1. Introduction
Health and medicine are important areas of sociological specialization, but they are facing rapid global challenges [
1]. The vital themes in the sociology of health and medicine are changes in the demographics and their behavior [
2]. Understanding the association between healthcare facility design and patient experience have become crucial [
3]. Therefore, the potential of health sociology is not limited to the fields where it stands “naturally”—social sciences—but also applies to other areas, such as city and community planning, environmental studies, and sustainable development [
4]. Hence, the sociology of health and illness has gained the attention of many scholars not just from the lens of the built environment, but also from the experiences of patients and visitors [
4,
5]. It is argued that the design of healthcare buildings should consider a healing environment and visitors’ well-being [
5,
6]. Multiple design factors are often associated with positive healthcare experience [
6,
7] and the development of therapeutic environments in hospital settings [
7,
8]. Regarding healing architecture, there are advanced features of recent healthcare building design that positively influence treatment outcomes in the sick parts of the body. These features are, for example, using colored LED light, an internal garden, colored poster glass for the walls and ceilings in the operation room, wall paints to absorb humidity and provide odor control, modern library space, etc. However, this relationship still needs further examination for advanced impacts, especially how these positive outcomes could be maintained [
9,
10]. Additionally, the design and clinical practices lead to positive healing outcomes through relieving stress, reducing noise, supporting internal hope, and connecting with the spiritual atmosphere [
11].
Contemporary organizations are increasingly emphasizing sustainability by incorporating a triangle of three dimensions, namely economic, environmental, and social, when making ethical management decisions about corporate development and growth [
12,
13,
14]. Sustainable management in healthcare projects is the practice of managing a firm’s role in the triple bottom lines—people, planet, and profit—so that the three aspects can be sustained in the future [
15,
16]. Sustainable development in healing and healthcare contexts includes environmental, social, and economic dimensions. Green healthcare refers to the incorporation of ecological practices in service delivery. It has many benefits economically, socially, and environmentally [
17,
18]. Examples of economic benefits are the reduction of costs and the provision of eco-friendly products and services. Examples of the social benefits are stimulating occupants’ healing and well-being. Moreover, examples of environmental benefits are maintaining the ecosystem and saving resources.
Healing architecture is a characteristic of recent healthcare-facility design [
19]. Healing architectures positively impact patient well-being and transform psychiatric services [
20]. Thus, healing architecture in hospitals can influence patient experiences. However, it is confirmed that there is limited awareness of how healing architecture shapes clinical and patient outcomes [
21]. Healing architecture is a significant issue because it offers a crucial intervention in the relationship between the architectural design of the built environment and the health outcomes. The term “healing architecture” is a specific discipline of the healing environment for healthcare buildings that investigates the influence of the environment content on patients’ healing and recovery process. This highlights the value of space design in creating healing and positive outcomes [
22,
23].
The hospital design for medical and non-medical spaces can help improve a patient’s recovery situation and well-being, as well as relieve staff stress [
24]. Architectural structures, including interior and exterior design, should consider visitors’ needs and create a positive experience [
25]. It describes the physical ethos of the ward as a latent message of expectations for improving patient satisfaction, creating a positive self-image, and its influence on the staff’s mood and behavior [
26,
27]. The interior design features for healthcare well-being and healing include medical and non-medical furnishings. The finished materials and color schemes of the patient’s room have an impact on their healing and well-being [
28]. Some implications, such as unit design, should accommodate the competing goals of stimulating patients. Moreover, functional areas should be differentiated through music, color, lighting, flooring finish, wall design, natural plants, and furnishings [
29,
30,
31,
32].
The current research aims to ensure an appropriate healing environment in healthcare projects. The research focuses on interior architectural finishing materials through a newly developed assessment tool for interior design materials. This research adopted this newly developed assessment tool on a teaching hospital of 400 beds as the research case study. The guiding research questions for the current study is as follows: how can interior finishing materials and color be enhanced with healthcare sustainability standards? The current study addresses a gap in the literature concerning the availability of an integrated approach to ensure a proper healing environment. There are several international standards for ensuring green building and its sustainability, such as LEED and WELL. However, it is difficult to adopt several standards, especially with some repetitions between standards. Hence, the current research develops an integrated assessment tool for ensuring healing environment and sustainability in healthcare buildings. The assessment tool was developed by integrating the LEED healthcare standards, WELL building standards, and the chromotherapy method. The integration of these two well-known standards with chromotherapy method in one single assessment tool ensure the provision of green buildings and a healing environment. This tool will cover interior design and finishing materials. The developed tool supports decision makers, interior designers, and client committees to identify the compatible interior materials specifications with healing environment to meet the expectations of building users such as patient, staff, and visitors.
