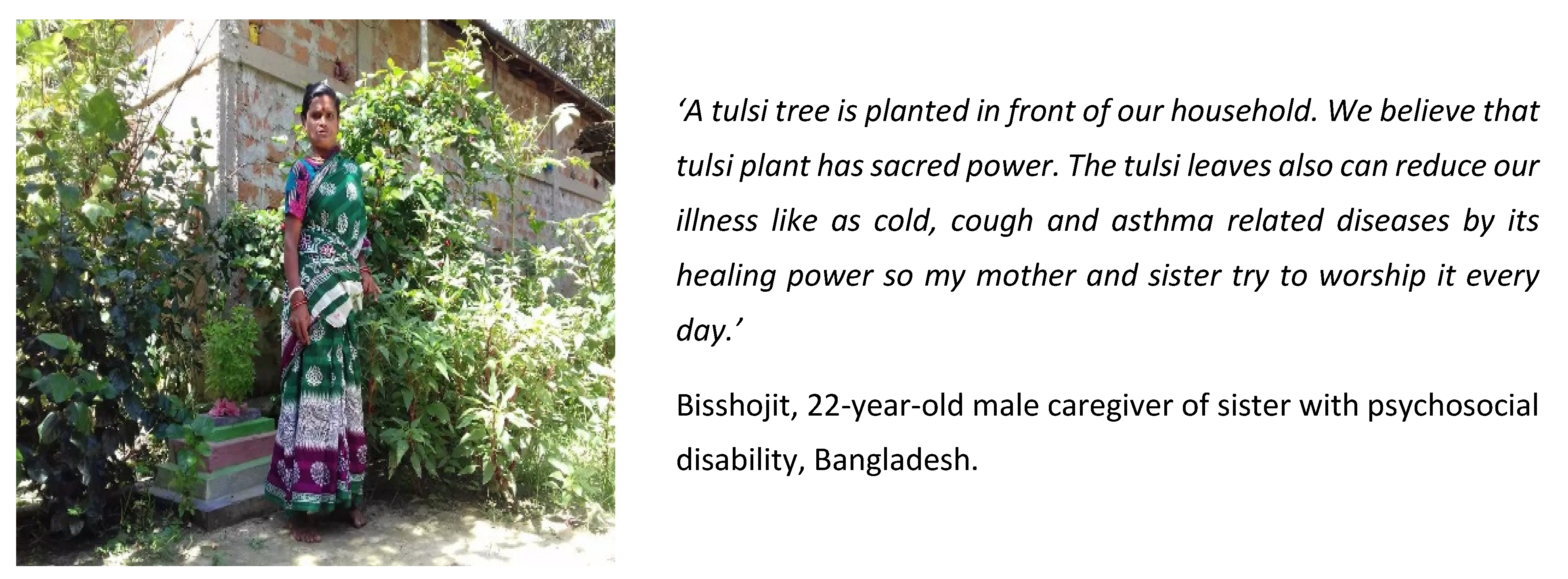
5.6. Faith and Nature
6. Discussion
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Banks, Lena Morgon, Hannah Kuper, and Sarah Polack. 2017. Poverty and disability in low-and middle-income countries: A systematic review. PLoS ONE 12: e0189996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banks, Lena Morgon, Calum Davey, Tom Shakespeare, and Hannah Kuper. 2021. Disability-inclusive responses to COVID-19: Lessons learnt from research on social protection in low- and middle-income countries. World Development 137: 105178. [Google Scholar] [CrossRef] [PubMed]
- Bertuzzi, Vanessa, Michelle Semonella, Denise Bruno, Chiara Manna, Julian Edbrook-Childs, Emanuele M. Giusti, Gianluca Castelnuovo, and Giada Pietrabissa. 2021. Psychological support interventions for healthcare providers and informal caregivers during the COVID-19 pandemic: A systematic review of the literature. International Journal of Environmental Research and Public Health 18: 6939. [Google Scholar] [CrossRef]
- Books Beyond Words. 2020. Coping with Coronavirus. Available online: https://booksbeyondwords.co.uk/coping-with-coronavirus (accessed on 3 September 2021).
