
Gender and Place of Settlement as Predictors of Perceived Social Support, PTSD, and Insomnia among Internally Displaced Adolescents in North-East Nigeria


Abstract
:1. Introduction
1.1. Gender
1.2. Place of Settlement
1.3. Social Support
1.4. Interaction Effects
2. The Present Study
3. Materials and Methods
3.1. Participants and Sampling Strategy
3.1.1. Data Collection Procedure from the Camp
3.1.2. Data Collection Procedure in the Host Community
3.2. Measures
4. Data Analysis
5. Results
5.1. Mean Scores across Gender and Place of Settlement
5.2. Main and Interaction Effects of Gender and Place of Settlement on Social Support, Insomnia, and PTSD Symptoms
6. Discussion
6.1. Gender Main Effects
6.2. Place of Settlement Main Effects
6.3. Interaction Effects
6.4. Limitations and Future Research Suggestions
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ainamani, Herbert E., Thomas Elbert, D. Kani Olema, and Tobias Hecker. 2020. Gender differences in response to war-related trauma and posttraumatic stress disorder—A study among the Congolese refugees in Uganda. BMC Psychiatry 20: 1–9. [Google Scholar] [CrossRef] [Green Version]
- Akiyama, Takeshi, Thar Win, Cynthia Maung, Paw Ray, Kayako Sakisaka, Aya Tanabe, Jun Kobayashi, and Masamine Jimba. 2013. Mental health status among Burmese adolescent students living in boarding houses in Thailand: A cross-sectional study. Journal of Bio-Medical Central Public Health 13: 337. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association (APA). 2013. Diagnostic and Statistical Manuel of Mental Disorders, 5th ed. Washington, DC and Arlington: American Psychiatric Association. [Google Scholar]
- Araya, Mesfin, Jayanti Chotai, Ivan H. Komproe, and J. T. V. M. de Jong. 2007. Gender differences in traumatic life events, coping strategies, perceived social support and socio-demographics among post-conflict displaced persons in Ethiopia. Social Psychiatry and Psychiatric Epidemiology 42: 307–15. [Google Scholar] [CrossRef]
- Ayazi, Touraj, Lars Lien, Arne Eide, Leslie Swartz, and Edward Hauff. 2014. Association between exposure to traumatic events and anxiety disorders in a post-conflict setting: A cross-sectional community study in South Sudan. BMC Psychiatry 14: 1–10. [Google Scholar] [CrossRef] [Green Version]
- Barrera, M., Jr. 2000. Social support research in community psychology. In The Handbook of Community Psychology. Edited by Julian Rappaport and Edward Seidman. New York: Kluwer Academic/Plenum Publishers, pp. 215–45. [Google Scholar]
- Basishvili, Tamar, Marine Eliozishvili, Lia Maisuradze, Nani Lortkipanidze, Nargiz Nachkebia, Tengiz Oniani, Irma Gvilia, and Nato Darchia. 2012. Insomnia in a displaced population is related to war-associated remembered stress. Stress Health 28: 186–92. [Google Scholar] [CrossRef]
- Bastien, Célyne H., Annie Vallières, and Charles M. Morin. 2001. Validation of the insomnia severity index (ISI) as an outcome measure for insomnia research. Sleep Medicine 2: 297–307. [Google Scholar] [CrossRef]
- Betancourt, Theresa S., Carmal Salhi, Stephen Buka, Jennifer Leaning, Gillian Dunn, and Felton Earls. 2012. Connectedness, social support and internalizing emotional and behavioural problems in adolescents displaced by the Chechen conflict. National Institutes of Health 36: 635–55. [Google Scholar] [CrossRef] [Green Version]
- Blais, France C., Linda Gendron, Véronique Mimeault, and Charles M. Morin. 1997. Evaluation de l’insomnie: Validation de trois questionnaires. Encephale 23: 447–53. [Google Scholar] [PubMed]
- Bronstein, Israel, and Paul Montgomery. 2011. Psychological distress in refugee children: A systematic review. Clinical Child Family and Psychological Review 14: 44–56. [Google Scholar] [CrossRef] [PubMed]