2. Literature Review
Some studies (e.g., [
6,
7]) have highlighted the value of an evidence-based design approach to healthcare architecture by focusing on the challenges of implementing the findings of studies in building design. Evidence-based design is constructing a building process or physical environment based on scientific research to achieve the best possible outcomes. Evidence-based design is used in architecture, interior design, landscape architecture, facilities’ management, education, and urban planning. Water et al. [
15] discussed the role of design in creating a unique experience for users and positive energy, which helped in actual healing. However, the same authors [
15] argued that such a design is limited, despite its value in creating sustainable healing. A study by Buffoli et al. [
19] confirmed that it should allow them to embrace the tacit emotions and mental-image knowledge accumulated over time with the surrounding physical environment through their experiences. This research contributes to this debate by providing an assessment tool for ensuring sustainable interior design which would lead to proper healing in healthcare buildings.
A study by Coussens et al. [
20] proposed several geographic views on health and the environment that could create valuable connections between geography and public health via social epidemiology, according to country location, atmosphere, and natural environment. Payne et al. [
26] highlighted some crucial features, such as ambient, interior-design, and social features, which could contribute to patient care and staff functioning. The World Health Organization [
33] stressed the importance of a physically built environment in creating a healing environment in healthcare buildings. Ertz and Patrick [
34] explored the role of evidence-based design, i.e., buildings based on scientific research to receive the best outcomes, in fostering healing at hospitals. Aripin [
35] showed that hospitals should accomplish a specific mixture of physical, aesthetic, social, and symbolic functions. However, it is not an easy task to ensure all of these functions in most buildings. The literature (see, for example, Codinhoto [
36]; Van Den Berg and Wagenaar [
37]) confirmed that a hospital’s design should prioritize the safety of users. Joseph and Rashid [
25] examined the associated materials, products, and chemical used. The research pushes for moving toward a more sustainable approach, which could have better influence on all stakeholders, including users, suppliers, and even the local community. Harris et al. [
38] investigated the relationship between healing architecture and clinical practices, as well as the experience of the patient. Kokulu and Ozgunler [
39] showed the influence of building and interior design on the experience of patients. The transition to green materials encounters challenges through assessing materials specifications as green materials [
13,
40]. It is well approved that interior design not only affects the patients’ experience, but also that of their families and friends when visiting patients in their hospital room [
41].
Prandini [
42] defined a green material as having green chemicals with 12 principles of green chemistry in production, without toxic chemistry, and being healthy to both people and nature. The Green Guide for Healthcare [
42] and Dixit et al. [
43] explained that the Optimal Healing Environment (OHE) framework considers four environments (Internal Environment, Interpersonal Environment, Behavioral Environment, and External Environment) and eight constructs (Healing Intention, Personal Wholeness, Healing Organizations, Healing Relationships, Healthy Lifestyles, Integrative Care, Healing Spaces, and Ecological Sustainability). The healing environment includes both physical aspects and a supportive culture that nurtures the physical, intellectual, social, and spiritual well-being of patients, families, and workers and helps them deal with the pressure of illness and hospitalization [
44]. According to sustainability standards, healing places focus mainly on how different environments affect our physical, mental, spiritual, social, and emotional healing [
45,
46,
47,
48]. Dekkers [
49] illustrated that color scientifically affects the mind, moods, healing, and personal well-being. Rahmanian and Ro [
50] focused on chromotherapy for making harmony and adaptation between the function of medical and non-medical spaces, the patient’s medical situation, and the physiological nature of the color. Gupta [
51] explained the chromotherapy method in healthcare to adopt colors that will help create a good experience. IDS [
52] focused on explaining how chromotherapy treats both physical and emotional problems; affects physical, mental, and spiritual well-being; and stabilizes energy levels in body parts.
This study developed and implemented an assessment tool as a checklist for ensuring the provision of a proper healing architecture environment in healthcare projects depending on LEED healthcare standards, WELL building standards, and chromotherapy. The study built an evaluation tool or matrix for assessing interior finishes that affect the healing environment of healthcare buildings in the case study of KFU’s teaching hospital, as is discussed later in
Section 4.1. The tool ensures that the healing architecture environment fits sustainable healthcare construction projects. The tool was developed based on the consensus of different stakeholders.
3. Healing and Sustainability in Healthcare Projects
3.1. Green Guide and Strategies in Healthcare
The Green Guide for Healthcare [
42] shows how environmental performance can be enhanced in 10 main domains: site selection, water conservation, energy efficiency, recycled and renewable materials, low-emitting materials, alternative transportation, daylighting, reduced waste generation, local and organic food use, and green cleaning materials. Several of these domains should be considered before constructing the building, while they should be during the construction of the operation phase. There is a growing awareness among the leadership of hospital aims to accelerate the adoption of eco-friendly globally [
34]. According to GGH, a green hospital is defined as a hospital that has taken the initiative to do one or more of the following: an environmentally friendly site, sustainable and efficient designs, green building materials and products, green during construction, and keeping the greening process going, a facility that recycles, reuses materials, reduces waste, and produces cleaner air [
6,
35,
40]. Green and eco-friendly hospitals have become a key feature of healthcare design and execution to ensure adaptation to national environmental sustainability policy for health systems and show how organizations can be committed to their environment [
25,
36]. Healthcare organizations must adopt such a policy. This includes dealing with waste and chemicals. Organizations must properly manage their resources and reduce their emissions. A part of their sustainable and eco-friendly practices is prioritizing the prevention of diseases and engaging healthcare staff in the process.
