
21-Day Stress Detox: Open Trial of a Universal Well-Being Chatbot for Young Adults

 and
and
Abstract
:1. Introduction
Rationale for the Current Study
2. Materials and Methods
2.1. Study Design
2.1.1. Recruitment
2.1.2. Procedure
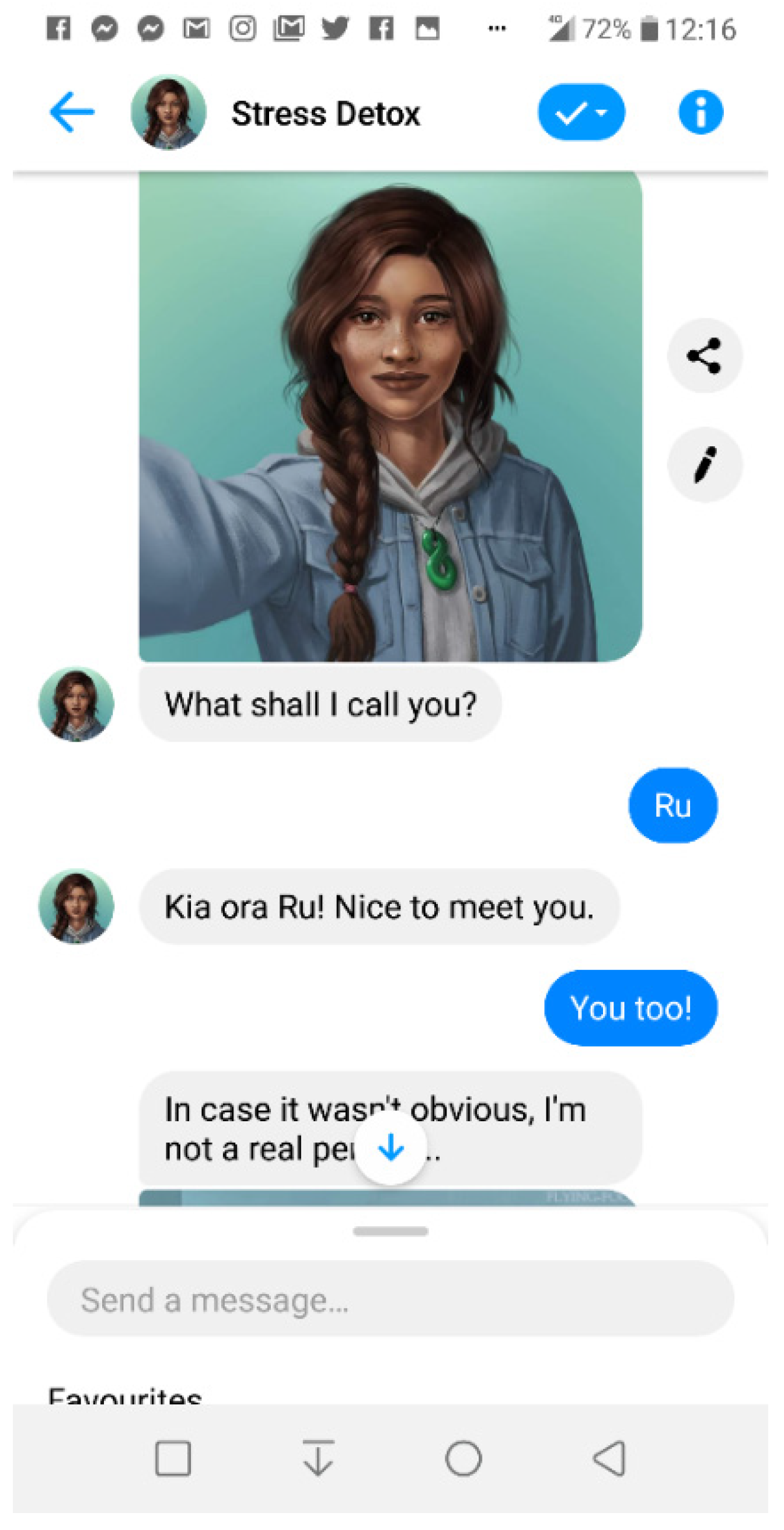
2.1.3. Intervention
 ); week two focused on cognitive appraisal of stress and anxiety (i.e., thinking–represented in the chatbot as
); week two focused on cognitive appraisal of stress and anxiety (i.e., thinking–represented in the chatbot as  ); and week three focused on behavioural response (i.e., action–represented in the chatbot as
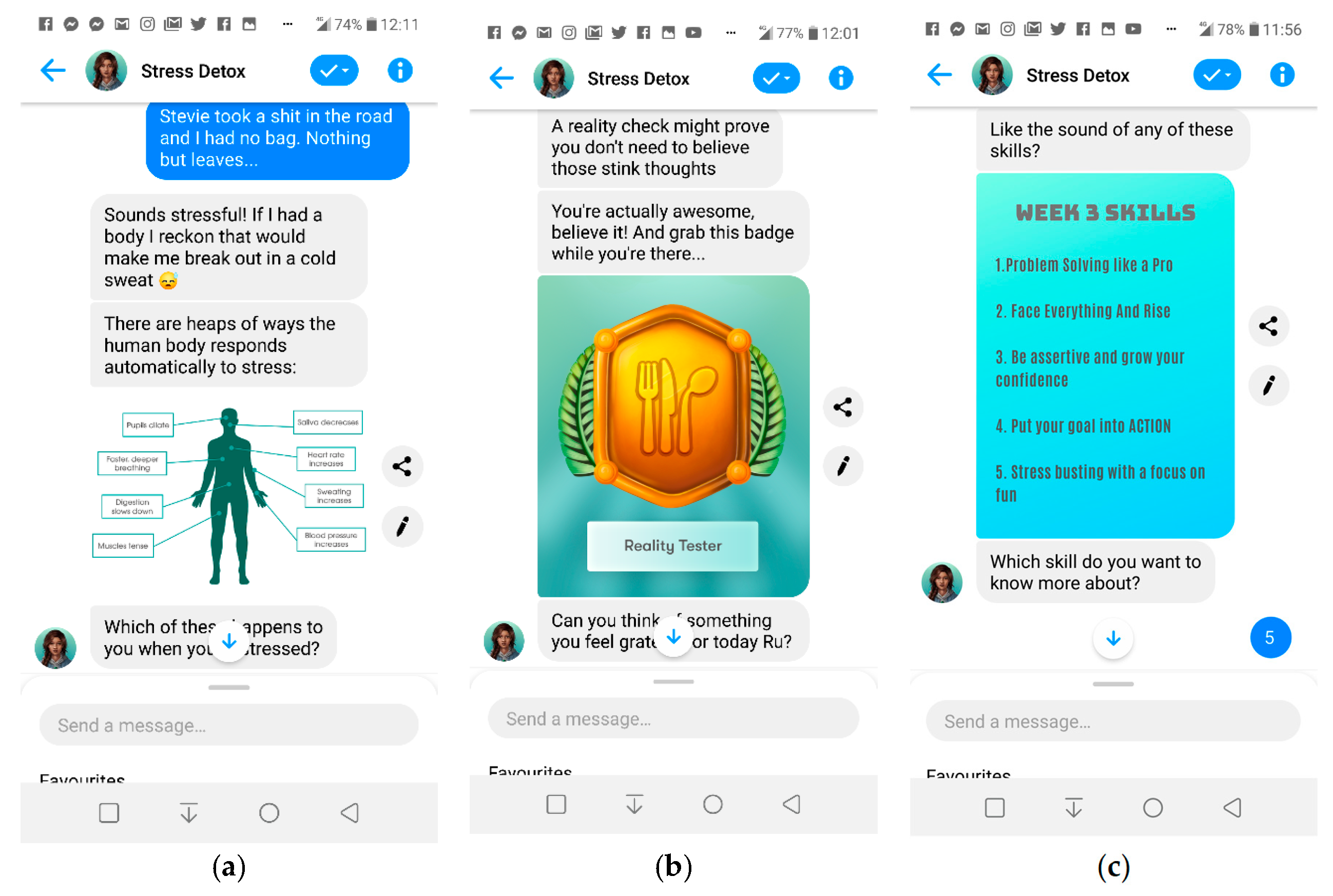
); and week three focused on behavioural response (i.e., action–represented in the chatbot as  ). Day 22 was ‘content-free’ and consisted of a message prompting the participant to complete the post-intervention assessment. Participants who did not reach that point were sent an email on day 22 and two reminders (a week apart) to complete the post-intervention measures via the online study portal. The chatbot content is based on the cognitive behavioural (CBT) model alongside techniques derived from positive psychology i.e., expressing gratitude (Fava et al. 1998) and scheduling time for pleasant activities (Fuchs and Rehm 1977; Wirtz and von Känel 2017). This is conveyed through motivational quotes, jokes, gratitude journaling, and activities to help form positive habits. A summary of content of the intervention is presented in Table 1.
). Day 22 was ‘content-free’ and consisted of a message prompting the participant to complete the post-intervention assessment. Participants who did not reach that point were sent an email on day 22 and two reminders (a week apart) to complete the post-intervention measures via the online study portal. The chatbot content is based on the cognitive behavioural (CBT) model