- Braun, Virginia, and Victoria Clarke. 2006. Using thematic analysis in psychology. Qualitative Research in Psychology 3: 77–101. [Google Scholar] [CrossRef] [Green Version]
- Budig, Kirsten, Julia Diez, Paloma Conde, Marta Sastre, Mariano Hernán, and Manuel Franc. 2018. Photovoice and empowerment: Evaluating the transformative potential of a participatory action research project. BMC Public Health 18: 432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christensen, Ann-Dorte, and Sune Qvotrup Jensen. 2012. Doing intersectional analysis: Methodological implications for qualitative research. NORA-Nordic Journal of Feminist and Gender Research 20: 109–25. [Google Scholar] [CrossRef]
- Courtenay, Ken, and Bhathika Perera. 2020. COVID-19 and People with Intellectual Disability: Impacts of a pandemic. Irish Journal of Psychological Medicine 37: 231–36. [Google Scholar] [CrossRef]
- Dean, Laura, Rachel Tolhurst, Renu Khanna, and Kate Jehan. 2017. ‘You’re disabled, why did you have sex in the first place?’ An intersectional analysis of experiences of disabled women with regard to their sexual and reproductive health and rights in Gujarat State, India. Global Health Action 10: 1290316. [Google Scholar] [CrossRef] [Green Version]
- Dean, Laura, Kerry A. Millington, Rachael Thomson, and Rachel Tolhurst. 2018. Shaping Health Systems to Include People with Disabilities. K4D Emerging Issues Report. Brighton: Institute of Development Studies. [Google Scholar]
- Durrell, Shirley. 2016. Research with and by people with learning disabilities. Nursing Times 112: 15–18. [Google Scholar]
- Emerson, Eric. 2011. Health status and health risks of the “hidden majority” of adults with intellectual disability. Intellectual and Developmental Disabilities 49: 155–65. [Google Scholar] [CrossRef]
- Goethals, Tina, Elisabeth De Schauwer, and Geert Van Hove. 2015. Weaving intersectionality into disability studies research: Inclusion, reflexivity and anti-essentialism. DiGeSt Journal of Diversity and Gender Studies 2: 75–94. [Google Scholar] [CrossRef]
- Goggin, Gerard, and Katie Ellis. 2021. Disability and Communication in the COVID-19 Pandemic. In Communicating COVID-19. Cham: Palgrave Macmillan, pp. 139–62. [Google Scholar]
- Grech, Shaun. 2016. Disability and Development: Critical Connections, Gaps and Contradictions. In Disability in the Global South. International Perspectives on Social Policy, Administration, and Practice. Edited by Shaun Grech and Karen Soldatic. Cham: Springer. [Google Scholar] [CrossRef]
- Green, Mark A., Clare R. Evans, and Subu V. Subramanian. 2017. Can intersectionality theory enrich population health research? Social Science & Medicine 178: 214–16. [Google Scholar]
- Hankivsky, Olena, and Anuj Kapilashrami. 2020. Beyond Sex and Gender Analysis: An Intersectional View of the COVID-19 Pandemic Outbreak and Response. Available online: https://www.qmul.ac.uk/gpi/media/global-policy-institute/Policy-brief-COVID-19-and-intersectionality.pdf (accessed on 3 September 2021).
- Hasan, Md Tanvir, Adity Shayontony Das, Adeepto Intisar Ahmed, Ahmed Mushtaque Raza Chowdhury, and Sabina Faiz Rashid. 2021. COVID-19 in Bangladesh: An especially difficult time for an invisible population. Disability & Society 36: 1362–67. [Google Scholar]
- International Labour Organisation (ILO). 2020. Disability Inclusion in the Bangladesh Skills System. Available online: https://www.ilo.org/wcmsp5/groups/public/---asia/---ro-bangkok/---ilo-dhaka/documents/publication/wcms_543298.pdf (accessed on 1 April 2020).