3.2. Benefits of Sustainable Material in Healthcare Facilities
Adopting sustainable materials in healthcare facilities has several benefits, including social, environmental, and economic impacts [
38,
39]. It was confirmed that the products used in construction and operation directly influence users’ health [
8]. Therefore, green healthcare organizations adopt non-toxic products. Additionally, adopting sustainable materials is associated with lower costs [
14,
42]. For example, studies [
12,
41,
44] showed that the delivery rooms, children’s wards, and two hospitals in the USA imply that creating a healing environment requires paying attention to avoiding materials that have negative impacts on the building occupants, and moving to green materials, e.g., switch from vinyl (PVC) flooring plastic to other flooring materials, such as synthetic rubber, polyethylene, and polypropylene as green and sustainable materials. Concepts such as healthier hospitals and green health exchange increasingly adopt sustainable materials to harvest their benefits socially, economically, and environmentally. However, all stakeholders must become involved in this green process implementation. A green material has specific characteristics, such as non-toxic materials and adopting green chemicals. There are some international tools for assessing the green healthcare building, e.g., LEED and WELL. LEED is a holistic system focused on green building elements, such as energy, water, and health; instead, it looks at the big picture, factoring in all critical elements that work together to create the best building possible [
53]. The goal of LEED is to create better buildings that reduce contribution to global climate change, enhance individual human health, protect and restore water resources, protect and enhance biodiversity and ecosystem services, promote sustainable and regenerative material cycles, and enhance community quality of life [
54]. The WELL building standards are a performance-based system for measuring, certifying, and monitoring features of the built environment that impact human health and well-being through air, water, nourishment, light, fitness, comfort, and mind [
49,
53]. The WELL explores the connection between the buildings, health, and wellness of its occupants [
55].
3.3. Healing Environment in the Healthcare Projects
Healing is a dynamic process of recovery, repair, and renewal, enhancing individuals’ and groups’ well-being and spirits [
56,
57]. Research (e.g., [
58,
59]) showed that a healing environment in a healthcare facility could create a positive experience and help patients deal with the pressure of illness. From the institutional side, it could reduce costs in the long term. The proper design of a healing environment should consider some essential aspects [
60]: It should adapt to nature in both interior and exterior design. Moreover, users’ comfort is crucial by reducing any aspect that creates stress for them, albeit creating a good experience [
61].
The concept of the OHE was introduced by the Samueli Institute in 2004. It refers to a healthcare system that is designed to stimulate and support the inherent healing capacity of patients, families, and their care providers [
48]. The OHE framework [
57] considered all stakeholders in the healthcare sector. The framework work aims to enhance healing in healthcare buildings [
58]. The approach considered both the inner and outer environment. One of the modified models of OHE is coined in robust three principles, and its requirements intersect together to achieve the OHE concept: people require wellness, the process requires efficiency, and places require sustainability [
59,
60]; the other modified model of the OHE framework comprises interior, behavioral, and exterior environments. The interior environment includes three components: healing intention, personal wholeness, and healing relationship [
62]. The interpersonal environment should consider healing organization and relationships [
63]. On the other side, the exterior environment should consider ecological sustainability and healing spaces [
64].
4. Research Methods
As discussed earlier, this research aims to enhance healing environments inside healthcare construction projects by adjusting interior design materials and their color with healthcare sustainability standards to be effective for patients’ healing needs. This was undertaken by adopting sustainability standards such as LEED healthcare standards, WELL building standards, and the chromotherapy method. For achieving this purpose, the research adopted a qualitative research approach through in-depth group interviews. Interviewees included engineers who hold an LEED and/or WELL certificate, specialist engineer members in interior design, specialist engineer in green building, members from medical team who has previous experience in healthcare business, and manufacturer and supplier members who participated previously in green building certificate. The interviewee participants in this study exceeded 100 participants. Interviewees were accessed via a personal network of the research team members who are in direct contact with some of the interviewees. Snowballing was also used to recruit other interviewees, as some interviewees were invited through their colleagues. They all were invited to voluntarily participate in the research. The purpose of the interviews was to develop the assessment tool. Two rounds of interviews were conducted to gain the participant consensus regarding the developed tool. The group interviews were administered by the research team, with assistance from experts in qualitative data collection and analysis. The steps that were undertaken to develop and implement the assessment tool are discussed in the next paragraphs.
