1. Introduction
Architecture’s problem is marked by its period circumstances. Today, these difficulties are caused by, among other things, climate change, environmental decline, energy inefficiency, and the social transformation brought about by the silent, digital revolution, all affecting people’s health and wellbeing. An imperatively social demand for healthier cities and architecture sprang up a century ago, after a different concept of mobility arose, based on motorised transport such as motorbikes, cars, and buses. This was in addition to the ecological awareness emerging after the first oil crisis in 1973 and the technological and digital revolution of the last four decades.
Cities are places shaped by different strata that show the successive stages of their history. Some authors, composing an analogy that likens disease to destruction, maintain that a city’s architecture and layers are remains of social responses to the epidemics humanity has suffered throughout time [
1]. However, architecture has not been the discipline that has fought against disease; this has been medicine. Architecture’s contribution to health has been to design capable environments that promote and strengthen people’s physical and emotional health and build spaces that eliminate noxious and insalubrious conditions in order to prevent illnesses. Architecture can be understood as an extension of nature, like coral reefs or beaver dams [
2].
People spend most of their lives inside buildings; hence, homes, offices, residences, schools, and public facilities have to be not only environmentally sustainable but also designed and understood as places where people can live better, with greater wellbeing. The spatial and residential experiences of humans are stimulated by shapes, textures, sounds, lighting, and other signals, perceived physiologically by the senses, that shape the contours of memories and behaviours. Wellbeing and health are closely related to the way the human body interacts with the environment and how it influences the body and the brain [
3]. Nevertheless, the effect of architecture in improving healthcare and disease prevention has gone unnoticed. This is, perhaps, because the absence of health has been confused with disease or because the evidence of a relationship between a healthy environment and the absence of disease has not been clinically established.
Over the last century, architecture has generated progressive wellbeing and an improvement in people’s quality of life, promoting the construction of buildings with elements that provide better defences against pathogenic factors present in the environment [
4]. From this perspective, architecture has been shown to be one of the main agents of human health. In recent years, a new paradigm has been consolidated, aimed not only at combating pathogenic problems that arise in unhealthy environments and buildings but also at stimulating the presence of elements that favour and benefit human health in buildings and cities. It is a model whose attention is especially focused on the physiological, cognitive, and emotional influence that spaces have on people.
The World Health Organization (WHO) recognises that the design, performance, and maintenance of buildings have a significant impact on the health of their occupants and can generate or worsen diseases [
5]. Exposure to inadequate architectural parameters and indicators that affect indoor air quality (IAQ), thermal comfort, noise, lighting, atmospheric and ionization, among others, condition people’s quality of life in the short, medium, and long term. In the wake of the recent global public health crisis, the generation of theoretical, practical, and interdisciplinary knowledge of the characteristics of buildings that provide positive sensory experiences, as well as physical and mental health outcomes, is timely and responsible [
6]. The hypothesis of this paper is that architecture is no longer defined solely by visual or geometrical parameters but also by other dimensions involving environmental, cognitive, psychological, and physiological aspects, affecting comfort, wellbeing, and the physical and mental health of people. This article aims to demonstrate this proposition, and it is the main goal of this work.
To address this objective, the methodology is mixed, first developing a theoretical character and afterwards defining an analytical framework, with some examples demonstrating this new concept of healthy architecture. On the one hand, this research’s state-of-art will be defined after an examination of the main related literature following the critical review foundations: search, appraisal, analysis, and synthesis [
7]. On the other hand, it uses the empirical experiences of several projects, buildings, and installations that will help to contextualise the problem and obtain certain patterns, serving as a basis for the results obtained.
These contemporary architectural examples, built over the last thirty years for groups with specific needs, have been chosen for being initiatives in which architecture is considered not only essential to the functional aspects of health, but also for the incorporated symbolic, cognitive, and emotional elements. Furthermore, a series of experimental installations were evaluated, in which the understanding of architectural space was approached from a phenomenological dimension, sensitive to cognitive, sensory, neurological, or even chemical stimuli from human beings, just as biology and neurosciences have revealed. In this article, these buildings and environments are presented and analysed as case studies, and from these, the main results are obtained and presented below.
