
A Conceptual Framework to Promote the Transition to Positive Mental Health among Young Construction Workers

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Research Methods
3. Theoretical Background
3.1. Transitions Theory
3.1.1. Background and Key Assumptions
3.1.2. Constructs of Transitions Theory
3.2. The Dual-Continuum Model of Mental Health
3.2.1. Background
3.2.2. Domain Concepts of Positive Mental Health
3.3. Reasons for the Selection of Transitions Theory and the Dual-Continuum Model
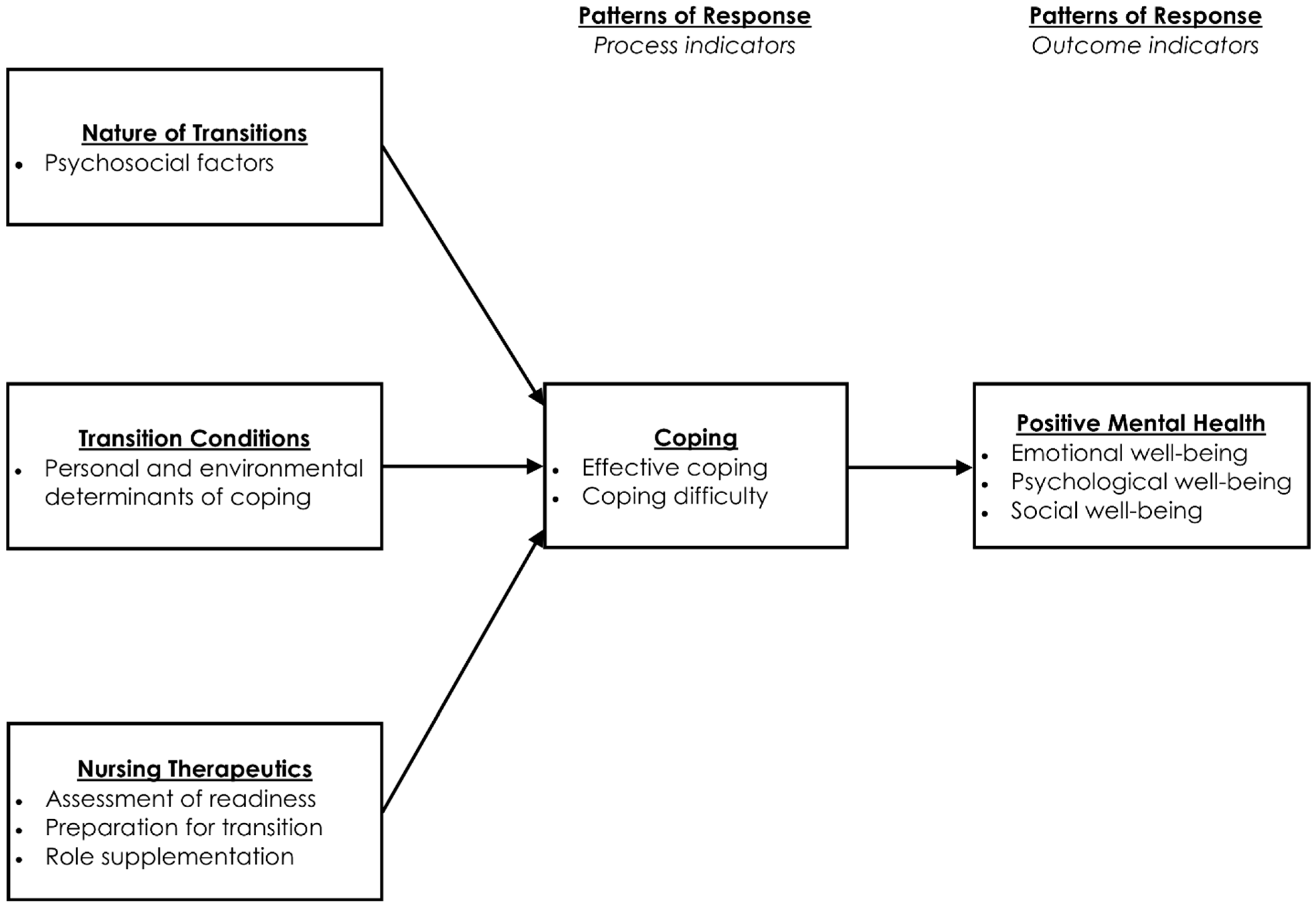
4. Proposed Conceptual Framework
5. Evaluation of Framework
5.1. Clarity and Consistency
5.2. Generalisability
5.3. Simplicity
5.4. Accessibility
5.5. Importance
6. Discussion of Framework and Development of Propositions
6.1. Nature of Transitions
6.2. Transition Conditions
6.3. Nursing Therapeutics
6.4. Patterns of Response
7. Conclusions and Recommendations
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lancet Psychiatry. Embracing a positive view of mental health. Lancet Child Adolesc Health 2021, 5, 767. [Google Scholar] [CrossRef] [PubMed]
- United Nations Children’s Fund (UNICEF). The State of the World’s Children 2021: On My Mind—Promoting, Protecting and Caring for Children’s Mental Health; UNICEF: New York, NY, USA, 2021. [Google Scholar]
- Keyes, C.L.M. Promoting and protecting positive mental health: Early and often throughout the lifespan. In Mental Well-Being: International Contributions to the Study of Positive Mental Health; Keyes, C.L.M., Ed.; Springer: Dordrecht, The Netherlands, 2013. [Google Scholar] [CrossRef]
- Milner, A.; Law, P. Summary Report: Mental Health in the Construction Industry; MATES in Construction: Spring Hill, Australia, 2017. [Google Scholar]
- Hutton, E.A.; Skues, J.L.; Sullivan, J.A.; Wise, L.Z. Mental health research in the global construction industry: A scoping review using a dual-continuum model of mental health. Ment. Health Prev. 2022, 28, 200249. [Google Scholar] [CrossRef]
- Frimpong, S.; Sunindijo, R.Y.; Wang, C.C.; Boadu, E.F. Domains of Psychosocial Risk Factors Affecting Young Construction Workers: A Systematic Review. Buildings 2022, 12, 335. [Google Scholar] [CrossRef]
- Dong, X.S.; Brooks, R.D.; Cain, T.R. Overdose Fatalities at Worksites and Opioid Use in the Construction Industry; Quarterly Data Report (Fourth Quarter, 2019); The Center for Construction Research and Training (CPWR): Silver Spring, MD, USA, 2019. [Google Scholar]
- International Labour Organization [ILO]. Improving the Safety and Health of Young Workers; International Labour Office: Geneva, Switzerland, 2018. [Google Scholar]
- Pidd, K.; Duraisingam, V.; Roche, A.; Trifonoff, A. Young construction workers: Substance use, mental health, and workplace psychosocial factors. Adv. Dual Diagn. 2017, 10, 155–168. [Google Scholar] [CrossRef]
- Meleis, A.; Sawyer, L.; Im, E.-O.; Messias, D.H.; Schumacher, K. Experiencing transitions: An emerging middle-range theory. Adv. Nurs. Sci. 2000, 23, 12–28. [Google Scholar] [CrossRef]