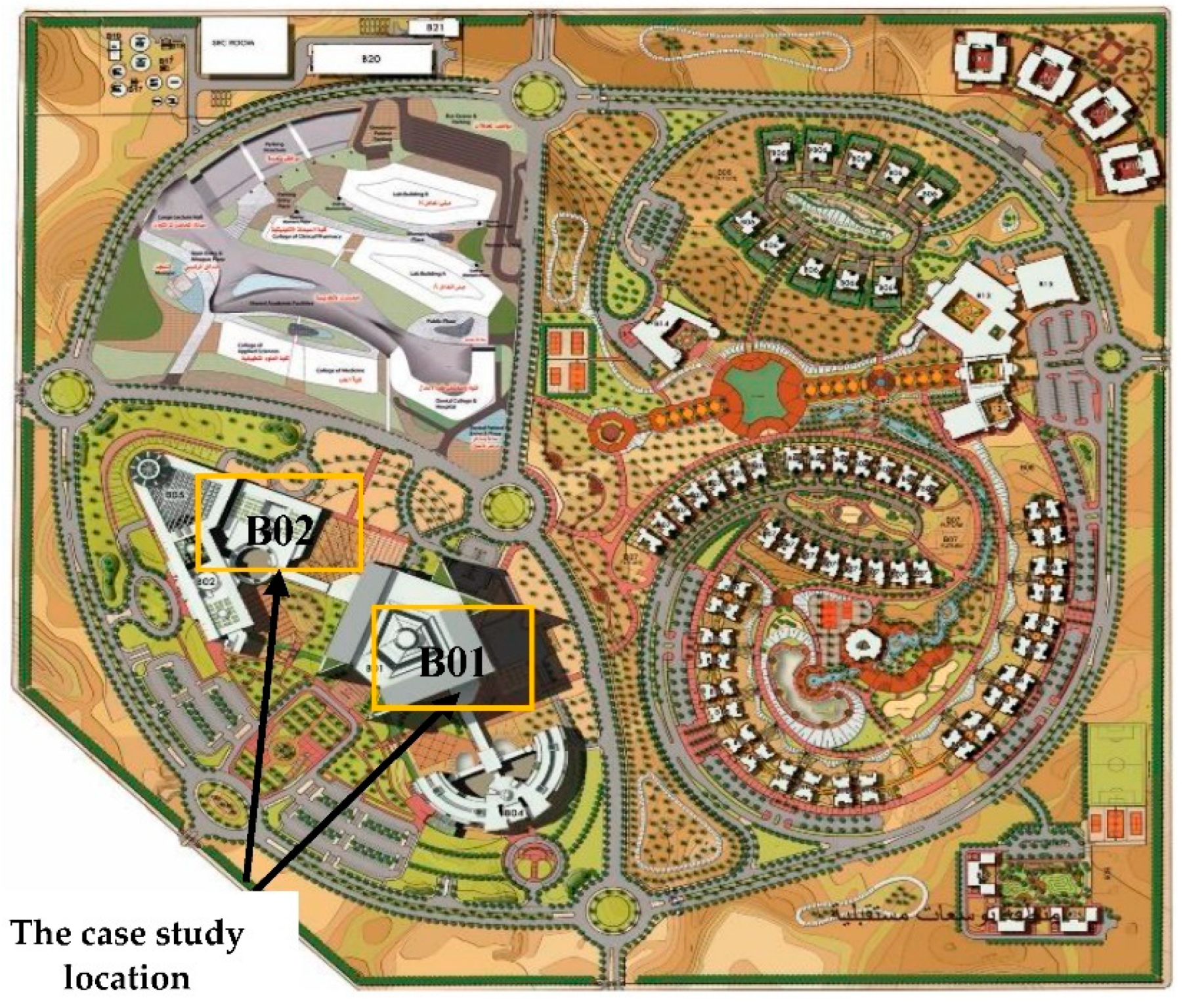
4.1. The Case Study
The current research adopted the KFU Hospital as the case study. The KFU case study was chosen for several reasons. First, the KFU Hospital was an under-construction project during the implementation of research; hence, it was easier for the team to try several things and change this based on experiments and experts’ opinion. Second, it was chosen for pragmatic reasons, as the research team was working at the same university and gained the approval of the leadership to undertake the research. The KFU Hospital is located on the eastern side of Al-Ahsa Governorate at the intersection of Riyadh-Al-Aqeer Road with the Eastern Ring Road. It is located on the main roads with an area of 1,000,000 m
2. The master site plan includes a hospital area, a complex of medical colleges, staff housing, and a service area. The hospital area includes the main hospital building (B01), outpatient clinics building (B02), a physiotherapy center (B03), an oncology and nephrology center (B04), and parking building.
Figure 1 shows the main hospital and outpatient building at the case study location, and
Figure 2 shows the hospital area perspective. It is under construction, with a progress level of 82% as of March 2021, with 400 beds; no. of patients (annually) more than 90,000, main hospital building.
Figure 2 Shows perspective of the hospital area and two buildings, B01 and B02, as a case study. The main hospital building (B01) is a 163,821 m
2 built area and consists of 11 floors containing 11 operating rooms, an X-ray department, thoracic diseases department, cardiology department, obstetrics and gynecology department, classrooms and labs, neonatology department, one-day surgery department, burns department, and ward inpatient rooms. The outpatient building (B02) consists of 4 floors with 29 clinics as follows: basement—car parking; ground floor—orthopedic, diabetes, internal medicine, radiation, psychological, dermatology, dentistry, general surgery, and pharmacy; first floor—nephrology, obstetrics and gynecology, pediatric, thoracic, rheumatology, endocrine, urinary tract, and heart disease; second floor—gastroenterology, plastic surgery, blood diseases, neurosurgery, otolaryngology (ENT), ophthalmology, neurosurgery, and infectious diseases.
