
Quarantine Hotels: The Adaptation of Hotels for Quarantine Use in Australia


Abstract
:1. Introduction
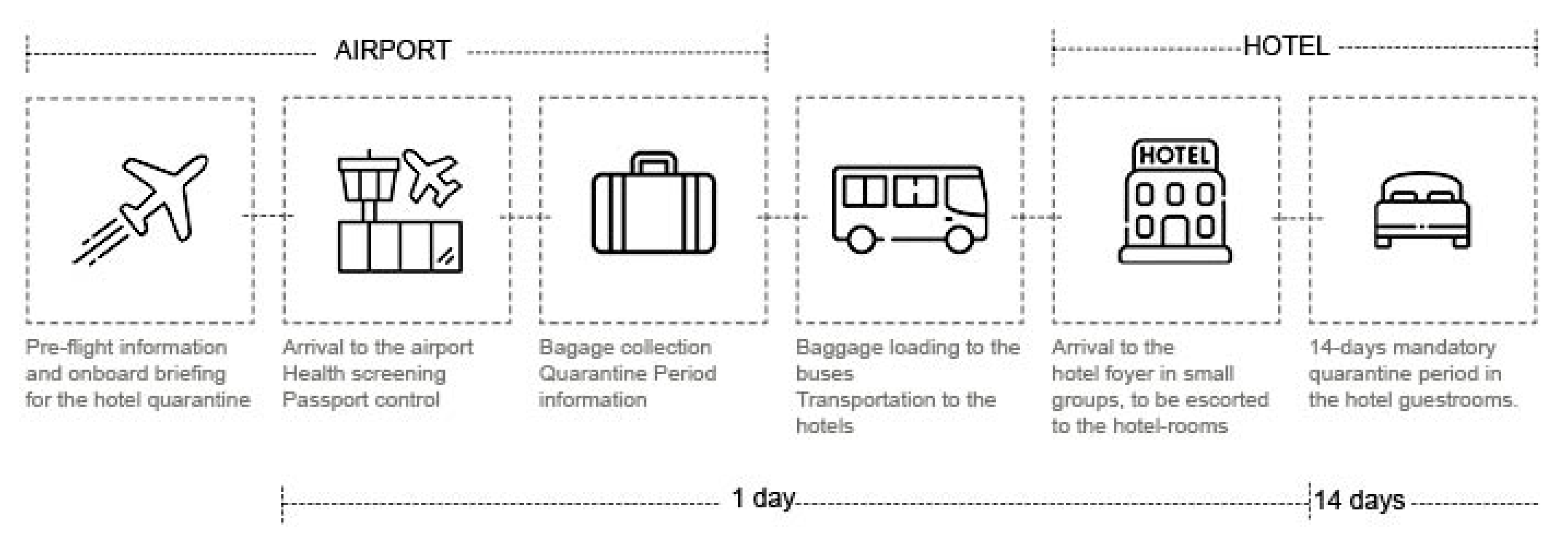
2. Research Framework: Quarantine Hotels
3. Research Methodology
- (1)
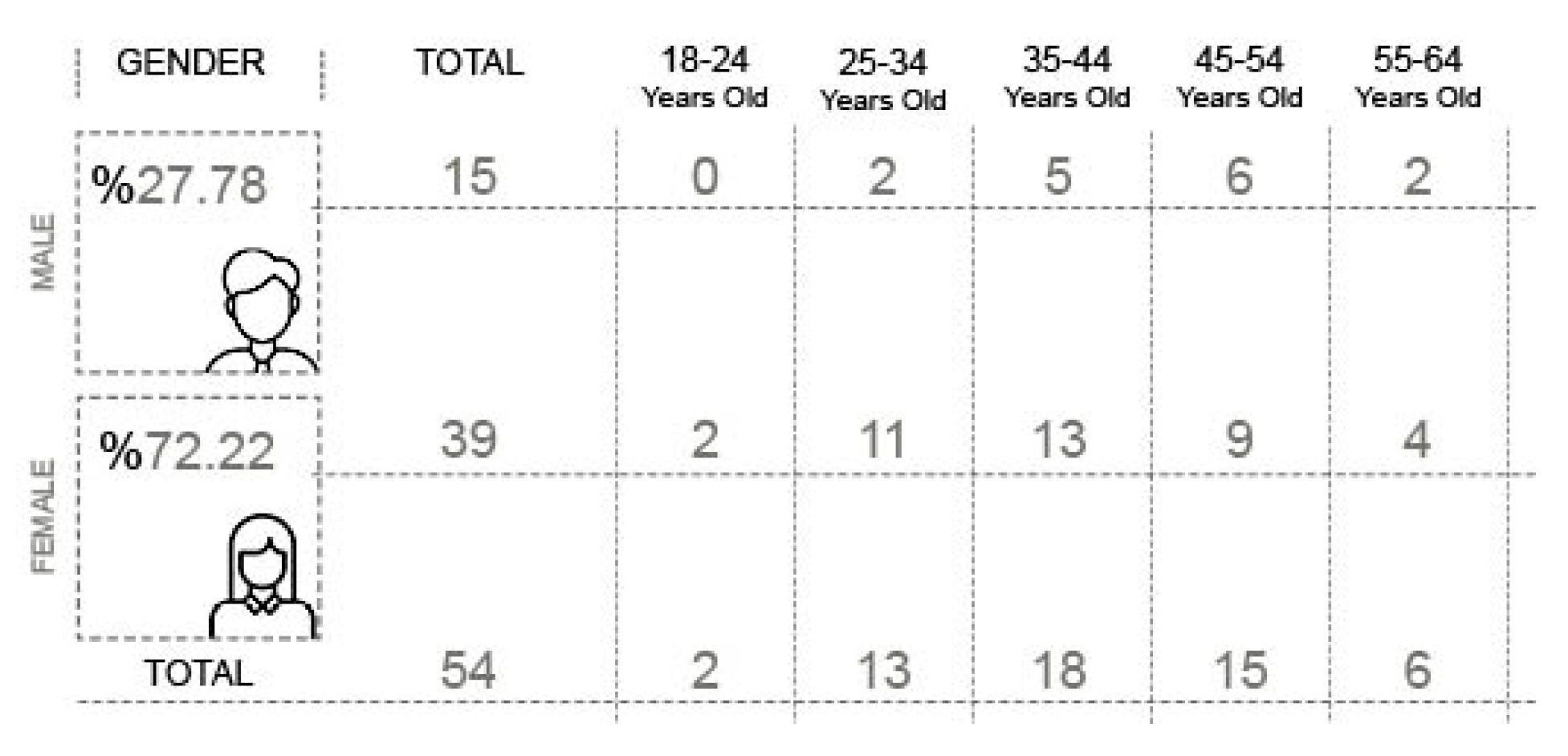
- Descriptive data on participants, such as age and gender;
- (2)
- data on hotel room experiences, such as guestroom physical conditions (for example, lighting and ventilation) and their outcomes on users’ well-being during and after quarantine (Table 1). The survey questions did not include specific questions about families and their quarantine experience with children.