This work has been structured in several sections. After this introduction, the previous and present theoretical background of how the architectural discipline has developed to build increasingly healthier environments is presented. The period from the hygienist movements of the 19th century up to the beginning of the 21st century will be described and contextualised.
Section 3 presents the hypothesis, three contemporary approaches to healthy architecture, and a series of experimental installations. These installations demonstrate how an understanding of the physical–chemical mechanisms that govern organisms represents an important change in our way of thinking and understanding space, and not just from a visual and/or aesthetic or compositional point of view. This implies new ways of planning or designing buildings, environments, and spaces to make them healthier.
Section 4 presents the results, accompanied by a Decalogue of points or criteria that an environment or building should meet to be considered healthy.
Section 5 and
Section 6 present the discussion and conclusions, respectively, and the definition of healthy architecture.
2. Background and Current Context
2.1. Hygiene Movements: The Genesis of Building Wellness
Mid-nineteenth-century hygiene movements have been described as the starting point, arising from social demands to address the unsanitary, urban agglomerations that emerged after the Industrial Revolution. From these demands, new concepts and urban models arose, such as the Garden City or Linear City [
8]. Another important step was the programmatic claims of the European architectural avant-gardes of the early 20th century. A paradigmatic example of what these meant for the improvement of human health was the introduction of individual rooms into homes, intended to be bathrooms or kitchens.
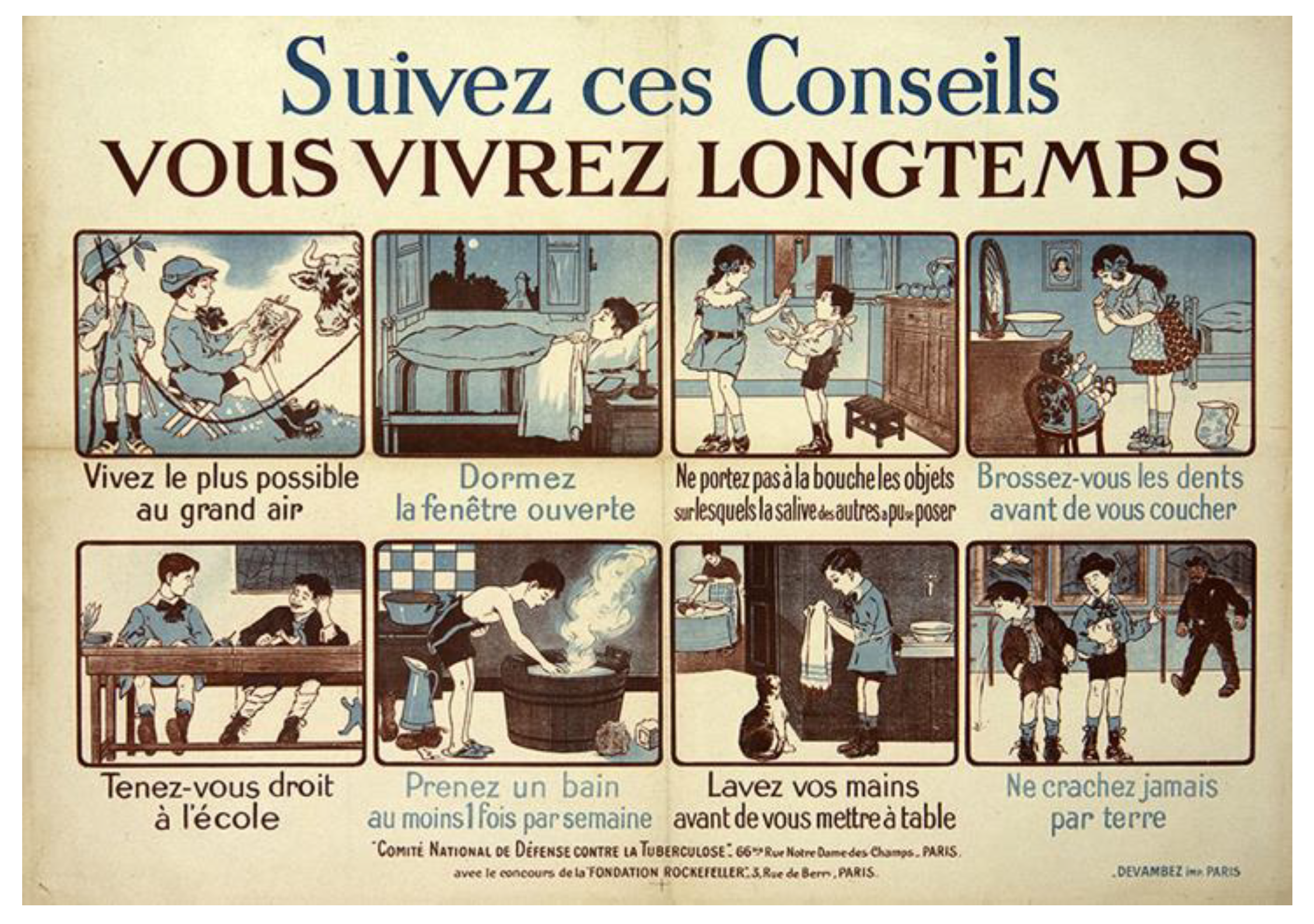
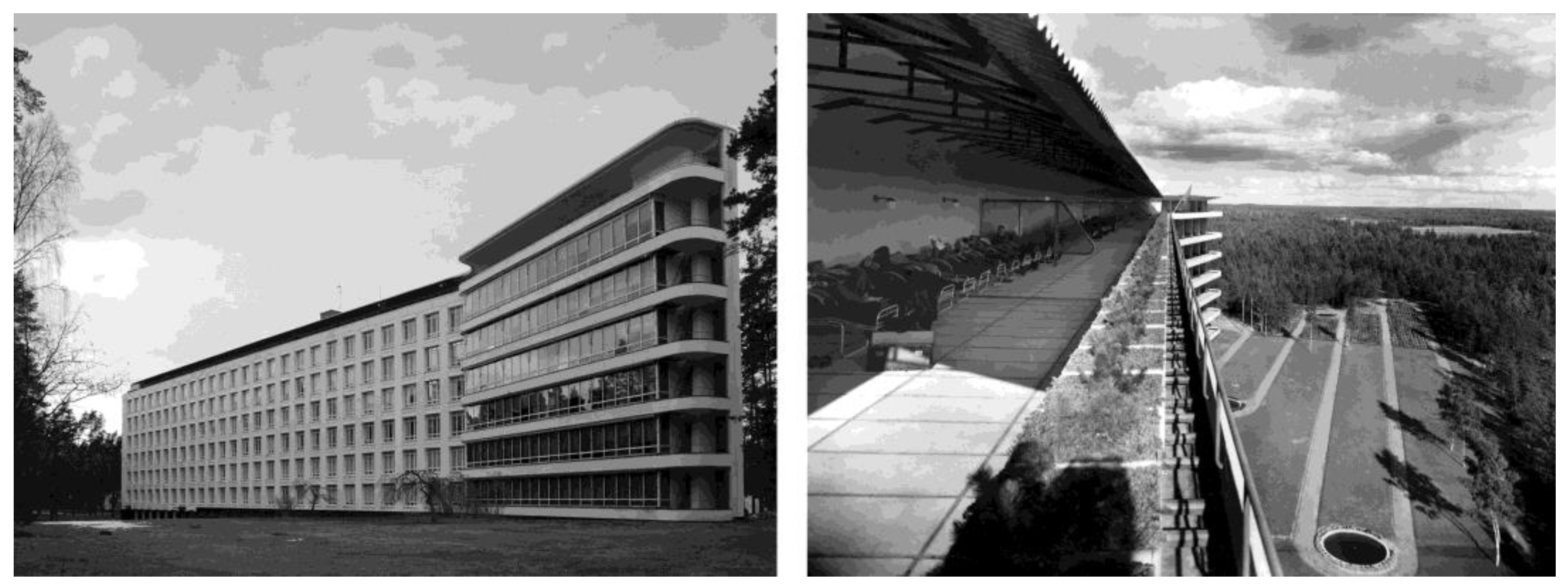
One of the catalysts in identifying hygienic solutions in buildings and dwellings was the decades-long lack of effective remedies against cholera and tuberculosis. The only thing that seemed to combat the latter disease was sunlight, cleanliness, and rest, so buildings began to be designed to promote those factors (
Figure 1). Hospitals were built with large windows and sanatoriums with enormous terraces; dwellings were raised above the ground to distance them from dampness; and aerodynamic furniture was designed so that dust would not settle and host germs (
Figure 2).
Those unsanitary environmental conditions motivated the pioneers of the modern movement, although dealing with these was not its objective. Its priorities were far from a linear response to the functional problems derived from a health situation. Its main concern was aesthetics, and its purpose was to create a new style. Based on the premise that all buildings should meet minimum functional standards, they proposed a new architecture that should be a faithful expression of the use for which it was intended. For the avant-gardes, the redeeming myth for humanity was the machine. Buildings, products, and objects targeted a single prototype of an individual, the mass man, whose desires and needs were seen as being common throughout the world.
With these foundations, architects constructed buildings which, like machines, resolved the required functional problems effectively, but they did not easily fulfil people’s need to express emotions, recognise themselves, or self-actualise. The concepts of life and death, with their respective emotions of joy and sadness, were excluded from care and health institutions. The consequences were impersonal spaces and oppressively alienating buildings. Faithful to their programmatic principles, healthcare buildings incorporated such technical features as sanitation, accessibility, and safety. These were built on the basis of the symptoms of a disease, whereby a medical cure was considered the only useful factor in treatments. This utilitarian approach gave rise to sterile, hard surfaces; shiny, colourless spaces; long internal corridors, isolated from the outside and devoid of natural light; and artificial ventilation systems, with batteries of minimalist rooms. These features made healthcare buildings effective healing factories, but with no identity, meaningless and soulless. Rarely was any thought given to the occupant’s emotional needs, whether healthy or sick, when they experienced these spaces.
In reaction to the machines that had created so much destruction during the Second World War, through the reconstruction of Europe, the person was placed at the centre of architectural thinking. At the CIAM Congresses (
Congrès Internationaux d’Architecture Moderne, or International Congresses of Modern Architecture), which took place between 1947 and 1953, the conclusion was reached finding that it was necessary to consider the person as an individual, with their own identity and various peculiarities, causing a multiplicity of situations and requiring various environments. In 1945, Henry Sigerist, a historian and health professional, was the first to refer to the promotion of health and the environment as one of the four fundamental actions of medical care, followed by the prevention of disease, treatment, and rehabilitation [
10].
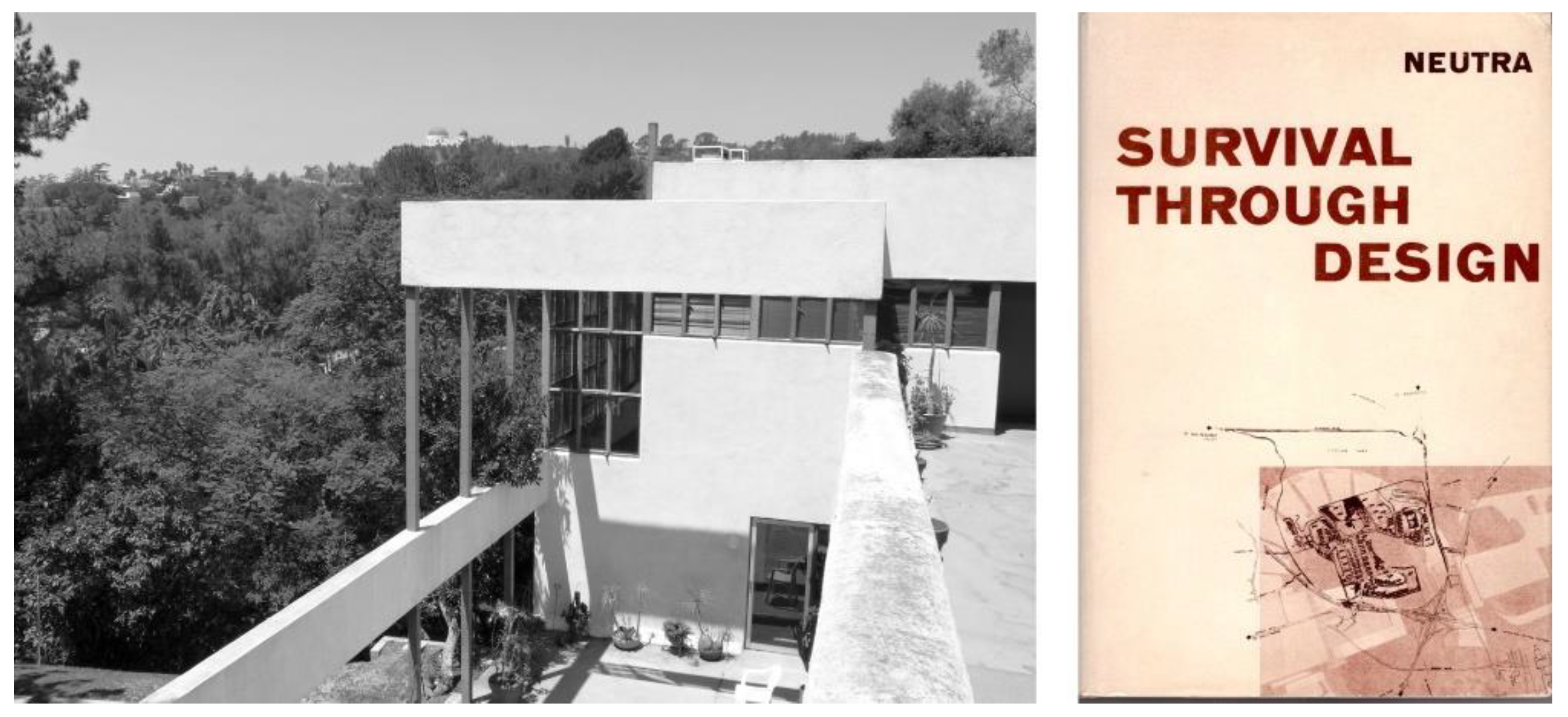
Richard Neutra is also considered one of the pioneers of environmental design, guided towards the physiological needs of human beings and their natural behaviour in space. In 1946, he designed and built the Lovell Health House on Dundee Drive (Los Angeles, California) for the naturopathic doctor Phillip Lovell. The architect explored the consideration of physiology and psychology in architectural design by publishing a series of writings and collected in his book Survival Through Design (
Figure 3). In it, he maintained that “we orient ourselves by physiological coordinates and we exist thanks to the sensory forms that surround and stimulate us” [
11].