Figure 3 shows the construction status for the outpatient building,
Figure 4 shows the construction status for the main building [
65].
4.2. Developing Assessment Tool for the Sustainable Material Finish in Healthcare Projects
Identifying the construction material database used commonly or newly recommended from the international and local manufacturers for healthcare projects with complete specifications is required for these types of projects. The approach is built on LEED healthcare standards, WELL standards, and chromotherapy method as follows. (1) LEED healthcare standards: This is the most used green building rating system, especially for healthcare buildings [
49]. (2) WELL standards: This adopts a holistic approach to health in the built environment [
55]. (3) Chromotherapy method: This is also called color therapy, as it pays sufficient attention to color, which enhances human physical, emotional, spiritual, or mental levels. [
64,
66]. The checklist integrates LEED–WELL–chronotherapy in one assessment tool for the material finish in the healthcare construction market. This range covers all architectural finishes, medical and non-medical loose and mobile furniture, electrical fixtures, and mechanical fixtures to support the LEED–WELL–chromotherapy checklist in a realistic situation [
53,
55].
4.3. The Development of Interior Finishing Material Checklist
The checklist categories specify the suitable criteria to evaluate interior-material alternatives and focus on the effects of the healing environment on the patient’s mental and physical health. This checklist supports choosing specific materials and color schemes in specific spaces in each medical and non-medical department. The research team adopted group interviews with intensive workshops that included interior designers, architects, and sustainability engineers who evaluated materials’ alternatives through the proposed checklist based on achieving the percentage of points from the LEED healthcare categories’ checklist [
54], WELL building standard categories’ checklist [
49], and chromotherapy method. Following these group interviews and workshops, the checklist was submitted in specific mood-board form to the decision-maker to decide, according to the cost and other parameters, the suitable group materials and colors for each hospital department. The sequence of the approach with the main criteria could be explained as follows [
53,
54,
55]. The first checklist criteria were drawn from the WELL building standard checklist 5 credits include 73 points, focusing on the air category, with 29 items; light category, with 7 items; fitness category, with 5 credits; comfort category, with 16 items; and mind category, with 16 items to help practically in prioritizing and selecting the high ranking for each interior material in the floor, ceiling, walls, skirting, furniture, and electromechanical fixtures). The total weight for the WELL checklist is 35 points. The second checklist’s criteria were drawn from the LEED healthcare standards’ checklist, with a total of 40 points containing 3 credits with 11 items, focusing on the energy and atmosphere (EA) category, with 2 items; materials and resources (MR) category, with 4 items; and indoor environmental quality (IEQ) category, with 5 items, to help practically in prioritizing and selecting the high ranking for each interior material in the floor, ceiling, walls, skirting, furniture, and electromechanical fixtures. The third matrix’s criteria were drawn from the chromotherapy method in the healthcare method of color scheme, with a total of 25 points. The criteria focused on making harmony and adaptation between the function of medical and non-medical spaces, the patient’s medical situation, and the physiological nature of the color. The chromotherapy method in healthcare adopts colors, creating a good experience [
67,
68]. The color scientifically affects the mind, mood, healing, and personal well-being [
68]. As well as treating both physical and emotional problems, it affects our physical, mental, and spiritual well-being by stabilize energy levels in body parts [
67].
Table 1 shows the sustainable-material checklist as a guide checklist with complete categories and credits based on LEED categories, WELL categories, and the chromotherapy method in healthcare to be as an evaluation checklist for all material alternatives in interior materials design to support the authorized committee to choose the high-ranking materials adapted with sustainability [
53,
54,
55,
68]. This checklist considers an assessment tool for interior finishes, focusing on sustainability, chromotherapy, and space function. This checklist is built in two steps: one is data register, and the other step is result summation for ranking each material with deserved points.