alongside techniques derived from positive psychology i.e., expressing gratitude (Fava et al. 1998) and scheduling time for pleasant activities (Fuchs and Rehm 1977; Wirtz and von Känel 2017). This is conveyed through motivational quotes, jokes, gratitude journaling, and activities to help form positive habits. A summary of content of the intervention is presented in Table 1.- a.
- Data Collection
- b.
- Outcome measurement
- c.
- Data analysis
3. Results
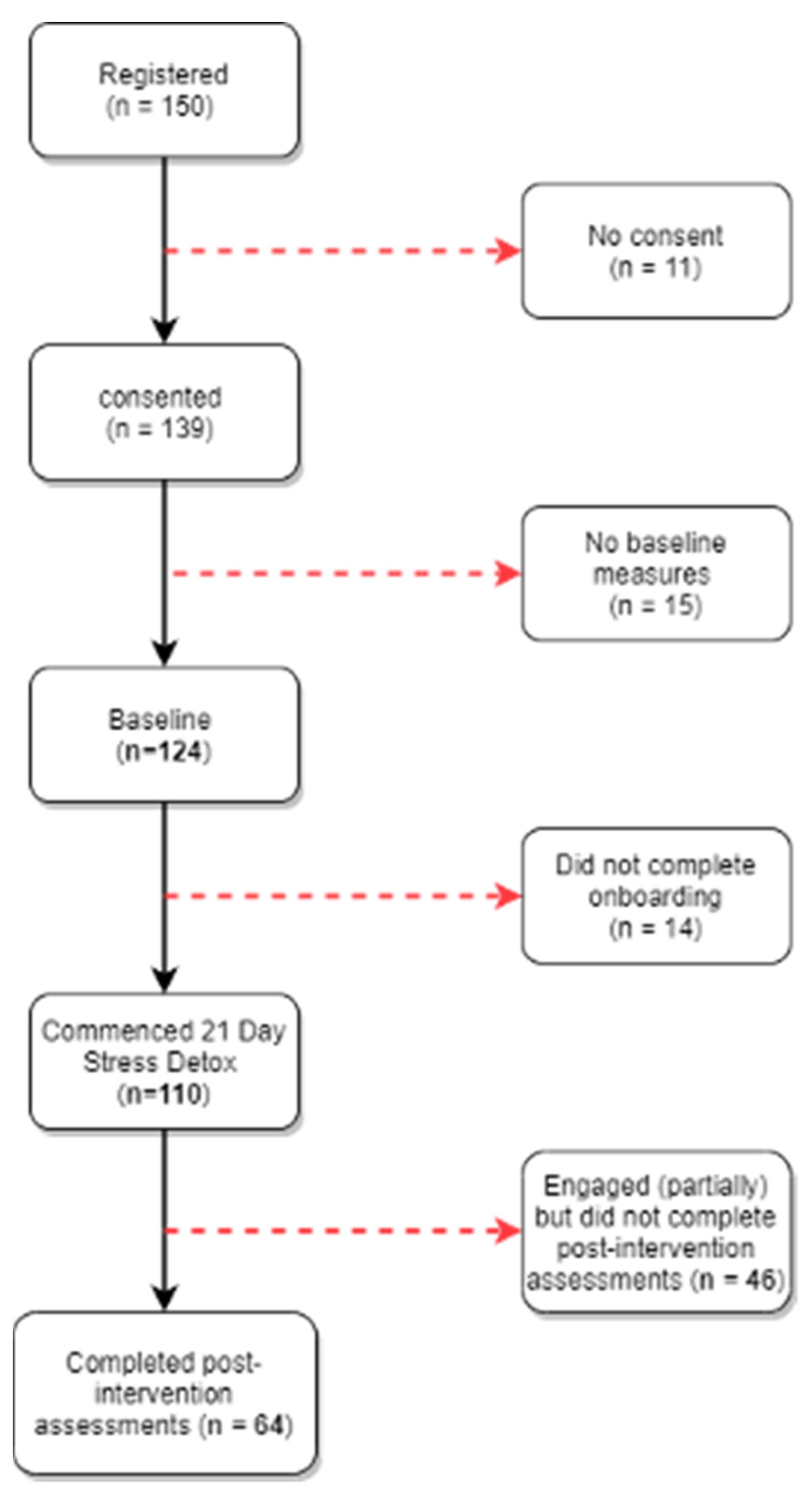
3.1. Participants
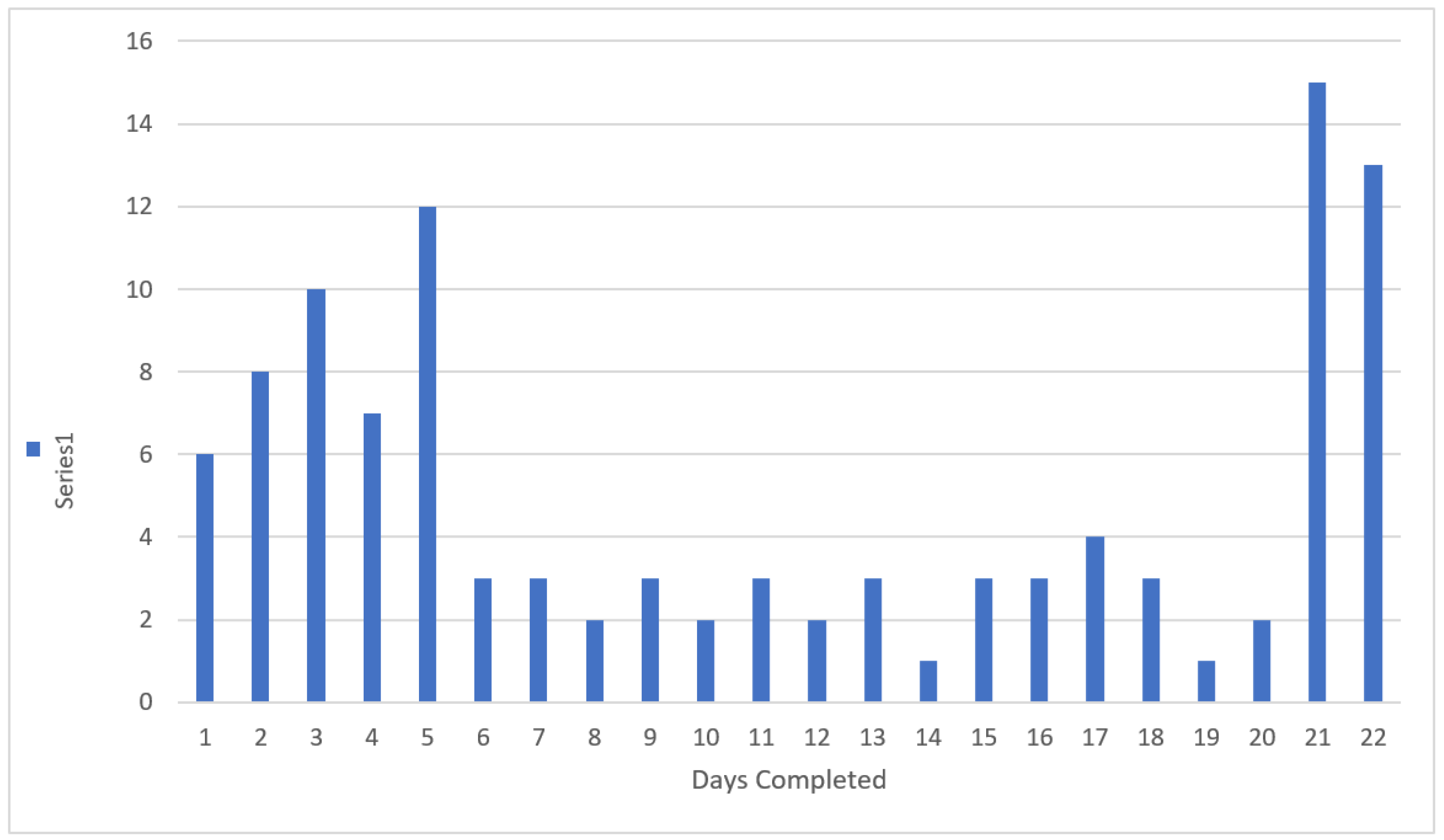
3.2. Engagement and Adherence to the Chatbot
3.3. Acceptability
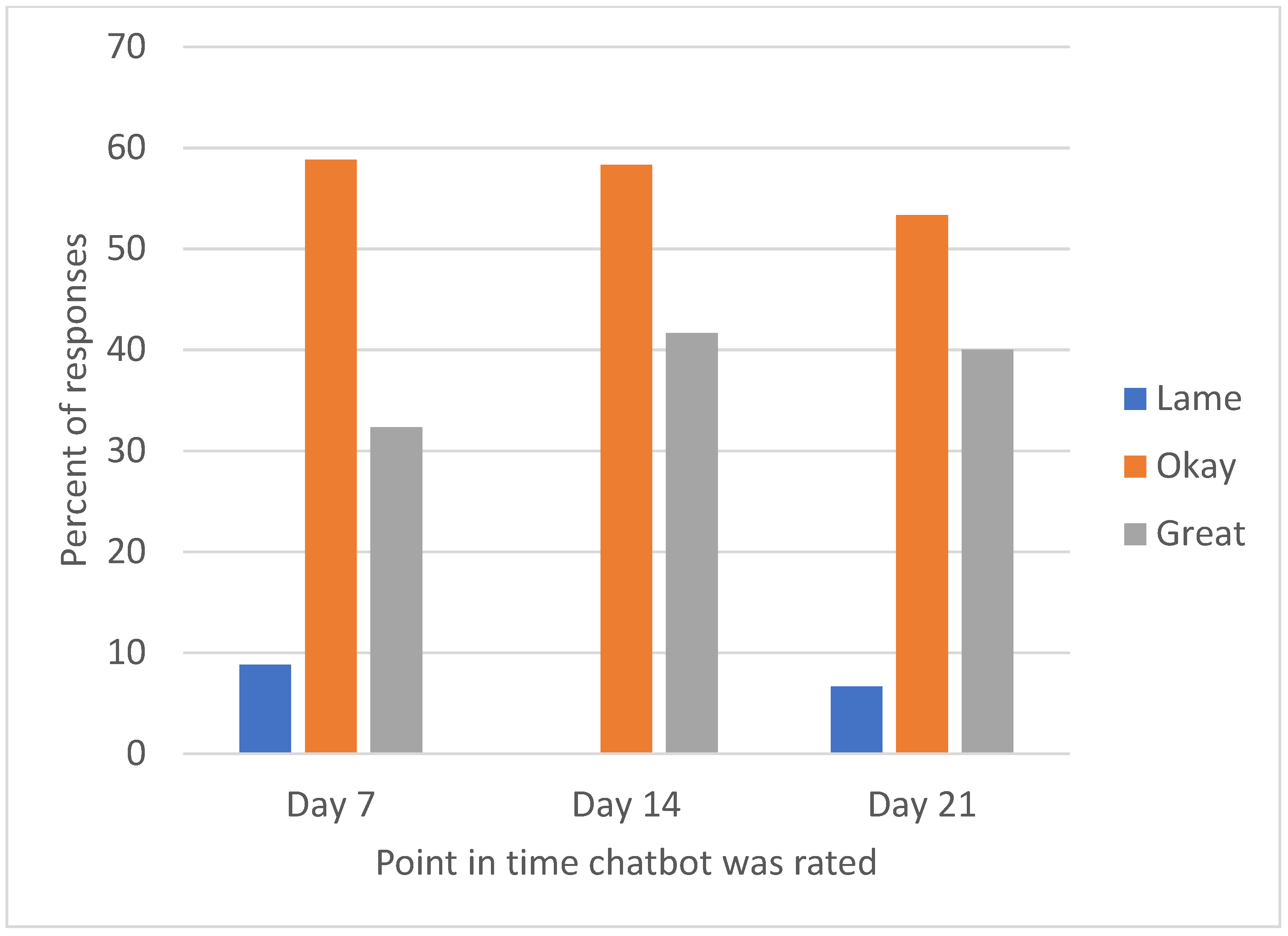
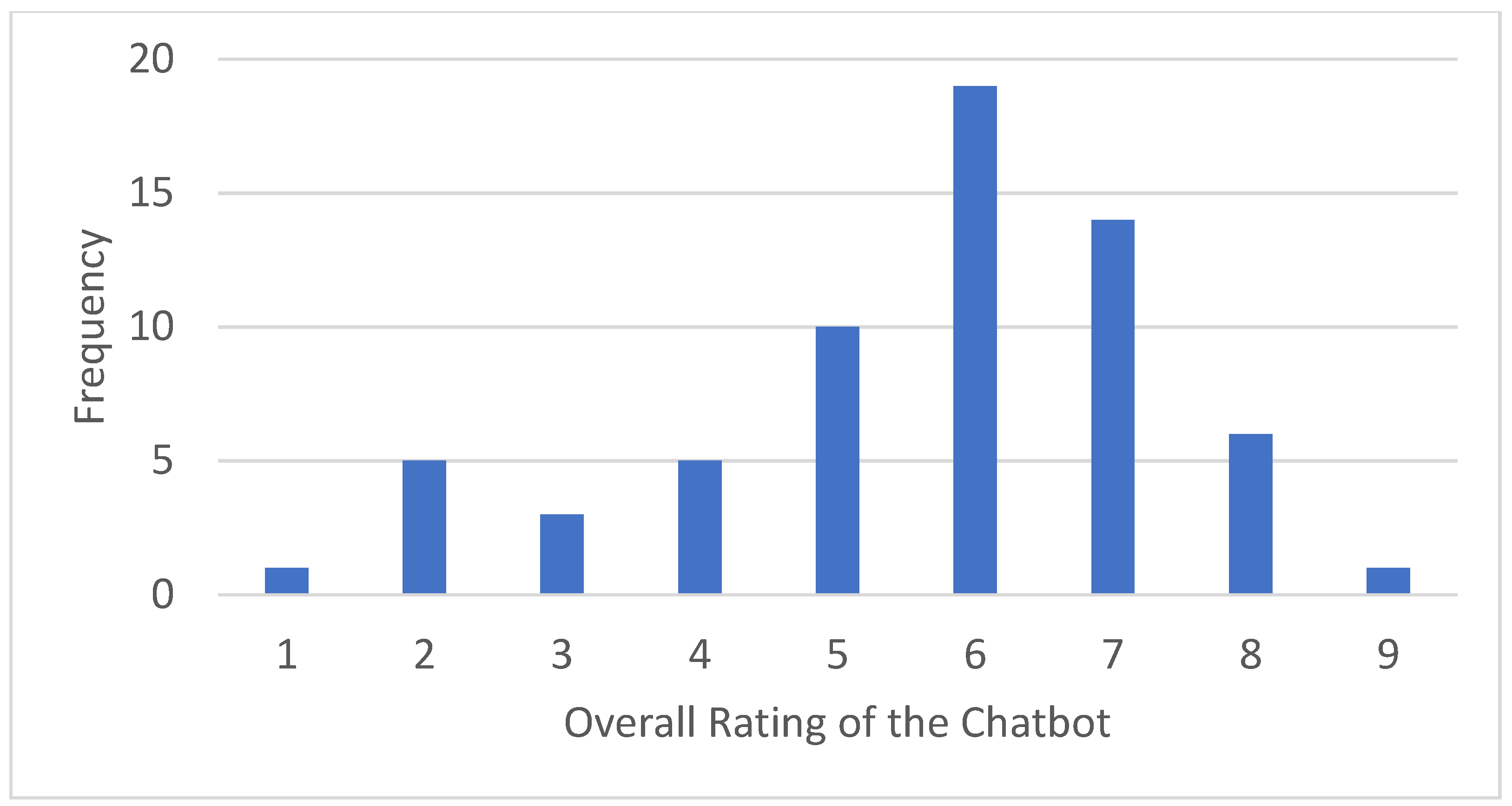
3.3.1. Quantitative Outcomes
3.3.2. Qualitative Feedback
- “What did you like most about the chatbot?” (most liked).
- “What did you like least about the chatbot?” (most disliked).
“I think Stress Detox reinforces the skill set I am already learning through therapy,”(most liked)
“The use of GIFs kept it interesting.”(most liked);
“Some of the things it talked about weren’t relevant to me or my current situation,”(most disliked); and
“I didn’t relate with the language, maybe it would be better to have a language choice,”(most disliked).
“I liked its friendly, outgoing nature. It was a positive addition to my day and made me feel validated,”(most liked);
“Like talking to a friend.”(most liked);
“Sometimes I wish I could be talking to a real person through text because it’s overwhelming to ring someone or talk face to face with them. Having a robot to talk to is nice but it kind of makes you feel alone sometimes,”(most disliked); and
“It didn’t listen to my preferences, and it seemed patronizing at times,”(most disliked).
“I can use it at any time after 8. I can pause and come back to it,”(most liked);
“I liked how it prompted you to use every day.”(most liked);