These new, person-centred perspectives represented a decisive paradigm shift in architecture. Its assimilation was slow but progressive over time. The way in which cities inhabited their environments and how these were perceived and understood began to be modified. To understand the legibility of urban space and know more about what a person perceives, when travelling through a city, the urban planner Kevin Lynch developed the concept of a cognitive map as a hypothetical construct, created on the basis of humans’ introspective stories [
12]. For the first time, he made environmental sketches and information systems, obtained by experiencing his route in order to improve our understanding of the urban space. Lynch’s research was a milestone in beginning to understand, in depth, the way a physical environment can have positive or negative emotional consequences for a person.
At the end of the sixties, Ian L. McHarg’s book Design with Nature was published [
13]. According to the American historian Lewis Mumford, in reaction to a polluted, dehumanised, and machine-dominated world, this publication established scientific, technical, and philosophical foundations for the development of a new human civilization. This would replace the current one, which, according to Mumford, was in the process of accelerated disintegration. McHarg, a town planner, landscape architect, and inspired ecologist, laid the groundwork for current environmental planning conforming to a certain ecological determinism, which was the origin of what would later be referred to with the pleonasm “sustainable architecture”.
With an insightful vision of the future, McHarg finished his book with a chapter called The City: Health and Disease. In it, he asked whether health is only the absence of disease. He argued that health is a symptom of creativity and adaptation and that illness is an expression of a capacity for destruction and a lack of adaptation. He wondered in what places the physical, mental, and social health environment and illness’s environment were located. He maintained that, if the healthy and unhealthy areas in cities could be identified, the environmental agents that promote health and the risk factors that cause the disease could be associated with them. From this intelligent approach, which was proposed more than fifty years ago, arose a fundamental action that all cities, counties, and countries should undertake—mapping healthy and unhealthy spaces [
13].
2.2. The Emergence of Salutogenesis and Neuroarchitecture
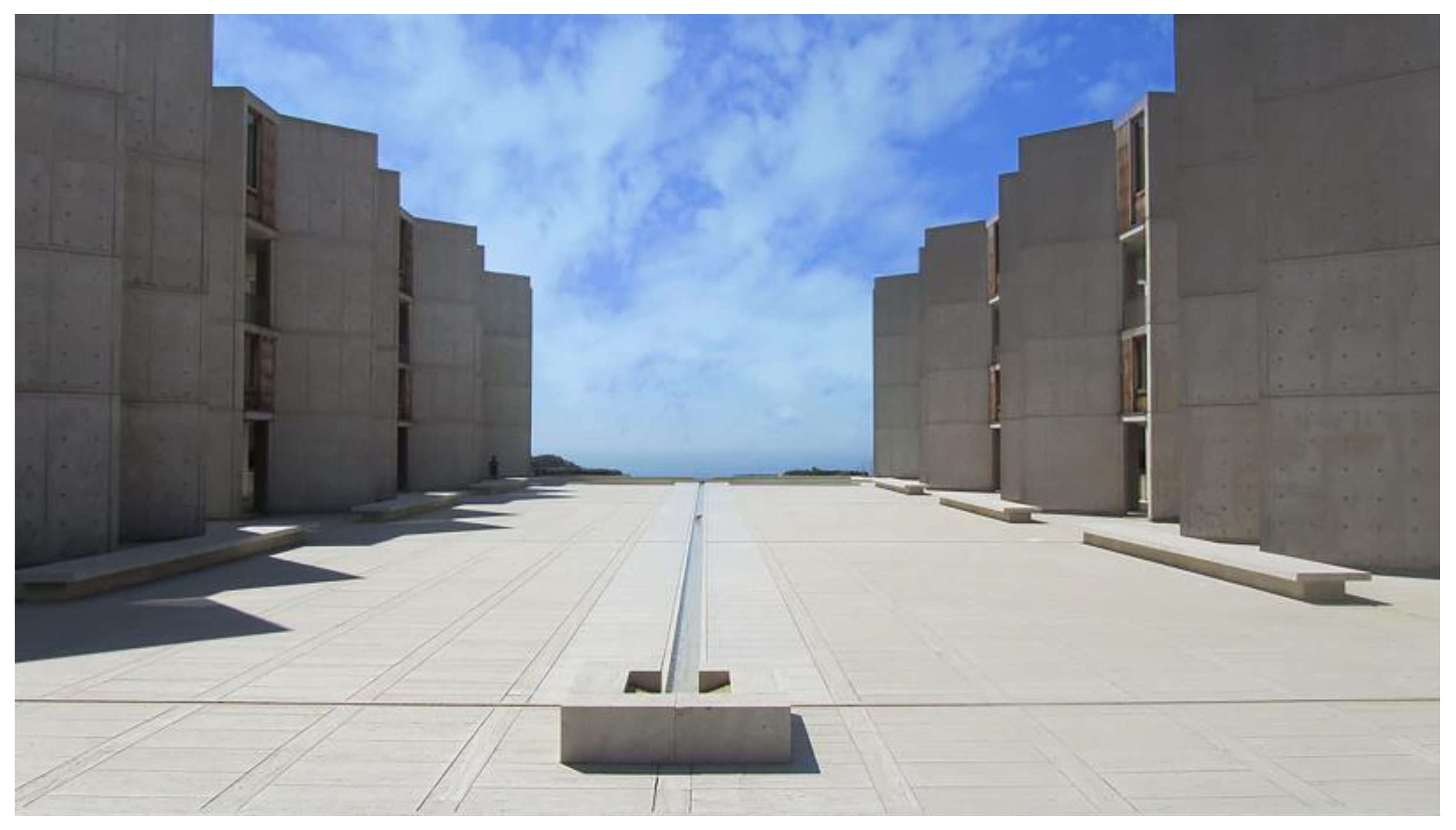
In parallel with these urban and environmental reflections, from a more sensory, poetic, aesthetic, and phenomenological position, the developer of the polio vaccine, the doctor and researcher Jonas E. Salk, warned of the enormous importance of spaces in which the creative process, ideas, inspiration, and knowledge can flow. With that conviction, in the mid-nineteen-fifties, he commissioned Louis I. Kahn to design and build the Salk Institute for Biological Studies (
Figure 4). Under the premises of that commission, in 1965, the prestigious architect built one of the masterpieces of contemporary architecture, located in San Diego, California. However, above all, he built the first example of the relationship between neuroscience and architecture. The building was designed specifically to promote the most comfortable intellectual and physical conditions, based on what was then believed about the functioning of the human brain.
In 1988, a group of neurobiologists demonstrated that neurons are produced in the hippocampus throughout a human’s lifetime [
14]. Ten years later, Russell Epstein and Nancy Kanwisher discovered that a part of a person’s brain is activated upon perceiving places or awareness of new spaces. The neurobiologist Fred Gage presented a key idea at a conference of the American Institute of Architecture in 2003: changes in the environment change the human brain and, therefore, also modify a person’s behaviour. Thus, a novel interdisciplinary relationship between neuroscience and architecture began, which would eventually bear fruit in the new field of neuroarchitecture [
15,
16,
17,
18].
The relationship between architecture and neuroscience systematises the knowledge acquired with respect to the influence of spaces on people. Above all, this is useful in establishing a scientific method that considers the relationship between them objectively, on the one hand, the built form and the space it generates and, on the other, the person’s cognitive capacities and motivation. Neuroarchitecture studies the functional requirements buildings must meet to promote the development of daily activities, the way people behave in different spaces, and the way different aspects of an architectural environmental influence brain functions, such as stress, emotion, memory, and learning. Its challenge is discovering the way the brain works given certain spatial requirements in order to understand why there are places that promote or inhibit particular emotional states and comprehend the way a person’s habitat affects their mental health, emotional state, and behaviour [
19,
20].