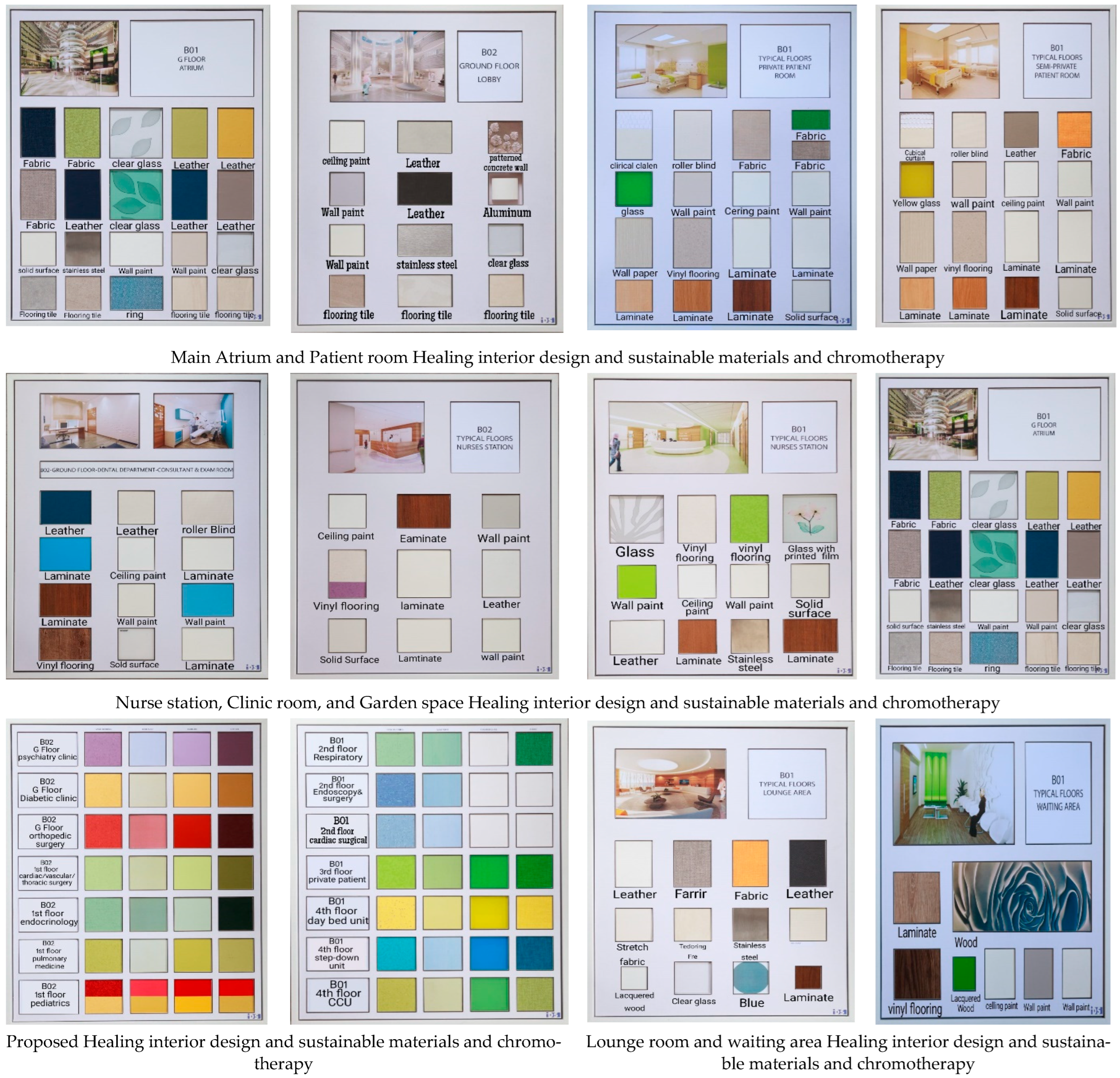
Figure 5 shows the approved mood board according to the interior-finish materials’ adoption-ranking checklist.
Each standard in the checklist has some credits. Each credit has a score or points. The summation calculation of all points equals 100 points (see
Table 1). The research team held several meetings with the official team from medical and KFU representatives to put the weight assessment points for the approach checklist to be rated system contain 100 total weight points and distributed between the three main criteria as follows: (a) WELL building standards, with a total of 35 weight points, containing 6 points for mind, 8 points for air, 8 points for fitness, 5 points for light, and 9 points for comfort; (b) LEED standards, with 40 weight points, containing 10 points for energy and atmosphere, 10 points for materials and resources, and 20 points for indoor environmental quality; and (c) the chromotherapy method has a total of 25 weight points.
The research team undertook several group meetings with the KFU authorization committee, interior designer, and medical specialist to develop and adopt the assessment tool or checklist in the case study. The checklist was adopted in medical and non-medical spaces of the under-construction case study of KFU Hospital. The case study was chosen for pragmatic reasons. Since the research team is based at KFU, the team was able to access the data and implement the checklist for this project. The team started identifying spaces needed in the main building (B01), with 11 floors and 164,000 m2, and in the outpatient building (B02) with 4 floors and 18,000 m2. To adopt the checklist in the case study, the following stages, which were developed by the various experts during the interviews, were undertaken:
Stage 1: Specified the spaces needed to apply the checklist, which reached about 19 operation rooms with an average of 1500 m2, all corridors on average 30,000 m2, all 98-nurse stations with 1600 m2, all staff rooms 160 number with an average of 2000 m2, all atrium spaces 4500 m2, and all 29 clinics rooms with area 600 m2.