- Meleis, A.I. Transitions Theory: Middle Range and Situation Specific Theories in Nursing Research and Practice; Springer Publishing Company: New York, NY, USA, 2010. [Google Scholar]
- Keyes, C.L.M. Mental illness and/or mental health? Investigating axioms of the complete state model of health. J. Consult. Clin. Psychol. 2005, 73, 539–548. [Google Scholar] [CrossRef] [Green Version]
- Efird, D.; Stoneham, T. What is the Principle of Recombination? Dialectica 2008, 62, 483–494. [Google Scholar] [CrossRef]
- Lewis, D. On the Plurality of Worlds; Basil Blackwell: Oxford, UK, 1986. [Google Scholar]
- Torraco, R.J. Writing integrative literature reviews: Guidelines and examples. Hum. Resour. Dev. Rev. 2005, 4, 356–367. [Google Scholar] [CrossRef]
- Im, E.-O. Theory Development Strategies for Middle-Range Theories. Adv. Nurs. Sci. 2018, 41, 275–292. [Google Scholar] [CrossRef]
- Chick, N.; Meleis, A.I. Transitions: A nursing concern. In Nursing Research Methodology; Chinn, P.L., Ed.; Aspen Publication: Boulder, CO, USA, 1986; pp. 237–257. [Google Scholar]
- Schumacher, K.; Meleis, A. Transitions: A central concept in nursing. Image J. Nurs. Scholarsh. 1994, 26, 119–127. [Google Scholar] [CrossRef]
- Benner, P. From novice to expert. Am. J. Nurs. 1982, 82, 402–407. [Google Scholar]
- Kislov, R.; Pope, C.; Martin, G.P.; Wilson, P.M. Harnessing the power of theorising in implementation science. Implement. Sci. 2019, 14, 103. [Google Scholar] [CrossRef] [Green Version]
- Joly, E. Transition to adulthood for young people with medical complexity: An integrative literature review. J. Pediatr. Nurs. 2015, 30, e91–e103. [Google Scholar] [CrossRef]
- Im, E.O. Theory of transitions. In Middle Range Theory for Nursing, 3rd ed.; Smith, M.J., Liehr, P.R., Eds.; Springer: Berlin/Heidelberg, Germany, 2014; pp. 253–276. [Google Scholar]
- Meleis, A.I. Transitions theory. In Nursing Theories and Nursing Practice, 4th ed.; Smith, M., Parker, M., Eds.; F. A. Davis Company: Philadelphia, PA, USA, 2015; pp. 361–380. [Google Scholar]
- Munck, B.; Björklund, A.; Jansson, I.; Lundberg, K.; Wagman, P. Adulthood transitions in health and welfare; a literature review. Nurs. Open 2018, 5, 254–260. [Google Scholar] [CrossRef] [Green Version]
- Messias, D.K.H. Narratives of Transnational Migration, Work, and Health: The Lived Experiences of Brazilian Women in the United States. Ph.D. Thesis, University of California, San Francisco, San Francisco, CA, USA, 1997. [Google Scholar]
- Im, E.O. Neglecting and Ignoring Menopause within a Gendered Multiple Transitional Context: Low Income Korean Immigrant Women. Ph.D. Thesis, University of California, San Francisco, San Francisco, CA, USA, 1997. [Google Scholar]
- Sawyer, L.M. Engaged Mothering within a Racist Environment: The Transition to Motherhood for a Group of African American Women. Ph.D. Thesis, University of California, San Francisco, San Francisco, CA, USA, 1997. [Google Scholar]