Interest in understanding the influence of space on a person and the reasons why a human feels well in a certain place transcended architecture and transferred to other disciplines, such as sociology and psychology. In his book Health, Stress and Coping, the doctor and sociologist Aaron Antonovsky [
21] proposed a new field of study referred to as “salutogenesis”. This field focuses on the origin of health and the so-called assets of health, which were understood to be a complement to the pathogenic approach. From this perspective, it encompasses the origins of illness and its risk factors. Antonovsky maintained that an environment or space must meet three basic criteria to facilitate a person’s wellbeing. Firstly, it has to be manageable, in that the space must be able to facilitate or manage resources that support the body’s resistance to diseases. Secondly, it must be comprehensible, in that a person can understand the environment adequately. Finally, and most importantly, it must be meaningful; the space must have a meaning or sense recognisable to the people who inhabit and use it [
22].
Illness absence and, from a salutogenic view, health assets have an influence on physical conditions, mental health, and comfort states. From this perspective, the environment is a significant factor, as it can act as a negative stressor, as well as a positive motivator [
23,
24]. Environmental psychology has various points in common with salutogenic theories, given that it holds that there are two factors that guide human preferences with respect to places: understanding and exploration. Understanding is the ability to appreciate the environment through cognitive frameworks. For this, the space must be coherent and legible, in that it must allow its forms to be understood within a certain cultural, historical, or aesthetic context, and it must be possible to perceive its structure and orient oneself within it properly. On the other hand, the exploration factor consists of the ability to expand one’s own capacity to understand the environment and foresee new situations. To explore a place, a variety of unknown components must appear within the environment, as well as an element of mystery, which is the promise of new information following the exploration [
23].
2.3. From US Medical Programmes to the WHO Healthy Cities Network
A space’s influence on humans, in emotional and cognitive terms, is an extremely abstract problem. Therefore, to comprehend them, the research on and projects for people with cognitive deficits are particularly important. The architectural solutions developed for these groups can be extrapolated to all other buildings because of the advantages these also offer society as a whole [
25]. Interest in studying the special needs of people with dementia appeared in the US in the mid-nineteen-sixties, when new care models were developed for patients with cognitive deficits who were confined to psychiatric institutions, until that point in time. The medical programmes “Medicare” and “Medicaid” provided the financial support necessary so those people could reside in centres focused on their cognitive and social needs, not simply on the symptoms of the disease. These places provided specialised care to meet the specific needs of these groups and created personalised surroundings, improving the physical environment in which the residents lived. It was a model of care that progressed very rapidly and that, in the 1980s, stimulated the development of buildings and residences, the design of which considered the emotional requirements of the users for whom they were intended.
The demand for the construction of this new type of care centre led to the publication of various architectural practice guides, with technical and compositional solutions applied to those environments. These publications prescribed measures and criteria for spatial organisation based on the project experience of the architects themselves, as well as on the empirical experiences of the caregivers and workers in the care units. Occasionally, the solutions were based on results obtained in clinical tests and research [
26]. These manuals proposed that an environment intended for people with dementia had to have design guidelines that met safety, orientation, functionality, integration, and personalisation criteria [
27,
28].
Some of these criteria were already being considered in the construction of buildings intended for groups with physical or sensory disorders. However, the novel contribution at that time was the introduction of concepts based on a subjective perception of the space, such as integration or personalisation. To promote and support the autonomy and independence of people with cognitive deficits, Cohen and Weisman [
29] introduced new concepts; support for people to help them perform the instrumental activities of daily life; optimal sensory stimulation within an environment; and the provision of spaces, making it possible to maintain patients’ social bonds with their families for as long as possible. Calkins [
30] argues that person-centred care provides a more cohesive basis for the designer, as it combines the various recommendations and regulations in a more meaningful way. Therapeutic purposes are still inherent in building practice recommendations but are subordinate to higher-level objectives focused on the person and, therefore, entail adaptation and a different hierarchical understanding of the environment.
All of these ideas confirmed the fact that the design of the environment had a direct effect on people with dementia, and they showed no reduced ability to engage in their daily behaviours, in contrast to what is normally associated with the deterioration and progression of the disease. Since then, there has been growing interest in understanding and knowing how and why mental health requires responsible and sustainable environments, providing wellbeing and allowing people to adopt and maintain healthy lifestyles [
31].
The Ottawa Charter, established in 1986, indicated that promoting health consists of providing the population with the means necessary to improve and control it [
32]. One of those means is the environment in which the person lives and works. Beginning with that declaration, various plans emerged promoted by the WHO and were intended to create healthy environments. In the same year, the WHO Healthy Cities Network was created to enhance and protect citizens’ health and wellbeing by interrelating aspects that influence health and political, economic, cultural, social, and environmental sectors. The initiative had laudable intentions, and when its ambitious programmes and recommendations had the necessary funding, its visible effects were seen in cities, and the meanings of abstract concepts such as “friendly”, “resilient”, or “healthy cities” (a description in which a human attribute is applied to an artificial product) were specified and concrete. Finally, it also required particular measures being proposed and conducted by experts in disciplines such as public healthcare, town planning, and architecture.
3. A Hypothesis and Three Contemporary Approaches to Healthy Architecture
The context and background described above allow us to propose the hypothesis that architecture is no longer defined solely by visual or geometrical parameters but also by other materials involving environmental, cognitive, psychological, and physiological aspects. Different environmental indicators and emotional factors define a new type of non-representational space that, despite not being seen, is perceived by the human body. In other words, the expression or representation of space ceases to be strictly formal, compositional, or visual but is able to define, work, or manipulate buildings with other types of quantifiable and measurable healthy parameters or indicators that must be incorporated into the architectural project process.
Although there has never been a specific theory or scientific systematisation related to them, the health-related functional principles that the architectural avant-gardes of the 20th century incorporated into buildings (healthiness, safety, and accessibility) are inescapable today and are, to a great extent, set out in all basic construction regulations. However, in the last thirty years, there has been empirical work in architectural research that has planted a new seed that has borne fruit in a series of buildings. There are examples of architecture focusing on emotional and cognitive aspects, contributing to wellbeing and human health and supplying one more component in this new paradigm of healthy architecture. Centres for individuals with cancer or Alzheimer’s disease and palliative care units have been built in various places around the world that are not focused solely on technical or regulatory aspects. Their attention is centred, in a special way, on the physiological, cognitive, and emotional influences that spaces have on people. These are buildings that have been designed for specific groups of people with illnesses, deficiencies, or particular conditions. However, the findings applied to respond to these physical, mental, and emotional needs provide solutions that, because of their comfort, effectiveness, and usefulness, can be extrapolated to the rest of the population and society. These, therefore, point to a path to follow for the implementation of healthier cities and architecture for the benefit of all [
33]. These empirical experiences and the results that are extracted from them are those that will be used to demonstrate the proposed hypothesis and draw a series of useful conclusions in understanding what healthy architecture means today.
Next, a series of these case studies will be presented that correspond to a classification according to three contemporary approaches to healthy architecture: emotional, psychological, and physiological. On the one hand, for the emotional influence of architecture, Palliative Care Units in France and Maggie’s Centres will be analysed. On the other hand, keeping in mind the environmental cognitive impact, an appraisal will be made of residences intended for people with Alzheimer’s disease. Finally, in regard to their physiological effect on people, a selection of installations is presented.
3.1. Emotional Influence of Architectural Space
One of the main examples is that of the
Unités de Soins Palliatifs (USPs) or Palliative Care Units in France. The first USP, named Paul Brousse, was designed by Avant-Travaux architects and was built in the city of Villejuif in 1988. The challenge the architects who built the USP faced was to design a place that did not remind users constantly of their imminent demise. To do so, they created a material and psychological environment in order to allow patients and their families to enjoy the greatest possible wellbeing while they were in the healthcare institution. Therefore, they included elements that enabled them to express their individuality or sense of belonging by personalising the spaces. Another fundamental feature of USPs is that their architectural language has strong symbolism, so these spaces elicit emotion in the people who visit and reside in them [
34]. This healthcare facility model, intended for a specific group of people, reached maturity in 2006, when the Japanese architect Toyo Ito, winner of the Pritzker Architecture Prize, built a USP at the Cognacq-Jay Hospital in Paris (
Figure 5).