“Having to do it every day felt like a chore,”(most disliked); and
“Time consuming sometimes,”(most disliked).
“How interactive it was,”(most liked);
“How realistic it is,”(most liked);
“The responses were very limited, you couldn’t really say much,”(most disliked); and
“The same old questions every day,”(most disliked).
3.4. Clinical Efficacy
4. Discussion
4.1. Principal Findings
4.2. Comparisons with Prior Work
4.3. Strengths and Limitations of the Study
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barrett, Marna S., Wee-Jhong Chua, Paul Crits-Christoph, Mary Beth Gibbons, and Don Thompson. 2008. Early withdrawal from mental health treatment: Implications for psychotherapy practice. Psychotherapy: Theory, Research, Practice, Training 45: 247. [Google Scholar] [CrossRef] [PubMed]
- Bech, Per, Lis Raabaek Olsen, Mette Kjoller, and Niels Kristian Rasmussen. 2003. Measuring well-being rather than the absence of distress symptoms: A comparison of the SF-36 Mental Health subscale and the WHO-Five Well-Being Scale. International Journal of Methods in Psychiatric Research 12: 85. [Google Scholar] [CrossRef] [PubMed]
- Benson, Tim, Joe Sladen, Andrew Liles, and Henry W. W. Potts. 2019. Personal Wellbeing Score (PWS)—A short version of ONS4: Development and validation in social prescribing. BMJ Open Qual 8: e000394. [Google Scholar] [CrossRef]
- Carey, Timothy A., Jennifer Haviland, Sara J. Tai, Thea Vanags, and Warren Mansell. 2016. MindSurf: A pilot study to assess the usability and acceptability of a smartphone app designed to promote contentment, wellbeing, and goal achievement. BMC Psychiatry 16: 442. [Google Scholar] [CrossRef] [PubMed]
- Cohen, Sheldon, Tom Kamarck, and Robin Mermelstein. 1994. Perceived stress scale. Measuring Stress: A Guide for Health and Social Scientists 10: 1–2. [Google Scholar]