- Bruck, Dorothy, S. Atem Deng, Bichok Kot, and Michele Grossman. 2020. Sleep difficulties among South Sudanese former refugees settled in Australia. Transcultural Psychiatry 58: 172–86. [Google Scholar] [CrossRef]
- Cairo, Javier B., Suparna Dutta, Haq Nawaz, Shahrukh Hashmi, Stanislav Kasl, and Edgar Bellido. 2010. The prevalence of posttraumatic stress disorder among adult earthquake survivors in Peru. Disaster Medicine and Public Health Preparedness 4: 39–46. [Google Scholar] [CrossRef]
- Charak, Ruby, Cherie Armour, Ask Elklit, Disket Angmo, Jon D. Elhai, and Hans M. Koot. 2014. Factor structure of PTSD, and relation with gender in trauma survivors from India. European Journal of Psychotraumatology 5: 25547. [Google Scholar] [CrossRef]
- Chung, Ka-Fai, Katherine K. Kan, and Wing-Fai Yeung. 2011. Assessing insomnia in adolescents: Comparison of insomnia severity index, Athens insomnia scale and Sleep quality index. Sleep Medicine 12: 463–70. [Google Scholar] [CrossRef]
- De Jong, Joop T. V. M., Ivan H. Komproe, Mark Van Ommeren, Mustafa El Masri, Mesfin Araya, Noureddine Khaled, Willem van de Put, and Daya Somasundaram. 2001. Lifetime events and posttraumatic stress disorder in 4 post conflict settings. Journal of American Medical Association 286: 555–62. [Google Scholar] [CrossRef]
- DeLong, Hannah. 2012. Social Support in PTSD: An analysis of gender, race, and trauma type. Discussions 8: 1–3. [Google Scholar]
- Ditlevsen, Daniel N., and Ask Elklit. 2010. The combined effect of gender and age on posttraumatic stress disorder: Do men and women show differences in the lifespan distribution of PTSD? Annals of General Psychiatry 9: 44–59. [Google Scholar] [CrossRef] [Green Version]
- Elbedour, Salman, Anthony J. Onwuegbuzie, Jess Ghannam, Janine A. Whitcome, and F. Abu Hein. 2007. Post-traumatic stress disorder, depression, and anxiety among Gaza Strip adolescents in the wake of the second uprising (Intifada). Journal of Child Abuse and Neglect 31: 719–29. [Google Scholar] [CrossRef] [PubMed]
- Elklit, Ask, Kjaer K. Ostergard, Mathias Lasgaard, and Sabina Palic. 2012. Social support, coping and posttraumatic stress symptoms in young refugees. Journal of Torture 22: 11–23. [Google Scholar] [PubMed]
- Ellis, B. Heidi, Helen Z. MacDonald, Alisa K. Lincoln, and Howard J. Cabral. 2008. Mental health of Somali adolescent refugees: The role of trauma, stress, and perceived discrimination. Journal of Consulting Clinical Psychology 76: 184–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farhood, Laila F., and Hani Dimassi. 2012. Prevalence and predictors for posttraumatic stress disorder, depression and general health in a population from six villages in South Lebanon. Social Psychiatry Epidemiology 47: 639–49. [Google Scholar] [CrossRef]
- Field, Andy. 2009. Discovering Statistics Using SPSS. London: Sage Publications. [Google Scholar]
- Finch, Holmes, and Brian French. 2013. A Monte Carlo comparison of robust MANOVA test statistics. Journal of Modern Applied Statistical Methods 12: 35–81. [Google Scholar] [CrossRef] [Green Version]
- Frans, Örjan, Per-Arne Rimmö, Lars Aberg, and Mats Fredrikson. 2005. Trauma exposure and post-traumatic stress disorder in the general population. Acta Psychiatry Scandinavian 111: 291–99. [Google Scholar] [CrossRef] [PubMed]
- Hamid, Abdalla R. M. A., and Saif A. Musa. 2010. Mental health problems among internally displaced persons in Darfur. International Journal of Psychology 45: 278–85. [Google Scholar] [CrossRef]
- IASC. 1993. Inter-Agency Standing Committee. In Proceedings of the 7th Working Group Meeting, Internally Displaced Persons Outside Camps: Achieving a More Equitable Humanitarian Response; Available online: https://reliefweb.int/report/world/under-radar-internally-displaced-persons-non-camp-settings (accessed on 12 April 2021).