- Karuga, Robinson, Rosie Steege, Inviolata Njoroge, Millicent Liani, Neele Wiltgen Georgi, Lilian Otiso, Nelly Muturi, Linet Atieno Okoth, Sally Theobald, and Rachel Tolhurst. 2022. Leaving No One Behind: A Photovoice Case Study on Vulnerability and Wellbeing of Children Heading Households in Two Informal Settlements in Nairobi. Social Sciences 11: 296. [Google Scholar] [CrossRef]
- Kuper, Hannah, Shaffa Hameed, Veronika Reichenberger, Nathaniel Scherer, Jane Wilbur, Maria Zuurmond, Islay Mactaggart, Tess Bright, and Tom Shakespeare. 2021. Participatory Research in Disability in Low-and Middle-Income Countries: What have we Learnt and what Should we Do? Scandinavian Journal of Disability Research 23: 328–37. [Google Scholar] [CrossRef]
- Liegghio, Maria, and Lea Caragata. 2020. COVID-19 and youth living in poverty: The ethical considerations of moving from in-person interviews to a photovoice using remote methods. Affilia—Journal of Women and Social Work 36: 149–55. [Google Scholar] [CrossRef]
- Liberia Institute of Statistics and Geo-Information Services (LISGIS). 2017. 2017 Population and Housing Census: Final Results. Monrovia. Available online: https://ghdx.healthdata.org/record/liberia-household-income-and-expenditure-survey-2016-2017 (accessed on 3 September 2021).
- López, Cristina M., Suparna Qanungo, Carolyn M. Jenkins, and Ron Acierno. 2018. Technology as a Means to Address Disparities in Mental Health Research: A Guide to “Tele-Tailoring” your Research Methods. Professional Psychology: Research and Practice 49: 57–64. [Google Scholar] [CrossRef]
- Lund, Emily M., Anjali J. Forber-Pratt, Catherine Wilson, and Linda R. Mona. 2020. The COVID-19 pandemic, stress, and trauma in the disability community: A call to action. Rehabilitation Psychology 65: 313. [Google Scholar] [CrossRef]
- McCollum, Rosalind, Miriam Taegtmeyer, Lilian Otiso, Rachel Tolhurst, Maryline Mireku, Tim Martineau, Robinson Karuga, and Sally Theobald. 2019. Applying an intersectionality lens to examine health for vulnerable individuals following devolution in Kenya. International Journal for Equity in Health 18: 1–15. [Google Scholar] [CrossRef]
- Povee, Kate, Brian J. Bishop, and Lynne D. Roberts. 2014. The use of photovoice with people with intellectual disabilities: Reflections, challenges and opportunities. Disability & Society 29: 893–907. [Google Scholar]
- Rashid, Sabina Faiz, Bachera Aktar, Nadia Farnaz, Sally Theobald, Samiha Ali, Wafa Alam, and Kim Ozano. 2020. Fault-lines in the public health approach to COVID-19: Recognizing inequities and ground realities of poor residents lives in the slums of Dhaka City, Bangladesh. Social Sciences & Humanities Open. under review. [Google Scholar]
- Ritchie, Jane, and Liz Spencer. 2002. Qualitative data analysis for applied policy research. The Qualitative Researcher’s Companion 573: 305–29. [Google Scholar]
- Ronzi, Sara, Daniel Pope, Lois Orton, and Nigel Bruce. 2016. Using photovoice methods to explore older people’s perceptions of respect and social inclusion in cities: Opportunities, challenges and solutions. SSM-Population Health 2: 732–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronzi, Sara, Elisa Puzzolo, Lirije Hyseni, James Higgerson, Debbi Stanistreet, Mbatchou Ngahane Bertrand Hugo, Nigel Bruce, and Daniel Pope. 2019. Using photovoice methods as a community-based participatory research tool to advance uptake of clean cooking and improve health: The LPG adoption in Cameroon evaluation studies. Social Science & Medicine 228: 30–40. [Google Scholar]
- Ryan, Frances. 2020. Coronavirus Hits Ill and Disabled People Hardest, So Why Is Society Writing Us Off? The Guardian. Available online: https://www.theguardian.com/commentisfree/2020/mar/11/coronavirus-illdisabled-people (accessed on 3 September 2021).