- Fava, Giovanni A., Chiara Rafanelli, Manuela Cazzaro, Sandra Conti, and Silvana Grandi. 1998. Well-being therapy. A novel psychotherapeutic approach for residual symptoms of affective disorders. Psychological Medicine 28: 475–80. [Google Scholar] [CrossRef]
- Feicht, T., M. Wittmann, G. Jose, A. Mock, E. von Hirschhausen, and T. Esch. 2013. Evaluation of a seven-week web-based happiness training to improve psychological well-being, reduce stress, and enhance mindfulness and flourishing: A randomized controlled occupational health study. Evid Based Complement Alternat Med 2013: 676953. [Google Scholar] [CrossRef]
- Fitzpatrick, Kathleen Kara, Alison Darcy, and Molly Vierhile. 2017. Delivering Cognitive Behavior Therapy to Young Adults With Symptoms of Depression and Anxiety Using a Fully Automated Conversational Agent (Woebot): A Randomized Controlled Trial. JMIR Ment Health 4: e19. [Google Scholar] [CrossRef]
- Fleming, Theresa, Lynda Bavin, Mathijs Lucassen, Karolina Stasiak, Sarah Hopkins, and Sally Merry. 2018. Beyond the trial: Systematic review of real-world uptake and engagement with digital self-help interventions for depression, low mood, or anxiety. Journal of Medical Internet Research 20: e9275. [Google Scholar] [CrossRef]
- Forbes, M. K., E. Crome, M. Sunderland, and V. M. Wuthrich. 2017. Perceived needs for mental health care and barriers to treatment across age groups. Aging & Mental Health 21: 1072–78. [Google Scholar] [CrossRef]
- Fuchs, Carilyn Z., and Lynn P. Rehm. 1977. A self-control behavior therapy program for depression. Journal of Consulting and Clinical Psychology 45: 206. [Google Scholar] [CrossRef]