- Meleis, A.I.; Trangenstein, P.A. Facilitating transitions: Redefinition of the nursing mission. Nurs. Outlook 1994, 42, 255–259. [Google Scholar] [CrossRef]
- Keyes, C.L. The mental health continuum: From languishing to flourishing in life. J. Health Soc. Behav. 2002, 43, 207–222. [Google Scholar] [CrossRef] [Green Version]
- Keyes, C.L.M.; Martin, C.C. The Complete State Model of Mental Health. In Wellbeing, Recovery and Mental Health; Cambridge University Press: Cambridge, UK, 2017; pp. 86–98. [Google Scholar] [CrossRef]
- Westerhof, G.J.; Keyes, C.L. Mental illness and mental health: The two continua model across the lifespan. J. Adult Dev. 2010, 17, 110–119. [Google Scholar] [CrossRef] [Green Version]
- Seligman, M.E. Flourish; Free Press: New York, NY, USA, 2011. [Google Scholar]
- Diener, E. Subjective wellbeing. Psychol. Bull. 1984, 95, 52–575. [Google Scholar] [CrossRef]
- Ryff, C.D. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J. Personal. Soc. Psychol. 1989, 57, 1069–1081. [Google Scholar] [CrossRef]
- Keyes, C.L.M. Social well-being. Soc. Psychol. Q. 1998, 61, 121–140. [Google Scholar] [CrossRef]
- Gallagher, M.W.; Lopez, S.J.; Preacher, K.J. The hierarchical structure of well-being. J. Personal. 2009, 77, 1025–1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryff, C.; Keyes, C.L.M. The structure of psychological well-being revisited. J. Personal. Soc. Psychol. 1995, 69, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Flaskerud, J.H.; Winslow, B.J. Conceptualizing vulnerable populations health-related research. Nurs. Res. 1998, 47, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Dyrbye, L.N.; Harper, W.; Moutier, C.; Durning, S.J.; Power, D.V.; Massie, F.S.; Eacker, A.; Thomas, M.R.; Satele, D.; Sloan, J.A.; et al. A multi-institutional study exploring the impact of positive mental health on medical students’ professionalism in an era of high burnout. Acad. Med. 2012, 87, 1024–1031. [Google Scholar] [CrossRef]
- Grant, F.; Guille, C.; Sen, S. Well-being and the risk of depression under stress. PLoS ONE 2013, 8, e67395. [Google Scholar] [CrossRef]
- Huppert, F.A.; So, T.T. Flourishing across Europe: Application of a new conceptual framework for defining well-being. Soc. Indic. Res. 2013, 110, 837–861. [Google Scholar] [CrossRef] [Green Version]
- Keyes, C.L. Mental health as a complete state: How the salutogenic perspective completes the picture. In Bridging Occupational, Organizational and Public Health; Bauer, G.F., H’ammig, O., Eds.; Springer: Dordrecht, The Netherlands, 2014; pp. 179–192. [Google Scholar]
- Keyes, C.L.; Dhingra, S.S.; Simoes, E.J. Change in level of positive mental health as a predictor of future risk of mental illness. Am. J. Public Health 2010, 100, 2366–2371. [Google Scholar] [CrossRef]
- Weiss, M.B.; Piacentine, L.B.; Lokken, L.; Ancona, J.; Archer, J.; Gresser, S.; Holmes, S.B.; Toman, S.; Toy, A.; Vega-Stromberg, T. Perceived readiness for hospital discharge in adult medical-surgical patients. Clin. Nurse Spec. 2007, 21, 31–42. [Google Scholar] [CrossRef] [Green Version]