- Swanwick, Ruth, Alexander M. Oppong, Yaw N. Offei, Daniel Fobi, Obed Appau, Joyce Fobi, and F. Frempomaa Mantey. 2020. The impact of the COVID-19 pandemic on deaf adults, children and their families in Ghana. Journal of the British Academy 8: 141–65. [Google Scholar] [CrossRef]
- Terras, Melody M., and Dominic Jarrett. 2021. Accessible information isn’t easy: Shifting practice and production perspectives of information accessibility. Global Journal of Intellectual and Developmental Disabilites 9: 1–3. [Google Scholar]
- Tolhurst, Rachel, Beryl Leach, Janet Price, Jude Robinson, Elizabeth Ettore, Alex Scott-Samuel, Nduku Kilonzo, Louis P. Sabuni, Steve Robertson, Anuj Kapilashrami, and et al. 2012. Intersectionality and gender mainstreaming in international health: Using a feminist participatory action research process to analyse voices and debates from the global south and north. Social Science & Medicine 74: 1825–32. [Google Scholar]
- Torres, E. 2020. Social Distancing ‘Not Possible’ for People with Disabilities, Raising Challenges. Available online: https://abcnews.go.com/Health/social-distancing-people-disabilities-raising-challenges/story?id=69486075 (accessed on 3 March 2022).
- Tuffrey-Wijne, Irene, Lucy Goulding, Nikoletta Giatras, Elisabeth Abraham, Steve Gillard, Sarah White, Christine Edwards, and Sheila Hollins. 2014. The barriers to and enablers of providing reasonably adjusted health services to people with intellectual disabilities in acute hospitals: Evidence from a mixed-methods study. BMJ Open 4: e004606. [Google Scholar] [CrossRef] [Green Version]
- United Nations. 2019. The Sustainable Development Agenda. Available online: https://www.un.org/sustainabledevelopment/development-agenda/ (accessed on 1 February 2022).
- Wang, Caroline, and Mary Ann Burris. 1997. Photovoice: Concept, methodology, and use for participatory needs assessment. Health Education & Behavior 24: 369–87. [Google Scholar]
- Zaagsma, Miriam, Karin M. Volkers, Eline A. K. Swart, Alice P. Schippers, and Geert Van Hove. 2020. The use of online support by people with intellectual disabilities living independently during COVID-19. Journal of Intellectual Disability Research 64: 750–56. [Google Scholar] [CrossRef]




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Co-Researcher Name | Gender | Type of Impairment/Caregiver | Age | Socioeconomic Status | Location |
|---|---|---|---|---|---|
| Liberia | |||||
| Heylove R. Mark Sr | Male | Physical impairment | 25–49 years | Middle-income family | Monrovia, Montserrado County |
| Boakai A. Nyehn Jr | Male | Physical impairment | 25–49 years | Middle-income family | Monrovia, Montserrado County |
| Francis C. Sibley | Male | Visual impairment | 25–49 years | Middle-income family | Monrovia, Montserrado County |
| Jochebad Morweh | Female | Physical impairment | 25–49 years | Middle-income family | Monrovia, Montserrado County |
| Benjamin Ballah | Male | Psychosocial impairment | 25–49 years | Middle-income family | Monrovia, Montserrado County |
| Sadiatu Kamara | Female | Physical impairment | 25–49 years | Middle-income family | Monrovia, Montserrado County |
| Rose Dargbe | Female | Physical impairment | 25–49 years | Middle-income family | Monrovia, Montserrado County |
| Patience Duonnah | Female | Hearing impairment | 25–49 years | Middle-income family | Monrovia, Montserrado County |
| David Hne Wallace | Male | Physical and psychosocial impairment | Over 49 years | Lower-income family | Monrovia, Montserrado County |
| Susan K.C. Nyehn | Female | Caregiver of Boakai, husband with physical impairment | 25–49 years | Middle-income family | Monrovia, Montserrado County |