- Gardiner, Paula M., Kelly D. McCue, Lily M. Negash, Teresa Cheng, Laura F. White, Leanne Yinusa-Nyahkoon, Brian W. Jack, and Timothy W. Bickmore. 2017. Engaging women with an embodied conversational agent to deliver mindfulness and lifestyle recommendations: A feasibility randomized control trial. Patient Education and Counseling 100: 1720–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greer, Stephanie, Danielle Ramo, Yin-Juei Chang, Michael Fu, Judith Moskowitz, and Jana Haritatos. 2019. Use of the Chatbot “Vivibot” to Deliver Positive Psychology Skills and Promote Well-Being Among Young People After Cancer Treatment: Randomized Controlled Feasibility Trial. JMIR mHealth and uHealth 7: e15018. [Google Scholar] [CrossRef]
- Gulliver, Amelia, Kathleen M. Griffiths, and Helen Christensen. 2010. Perceived barriers and facilitators to mental health help-seeking in young people: A systematic review. BMC Psychiatry 10: 113. [Google Scholar] [CrossRef] [Green Version]
- Gustavson, Kristin, Ann Kristin Knudsen, Ragnar Nesvåg, Gun Peggy Knudsen, Stein Emil Vollset, and Ted Reichborn-Kjennerud. 2018. Prevalence and stability of mental disorders among young adults: Findings from a longitudinal study. BMC Psychiatry 18: 65. [Google Scholar] [CrossRef] [PubMed]
- Holt-Quick, Chester, Jim Warren, Karolina Stasiak, Ruth Williams, Grant Christie, Sarah Hetrick, Sarah Hopkins, Tania Cargo, and Sally Merry. 2021. A chatbot architecture for promoting youth resilience. In Studies in Health Technology and Informatics. pp. 99–105. Available online: https://minerva-access.unimelb.edu.au/bitstream/handle/11343/280661/SHTI210017.pdf (accessed on 20 October 2021).
- Huckins, Jeremy F., Alex W. DaSilva, Weichen Wang, Elin Hedlund, Courtney Rogers, Subigya K. Nepal, Jialing Wu, Mikio Obuchi, Eilis I. Murphy, and Meghan L. Meyer. 2020. Mental health and behavior of college students during the early phases of the COVID-19 pandemic: Longitudinal smartphone and ecological momentary assessment study. Journal of Medical Internet Research 22: e20185. [Google Scholar] [CrossRef]