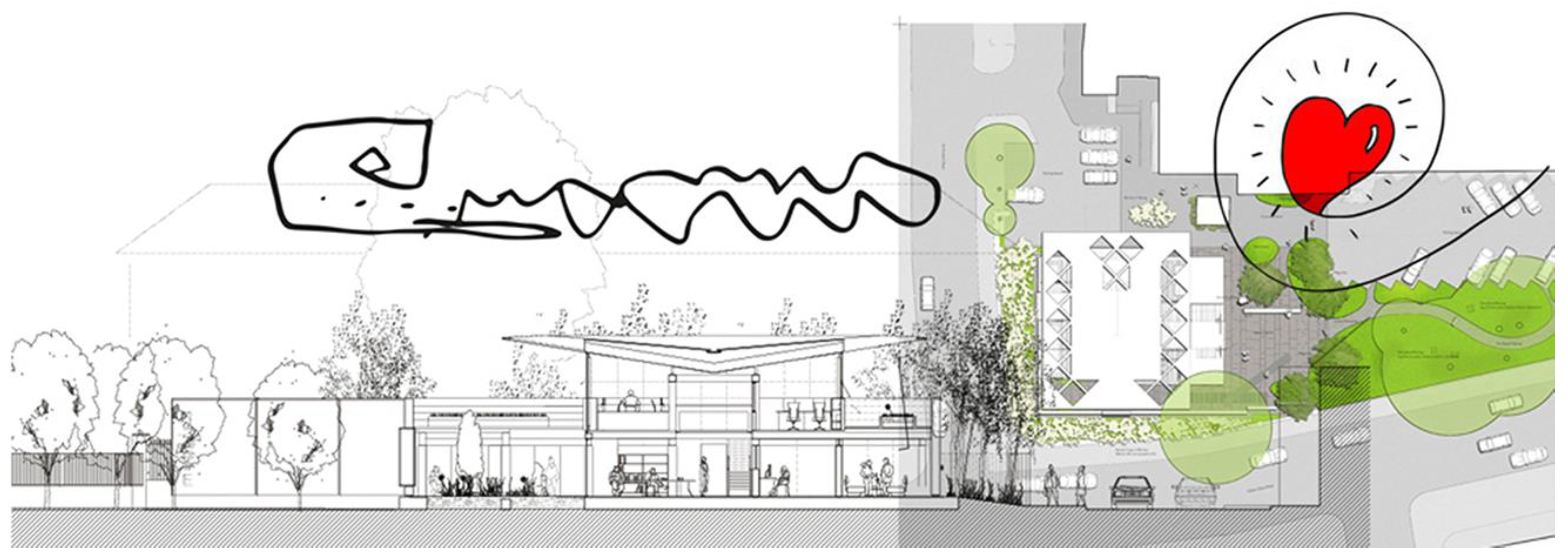
Sometime after the case above, the Maggie Keswick Jencks Cancer Caring Trust network emerged in the United Kingdom. This was an initiative that began with the landscaper Maggie Keswick Jencks based on her own spatial and environmental experiences when she was diagnosed with cancer [
36]. Maggie’s Centres are part of an association that distinguishes itself by providing practical, emotional, and social support beyond medical treatment. These are not only for people with cancer but also for their families and friends in places conceived and designed specifically to meet these individuals’ emotional needs. These centres are positioned as annexes to hospitals and are places where no direct medical treatment is provided.
These buildings are designed by qualified contemporary architects who apply their personal architectural language to the construction. In all of them, one can recognise the power of the idea that produced them and the meaning that architecture brings to a specific place. The architecture of Maggie’s Centres is expressive, artistic, and high quality and creates a sense of space adapted to a certain group’s specific needs. These characteristics lead patients to identify with and have a sense of belonging to a group that enjoys the privilege of using these spaces, as the Centres’ buildings are places worth going to. The first Centre, designed by architect Richard Murphy, was built in 1996 on the grounds of the Western General Hospital in Edinburgh (
Figure 6). Currently, there are twenty-six centres in the United Kingdom, two in Asia, and only one on the European continent, which is adjacent to Sant Pau Hospital in Barcelona, Spain (
Figure 7) [
37].
3.2. Cognitive Impact of the Environment on People
Another case study is the residences intended for those who suffer from Alzheimer’s disease. As with tuberculosis at the beginning of the 20th century, architecture is also now used to alleviate the symptoms of an as-yet incurable disease. Based on American care programmes intended for patients with cognitive deficits, some residences for people with Alzheimer’s disease began to incorporate places for social interactions with the family and other people to arouse recollections of home and stimulate the residents’ memories. The first institution built according to these criteria was the Corinne Dolan Alzheimer Center in Cleveland, Ohio, designed by Taliesin Associated Architects in 1985 [
40].
At the end of the nineteen-eighties, the architectural studio Perkins Eastman developed the Woodside Place residential complex in Oakmont, Pennsylvania (
Figure 8). This building was the beginning of the development of a residence typology for people with Alzheimer’s that includes innovative design guidelines. It was a new type of architecture that had the peculiarity of adapting and personalising spaces for the users for whom it was intended. The small-scaled, small-sized buildings were for a limited number of inhabitants and had well-planned itineraries and routes in a simple arrangement. Consisting of a nucleus of small houses, it recreates the atmosphere of a home and opens to green areas outside. In the buildings’ designs, forms, symbols, and elements are introduced that lead to reminiscence and reference cognitive archetypes, such as gabled roofs, particular types of windows and doors, chimneys, etc. These residences also include spaces intended for caregivers and care services, such as day units, medical centres, or research areas [
41]. This is a new type of building with interesting examples, such as Boswijk, which EGM architects built in Vught, Holland, in 2010 (
Figure 9).
All these experiences—French USPs, Maggie’s Centres, and the new buildings for users with Alzheimer’s disease—include spacious areas with natural light that convey a balanced sensation using scale, proportion, materials, textures, sound, colours, and odours. The arrangement of these spaces focuses on a comfortable place to be in and relax, to have a cup of tea together, or to have an informal conversation, a concept that is far removed from that of traditional hospital settings. Generally, these open to the outside, for example, outdoor spaces that are inserted in the interior of the building, producing the well-known beneficial psychological effect of natural green vegetation. Another important aspect is that all buildings “care for” the caregivers as well. The spaces these workers use are studied in detail so that they may perform their work with maximum efficiency but, at the same time, relax adequately after the innumerable moments of tension they must experience. This generates a very favourable psychological atmosphere by reducing the emotional distress caused by difficult situations [
42].
3.3. Physiological Architecture: A Novel Approach
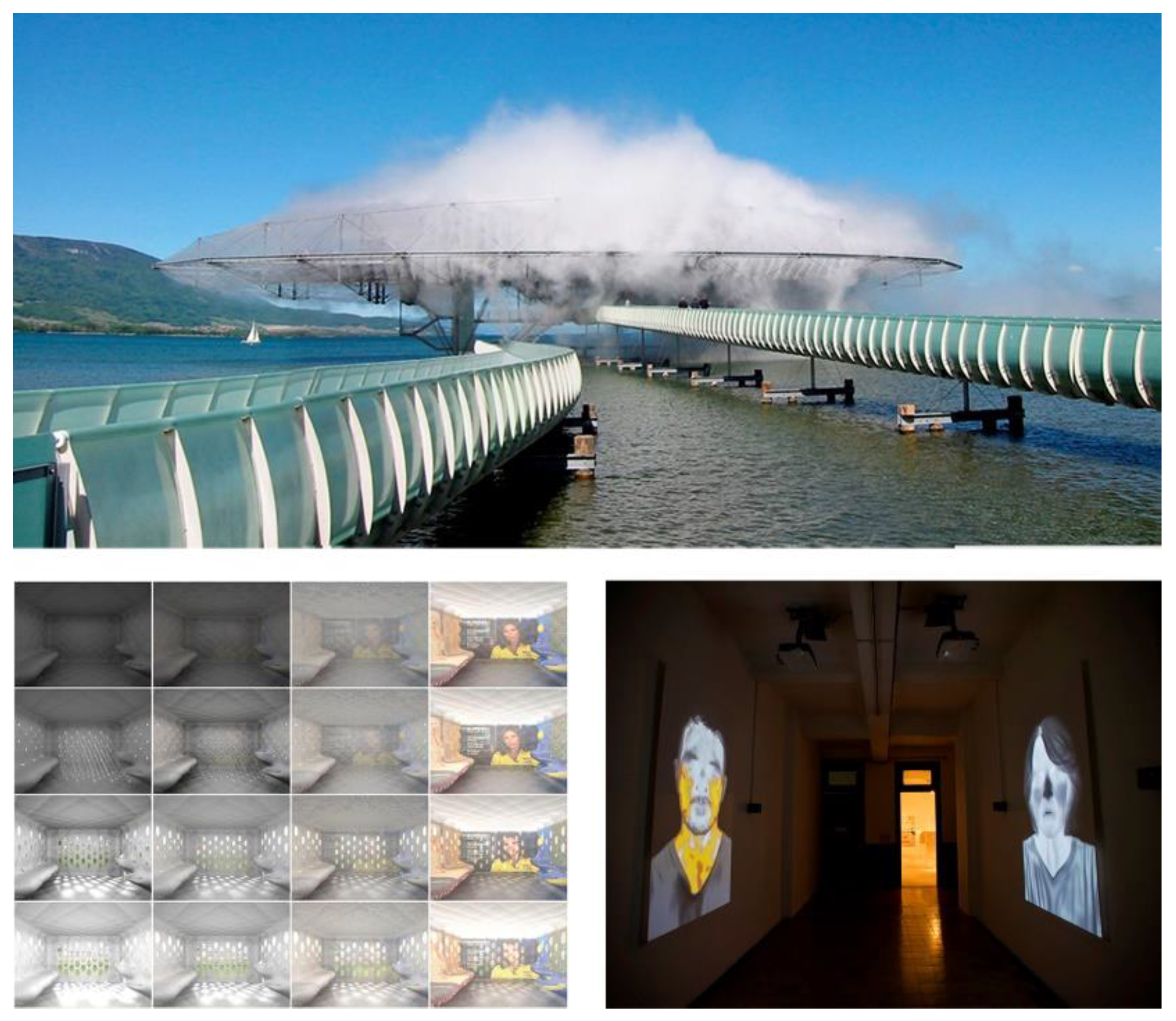
From 2001 onwards, at the same time as the development of the examples described in the previous section, a series of experiments was carried out by various teams of architects. These experiments and tests were presented in installations assembled at exhibitions, biennials, and shows. The aim of these projects was to investigate how space actively stimulates people’s chemical, organic, and emotional mechanisms, effectively influencing their wellbeing.