- (1)
- Participants were hotel users obliged to stay in isolation for two weeks due to Australian COVID-19 health requirements;
- (2)
- Participants were over 18 years old. The survey was available to people who had previously been quarantined and/or were in the second week of their quarantine period.
4. Data Analysis
4.1. Descriptive Data
4.2. User Experience Data
5. Results and Discussion
5.1. Critical Sources of Well-Being during Quarantine
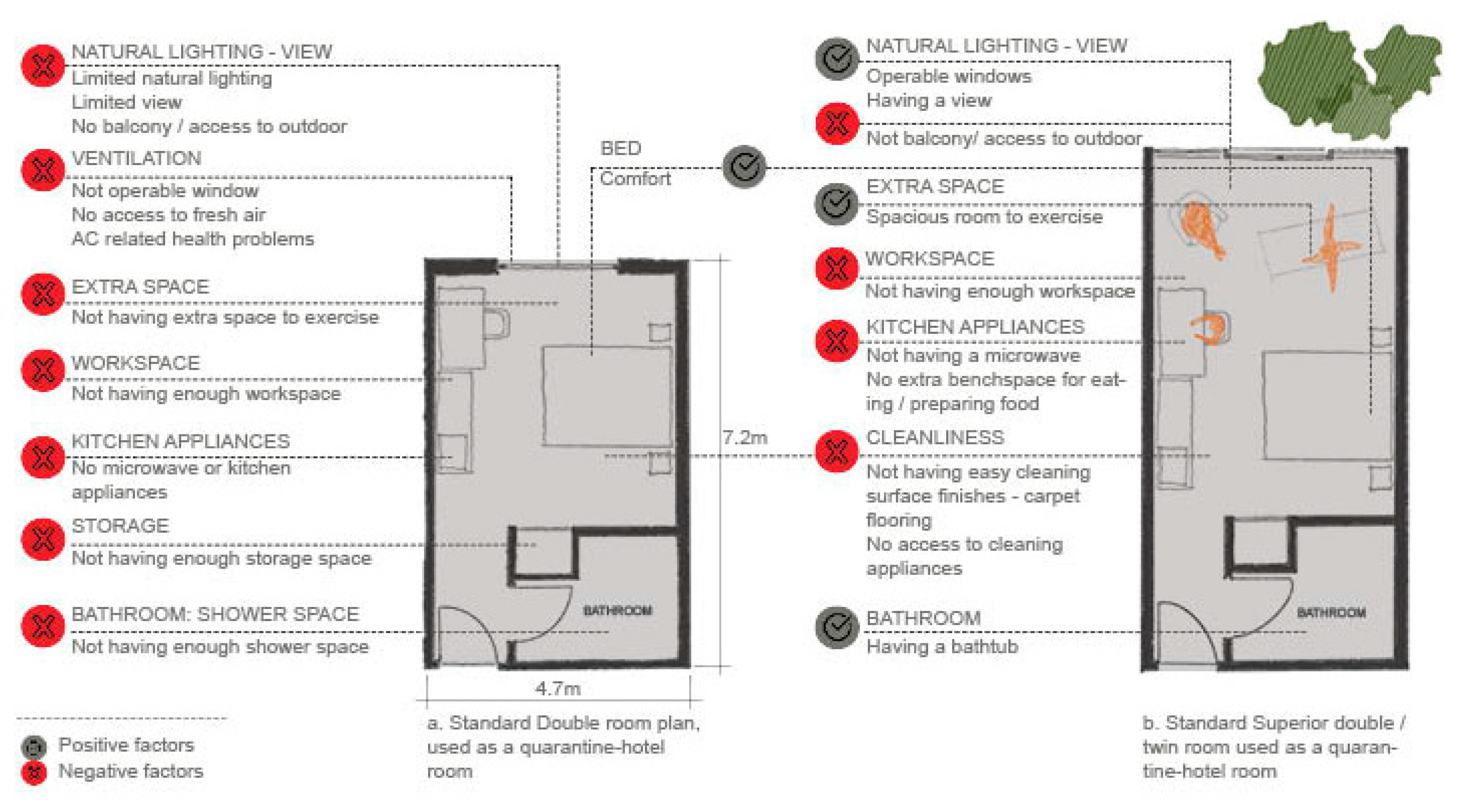
5.2. Spatial Requirements for Quarantine Hotel Rooms
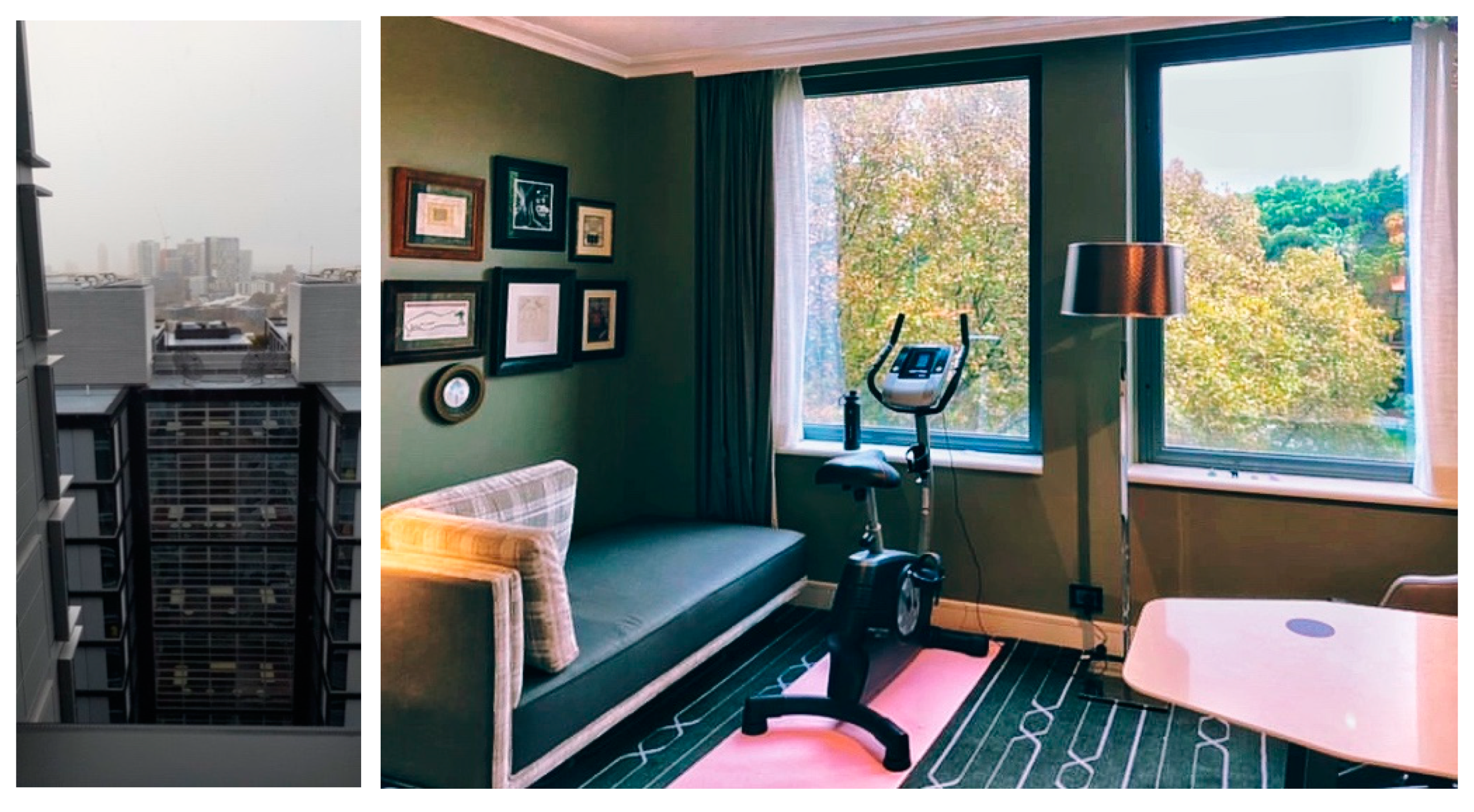
5.2.1. View and Ventilation
“A view, view, Reasonable outlook/view of the city. There were large windows looking over the harbor. That was where I spent most of my time in quarantine.”
“Love the sun coming in through the window; sunlight coming in, full-height window; a lot natural lighting and big windows.”
“No fresh air was incredibly challenging.”
“The lack of opening windows and fresh air drove me insane. It was horrible.”
“No openable window, no balcony, no room for exercise, tall buildings surrounding so limited natural light air-conditioning (made me sick).”
“Not being able to open the windows did make it feel claustrophobic at times, I would rather have had a smaller room with a balcony.”
“Having a balcony and … with an ocean view made a massive difference.”
“The balcony was a life-saver for air and a view.”
“It has a balcony; I don’t think I would have coped with no fresh air.”
“The balcony and view have been amazing with the fresh air.”
“There were two large balconies. We had fresh air and nice our breakfast there.”