- Inkster, Becky, Shubhankar Sarda, and Vinod Subramanian. 2018. An Empathy-Driven, Conversational Artificial Intelligence Agent (Wysa) for Digital Mental Well-Being: Real-World Data Evaluation Mixed-Methods Study. JMIR mHealth uHealth 6: e12106. [Google Scholar] [CrossRef] [Green Version]
- Kessler, Ronald C., Wai Tat Chiu, Olga Demler, and Ellen E. Walters. 2005. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry 62: 617–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, Ronald C., G. Paul Amminger, Sergio Aguilar-Gaxiola, Jordi Alonso, Sing Lee, and T. Bedirhan Ustun. 2007. Age of onset of mental disorders: A review of recent literature. Current Opinion in Psychiatry 20: 359. [Google Scholar] [CrossRef] [PubMed]
- Kessler, Ronald C., Maria Petukhova, Nancy A. Sampson, Alan M. Zaslavsky, and Hans-Ullrich Wittchen. 2012. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. International Journal of Methods in Psychiatric Research 21: 169–84. [Google Scholar] [CrossRef] [PubMed]
- Lattie, Emily G., Elizabeth C. Adkins, Nathan Winquist, Colleen Stiles-Shields, Q. Eileen Wafford, and Andrea K. Graham. 2019. Digital Mental Health Interventions for Depression, Anxiety, and Enhancement of Psychological Well-Being Among College Students: Systematic Review. Journal of Medical Internet Research 21: e12869. [Google Scholar] [CrossRef] [PubMed]
- Linardon, Jake, Pim Cuijpers, Per Carlbring, Mariel Messer, and Matthew Fuller-Tyszkiewicz. 2019. The efficacy of app-supported smartphone interventions for mental health problems: A meta-analysis of randomized controlled trials. World Psychiatry 18: 325–36. [Google Scholar] [CrossRef] [Green Version]
- MHA National. 2021. COVID-19 and Mental Health: A Growing Crisis. Available online: https://mhanational.org/sites/default/files/Spotlight%202021%20-%20COVID-19%20and%20Mental%20Health.pdf (accessed on 20 October 2021).
