1. Background
Participation and contextualism are essential in health promotion and of particular importance in interventions aimed at reducing social inequalities in health through health education and empowerment [
1,
2,
3,
4,
5]. The shift towards participatory health promotion builds upon Freire and Rogers’ approach to change and learning, shifting the traditional role of the health professional (HP) from a health educator to a facilitator for change and learning. This entails a commitment to participation and empowerment and attention to process as well as content for health promotion practitioners [
6].
Norwegian municipalities are encouraged to establish Healthy Life Centres (HLCs) to offer preventive and health-promoting services to people with lifestyle related diseases or at risk for such diseases. This initiative is regarded as a contribution to coherent and coordinated health services and reduced social inequalities in health [
7]. HLCs are municipal primary-health services that offer primarily group-based guidance on behaviours such as physical activity, nutrition, and tobacco use, that represent important risk factors for lifestyle-related diseases. Studies have shown that service users in Norwegian HLCs are predominantly female and middle-aged and that a high proportion have a low education level and low income [
8]. Ninety-one percent of service users are of Norwegian origin [
8,
9] and more than sixty percent report having two or more chronic conditions. This points to complex social, emotional and physical challenges among the service users [
10]. It is in line with the HLCs’ objective to recruit people from socioeconomically disadvantaged groups [
11]. Approximately 30,000 people received services from Norwegian HLCs, and 60% of Norwegian municipalities provided HLC services, covering 80% of the Norwegian population in 2019 [
12].
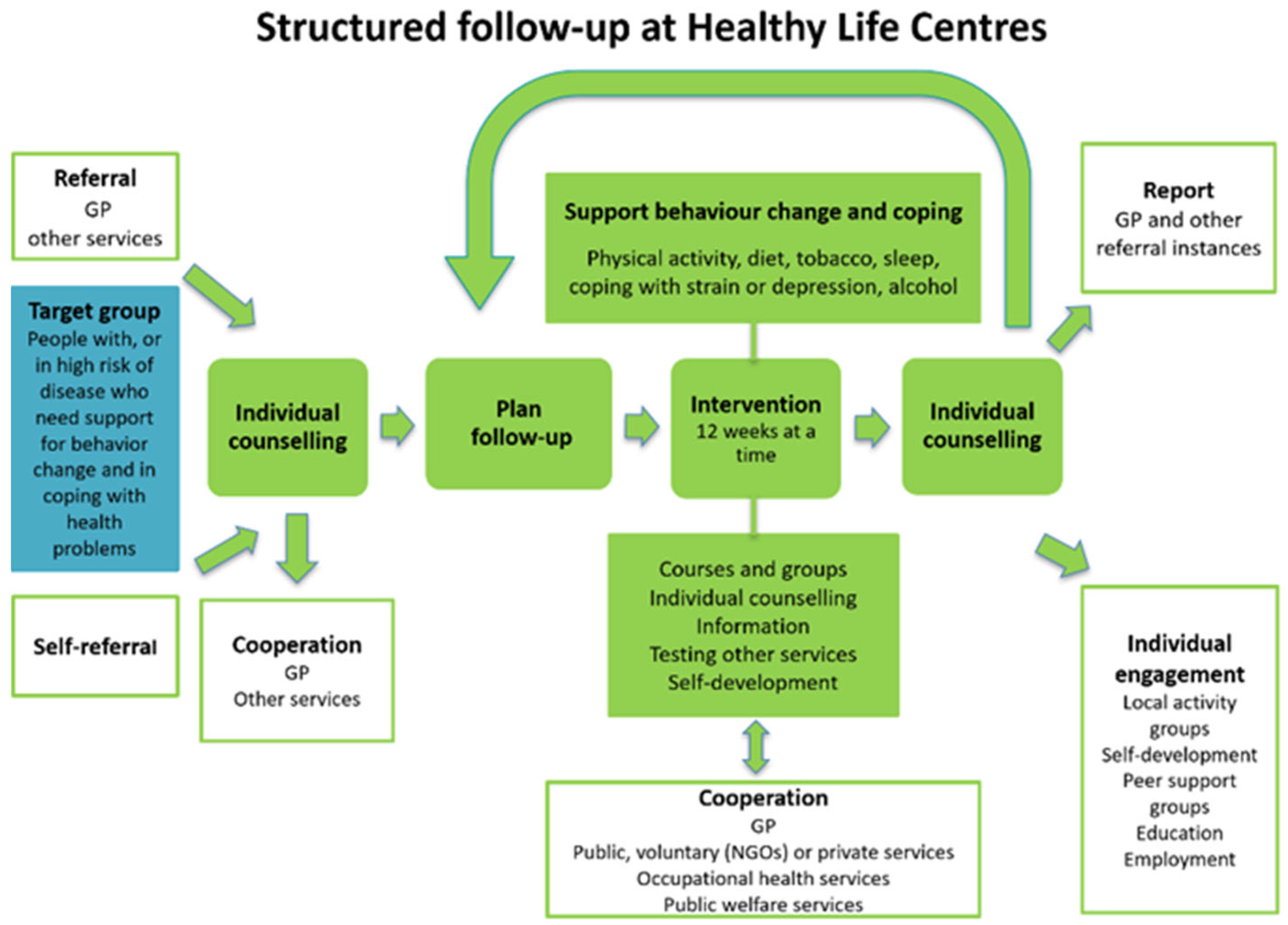
According to the HLC guidelines, the services build upon individual needs and goals, and service users should participate in planning, implementation, and evaluation of the services [
7]. The HLCs offer structured and adapted follow-up for 12 weeks at a time, and the period can be prolonged twice, comprising up to 36 weeks of follow-up in total. The intervention is primarily group-based but starts and ends with an individual health conversation. An opportunity for additional individual conversations is provided if needed. The purpose of the conversations is to map each service user’s situation and to work out a plan based on individual challenges and goals [
7]. See
Figure 1 for an illustration of the follow-up process.