- Idemudia, Erhabor S., John K. William, Klaus Boehnke, and Gail Wyatt. 2013. Gender differences in trauma and posttraumatic stress symptoms among displaced Zimbabweans in South Africa. Journal of Trauma Stress Disorder Treatment 2: 1340. [Google Scholar] [CrossRef]
- IDMC. 2008. Internal displacement Monitoring Centre. Profiling Studies on IDPs in Urban Areas: Internal Displacement to Urban Areas: Khartoum, Sudan. September. Available online: http://sites.tufts.edu/feinstein/research/research-by-topic/internally-displaced-persons?submit=Go (accessed on 20 May 2021).
- IDMC. 2011. Internal displacement Monitoring Centre. Internal Displacement: Global Overview of Trends and Developments in 2010. Available online: www.internal-displacement.org/31FFB20A-37C4-4D48-85D1-4BC7B5C73277 (accessed on 19 June 2021).
- IOM. 2018. International Organization for Migration. Displacement Tracking Matrix, Round 23 Report—June 2018. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/Nigeria%20-%20.pdf (accessed on 12 April 2021).
- IOM. 2021. International Organization for Migration. Displacement Tracking Matrix (DTM) of Nigeria North-East Zone Displacement Report Round 37 (August 2021). Available online: https://displacement.iom.int/system/tdf/reports/DTM%20Report%20Round%2037%20%20NE.pdf?file=1&type=node&id=12093 (accessed on 8 October 2021).
- IRIN. 2013. Integrated Regional Information Network. With regard to Pakistan: How Best to Serve Pakistan’s 750,000 IDPs? Available online: www.irinnews.org (accessed on 10 April 2021).
- Jenchura, Emily C., Nancy A. Gonzales, Jenn-Yun Tein, and Linda J. Luecken. 2017. Gender and the Interplay of Source of Support and Peer Social Rejection on Internalizing Among Mexican American Youth. Journal of Youth and Adolescence 46: 787–800. [Google Scholar] [CrossRef]
- Johansen, Venke A., Astrid K. Wahl, Dag E. Eilertsen, and Lars Weisaeth. 2007. Prevalence and predictors of post-traumatic stress disorder (PTSD) in physically injured victims of non-domestic violence. A longitudinal study. Social Psychiatry Epidemiology 42: 583–93. [Google Scholar] [CrossRef]
- John, Prashantham B., Sushila Russell, and Paul S. S. Russell. 2007. The prevalence of posttraumatic stress disorder among children and adolescents affected by Tsunami disaster in Tamil Nadu. Disaster Management Response 5: 3–7. [Google Scholar] [CrossRef]
- Joseph, Steve, Bernice Andrews, Ruth Williams, and William Yule. 1992. Crisis support and psychiatric symptomatology in adult survivors of the Jupiter cruise ship disaster. British Journal of Clinical Psychology 31: 63–73. [Google Scholar] [CrossRef]
- Kamungi, Prisca. 2013. Municipal and IDPs Outside of Camps: The Case of Kenya’s Integrated Displaced Persons, Brookings-LSE Project on Internal Displacement. Available online: http://www.brookings.edu/research/reports/2013/05/kenya-displacement-kamungi (accessed on 11 April 2021).