This line of research was developed in North America by architects such as Elisabeth Diller and Ricardo Scofidio with Renfro (DS+R). On the occasion of the 2002 Swiss National Exhibition, as part of the “Blur” project, this team explored how the construction of an artificial atmosphere can encourage the use of the senses to generate collective experiences to improve the perception of the environment [
43]. Later, in an installation presented in 2008 at the Sandreto de Rebaudengo Foundation in Venice 2008, they created an experimental montage based on virtual reality, entitled “Does the Punishment Fit the Crime?”. In it, they analysed the sensations produced by a person after being locked up in a cell, designed according to the crime they had committed [
44]. Their investigations continued with the installation ‘Unspoken’. This installation, presented in 2016 at the Third Istanbul Biennial, studied the process of people blushing when they pass through an enclosure purposely designed to produce this emotion [
45] (
Figure 10).
However, it was the Swiss team of architects Décosterd and Rahm who proposed the novel concept of physiological architecture. This is a new paradigm based on the principle that the phenomena sustaining life are constantly determined by physicochemical conditions. Depending on their presence, absence, or intensity, these constitute some of the main causes that influence a human being’s dwelling and wellbeing [
45]. According to Philippe Rahm, the way in which human beings deal with the sensations of inhabiting can be translated into five different actions: 1. Atmospheric, by changing the temperature through natural or artificial conditioning systems. 2. Physiological, by drinking hot or cold drinks or food. 3. Social, by changing clothing. 4. Physical, by resting to adapt the body to the environment. 5. Neurological, by stimulating a feeling of freshness within the mind through taste and smell activators.
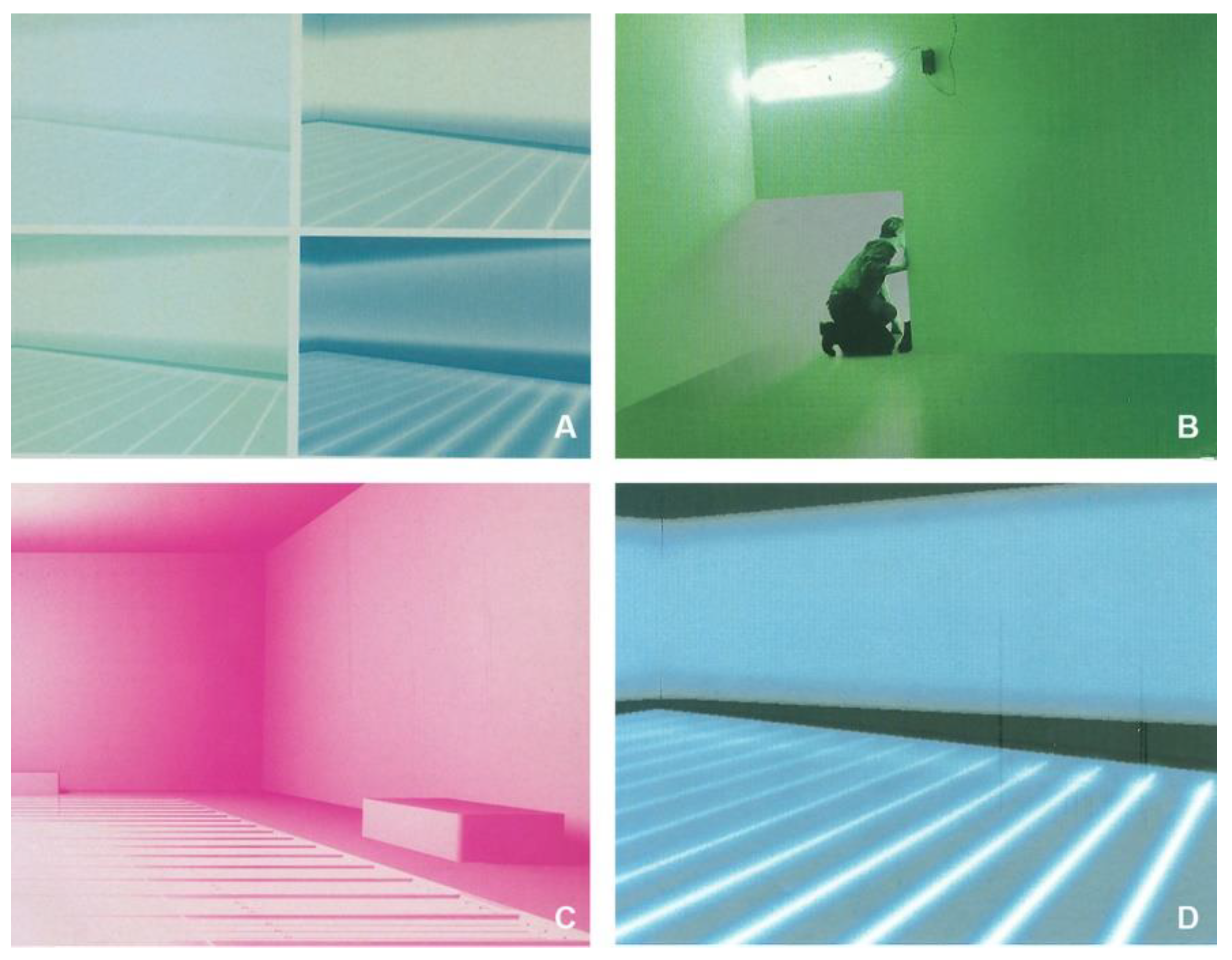
This team of Swiss architects has developed its experimental work based on this intangible or invisible dimension of architecture with research that they carried out at installations and assemblies created in art galleries, first at the Arteplage of Expo 01 in Switzerland, on the beaches of Lake Neuchâtel, and later at the MoMA in San Francisco. In their installations, which they significantly termed Melatonin Room, the Hormonarium, or Paysage électromagnétiques, among others, they investigated the influence of different stimuli generated in specific spaces on human beings. Taim directed architectural research towards the characterisation of space and its physiological impact on human metabolism via the design and implementation of certain parameters.
The Melatonin Room installation consisted of a space for hormone stimulation, distributed in two consecutive rooms connected to each other, which could be accessed independently. This produced two alternating climates. The first was defined by the emission of electromagnetic rays at 509 nm with an intensity of 5000 lux, which suppressed the production of melatonin in the pineal gland. The space thus became a physically stimulating, motivating, and chemically exciting place. The second climate, with green light mimicking the diffusion of ultraviolet rays in a natural environment, stimulated the production of melatonin and thereby became a relaxing place. The Melatonin Room was a non-representational space that acted on the chemical mechanisms of the human organism [
46].
The
Hormonorium was another proposal for the design of a new public space. It was a space climatically defined by light, temperature, and air quality, all parameters that involve the body. The
Hormonorium was an assembly of physiological devices that acted on the endocrine and neurovegetative systems of the human body. It was built with a luminous floor made of plexiglass to allow ultraviolet light to pass through using 528 fluorescent tubes; these emitted a white light that reproduced the solar spectrum, with UV-A and UV-B. This inverted radiation, emitted from the ground, meant the light radiation was not blocked by eyelids, eyelashes, or the natural inclination of the head. This very bright light, between 5000 and 10,000 lux, stimulated the retina and transmitted information to the pineal gland, which caused a decrease in the secretion of melatonin. In lowering the level of this hormone in the body, this environment made it possible to experience a decrease in fatigue and regulation of mood [
46] (
Figure 11).
Philippe Rahm continued this line of work with a study of the alterations that hormonal balance exerts on the quality and ways of life. He designed the installations Noctambulisme, Diurnisme (2007), and Digestible Gulf Stream (2008). In the latter, he set out to imitate the physical principles of the Gulf Stream to build a habitable space based on a natural climate with changing atmospheric conditions, thus freeing it from the sophisticated and expensive technical solutions of artificial thermal conditioning.
4. Results: A Decalogue That Leads towards Healthy Architecture
The common denominator in all of the previous case studies is the creation of healthy environments. However, their principal contribution has been the construction of spaces with a comprehensible and recognisable meaning, helping to improve the emotional balance of the people who use them. In those experiences, all of the buildings provide spaces with a strong identity so that those who use them, whether healthy or sick, recognise and, moreover, feel welcome in their relaxed and non-institutional environment (
Figure 12).