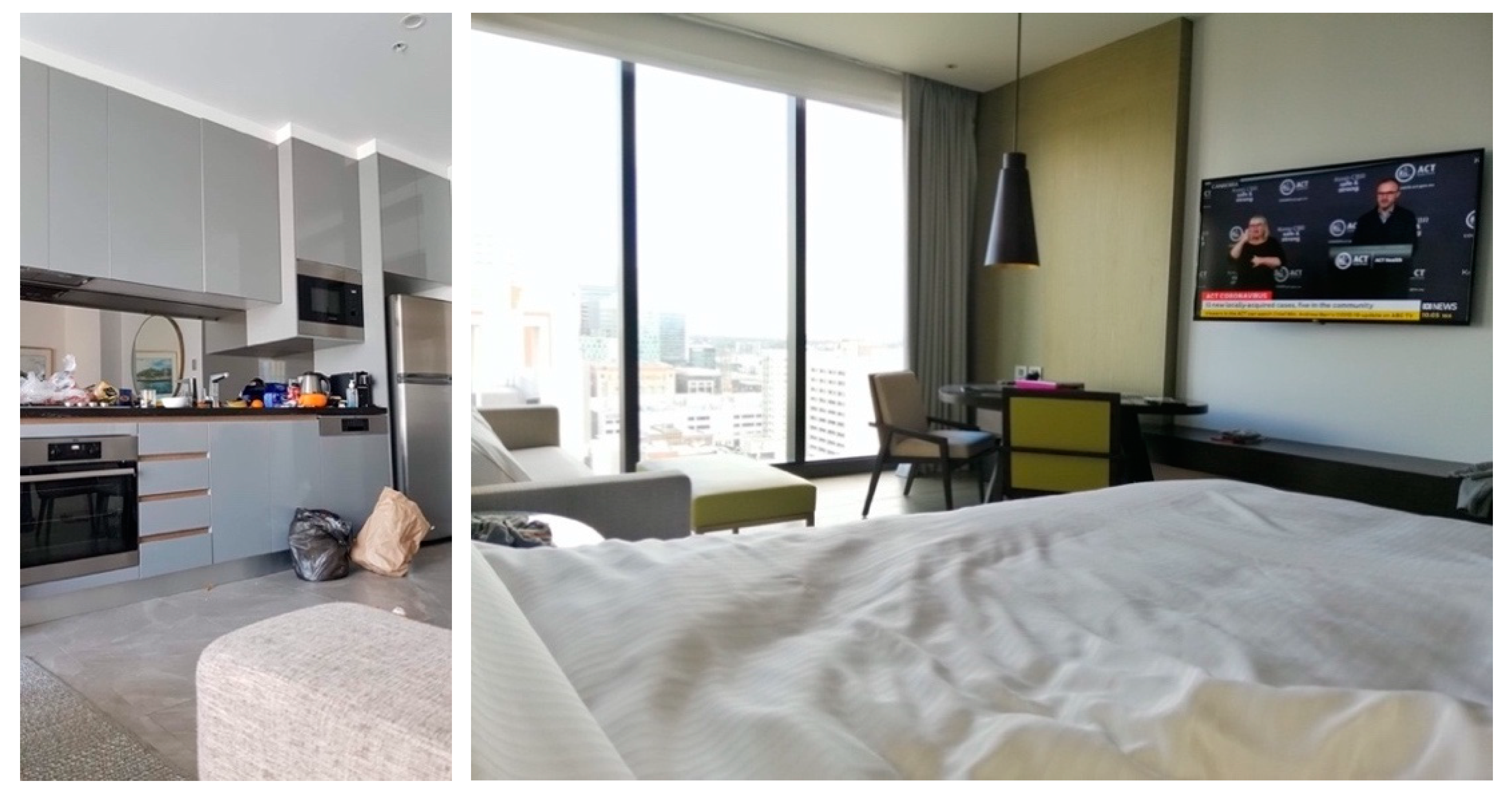
5.2.2. Additional Space and Appliances
“Having a large space with a view/sunlight, a workspace, an area where I could relax, and a bathtub made a big difference to my experience.”
“Clean and qualitative bathroom.”
“The bathroom sink is difficult to wash dishes or clothes in.”
“No kitchen facility to prepare food for the children, and what was delivered was inadequate.”
“No means to reheat food which was always cold. Appliances were stripped, so I do not know if this hotel usually provides a microwave.”
“No microwave meant constantly eating cold food and made food choice hard.”
“The food was really good but unhealthy, so I would have rather have had the option to have a kitchen (rather than just a microwave and kettle) and order my own food to cook and not get food delivered and get a discount on the bill. I definitely put on weight during quarantine even though I was working out three times a day.”
5.2.3. Cleanliness and Hygiene
“Carpet and general room cleanliness below average”
“It is very small. There is no cleaning equipment like toilet brush or way to clean carpet. Cleaning dishes in bathroom sink and clothes in the bathtub is not great.”
“Doona had no doona cover-just flat sheets.”
“No vacuum cleaner or other appliances to clean the room.”