- Kessler, Ronald C., Amanda Sonnega, Evelyn Bromet, Michael Hughes, and Christopher B. Nelson. 1995. Posttraumatic stress disorder in the national comorbidity survey. Archives of General Psychiatry 52: 1048–60. [Google Scholar] [CrossRef] [PubMed]
- Kolakowsky-Hayner, Stephanie A., Yelena Goldin, Kristine Kingsley, Elisabet Alzueta, Juan C. Arango-Lasprilla, Paul B. Perrin, Fiona C. Baker, Daniela Ramos-Usuga, and Fofi Constantinidou. 2021. Psychosocial Impacts of the COVID-19 Quarantine: A Study of Gender Differences in 59 Countries. Medicina 57: 789. [Google Scholar] [CrossRef] [PubMed]
- Kubzansky, Laura D., Paula Bordelois, H. Jin Jun, Andrea L. Roberts, Magdalena Cerda, Noah Bluestone, and Karestan C. Koenen. 2014. The weight of traumatic stress: A prospective study of posttraumatic stress disorder symptoms and weight status in women. JAMA Psychiatry 71: 4451. [Google Scholar] [CrossRef]
- Kumar, M. Suresh, Manoj V. Murhekar, Yvan Hutin, Thilakavathi Subramanian, Vidya Ramachandran, and Mohan D. Gupte. 2007. Prevalence of posttraumatic stress disorder in coastal fishing village in Tamil Nadu, India, after the December 2004 Tsunami. American Journal of Public Health 97: 99–101. [Google Scholar] [CrossRef]
- Kunovich, Robert M. 1999. Civil war, social integration and mental health in Croatia. Journal of Health and Social Behavour 40: 323–43. [Google Scholar] [CrossRef]
- Lee, Yu-Jin G., Jin Yong Jun, Yu Jin Lee, Juhyun Park, Soohyun Kim, So Hee Lee, So Young Yu, and Seog Ju Kim. 2016. Insomnia in North Korean refugees: Association with depression and post-traumatic stress symptoms. Psychiatry Investigation 13: 67–73. [Google Scholar] [CrossRef]
- Lee, Chih-Yuan S., and Sara E. Goldstein. 2016. Loneliness, stress, and social support in young adulthood: Does the source of support matter? Journal of Youth and Adolescence 45: 568–80. [Google Scholar] [CrossRef]
- Lies, July, Laura Jobson, Luis Mascaro, Theoni Whyman, and Sean P. A. Drummond. 2021. Postmigration stress and sleep disturbances mediate the relationship between trauma exposure and posttraumatic stress symptoms among Syrian and Iraqi refugees. Journal of Clinical Sleep Medicine 17: 479–89. [Google Scholar] [CrossRef] [PubMed]
- Llabre, Maria M., and Foaziah Hadi. 1997. Social support and psychological distress in Kuwaiti boys and girls exposed to the gulf crisis. Journal of Clinical Child Psychology 26: 247–55. [Google Scholar] [CrossRef]
- López-Torres Hidalgo, J., B. Navarro Bravo, I. Párraga Martínez, F. Andrés Pretel, J. Téllez Lapeira, and C. Boix Gras. 2012. Understanding insomnia in older adults. Intern Journal Geriatrics Psychiatry 27: 1086–93. [Google Scholar] [CrossRef] [PubMed]
- Mallampalli, Monica P., and Christine L. Carter. 2014. Exploring sex and gender differences in sleep health: A society for women’s health research report. Journal of Women’s Health Larchmt 23: 553–62. [Google Scholar] [CrossRef] [Green Version]
- Mels, Cind, Ilsa Derluyn, Eric Broekaert, and Yves Rosseel. 2010. The psychological impact of forced displacement and related risk factors on Eastern Congolese adolescents affected by war. Journal of Child Psychology and Psychiatry 5: 1096–104. [Google Scholar] [CrossRef] [PubMed]