| Eric Solomon Biawogee | Male | Caregiver of best friend with physical impairment | 25–49 years | Middle-income family | Monrovia, Montserrado County |
| Jonathan Corlon | Male | Caregiver of relative with physical impairment | 25–49 years | Middle-income family | Monrovia, Montserrado County |
| Janet M. Kai | Female | Caregiver of Heylove, partner with physical impairment | 25–49 years | Middle-income family | Monrovia, Montserrado County |
| Bangladesh | |||||
| Ashraful Alam | Male | Physical impairment | 25–49 years | Middle-income family | Dhaka District, Dhaka Division |
| Marjana Binte Forhad | Female | Physical impairment | 18–24 years | Middle-income family | Faridpur District, Dhaka Division |
| Ataur Islam | Male | Physical impairment | 25–49 years | Middle-income family | Narayanganj District, Dhaka Division |
| Delowar Hossain | Male | Physical impairment | 25–49 years | Lower-income family | Khulna District, Kulna Division |
| Halima Akter | Female | Physical impairment | 18–24 years | Middle-income family | Dhaka District, Dhaka Division |
| Shomoy Chowdhury | Male | Physical impairment | 25–49 years | Higher-income family | Dhaka District, Dhaka Division |
| Saddam Hossian | Male | Physical impairment | 25–49 years | Lower-income family | Manikganj, Dhaka Division |
| Sonia Akter | Female | Caregiver of son with cerebral palsy | 25–49 years | Middle-income family | Dhaka District, Dhaka Division |
| Fatema Rahman Sumi | Female | Caregiver of sister-in-law with psychosocial impairment | 25–49 years | Higher-income family | Dhaka District, Dhaka Division |
| Mehedi Hasan Bokul | Male | Caregiver of brother with hearing and speech impairment | 25–49 years | Middle-income family | Dhaka District, Dhaka Division |
| Bisshojit | Male | Caregiver of sister with psychosocial impairment | 25–49 years | Lower-income family | Khulna District, Kulna Division |
| Nasrin Begum | Female | Caregiver of son with psychosocial impairment | 25–49 years | Middle-income family | Dhaka District, Dhaka Division |
| Bithi Akter | Female | Caregiver of son with cerebral palsy | 25–49 years | Middle-income family | Dhaka District, Dhaka Division |
| Israt Jahan Isha | Female | Caregiver of Marjana, sister with physical impairment | 18–24 years | Middle-income family | Faridpur District, Dhaka Division |
| Themes | Sub-Themes |
|---|---|
| Social connection |
|
| Accessibility and awareness |
|
| Impact on livelihoods |
|
| Gendered impacts |
|
| Adaptability and technology |
|
| Faith and Nature |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chowdhury, S.; Urme, S.A.; Nyehn, B.A., Jr.; Mark, H.R., Sr.; Hassan, M.T.; Rashid, S.F.; Harris, N.B.; Dean, L. Pandemic Portraits—An Intersectional Analysis of the Experiences of People with Disabilities and Caregivers during COVID-19 in Bangladesh and Liberia. Soc. Sci. 2022, 11, 378. https://doi.org/10.3390/socsci11090378
Chowdhury S, Urme SA, Nyehn BA Jr., Mark HR Sr., Hassan MT, Rashid SF, Harris NB, Dean L. Pandemic Portraits—An Intersectional Analysis of the Experiences of People with Disabilities and Caregivers during COVID-19 in Bangladesh and Liberia. Social Sciences. 2022; 11(9):378. https://doi.org/10.3390/socsci11090378
Chicago/Turabian StyleChowdhury, Shahreen, Salma Akter Urme, Boakai A. Nyehn, Jr., Heylove R. Mark, Sr., Md. Tanvir Hassan, Sabina F. Rashid, Naomi B. Harris, and Laura Dean. 2022. "Pandemic Portraits—An Intersectional Analysis of the Experiences of People with Disabilities and Caregivers during COVID-19 in Bangladesh and Liberia" Social Sciences 11, no. 9: 378. https://doi.org/10.3390/socsci11090378