- Chan, A.P.C.; Nwaogu, J.M.; Naslund, J.A. Mental Ill-Health Risk Factors in the Construction Industry: Systematic Review. J. Constr. Eng. Manag. 2020, 146, 04020004. [Google Scholar] [CrossRef]
- Sun, C.; Hon, C.K.H.; Way, K.A.; Jimmieson, N.L.; Xia, B.; Wu, P.P. A Bayesian network model for the impacts of psychosocial hazards on the mental health of site-based construction practitioners. J. Constr. Eng. Manag. 2023, 149, 04022184. [Google Scholar] [CrossRef]
- Tijani, B.; Jin, X.; Osei-kyei, R. A systematic review of mental stressors in the construction industry. Int. J. Build. Pathol. Adapt. 2021, 39, 433–460. [Google Scholar] [CrossRef]
- Frimpong, S.; Sunindijo, R.Y.; Wang, C.C.; Boadu, E.F.; Dansoh, A.; Fagbenro, R.K. Coping with psychosocial hazards: A systematic review of young construction workers’ practices and their determinants. Buildings 2023, 13, 22. [Google Scholar] [CrossRef]
- Australian Institute for Suicide Research and Prevention [AISRAP]. Report on the Construction Industry Apprentices’ Focus Groups; Report for Mates in Construction and Griffiths University; Griffith University: Brisbane, Australia, 2018. [Google Scholar]
- Broadbent, R.; Papadopoulos, T. Improving mental health and wellbeing for young men in the building and construction industry. J. Child Adolesc. Ment. Health 2014, 26, 217–227. [Google Scholar] [CrossRef]
- Doran, C.; Rebar, A.; Waters, K.; Meredith, P. A Review of the Evidence Related to the Impacts of, and Interventions for, Workplace Bullying in the Construction Industry; Mates in Construction: Spring Hill, Australia, 2020. [Google Scholar]
- King, T.L.; Batterham, P.J.; Lingard, H.; Gullestrup, J.; Lockwood, C.; Harvey, S.B.; Kelly, B.; LaMontagne, A.D.; Milner, A. Are young men getting the message? Age differences in suicide prevention literacy among male construction workers. Int. J. Environ. Res. Public Health 2019, 16, 475. [Google Scholar] [CrossRef] [Green Version]
- Turner, M.; Mills, T.; Kleiner, B.; Lingard, H. Suicide in the construction industry: It is time to talk. In Proceedings of the Joint CIB W099 & TG59 International Safety, Health, and People in Construction Conference, Cape Town, South Africa, 11–13 June 2017; p. 45. [Google Scholar]
- Flannery, J.; Ajayi, S.O.; Oyegoke, A.S. Alcohol and substance misuse in the construction industry. Int. J. Occup. Saf. Ergon. 2019, 27, 472–487. [Google Scholar] [CrossRef]
- Fordjour, G.A.; Chan, A.P.C. Exploring occupational psychological health indicators among construction employees: A study in Ghana. J. Ment. Health Clin. Psychol. 2019, 3, 6–18. [Google Scholar] [CrossRef]
- Zhang, S.; Sunindijo, R.Y.; Frimpong, S.; Su, Z. Work stressors, coping strategies, and poor mental health in the Chinese construction industry. Saf. Sci. 2023, 159, 106039. [Google Scholar] [CrossRef]