- Mollica, Richard F., Yael Caspi-Yavin, Paola Bollini, Toan Truong, Svang Tor, and James Lavelle. 1992. Harvard trauma questionnaire. Validating a cross-cultural instrument for measuring torture, trauma, and posttraumatic stress disorder in Indochinese refugees. Journal of Nervous and Mental Disorders 180: 111–16. [Google Scholar] [CrossRef]
- Morin, Charles M. 1993. Insomnia: Psychological Assessments and Management. New York: The Guilford Press. [Google Scholar]
- Nader, Kathleen O., Robert S. Pynoos, Lynn A. Fairbanks, Manal Al-Ajeel, and Abdulrahman Al-Asfour. 1993. A preliminary study of PTSD and grief among the children of Kuwait following the Gulf crisis. British Journal of Clinical Psychology 32: 407–16. [Google Scholar] [CrossRef]
- Ogundele, Adefolakemi, Maroh Ighoroje, and Olukayode Abayomi. 2017. Insomnia and dysfunctional beliefs and attitudes about sleep among elderly persons in Abeokuta, Nigeria. International Journal of Clinical Psychiatry 5: 25–31. [Google Scholar] [CrossRef]
- Olff, Miranda. 2017. Sex and gender differences in post-traumatic stress disorder: An update. European of Journal Psychotraumatology 8: 1–2. [Google Scholar] [CrossRef]
- Olff, Miranda, Willie Langeland, Nel Draijer, and Berthold P. R. Gersons. 2007. Gender differences in posttraumatic stress disorder. Psychological Bulletin 133: 183–204. [Google Scholar] [CrossRef] [PubMed]
- Pettus-Davis, Carrie, Christopher A. Veeh, Maxine Davis, and Stephen Tripodi. 2018. Gender Differences in Experiences of Social Support among Men and Women Releasing from Prison. Journal of Social and Personal Relationships 35: 1161–82. [Google Scholar] [CrossRef]
- Pillai, Sreedharan K. C. 1955. Some new test criteria in multivariate analysis. Annual Mathematic Statistic 26: 117–21. [Google Scholar] [CrossRef]
- Polyné, Nina C., Katherine E. Miller, Janeese Brownlow, and Philip R. Gehrman. 2021. Insomnia: Sex differences and age of onset in active duty Army soldiers. Sleep Health 7: 504–7. [Google Scholar] [CrossRef] [PubMed]
- Raji, Shittu, Arinola F. Adekayaoja, E. Ayila Agaku, James Akujobi, and Ayinde Hamzat. 2021. North-eastern Nigeria: Assessing the response capacity of National Emergency Management Agency to the plights of internally displaced persons. Heliyon 7: e07274. [Google Scholar] [CrossRef]
- Rothe, Eugenio M., John Lewis, Hector Castillo-Matos, Orestes Martinez, Ruben Busquets, and Igna Martinez. 2002. Posttraumatic stress disorder among Cuban children and adolescents after release from a refugee camp. Psychiatric Service 53: 970–76. [Google Scholar] [CrossRef]
- Ruth, Abiola A., and Ignatius N. Ijere. 2018. Psycho-social traumatic events among women in Nigeria. Madridge Journal of AIDS 1: 17–28. [Google Scholar] [CrossRef] [Green Version]
- Schraedley, Pamela K., Ian H. Gotlib, and Chris Hayward. 1999. Gender differences in correlates of depressive symptoms in adolescents. Journal of Adolescence Health 25: 98–108. [Google Scholar] [CrossRef]