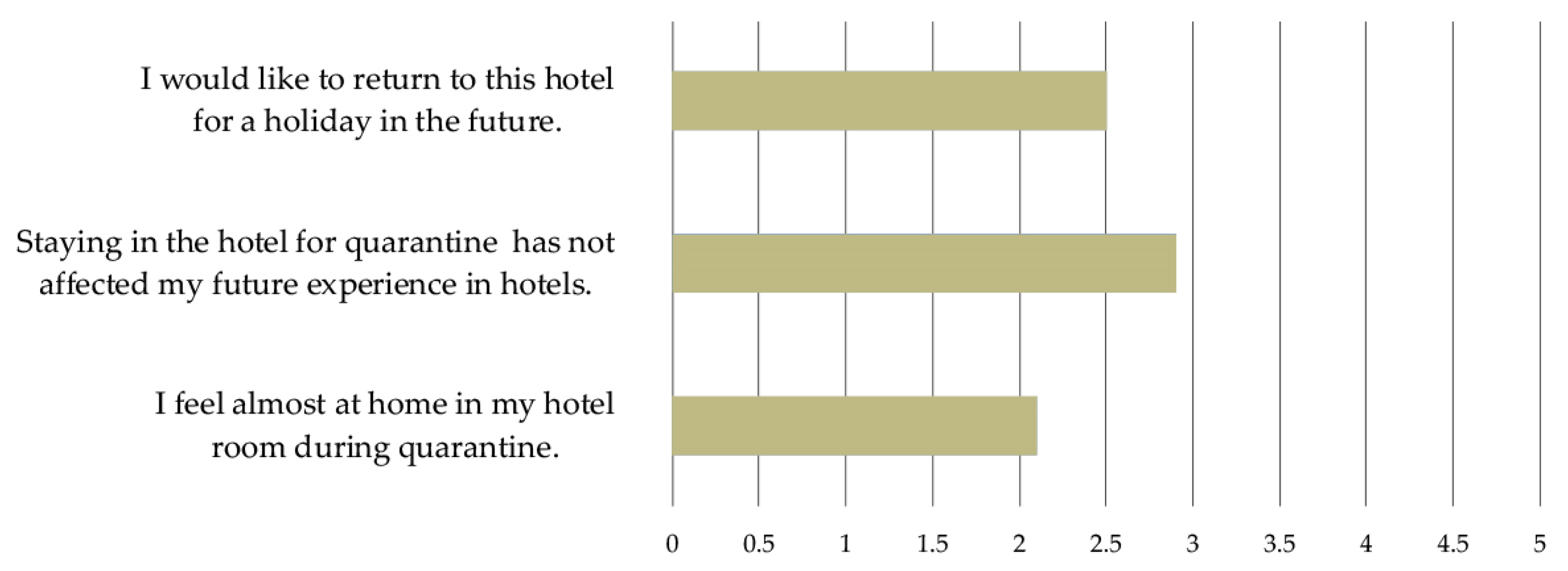
5.3. Impacts of Quarantine Experience on Future Use
“I feel almost at home in my hotel room during quarantine.”
“I would like to return to this hotel for a holiday in the future.”
“Staying in the hotel for quarantine has not affected my future experience in hotels.”
6. Conclusions
7. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deloitte. Tourism and Hotel Market Outlook Executive Summary. 2021. Available online: https://www2.deloitte.com/au/en/pages/consumer-industrial-products/articles/tourism-hotel-outlook.html (accessed on 17 September 2021).
- Choi, M.; Choi, Y. Employee Perceptions of Hotel CSR Activities during the COVID-19 Pandemic. Int. J. Contemp. Hosp. Manag. 2021, 33, 3355–3378. [Google Scholar] [CrossRef]
- Hao, F.; Xiao, Q.; Chon, K. COVID-19 and China’s Hotel Industry: Impacts, a Disaster Management Framework, and Post-pandemic Agenda. Int. J. Hosp. Manag. 2020, 90, 102636. [Google Scholar] [CrossRef] [PubMed]
- National Review of Hotel Quarantine Report Australian Government Department of Health. 2020. Available online: https://www.health.gov.au/resources/publications/national-review-of-hotel-quarantine (accessed on 11 July 2021).
- New South Wales Health Government Website Announcements. 2021. Available online: https://www.health.nsw.gov.au (accessed on 11 June 2021).
- Dinh, M.; Hutchings, O.; Bein, K.; Shaw, J.; Raut, A.; Russell, S.B.; Jager, D.; Thapa, R.; Fox, G.; Edwards, J.; et al. Emergency department presentations by residents of Sydney quarantine hotels during the COVID-19 outbreak. Med. J. Aust. 2021, 214, 473. [Google Scholar] [CrossRef]
- Grout, L.; Katar, A.; Ouakrim, D.A.; Summers, J.A.; Kvalsvig, A.; Baker, M.G.; Blakely, T.; Wilson, N. Estimating the Failure Risk of Hotel-based Quarantine for Preventing COVID-19 Outbreaks in Australia and New Zealand. medRxiv 2021. Available online: https://www.medrxiv.org/content/10.1101/2021.02.17.21251946v1 (accessed on 24 July 2021).
- Young, J. COVID Delta Variant is ‘in the Air You Breathe’: What You Need to Know about Sydney Outbreak Strain. 2021. Available online: https://www.theguardian.com/australia-news/2021/jun/24/its-in-the-air-you-breathe-what-you-need-to-know-about-sydneys-delta-covid-variant (accessed on 24 July 2021).
- Nickson, S. Coronavirus Hotel Quarantine: Key Questions for the Government. 2021. Available online: https://apo.org.au/node/310895 (accessed on 15 May 2021).