- Ministry of Health. 2017. Ethnicity Data Protocols. Wellington: Ministry of Health. [Google Scholar]
- Mojtabai, Ramin, Mark Olfson, Nancy A. Sampson, Robert Jin, Benjamin Druss, Philip S. Wang, Kenneth B. Wells, Harold A. Pincus, and Ronald C. Kessler. 2011. Barriers to mental health treatment: Results from the National Comorbidity Survey Replication. Psychological Medicine 41: 1751–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oakley Browne, Mark A., J. Elisabeth Wells, Kate M. Scott, and Magnus A. McGee. 2006. Lifetime prevalence and projected lifetime risk of DSM-IV disorders in Te Rau Hinengaro: The New Zealand Mental Health Survey. The Australian and New Zealand journal of psychiatry 40: 865–74. [Google Scholar] [CrossRef] [PubMed]
- Ollendick, Thomas H., Lars-Göran Öst, and Lara J. Farrell. 2018. Innovations in the psychosocial treatment of youth with anxiety disorders: Implications for a stepped care approach. Evidence Based Mental Health 21: 112. [Google Scholar] [CrossRef]
- Patel, Vikram, Alan J. Flisher, Sarah Hetrick, and Patrick McGorry. 2007. Mental health of young people: A global public-health challenge. The Lancet 369: 1302–13. [Google Scholar] [CrossRef]
- Patton, Michael Quinn. 2002. Two Decades of Developments in Qualitative Inquiry: A Personal, Experiential Perspective. Qualitative Social Work 1: 261–83. [Google Scholar] [CrossRef]
- Roberti, Jonathan W., Lisa N. Harrington, and Eric A. Storch. 2006. Further psychometric support for the 10-item version of the perceived stress scale. Journal of College Counseling 9: 135–47. [Google Scholar] [CrossRef]
- Rowland, Simon P., J. Edward Fitzgerald, Thomas Holme, John Powell, and Alison McGregor. 2020. What is the clinical value of mHealth for patients? Npj Digital Medicine 3: 4. [Google Scholar] [CrossRef] [PubMed]
- Schegloff, Emanuel A. 1968. Sequencing in Conversational Openings1. American Anthropologist 70: 1075–95. [Google Scholar] [CrossRef]
- Shanahan, Michael J. 2000. Pathways to Adulthood in Changing Societies: Variability and Mechanisms in Life Course Perspective. Annual Review of Sociology 26: 667–92. [Google Scholar] [CrossRef]
- Silfvernagel, Kristin, Carolina Wassermann, and Gerhard Andersson. 2017. Individually tailored internet-based cognitive behavioural therapy for young adults with anxiety disorders: A pilot effectiveness study. Internet Interventions 8: 48–52. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, Robert L., Kurt Kroenke, Janet B. W. Williams, and Bernd Löwe. 2006. A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine 166: 1092–97. [Google Scholar] [CrossRef] [Green Version]
- Staehr Johansen, K. 1998. The Use of Well-Being Measures in Primary Health Care—the DepCare Project. target 12, E60246. Geneva: World Health Organization. [Google Scholar]
- Swift, Joshua K., and Roger P. Greenberg. 2012. Premature discontinuation in adult psychotherapy: A meta-analysis. Journal of Consulting and Clinical Psychology 80: 547. [Google Scholar] [CrossRef]
- Taylor, John M. 2015. Psychometric analysis of the Ten-Item Perceived Stress Scale. Psychological Assessment 27: 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, David R. 2006. A General Inductive Approach for Analyzing Qualitative Evaluation Data. American Journal of Evaluation 27: 237–46. [Google Scholar] [CrossRef]
- Tinkler, Lucy, and Stephen Hicks. 2011. Measuring subjective well-being. London: Office for National Statistics 2011: 443–55. [Google Scholar]
- Topp, Christian Winther, Søren Dinesen Østergaard, Susan Søndergaard, and Per Bech. 2015. The WHO-5 Well-Being Index: A systematic review of the literature. Psychotherapy and Psychosomatics 84: 167–76. [Google Scholar] [CrossRef]
- Vaidyam, Aditya Nrusimha, Hannah Wisniewski, John David Halamka, Matcheri S. Kashavan, and John Blake Torous. 2019. Chatbots and conversational agents in mental health: A review of the psychiatric landscape. The Canadian Journal of Psychiatry 64: 456–64. [Google Scholar] [CrossRef]
- VanderWeele, Tyler J., Claudia Trudel-Fitzgerald, Paul Allin, Colin Farrelly, Guy Fletcher, Donald E. Frederick, Jon Hall, John F. Helliwell, Eric S. Kim, William A. Lauinger, and et al. 2020. Current recommendations on the selection of measures for well-being. Preventive Medicine, 106004. [Google Scholar] [CrossRef] [PubMed]
- Warren, Jim, Sarah Hopkins, Andy Leung, Sarah Hetrick, and Sally Merry. 2020. Building a Digital Platform for Behavioral Intervention Technology Research and Deployment. In Paper presented at the Proceedings of the 53rd Hawaii International Conference on System Sciences, Wailea, HI, USA, January 7. [Google Scholar]
- Wirtz, Petra H., and Roland von Känel. 2017. Psychological stress, inflammation, and coronary heart disease. Current Cardiology Reports 19: 111. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Henry, Dever M. Carney, Soo Jeong Youn, Rebecca A. Janis, Louis G. Castonguay, Jeffrey A. Hayes, and Benjamin D. Locke. 2017. Are we in crisis? National mental health and treatment trends in college counseling centers. Psychological Services 14: 407. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Focus | Day | Module |