- Seelig, Amber D., Isabel G. Jacobson, Besa Smith, Tomoko I. Hooper, Edward J. Boyko, Gary D. Gackstetter, Philip Gehrman, Carol A. Macera, and Tyler C. Smith. 2010. Sleep patterns before, during, and after deployment to Iraq and Afghanistan. Sleep 33: 1615–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheikh, Taiwo L., Abdulaziz Mohammed, Edwin Eseigbe, Tosin Adekeye, Folorunsho T. Nuhu, Modupe Lasisi, Abdulaziz Muhammad, Zainab T. Sulaiman, Aishatu A. Abdullateef, Nafisatu Hayyatudeen, and et al. 2016. Descriptive characterization of psycho-trauma, psychological distress, and post-traumatic stress disorder among children and adolescent internally displaced persons in Kaduna, Nigeria. Front in Psychiatry 7: 179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steel, Zachary, Tien Chey, Derrick Silove, Claire Marnane, Richard A. Bryant, and Ommeren van Mark. 2009. Association of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and displacement: A systematic review and meta-analysis. Journal of American Medical Association 302: 537–49. [Google Scholar] [CrossRef] [PubMed]
- Stupar, Dusko, Dejan Stevanovic, Panos Vostanis, Olayinka Atilola, Paulo Moreira, Katerina Dodig-Curkovic, Tomislay Franic, Ana Doric, Nikolina Davidovic, Mohamad Avicenna, and et al. 2021. Posttraumatic stress disorder symptoms among trauma-exposed adolescents from low- and middle-income countries. Child Adolesc Psychiatry Ment Health 15: 1–10. [Google Scholar] [CrossRef] [PubMed]
- Tabachnick, Barbara G., and Linda S. Fidell. 1983. Using Multivariate Statistics. New York: Harper and Row. [Google Scholar]
- Taha, Perjan H., and Marit Sijbrandij. 2021. Gender Differences in Traumatic Experiences, PTSD, and Relevant Symptoms among the Iraqi Internally Displaced Persons. International Journal of Environmental Research and Public Health 18: 9779. [Google Scholar] [CrossRef]
- Thabet, Abdelaziz M., and Sanaa S. Thabet. 2017. Stress, trauma and post-traumatic stress disorder among adolescents in the Gaza strip. Journal of Trauma Critical Care 1: 25–33. [Google Scholar]
- Thoits, Peggy A. 2011. Mechanisms linking socialites and support to physical and mental health. Journal of Health Social Behavour 52: 145–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Droogenbroeck, Filip, Bram Spruyt, and Gil Keppens. 2018. Gender differences in mental health problems among adolescents and the role of social support: Results from the Belgian health interview surveys 2008 and 2013. Bio-Medical Central Psychiatry 18: 6–10. [Google Scholar] [CrossRef] [Green Version]
- WCRWC. 2006. Women’s Commission for Refugee Women and Children. Displaced Women and Girls at Risk: Risk Factors, Protection Solutions and Resource Tools. Available online: https://www.womensrefugeecommission.org/images/stories/WomRisk.pdf (accessed on 10 April 2021).
- WHO. 1989. The Health of Youth. (Background Document A42/Technical Discussions/2), Geneva. Available online: https://apps.who.int/iris/handle/10665/172242 (accessed on 10 April 2021).
- WHO. 2004. World Health Organization. Gender in Mental Health Research. Department of Gender, Women and Health (GWH) world Health Organization. Available online: http://apps.who.int/iris/bitstream/handle10665/43084/9241592532.pdf (accessed on 10 April 2021).
- WHO and CGF. 2014. World Health Organization and Calouste Gulbenkian Foundation. In Social Determinants of Mental Health. Geneva: World Health Organization, Available online: http://apps.who.int/iris/bitstream/handle/10665/112828/9789241506809eng.pdf (accessed on 10 April 2021).