- Martha, L.; Vrasida, M.; Agaliotou, C. Redefining and Redesigning Modernity in the COVID-19 Era: The Case of Xenia Hotels in Greece. In Strategic Innovative Marketing and Tourism in the COVID-19 Era: 9th ICSIMAT Conference 2020; Kavoura, A., Havlovic, S.J., Totskaya, N., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 233–240. [Google Scholar]
- Goh, E.; Baum, T. Job Perceptions of Generation Z Hotel Employees towards Working in COVID-19 Quarantine Hotels: The Role of Meaningful Work. Int. J. Contemp. Hosp. Manag. 2021, 33, 1688–1710. [Google Scholar] [CrossRef]
- Bonfanti, A.; Vigolo, V.; Yfantidou, G. The Impact of the COVID-19 Pandemic on Customer Experience Design: The Hotel Managers’ Perspective. Int. J. Hosp. Manag. 2021, 94, 102871. [Google Scholar] [CrossRef]
- Teng, Y.M.; Wu, K.S.; Lin, K.L. Life or livelihood? Mental Health Concerns for Quarantine Hotel Workers During the COVID-19 Pandemic. Front. Psychol. 2020, 11, 2168. [Google Scholar] [CrossRef] [PubMed]
- Teng, X.; Teng, Y.M.; Wu, K.S.; Chang, B.G. Corporate Social Responsibility in Public Health During the COVID-19 Pandemic: Quarantine Hotel in China. Front. Public Health 2021, 9, 620930. [Google Scholar] [CrossRef]
- Majumdar, R. Surviving and growing in the post-Covid world: The case of Indian hotels. Worldw. Hosp. Tour. Themes 2021, 13, 584–598. [Google Scholar] [CrossRef]
- Teng, Y.M.; Wu, K.S.; Xu, D. The Association Between Fear of Coronavirus Disease 2019, Mental Health, and Turnover Intention Among Quarantine Hotel Employees in China. Front. Public Health 2021, 9, 557. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.C.; Chen, X.; Chang, Y.Y. Structural relationships between psychosocial risk, relationship quality, need for cognition, and quarantine intentions: The case of the quarantine hotel. Serv. Bus. 2021, 15, 1–25. [Google Scholar] [CrossRef]
- Wang, K.Y.; Ma, M.L.; Yu, J. Understanding the perceived satisfaction and revisiting intentions of lodgers in a restricted service scenario: Evidence from the hotel industry in quarantine. Serv. Bus. 2021, 15, 335–368. [Google Scholar] [CrossRef]
- Word Clouds Generator. 2021. Available online: http://www.wordclouds.com (accessed on 8 October 2021).
- Aviv, D.; Chen, K.W.; Teitelbaum, E.; Sheppard, D.; Pantelic, J.; Rysanek, A.; Meggers, F. A fresh (air) Look at Ventilation for COVID-19: Estimating the Global Energy Savings Potential of Coupling Natural Ventilation with Novel Radiant Cooling Strategies. Appl. Energy 2021, 292, 116848. [Google Scholar] [CrossRef]
- Zhuo, K.; Zacharias, J. The Impact of Out-of-home Leisure before Quarantine and Domestic Leisure during Quarantine on Subjective Well-being. Leis. Stud. 2021, 40, 321–337. [Google Scholar] [CrossRef]
- Buonocore, C.; De Vecchi, R.; Scalco, V.; Lamberts, R. Influence of Recent and Long-term Exposure to Air-conditioned Environments on Thermal Perception in Naturally-ventilated Classrooms. Build. Environ. 2019, 156, 233–242. [Google Scholar] [CrossRef]
- Emmanuel, R. Performance Standard for Tropical Outdoors: A Critique of Current Impasse and a Proposal for Way Forward. Urban Clim. 2018, 23, 250–259. [Google Scholar] [CrossRef] [Green Version]
- Xiong, J.; Lian, Z.; Zhang, H. Physiological Response to Typical Temperature Step-changes in Winter of China. Energy Build. 2017, 138, 687–694. [Google Scholar] [CrossRef]
- Ueno, T.; Ohnaka, T. Influence of Long-Term Exposure to an Air-conditioned Environment on the Diurnal Cortisol Rhythm. J. Physiol. Anthropol. 2006, 25, 357–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, J.; Ouyang, Q.; Zhu, Y.; Shen, H.; Cao, G.; Cui, W. A Comparison of the Thermal Adaptability of People Accustomed to Air-conditioned Environments and Naturally Ventilated Environments. Indoor Air 2012, 22, 110–118. [Google Scholar] [CrossRef]
- Grigoriadou, E.T. The Urban Balcony as the New Public Space for Well-being in Times of Social Distancing. Cities Health 2021, 4, 1–4. [Google Scholar] [CrossRef]
- Francisco, R.; Pedro, M.; Delvecchio, E.; Espada, J.P.; Morales, A.; Mazzeschi, C.; Orgilés, M. Psychological Symptoms and Behavioral Changes in Children and Adolescents during the Early Phase of COVID-19 Quarantine in Three European Countries. Front. Psychiatry 2020, 11, 1329. [Google Scholar] [CrossRef]
- Asim, F.; Chani, P.S.; Shree, V. Impact of COVID-19 Containment Zone Built-environments on Students’ Mental Health and Their Coping Mechanisms. Build. Environ. 2021, 203, 108107. [Google Scholar] [CrossRef]
- Dzhambov, A.M.; Lercher, P.; Browning, M.H.; Stoyanov, D.; Petrova, N.; Novakov, S.; Dimitrova, D.D. Does Greenery Experienced Indoors and Outdoors Provide an Escape and Support Mental Health during the COVID-19 Quarantine? Environ. Res. 2021, 196, 110420. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDCP). Cleaning and Disinfecting Your Facility. Available online: https://www.cdc.gov/coronavirus/2019-ncov/community/ventilation.html (accessed on 20 June 2021).