- Chinn, P.L.; Kramer, M.K. Description and critical reflection of empiric theory. In Knowledge Development in Nursing: Theory and Process, 9th ed.; Chinn, P.L., Kramer, M.K., Eds.; Mosby: Maryland Heights, MO, USA, 2015; pp. 186–209. [Google Scholar]
- Li, L.; Strachan, P.H. Transitioning to adult services for youth with medical complexity: A practice issue viewed through the lens of transitions theory. Nurs. Sci. Q. 2021, 34, 301–308. [Google Scholar] [CrossRef]
- Lamers, S.M.; Westerhof, G.J.; Bohlmeijer, E.T.; ten Klooster, P.M.; Keyes, C.L. Evaluating the psychometric properties of the Mental Health Continuum-Short Form (MHC-SF). J. Clin. Psychol. 2011, 67, 99–110. [Google Scholar] [CrossRef]
- Schwartz, L.A.; Daniel, L.C.; Brumley, L.D.; Barakat, L.P.; Wesley, K.M.; Tuchman, L.K. Measures of readiness to transition to adult health care for youth with chronic physical health conditions: A systematic review and recommendations for measurement testing and development. J. Pediatr. Psychol. 2014, 39, 588–601. [Google Scholar] [CrossRef] [Green Version]
- Baird, M.B. Resettlement Transition Experiences among Sudanese Refugee Women. Ph.D. Thesis, University of Arizona, Tucson, Tucson, AZ, USA, 2009. [Google Scholar]
- Nwaogu, J.; Chan, A.; Hon, C.; Darko, A. Review of global mental health research in the construction industry: A science mapping approach. Eng. Constr. Archit. Manag. 2019, 27, 385–410. [Google Scholar] [CrossRef]
- Frimpong, S.Y.; Antwi, A.B.; Boateng, E.S.; Hagan, J.A.; Mensah, P.A. The State of Youth Health in Ghana’s Construction Industry; Participatory Development Associates (PDA) Ltd.: Accra, Ghana, 2021. [Google Scholar]
- Gaffney, K.F. Nursing practice model for maternal role sufficiency. Adv. Nurs. Sci. 1992, 15, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Tilki, M. The social contexts of drinking among Irish men in London. Drugs: Educ. Prev. Policy 2006, 13, 247–261. [Google Scholar] [CrossRef]
- Kane, J.J. Allowing the novice to succeed: Transitional support in critical care. Crit. Care Nurs. Q. 1992, 15, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Turner, M.; Lingard, H. Examining the interaction between bodily pain and mental health of construction workers. Constr. Manag. Econ. 2020, 38, 1009–1023. [Google Scholar] [CrossRef]
- Ammad, S.; Alaloul, W.S.; Saad, S.; Qureshi, A.H. Personal protective equipment (PPE) usage in construction projects: A scientometric approach. J. Build. Eng. 2021, 35, 102086. [Google Scholar] [CrossRef]
- Ammad, S.; Alaloul, W.S.; Saad, S.; Qureshi, A.H. Personal Protective Equipment (PPE) usage in Construction Projects: A Systematic Review and Smart PLS Approach. Ain Shams Eng. J. 2021, 12, 3495–3507. [Google Scholar] [CrossRef]
- Bowen, P.; Govender, R.; Edwards, P. Structural equation modeling of occupational stress in the construction industry. J. Constr. Eng. Manag. 2014, 140, 04014042. [Google Scholar] [CrossRef]