- Yasan, Aziz, Gunay Saka, Mustafa Ozkan, and Meliksah Ertem. 2009. Trauma type, gender, and risk of PTSD in a region within an area of conflict. Journal of Trauma and Stress 22: 663–66. [Google Scholar] [CrossRef] [PubMed]
- Yatham, Swetha, Shalini Sivathasan, Rosalia Yoon, Tricia L. da Silva, and Arun V. Ravindran. 2018. Depression, anxiety, and post-traumatic stress disorder among youth in low- and middle-income countries: A review of prevalence and treatment interventions. Asian J Psychiatr 38: 78–91. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Liang-Nan, Qian-Qian Zong, Yuan Yang, Ling Zhang, Yi-Fan Xiang, Chee H. Ng, Li-Gang Chen, and Yu-Tao Xiang. 2020. Gender Difference in the Prevalence of Insomnia: A Meta-Analysis of Observational Studies. Frontiers in Psychiatry 11: 1162. [Google Scholar] [CrossRef]
- Zhang, Bin I., and Yun-Kwork Wing. 2006. Sex differences in insomnia: A meta-analysis. Journal of Sleep 29: 85–93. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | N | % |
|---|---|---|
| Age Group | ||
| Younger adolescent | 38 | 27.9 |
| Older adolescent | 98 | 72.1 |
| Gender | ||
| Male | 54 | 39.7 |
| Female | 82 | 60.3 |
| Religion | ||
| None | 1 | 0.7 |
| Christianity | 126 | 92.7 |
| Islam | 9 | 6.6 |
| Marital status | ||
| Single | 74 | 54.4 |
| Married | 58 | 42.6 |
| Widowed | 4 | 2.9 |
| Educational level | ||
| Non formal | 51 | 37.5 |
| Primary | 66 | 48.5 |
| Secondary | 17 | 12.5 |
| Tertiary | 2 | 1.5 |
| Occupational status | ||
| Unemployed | 73 | 53.7 |
| Self-employed | 21 | 15.4 |
| Student | 36 | 26.5 |
| Farming | 6 | 4.4 |
| Place of Settlements | ||
| Camp | 109 | 80.1 |
| Host community | 27 | 19.9 |
| Dependent Variable | Independent Variable | Mean | SE |
|---|---|---|---|