- The Environmental Protection Agency. Available online: https://www.epa.gov/coronavirus/about-list-n-disinfectants-coronavirus-covid-19-0 (accessed on 12 October 2021).
- Ineson, E.M.; Comic, D.; Kalmic, L. Towards a Hierarchy of Hotel Guests’ In-room Needs. Int. J. Contemp. Hosp. Manag. 2019, 31, 4401–4418. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptive Properties Questions | |||
| Descriptive Properties | Question Type | Response Options | |
| Age | Multiple-choice question type | 18 to 24 25 to 34 35 to 44 45 to 54 | 55 to 64 65 to 74 75 years and over |
| Gender | Multiple-choice question type | Male Female | Non-binary Prefer not to say |
| Hotel Room Experience Questions | |||
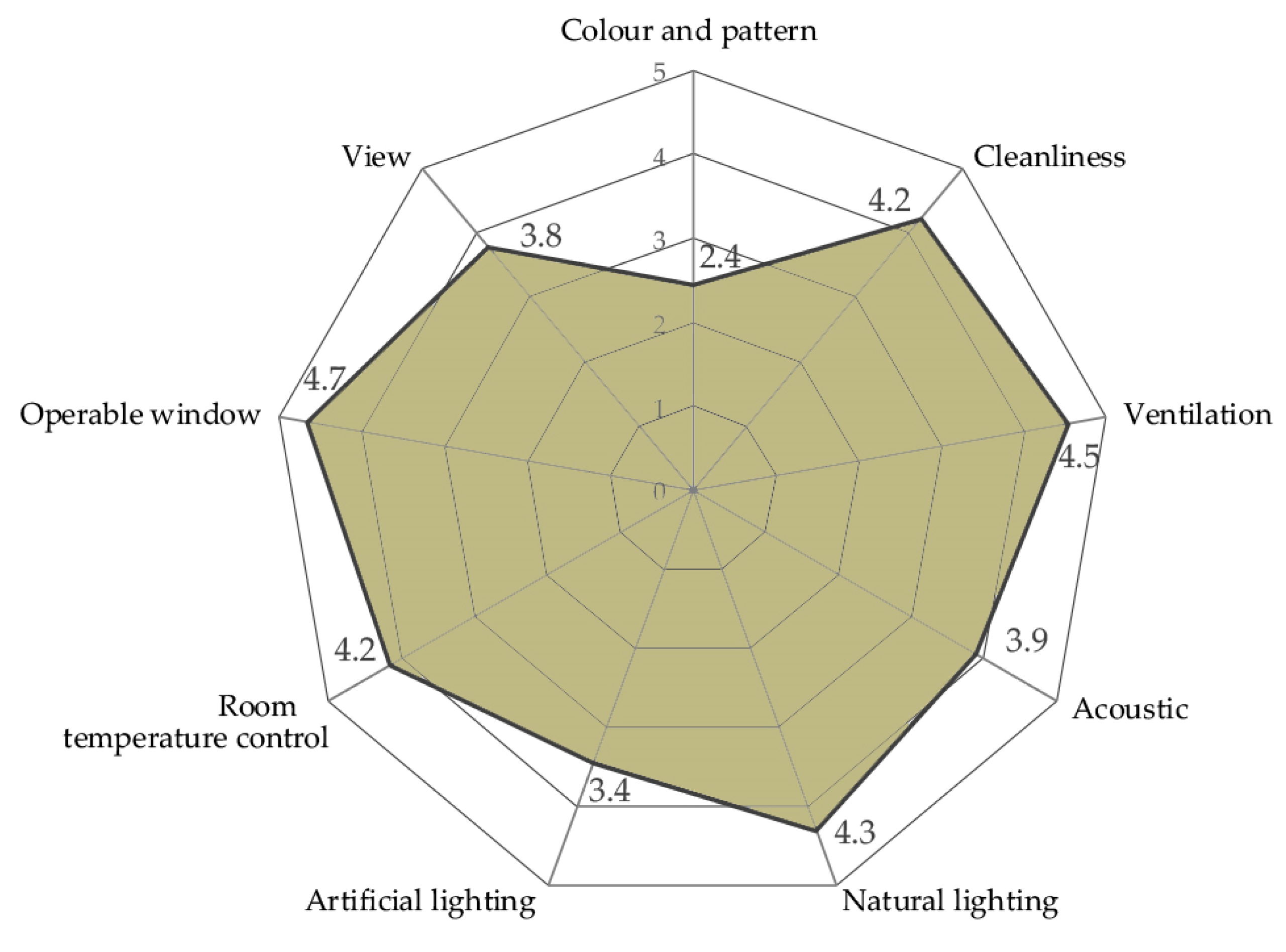
| Please rate the importance of the item to your well-being. | Matrix table, 9 items: 5 Likert Scale: Not at all—Extremely Important | Colour and pattern of the room, Maintenance of the room, cleanliness Ventilation system, Acoustics—noise control, Natural lighting, Artificial lighting, Room temperature control, Openable window View of the room | |
| Please rate your experience at the hotel quarantine. | Matrix table, 3 items: 1 item is repeated. 5 Likert Scale: Strongly disagree—Strongly agree | I feel almost at home in my hotel room during quarantine. Staying in the hotel for quarantine has not affected my future experience in hotels. I would like to return to this hotel for a holiday in the future. | |
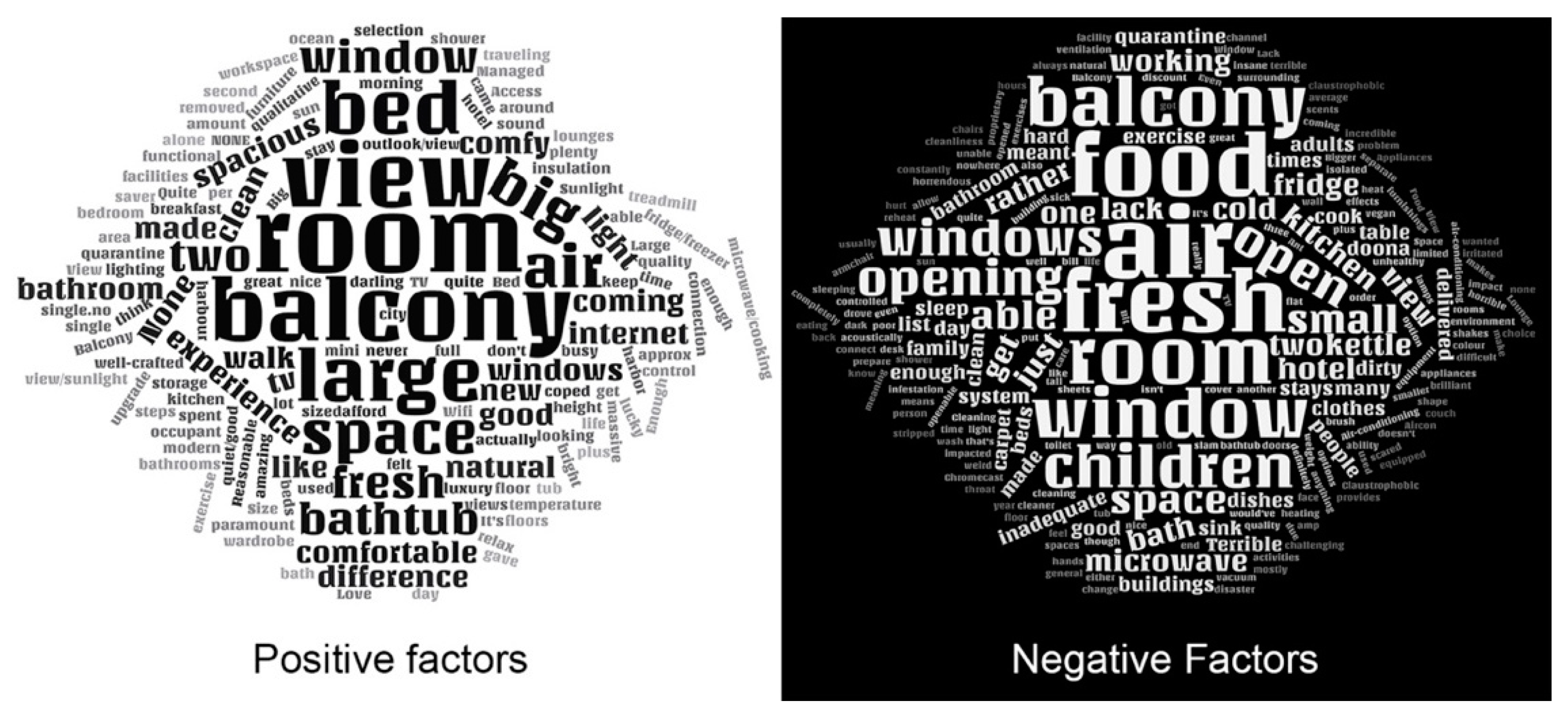
| Could you share any positive factors about the room affecting your well-being? | Open-ended question (Text entry) | ||