|---|---|---|
| Week 1:
Feelings | 1 | Onboarding (‘meet & greet’) |
| SMART Goal | ||
| Gratitude Journal introduced | ||
| 2 | Subjective Stress Rating | |
| Breathe Taster | ||
| Goal Setting | ||
| 3 | Stress Sensations | |
| Calm Breathing | ||
| 4 | Stress Psychoeducation | |
| Focusing Game | ||
| 5 | Cognitive Triad | |
| Progressive Muscle Relaxation (PMR) | ||
| 6 | Sleep Psychoeducation | |
| Self-Care Psychoeducation | ||
| 7 | Know Your Anxiety | |
| Meditation | ||
| Gratitude Journal Review | ||
| Week 2:
Thinking | 8 | Downloading the Positives |
| 9 | Stink Thoughts | |
| 10 | Reality Check | |
| 11 | Challenging Thoughts | |
| 12 | Brainstorming | |
| 13 | Perspective | |
| 14 | Recap | |
| Week 3:
Actions | 15 | STEPS |
| 16 | Stairwell of Stress | |
| 17 | Assertiveness | |
| 18 | Conflict Resolution | |
| 19 | Pleasant Activity Part1 | |
| 20 | Pleasant Activity Part 2 | |
| Communication Skills | ||
| 21 | Recap of modules | |
| Gratitude Journal Review | ||
| 22 | Outboarding |
| Measure | Time Point | ||||||
|---|---|---|---|---|---|---|---|
| Baseline | Day | Post-Intervention | Passively Throughout | ||||
| 7 | 14 | 21 | |||||
| Quantitative | Demographics |  | |||||
| WHO-5 | | | |||||
| ONS4 | | | |||||
| PSS-10 | | | |||||
| GAD-7 | | | |||||
| Chatbot use (engagement) | | ||||||
| Chatbot satisfaction | | | | ||||
| Chatbot Rating Scale | | ||||||
| Qualitative | |||||||
| Likes and dislikes | | | | | |||
| Suggestions for improvement | | ||||||
| Overall review | | ||||||
| Percentage * (Number) | ||
|---|---|---|
| Age | 18–20 | 46% (53) |
| 21–23 | 47% (54) | |
| Over 24 | 7% (8) | |
| Gender | Female | 81% (87) |
| Male | 16% (17) | |
| Transgender | 1% (1) | |
| None of these | 2% (2) | |
| Ethnicity ** | NZ European | 45% (48) |
| Asian | 41% (44) | |
| Māori | 6.5% (7) | |
| Other | 4.7% (5) | |
| Pacific | 2.7% (3) | |
| Stage at university | 1st year | 51.2% (63) |
| Other undergraduate | 46.3% (57) | |
| Post-graduate | 2.4% (3) |
| Mean Score | Min | Max | Possible Range | ||
|---|---|---|---|---|---|
| M | SD | ||||
| WHO-5 | 42.23 | 19.09 | 4 | 84 | 0–100 |
| PSS -10 | 22.02 | 6.43 | 4 | 40 | 0–40 |
| ONS4-1 | 6.10 | 2.21 | 0 | 10 | 0–10 |
| ONS4-2 | 6.82 | 2.05 | 0 | 10 | 0–10 |
| ONS4-3 | 5.64 | 2.36 | 0 | 10 | 0–10 |
| ONS4-4 | 5.73 | 2.45 | 0 | 10 | 0–10 |
| GAD-7 | 8.73 | 2.71 | 1 | 21 | 0–21 |
| Chatbot Rating Scale Item | Participant Rating out of 4
(N = 64) | |
|---|---|---|
| M | SD | |
| I thought it was helpful. | 2.47 | 1.04 |
| I thought it was easy to use. | 3.25 | 0.84 |
| I thought it was fun. | 2.36 | 1.07 |
| I thought it reflected my culture. | 2.05 | 1.15 |
| I thought it was nice to look at. | 2.77 | 0.89 |
| I thought it worked smoothly (e.g., without crashing). | 3.17 | 1.00 |
| I would like to keep it on my device. | 2.00 | 1.18 |
| Paired Differences | Effect Size | t | df | p | |||||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | SE | 95% CI | ||||||
| Lower | Upper | ||||||||
| WHO−5 | −7.38 | 15.07 | 1.88 | −11.14 | −3.61 | 0.49 | −3.91 | 63 | <0.001 |
| PSS−10 | 1.77 | 4.69 | 0.59 | 0.59 | 2.94 | 0.38 | 3.01 | 63 | 0.004 |
| ONS4−1 | −0.23 | 1.49 | 0.19 | −0.61 | 0.14 | 0.16 | −1.26 | 63 | 0.21 |
| ONS4−2 | −0.14 | 1.38 | 0.17 | −0.49 | 0.20 | 0.10 | −0.82 | 63 | 0.42 |
| ONS4−3 | −0.05 | 2.74 | 0.34 | −0.73 | 0.64 | 0.02 | −0.14 | 63 | 0.89 |
| ONS4−4 | 0.06 | 2.81 | 0.35 | −0.64 | 0.77 | 0.02 | 0.18 | 63 | 0.86 |
| GAD−7 | 0.20 | 3.45 | 0.43 | −0.66 | 1.07 | 0.06 | 0.47 | 63 | 0.64 |
| WHO-5 Change | ONS4-1 Change | ONS4-2 Change | ONS4-3 Change | ONS4-4 Change | GAD-7 Change | PSS Change | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | |
| GAD-7 < 10 (N = 39) | 6.67 | 14.89 | 0.13 | 1.26 | 0.33 | 1.38 | −0.33 | 3.06 | −0.08 | 3.18 | 0.67 | 3.30 | −1.54 | 4.58 |
| GAD-7 ≥ 10 (N = 25) | 8.48 | 15.59 | 0.40 | 1.80 | −0.16 | 1.34 | 0.64 | 2.08 | −0.04 | 2.17 | −1.56 | 3.31 | −2.12 | 4.94 |
| p-value | 0.64 | 0.48 | 0.16 | 0.17 | 0.96 | 0.01 | 0.63 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Williams, R.; Hopkins, S.; Frampton, C.; Holt-Quick, C.; Merry, S.N.; Stasiak, K. 21-Day Stress Detox: Open Trial of a Universal Well-Being Chatbot for Young Adults. Soc. Sci. 2021, 10, 416. https://doi.org/10.3390/socsci10110416
Williams R, Hopkins S, Frampton C, Holt-Quick C, Merry SN, Stasiak K. 21-Day Stress Detox: Open Trial of a Universal Well-Being Chatbot for Young Adults. Social Sciences. 2021; 10(11):416. https://doi.org/10.3390/socsci10110416
Chicago/Turabian StyleWilliams, Ruth, Sarah Hopkins, Chris Frampton, Chester Holt-Quick, Sally Nicola Merry, and Karolina Stasiak. 2021. "21-Day Stress Detox: Open Trial of a Universal Well-Being Chatbot for Young Adults" Social Sciences 10, no. 11: 416. https://doi.org/10.3390/socsci10110416