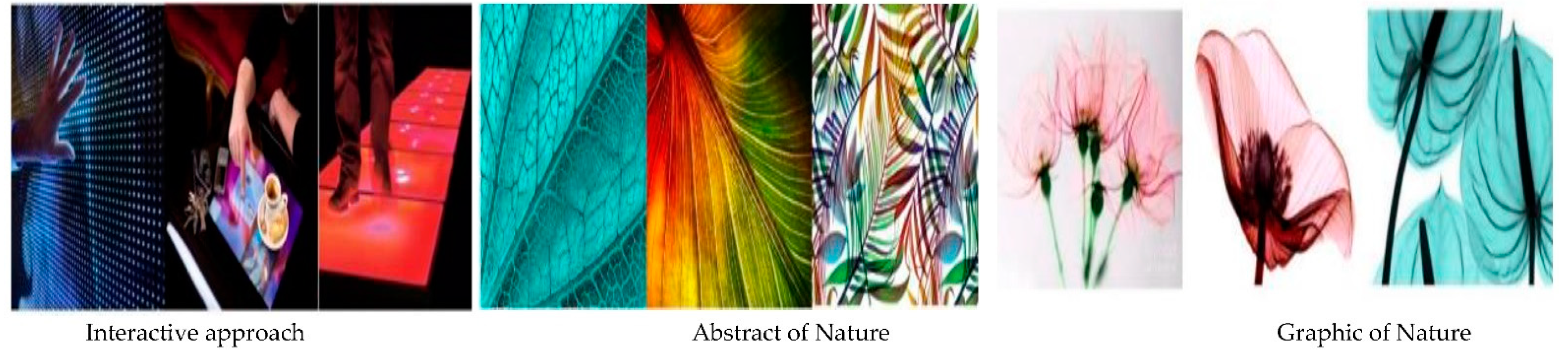
Stage 2: Approved one of the interior design concepts for the specific spaces from the three alternative concepts submitted to the owner committee for approval.
Figure 6 shows the concepts of interior design alternatives.
Stage 3: Proposed several alternative interior finish materials for the floor, ceiling, and walls.
Stage 4: Applied the approach checklist credits and items for each material alternative based on sustainable LEED healthcare standards, WELL building standards, and chromotherapy method. The technical-committee members applied the weight points in the checklist for each space, and each member registered the suitable point in front of each item inside the approach checklist, credits, and items. The team chose the high-ranking points for each material and adapted the color range. Based on the total average points from all members, each material with high-ranking points of more than 70 points was installed in the project for floors, ceilings, and walls.
Stage 5: The contractor arranged all material that gained more than 70 points in complete design as a general mood board for each medical and non-medical space with a complete board for the high-ranking material from Stage 4. These specific interior materials were installed in the project execution processes for the floors, ceilings, and walls.
Figure 5 shows examples of the sustainable approved mood board as a significant result of applying the checklist for architectural and furniture items in the under-construction case study for KFU Hospital. The team adopted the chosen interior concept and achieved a high ranking, with more than 70 points on the checklist of the LEED healthcare standards, WELL building standards, and chromotherapy method. Therefore, the project has become qualified to obtain golden certification in LEED standards and gold certification in optimization with the WELL standard.
5. Results and Discussion
The study achieved significant results in sustainability by adopting the developed checklist (
Table 1), which was developed by integrating the LEED healthcare standards, WELL building standards, and chromotherapy method, for all architectural materials inside an ongoing healthcare project. The significant results were as follows. After adopting the checklist, the case study project was awarded a high ranking in regard to healthcare sustainability-sourced materials and product credit. Additionally, the KFU Hospital can apply for golden LEED certification, which has become easier after applying the assessment tool. The recycled content was more than 40% of the total material. All interior materials are non-structural elements that form more than 55% of the completed building—these materials are manufactured within 500 miles of the case hospital. The case study project fulfilled persistent bioaccumulative and toxic (PBT) chemicals’ reduction and compliance with ASTM B828 2002 and ASTM B813 2010 in mercury in lamps, lead, cadmium, and copper by specifying and using lead-free roofing and flashing, electrical wire, and cable less than 300 parts per million. The paints adopted for the project have no cadmium and use a light-emitting diode (LED). The credits and items of the checklist included furniture components and medical furnishing assembly in the case study project, including finishes, which contain less than 100 parts per million (ppm) of urea-formaldehyde. The heavy metals include mercury, cadmium, lead, and antimony. Stain and non-stick handlings adopted perfluorinated mixtures, including perfluorooctanoic acid.
The case study project had more flexibility in design by providing quiet spaces, using demountable partitions for 50% of the areas, and using movable casework for a minimum of 50%. The furniture and medical furnishings inside the case study project enhance the environmental and human-health-performance attributes by using 40% of the total material with freestanding furniture and medical furnishing products. The environmental tobacco smoke (ETS) inside the case study project was controlled by providing smoking rooms. By adopting the checklist, the case study project reduced building occupants’ potential exposure to hazardous materials, particulates, indoor chemicals, and pollutants, such as asbestos and mercury. All standards used to specify the material specifications in the case study adopted sustainability standards. These standards are (SCAQMD) rule 1113, Environmental Chambers version 1.1 (CDPH/EHLB Standard Method v1.1), ASTM D2369 and D6886, EPA method 24, ISO 11890 parts one and two, National Ambient Air Quality Standards (NAAQS), Occupational Safety and Health Division (Oregon OSHA), American Conference of Governmental Industrial Hygienists (ACGIH), and National Institute for Occupational Safety and Health (NIOSH).