| PSS | Male | 31.06 | 1.30 |
| Female | 31.32 | 1.07 | |
| PTSD | Male | 48.26 | 1.82 |
| Female | 45.91 | 1.50 | |
| Insomnia | Male | 15.54 | 1.08 |
| Female | 14.12 | 0.89 | |
| PSS | Camp | 33.50 | 0.75 |
| Community | 28.88 | 1.50 | |
| PTSD | Camp | 45.70 | 1.05 |
| Community | 48.47 | 2.12 | |
| Insomnia | Camp | 13.90 | 0.63 |
| Community | 15.76 | 1.25 | |
| PSS | Male in Camp | 32.67 | 1.17 |
| Male in Community | 29.46 | 2.31 | |
| Female in Camp | 34.32 | 0.94 | |
| Female in Community | 28.31 | 1.92 | |
| PTSD | Male in Camp | 45.88 | 1.64 |
| Male in Community | 50.64 | 3.24 | |
| Female in Camp | 45.52 | 1.32 | |
| Female in Community | 46.31 | 2.69 | |
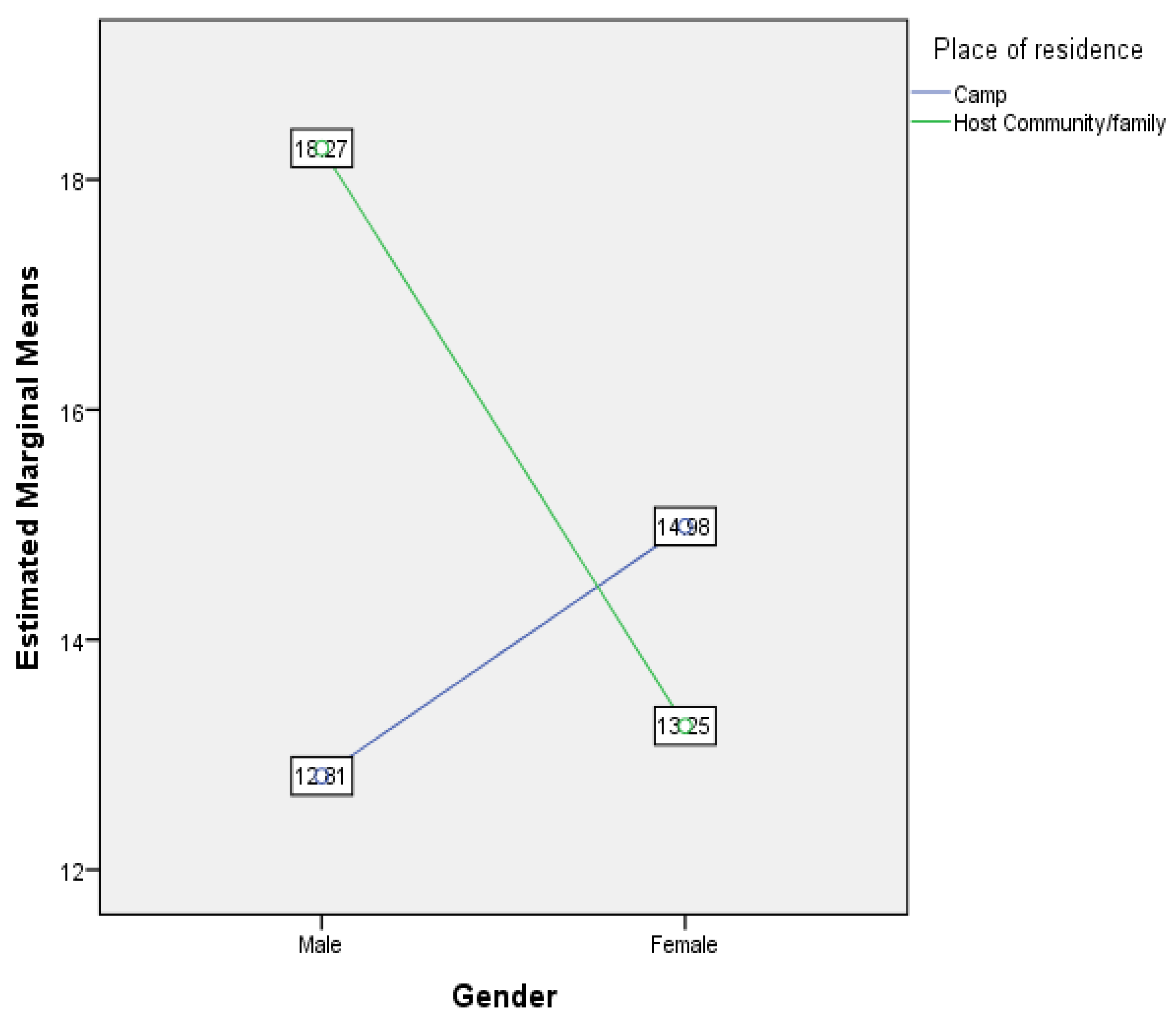
| Insomnia | Male in Camp | 12.81 | 0.97 |
| Male in Community | 18.27 | 1.92 | |
| Female in Camp | 14.99 | 0.79 | |
| Female in Community | 13.25 | 1.60 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
David, O.P.; Dammeyer, J.; Yakubu, I. Gender and Place of Settlement as Predictors of Perceived Social Support, PTSD, and Insomnia among Internally Displaced Adolescents in North-East Nigeria. Soc. Sci. 2021, 10, 428. https://doi.org/10.3390/socsci10110428
David OP, Dammeyer J, Yakubu I. Gender and Place of Settlement as Predictors of Perceived Social Support, PTSD, and Insomnia among Internally Displaced Adolescents in North-East Nigeria. Social Sciences. 2021; 10(11):428. https://doi.org/10.3390/socsci10110428
Chicago/Turabian StyleDavid, Onyekachi Prince, Jesper Dammeyer, and Ismaila Yakubu. 2021. "Gender and Place of Settlement as Predictors of Perceived Social Support, PTSD, and Insomnia among Internally Displaced Adolescents in North-East Nigeria" Social Sciences 10, no. 11: 428. https://doi.org/10.3390/socsci10110428