- Chen, Y.; McCabe, B.; Hyatt, D. Impact of individual resilience and safety climate on safety performance and psychological stress of construction workers: A case study of the Ontario construction industry. J. Saf. Res. 2017, 61, 167–176. [Google Scholar] [CrossRef]
- Scott-Young, C.M.; Turner, M.; Holdsworth, S. Male and female mental health differences in built environment undergraduates. Constr. Manag. Econ. 2020, 38, 789–806. [Google Scholar] [CrossRef]
- Fernando, S.; Moodley, R. Global Psychologies: Mental Health and the Global South; Palgrave Macmillan: London, UK, 2018. [Google Scholar]
- Joshanloo, M. Mental well-being in Iran: The importance of comprehensive well-being in understanding the linkages of personality and values. In Mental Well-Being: International Contributions to the Study of Positive Mental Health; Keyes, C.L.M., Ed.; Springer: Dordrecht, The Netherlands, 2013. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Construct | Components | Study Variables | Exemplar Studies |
|---|---|---|---|
| Nature of transitions | Types | Personal, socio-economic, and organisational/industrial domains of psychosocial factors | [6,45,46,47] |
| Patterns | |||
| (what the transition looks like) | Properties | ||
| Transition conditions | Personal | Personal, socio-cultural, and organisational/industry determinants of young construction workers’ coping strategies | [48] |
| Community | |||
| (what makes the transition easier or difficult) | Societal | ||
| Nursing therapeutics (care strategies) | Assessment of readiness | Assessment of mental health literacy | [49] |
| Preparation for transition | Educational interventions (professional and mental health) | [50,51] | |
| (other peoples’ actions aimed at ensuring a healthy transition process) | Role supplementation | Role model interventions for workplace and non-workplace support | [52,53] |
| Patterns of response | Process indicators | Effective coping (adaptive) | [48,54,55,56] |
| Coping difficulty (maladaptive) | |||
| (actions that signify the progress of a transition and a healthy transition outcome) | Outcome indicators | Positive mental health (emotional, psychological, and social) | [3,12] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frimpong, S.; Sunindijo, R.Y.; Wang, C.C.; Boadu, E.F.; Dansoh, A. A Conceptual Framework to Promote the Transition to Positive Mental Health among Young Construction Workers. Buildings 2023, 13, 1025. https://doi.org/10.3390/buildings13041025
Frimpong S, Sunindijo RY, Wang CC, Boadu EF, Dansoh A. A Conceptual Framework to Promote the Transition to Positive Mental Health among Young Construction Workers. Buildings. 2023; 13(4):1025. https://doi.org/10.3390/buildings13041025
Chicago/Turabian StyleFrimpong, Samuel, Riza Yosia Sunindijo, Cynthia Changxin Wang, Elijah Frimpong Boadu, and Ayirebi Dansoh. 2023. "A Conceptual Framework to Promote the Transition to Positive Mental Health among Young Construction Workers" Buildings 13, no. 4: 1025. https://doi.org/10.3390/buildings13041025