| Could you share any negative factors about the room affecting your well-being? | Open-ended question (Text entry) | ||
| Factors | Questionnaire Items | Component Loading the Contribution of Each Variable on Principal Components | Rotation Sums of Squared Loadings | ||
|---|---|---|---|---|---|
| 1 | 2 | 3 | % Variance | ||
| View | The view of the room | 0.776 | −0.114 | 24.40 | |
| Colour and pattern use in the room | 0.722 | 0.322 | |||
| Acoustics-noise control | 0.658 | 0.328 | 0.209 | ||
| Control of the room temperature | 0.584 | 0.413 | −0.131 | ||
| Cleanliness | Maintenance of the room-cleanliness | 0.195 | 0.798 | 19.58 | |
| Artificial lighting | 0.783 | 0.158 | |||
| Ventilation | Ventilation system | −0.130 | 0.303 | 0.799 | 21.31 |
| Operable window | 0.745 | ||||
| Natural lighting | 0.483 | −0.153 | 0.673 | ||
| Dependent Variable | Mean Difference (I–J) | Std. Error | Sig. | 95% Confidence Interval | |||
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| View | 45+ | 18–34 | 1.116 | 0.335 | 0.005 | 0.300 | 1.931 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dincer, D.; Gocer, O. Quarantine Hotels: The Adaptation of Hotels for Quarantine Use in Australia. Buildings 2021, 11, 617. https://doi.org/10.3390/buildings11120617
Dincer D, Gocer O. Quarantine Hotels: The Adaptation of Hotels for Quarantine Use in Australia. Buildings. 2021; 11(12):617. https://doi.org/10.3390/buildings11120617
Chicago/Turabian StyleDincer, Demet, and Ozgur Gocer. 2021. "Quarantine Hotels: The Adaptation of Hotels for Quarantine Use in Australia" Buildings 11, no. 12: 617. https://doi.org/10.3390/buildings11120617