In addition to the visual and tangible spatial qualities, the physiological architecture approach, offered by the exhibitions depicted above, takes into consideration the influence of electric, sound, magnetic, and thermal flows existing in today’s environments. This establishes a new geography that, like any location determined by a given amount of energy, can be measured and mapped through the corresponding electric, magnetic, or climatic energy emissions. This means a contemporary space is the result of capturing or mapping the environment through the data produced by the radiation of these flows. A new spatial dimension emerges, an ambience defined by parameters with various non-metric magnitudes that nevertheless delimit environments and irremediably alter and affect human metabolism. These environments are physical and cognitive stimulators for people, as well as natural, sociological, and cultural conditions that significantly interfere with the basic and instrumental activities of daily life.
From here, architecture enters the field of physical action, leaving its strict formal function to confront the limits of space. Architecture becomes physiological, acting on the corporeality of the air and the human body without intermediaries. It is like a forcefield, the fire of a bonfire, which, when released, unfolds the conquest of space and sets in motion various sources of energy, such as heat, light, or wavelengths, necessary and essential for balance in people’s metabolism. The habitable place thus becomes a modified and modifiable environment, a field without precise limits into which the human body enters and where its organs establish a physiological relationship.
Research by the European Network for Brain Evolution Research and the University of Bath found that, in addition to promoting wellbeing, well-planned environments have a positive effect on decisions and people’s personalities [
48]. That research highlights the fact that, depending on the experience the space produces, the environment may be understood differently, interfering with aspects such as familiarity, the relationship with the location, or even social relationships. A certain space can affect the quality of a person’s spatial and social cognition, which implies that inhabiting certain environments may have either harmful or beneficial effects. For instance, some places and spaces, such as underground parking, airports, and malls, cause particular cognitive symptoms like stress, spatial and temporal disorientation, anxiety, fear, etc. As seen above, these are reactions to which people with cognitive deficits, such as Alzheimer’s, autism, etc., are more prone.
There are also physical reactions to specific surroundings that are better known than cognitive and psychological reactions. These are symptoms seen in some people when they remain in certain buildings continually, the so-called Sick Building Syndrome (SBS). Symptoms consist of a suite of ailments that include headaches; eye, nasal, and buccopharyngeal discomfort; lethargy; allergies; etc. This syndrome was first noticed in the mid-1970s in offices and schools. It has varied aetiologies, from the building’s formal design (e.g., some of them are hermetically sealed and have large glass surfaces) to artificial climates or construction with unhealthy materials, such as lead, asbestos, or fibrillary insulation. SBS is also caused by products and installations that release carbon monoxide, sulphur dioxide, ozone, or even carbon dioxide, which people themselves exhale in an enclosed environment. In general, it is the result of a method of building that generates and continues to emit environmental, electrical, magnetic, and chemical pollution. To combat the symptoms of SBS, in 2017, the Harvard T.H. Chan School of Public Health proposed a series of points, or criteria, that must be controlled to achieve a healthy level in a building [
49]. Its document omits some important factors, as it does not mention the impact that spaces and environments have on the cognitive component of people.
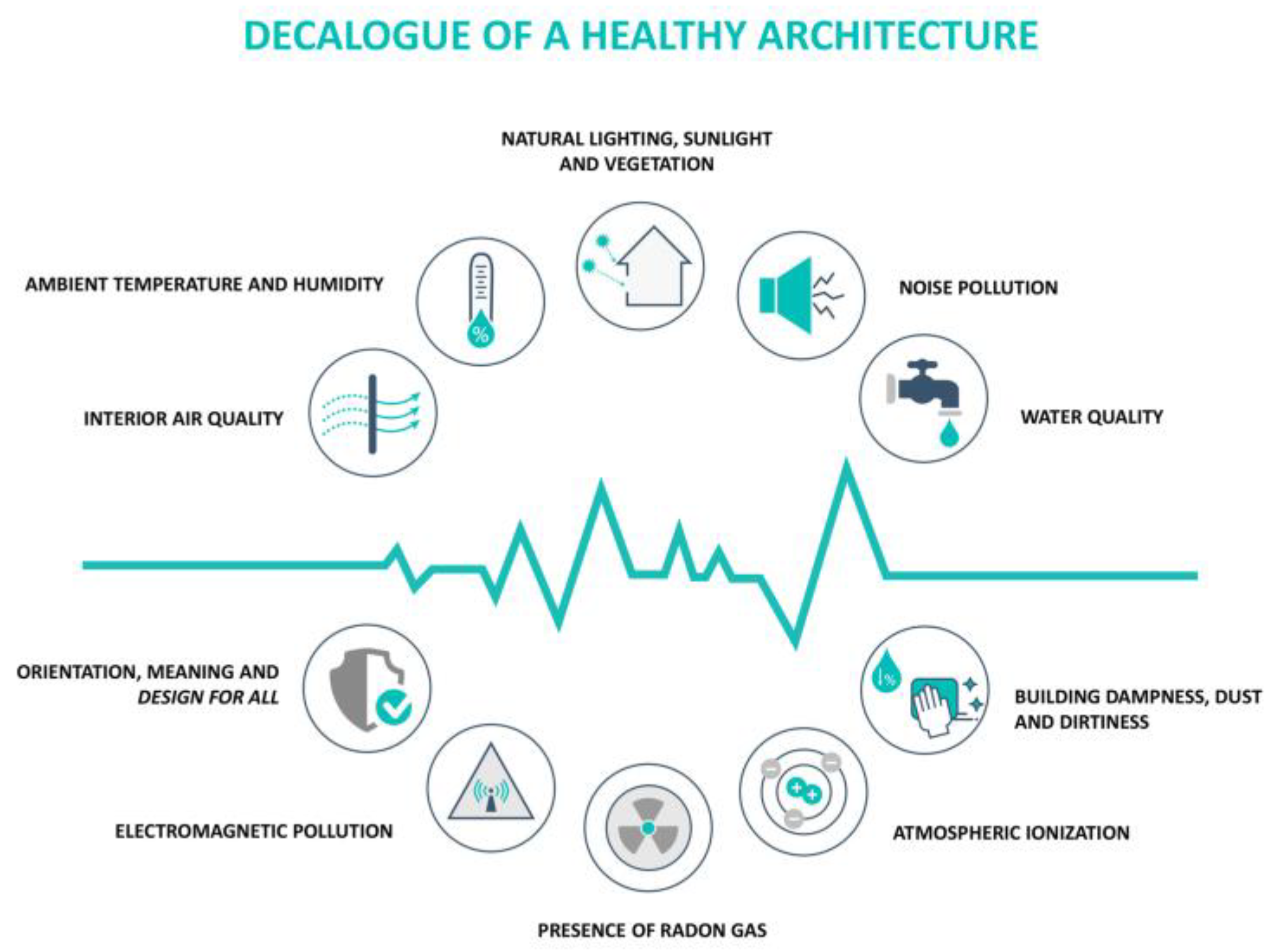
Based on the previous background, analyses of international architectural experiences and examinations of experiments centred on physiological architecture concepts, the Healthy Architecture & City Research Group at the University of Seville proposed a comprehensive list of ten control indicators for use in the construction of healthy buildings. There are nine environmental factors that influence sensory, physical, and cognitive aspects simultaneously, as well as a final, more abstract and holistic factor related to the meaning, orientation, organisation, and distribution of space (
Figure 13).
These issues are important to human health and are set out below:
Interior air quality (IAQ). The most effective way to control air quality is through adequate and essential natural ventilation in all spaces. Air quality is perceived largely by the nose upon breathing and by the eyes and skin. The body’s combined reaction determines whether the air is perceived to be fresh and pleasant or foul and irritating. To guarantee air quality, both natural ventilation and the choice of construction materials must be borne in mind. These should be innocuous and emit few volatile organic compounds, and the absence of pollutants such as lead, polychlorinated biphenyls, and asbestos, among others, should be verified.
Ambient temperature and humidity. The relationship between these parameters is very important for wellbeing, as the homeostasis of the human body depends upon these, among other factors. It is necessary to take measures to ensure indoor habitats and workplaces have a combination of temperature and humidity that is constant throughout the year. There are no constant, comparative parameters that can be applied around the world, as the sensation of comfort depends upon the climatic and geographic conditions of each location. It is, therefore, essential to establish a local range of optimum levels.
Natural lighting, sunlight, and green spaces. Indoor spaces should have as much natural light as possible to maintain visual comfort, but not dazzle. Moreover, spaces are needed that provide a certain number of hours of sunlight per day. An effort must be made to provide visual lines from the interior to the exterior and to introduce a view of areas with vegetation or open green spaces. This factor has a special effect on people’s mental and emotional wellbeing.
Noise pollution. It is important to control unwanted noise pollution by protecting and insulating indoor rooms from outside noise. It is also necessary to monitor internal noise sources that may be irritating, such as mechanical equipment, electrical appliances, air-conditioning, or even a neighbour rehearsing for a forthcoming concert.