The spaces were designed to support a healing environment based on the checklist according to international sustainability healthcare standards, such as FGI Guidelines 2010 (Facility Guidelines Institute). Therefore, the acoustic environments provided users with sound isolation. The acoustical sound pressure level was (NC) from 20 to 40. The noise-reduction coefficient (NRC) for ceilings was 0.8–0.9, and for walls and partitions, 0.8. In addition, it achieves a visual lighting design, a healthy entrance, and walk-off entryway systems by using a permanent entryway that is suitable for easy cleaning, rollout mats, and material manufactured as a walk-off entryway system. The interior well-being environment, using the checklist, in materials selection followed EN 779-2002 and BS 5228 international specialist standard in the construction IAQ (indoor air quality) management plan during construction. This was undertaken by developing and implementing a moisture-control plan; noise-isolation class (NIC) for occupants that is between 35 and 53, with sound masks between 40 and 48 dB; and humidity control between 30% and 50%, as well as providing individual daylight controls for 90% (minimum) of staff and patients.
The checklist ensured that material selection has become committed to volatile organic compound (VOC) emissions reduction in internal paints, internal adhesives and sealants, flooring, insulation, furniture, and furnishings. This was performed by using VOC content at a minimum of 90% for 100% of the installed products, equaling less than 500 μg/m3; Radon that is less than 4 pCi/Li; and formaldehyde levels that are less than 27 ppb. It meets the standards of the California Air Resources Board (CARB, 2007), Suggested Control Measure (SCM) for architectural coatings; South Coast Air Quality Management District (SCAQMD) Rule 1113; the California Department of Public Health (CDPH) standard method v1.1-2010 for VOC emissions; ASTM D2369-10; ISO 11890, part 1; ASTM D6886-03; ISO 11890-2; ANSI/BIFMA e3-2011; Furniture Sustainability Standard sections 7.6.1 and 7.6.2; and ANSI/BIFMA Standard Method M7.1-2011. The checklist ensured that each material, before the installation process, underwent microbe- and mold-control inspections by using ultraviolet lamps, construction pollution management, and internal liquid water management—the building materials related to condensation management, moisture-absorption management, and dust containment.
The checklist considered visual acuity for focus; brightness-management strategies; melanotic light intensity for work areas; lamp shielding; glare minimization; view window shading; daylight management by blinds controllable by the occupants, e.g., adaptable window shades and lights, which meet with IES-ANSI RP-1-12. The checklist facilitates connecting the building’s outdoor and indoor views with required privacy, facilitative aesthetics with the functional exterior design, pedestrian amenities promotion physical activity spaces, a water fountain or other water feature, wide area atrium plaza with garden and ergonomics visual and physical. There was a consideration of interior fitness circulation by promoting the use of stairs and walking through artwork, including decorative painting, and lighting color quality in the space. This makes users feel more comfortable. Lights met color rendering index Ra CRI, an average of Rr1 through r8) of 80 or higher, light levels of at least 215 lux [20 fc] when the stairs are in use. The thermal comfort, including humidity and airflow, ensured an appropriate comfort for users and followed the standards of ASHRAE, The American Society of Heating, Refrigerating, and Air-Conditioning Engineers. Enhancing familiarity by creating a visually acceptable design merging social and well-being supporting zones positively affects occupants’ moods and comfort levels. The design offers a health and wellness library. The biophilia qualitative features were free of distracting stimuli. This reduces physical and mental stress. The chromotherapy method identified the color scheme for all healthcare departments’ space finish patterns. For example, red is identified for activities of the circulatory and nervous systems, whereas intense pink is to strengthen the vines.
6. Conclusions
Healing architecture could create a positive experience for patients, staff, and visitors. One of the fundamental approaches to ensure this positive experience and create a healing environment is to identify an assessment tool for the interior finishing material in healthcare projects. This study developed an assessment tool integrating two well-identified standards: LEED healthcare and WELL building standards, with chromotherapy method. The developed checklist was applied in the case of the KFU teaching hospital, consisting of 164,000 m2 on 11 floors for the main building and 4 floors of the outpatient building, with 18,000 m2, as a case study. The comprehensive document contains specifications, drawings, and specifically approved mood boards for medical and non-medical spaces’ interior materials, as well as project execution processes. It is interesting how, after adopting the newly developed assessment, the KFU Hospital can obtain golden LEED certification; we consider this to be a significant result of this study. The study advocates for further research on creating a sustainable and healing environment at the healthcare facilities.
The current study focused on developing an assessment tool or checklist for ensuring the use of proper interior finish materials in healthcare projects. The study aimed to ensure sustainability, healing architecture, and well-being integration inside healthcare projects to enhance healing efforts for staff, patients, and visitors inside the healthcare case study project of KFU. The findings have some limitations, as the research was focused on a specific context of a single public university campus in an arid or semi-arid region. However, the research creates an opportunity for further research on healthcare projects concerning the use of healing-environment aspects such as thermal and air quality. Furthermore, the financial side of applying interior design material is an additional research opportunity.












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}