Water quality. Contaminants must be removed from drinking water as much as possible. To do so, in addition to the actions that suppliers are considering already, it is desirable to install domestic purification systems. Water stagnation in drains, buildings, and outdoor spaces must be prevented, as well as stagnant water in wells, puddles, etc., as these serve as breeding grounds for pests. As it is necessary to limit the use of pesticides and chemical products in pest control, it is better to avoid attracting them by eliminating where they live whenever possible.
Dampness and dirt in buildings. It is essential to prevent the build-up of dampness attributable to capillarity, condensation, or infiltration, as its existence promotes the presence of fungi and bacteria that are harmful to health. Materials that, because of their characteristics and distribution, can cause adverse reactions and allergies must also be eliminated.
Atmospheric ionization. Clean air is usually negatively ionized and an adequate percentage of negative ions contributes to a sensation of wellbeing. Air in cities is normally charged with positive ions, similar to air in the interior of buildings. The negative ion concentration in air is reduced by air flowing through metal ducts, tobacco smoke, static electricity produced by synthetic fibres, and human activities. This condition has been related to discomfort, lassitude, stress, and the loss of mental and physical capacity. Hence, maintaining an adequate number of negative ions in the environment is another factor to consider.
The presence of radon gas. Radon (Rn) is a natural gas produced by the decay of radium in the uranium-238 radioactive decay chain. It is present in the Earth’s crust and is water soluble, so radon can be found anywhere, although it is most commonly found in granite soils and in those containing uranium ore. Construction materials such as phosphogypsum or blocks manufactured with pieces of granite may also produce radon. The gas penetrates up to a maximum height of one meter via natural diffusion through joints between materials, cracks, or the passage of pipes, and hence, it is necessary to prevent it from concentrating. It is also essential to comply with the safety standards set out by the regulations for fire safety, the detection of carbon monoxide, etc.
Electromagnetic pollution. Although numerous studies have been performed in relation to electromagnetic fields (EMFs), it has not yet been possible to prove, with scientific evidence, that the consequences of prolonged exposure to the fields of high-voltage lines, telephone antennae, domestic electrical appliances, and/or workplace equipment are the cause of the fatigue, stress, or depression related to SBS. In all events, as a preventive measure, it seems important to plan and project this essential contemporary infrastructure at the right distances from residences and workplaces and also to have the necessary insulation.
Meaningful space with a holistic approach, clear orientation, rational distribution, and maximum safety. These are the compositional, symbolic and formal resources, supplying architectural spaces with meaning, in order to transcend their primary function. This generates comprehensible places where a narrative value, as well as a sense of belonging, can be found by the inhabitant. The connections with the symbolic and highly codified culture are reconstructed by architecture; thus, the habitat, in addition to being a shelter and a relief, is a cognitive appendix for the human being [
50]. Also, the standards of design for all or universal design must be met, bearing in mind full accessibility for people with functional diversity: physical, sensory, and cognitive.
5. Discussion of a New Paradigm in the Design and Construction of Buildings
As has been shown previously, interaction with the environment defines what people are capable of and the way they characterise themselves. The physical environment is identified as a definite place, with a specific organisational structure used for precise functions within the social field, where humans live and interact with each other. It is composed of a complex, artificial epidermis that surrounds a person’s habitat. This third skin, which completes that of the body itself and its textile covering of clothes, is designed and configured by architecture.
A certain spatial configuration can affect aspects of both physical health and human behaviour, positively or negatively. Perception is not solely limited to visual elements but is also formed with the other senses and cognition. The surroundings’ physical and environmental features also influence spatial perceptions. The effect of a space depends on the degree of control, understanding, and sense of coherence the person can experience within it, aspects that memory, culture, training, beliefs, and individual preferences can determine.
Nevertheless, designers do not always pay attention to the potential effect a space can have on people’s health, and the solutions are not usually applied to construction today. One of the reasons, as well as the main limitation of this framework, is that there is still a lack of literature and scholars who focus on this topic; its impact has been uneven until very recently. Moreover, another barrier to the implementation of this paradigm is that the few solutions proposed and the scant regulations that exist to promote healthy architecture are focused on physical aspects, and all of them are from a pathogenic point of view. The need for contributions responding to emotional and cognitive environmental influences is inescapable. It is important to establish a systematisation of key patterns from a salutogenic point of view.
As we have seen, the stimuli affecting human sensations function both internally and externally. They accumulate gradually within the body and mind and offer an information feedback system that leads people’s basic needs either to be satisfied or not [
51]. There are external stimuli, such as sound, smell, light, flavour, and temperature. These are detected by the five classic senses, which have their specific dispositions, and there are also multisensory stimuli, such as air quality, chemical agents, electromagnetic fields, noise, solar radiation, etc. These are detected by more than one sense and can have an effect on the body as a whole. All of these greatly influence a person’s degree of comfort, quality of life, and wellbeing and can promote human health. However, they may also cause a loss of physical or cognitive abilities and illnesses. Physical and cognitive stimuli are present in all different forms of environments. If they are positive, it may be desirable to integrate them, and if they are negative, they must be eliminated because they can produce pathogenic agents.
The main contribution of this theoretical work is to establish the basis for the creation of a novel and new healthy architecture epistemology, focussing on cognitive, emotional, and physiological stimuli. Therefore, the final point of the Decalogue is the one to spotlight, as it offers a salutogenic perspective on planning, design, and construction, with a holistic approach taking into account the positive aspects of the environment. Additionally, this paper provides a series of issues, definitions, and data with which to ask new questions, opening a potential path to continue research and filling in the gaps until this healthy architecture doctrine is developed.
6. Conclusions: A Definition of Healthy Architecture
Architecture is the art of creating the best living conditions for humans by building spaces that elicit emotions. “Healthy” is an attribute that expresses the quality of the architecture. Healthy architecture builds environments that improve wellbeing and increase people’s physical and cognitive capacities, thus generating assets that reduce risk factors and facilitate, enhance, and promote human health. It is a new paradigm based on five principles: 1. Building with harmless materials, zero emissions, and no environmental footprint. 2. Integrating emerging communication and information technologies safely and ethically. 3. Generating and having clean, efficient, and smart environments. 4. Designing environments that are adaptable and compatible with the development of a diversity of lifestyles. 5. Eliciting emotion with deeply meaningful architecture.
The way to address these matters, which are particularly important for people’s health, does not seem to be through expensive technological solutions designed to create or perpetuate artificial environments and climates. It is a question of meeting the challenge with another way of thinking, thus applying a new model. Architecture has effective tools and resources to do this. It is able to use materials that can be recycled, control energy saving in buildings, conserve energy sources, and monitor products’ ecological footprints. It is also able to build by adapting to the environment’s climatic conditions and exploiting the sun’s energy by capturing, accumulating, and controlling radiation processes to achieve natural heating and ventilation.
Building healthy environments with the materials available to architecture requires delving into the stimuli that their spaces generate and designing them in an intelligent and integrated manner. Thus, the third skin that envelops the human habitat is able to generate physical and cognitive stimuli in people. This is both in their memory and in the way they experience and live in a space that enhances their wellbeing, comfort, and quality of life. Delimiting, configuring, organising, and designing an environment and, above all, generating positive sensory experiences are projective actions that determine a space’s value and significance [
52]. This approach provides the basis of an alternative model to resolve problems and advance the knowledge necessary to have unequivocally healthy cities and architecture.
Healthy architecture involves an attitude in which, during the design and construction processes, the harmful elements that may appear during use, ageing, or demolition are eliminated. The materials and techniques to be used are chosen because of their positive effects on the environment, climate, or ecology. The solutions are adapted to the place, such that the minimum possible power supply is required to ventilate, heat, cool, or light the environment. However, healthy architecture’s primary differentiating feature is that it considers the parameters that influence people physically and cognitively. A design oriented towards people’s health produces social, economic, and environmental benefits. At the same time, it generates added value in planning cities and produces sustainable contexts and environments that conform better with the current demands of society. Everywhere people live and work—homes; residents’ associations; factories; offices; and the city itself—must be a healthy environment.
The inhabitants of a hyper-connected society know perfectly well what is beneficial for them: what foodstuffs they must or must not consume; what activities are best for their physical fitness; and the importance of both their physical and psychological conditions. The same is true of materials, spaces, environments, and cities. Humans have always surrounded themselves with what they consider most beneficial for their health. Looking after the environment and oneself offers significant, long-term savings for users, companies, authorities, and the state, as this prevents certain problems from reaching the hospital setting.
It is more cost-effective to invest in an architectural building design that considers health indicators and parameters, both physical and mental, than to retroactively resolve the harm their absence causes. One must understand, plan, and build the spaces where everyday life takes place to produce a balanced set of stimuli with assets that reduce risk factors and promote people’s health. After efficient, green, and sustainable architecture, a new paradigm has emerged that contemporary society demands should be implemented: healthy architecture.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}