The services in HLCs are based upon different theoretical approaches within a frame of health promotion and salutogenesis—approaches that emphasize participation [
2,
14,
15,
16]. Salutogenesis refers to the origin of health and opposes the pathogenic focus in a medical perspective of health. Salutogenesis focus on salutary factors and resources for health, and its core concept is the sense of coherence (SOC), which refers to the ability to use the resources at hand, an ability shaped by life experiences. It is a holistic and whole-person approach, placing the individual as an active participant in context [
6].
In the literature, the notion of participation is, however, characterized by a lack of conceptual clarity [
2,
17,
18]. It is a multifaceted concept, which is discussed from both democratic and utilitarian perspectives, discussed as a human right and an outcome of services, and as individual, interactional, or as an invitation from the environment [
18]. Some scholars emphasise external provisions for participation and present participation as a prerequisite and strategy for empowerment [
17]. The International Classification of Functioning, Disability and Health (ICF), describes participation as involvement in a life situation that encompasses individual and contextual aspects, such as social, attitudinal, or physical factors, and the reciprocal influence among them [
19]. In the field of health promotion, participation is considered a key principle and strategy premised on the Alma Ata declaration [
20]. Within the socioecological understanding of health that underlies health promotion, participation may be understood as a social process in which different actors negotiate various types of knowledge and perspectives through different phases, in line with Marent et al. [
2]. The notion of participation used in this study combines the ICF’s emphasis on the contextual aspects of participation and Marent et al.’s understanding of participation as a situated social negotiation process.
While research in this setting remains scarce due to the novelty of HLCs, a few relevant studies have been conducted. One study by Sagsveen et al. [
21] found that service users identified a relationship of respect and acknowledgement between service users and health personnel (HPs) as essential for involvement in their own care. Service users also stated that building trustworthy relationships was hampered by a lack of relational continuity and information lost between individual health consultations and follow-up in group activities [
21]. The study concluded that there is a need for observational studies on involvement in interactions between HPs and service users. Another study by Sagsveen et al. [
22] also identified the relationship between service users and HPs as essential to involvement and described a practice in which the user’s involvement, according to HPs, was obtained through motivational interviewing as a conversational method in individual health consultations.
In Salemonsen et al. [
23], HLC service users described user involvement as acknowledgement by personalising and tailoring support to users’ needs and everyday life situations. Salemonsen et al. [
24] found that HPs understand user involvement as ethical awareness, dialogue, and an attitude of non-judgement, viewing service users as partners in collaboration. The study concluded that there is a need to focus on shared responsibility and the conditions for services that facilitate such practice.
The understanding of participation as a situated social process entails a need to elaborate the social context where this process emerges [
2]. This seems to resonate with the research on user involvement in HLCs as called for by Salemonsen and Sagsveen. Given that most services in HLCs are organised as group activities, there is a need to explore the conditions of participation in such activities in Norwegian HLCs. This knowledge may be a valuable contribution to the HLCs’ aims to empower service users and reduce social inequalities in health.
The aim of the present study is to explore participation in group activities in the context of a Norwegian HLC by studying interactions among service users and between service users and health professionals (HPs).
2. Methods
2.1. Design
A qualitative and ethnographic study was designed to explore participation in group activities in the HLC, creating data through participant observation.
2.2. Participant Observation
To gain insight into interactions and communication among service users and between service users and HPs in group activities in the HLC, participant observation was chosen as the method of data collection. Observational studies can provide insight into social situations in their natural settings that have not been previously interpreted by the actors in the situation themselves. In observational studies, the researcher focuses on what people do, rather than what they say they do [
25]. Instead of seeking a fixed story from the field, the researcher contributes to a combination of collecting and creating the story [
26]. Thus, it is important to clarify the steps taken throughout the process of data creation, analysis, and the presentation of findings.
The first author participated in 24 group-based activities in a Norwegian HLC for a total of 42 h. See
Table 1 for further details.
Both physical activity groups (PAG) and the Healthy Nutrition group (HNG) took place in the same facilities. PAGs were organised as open groups that participants joined and left continuously, whereas the HNGs were organised as closed groups in which the same participants followed a fixed course plan consisting of five to six sessions. During the activities, the first author took on the role of ‘the participant as observer’, as termed by Tjora [
25]. This is a disclosed observer role, meaning that the service users are familiar with and consent to the researcher participating in activities and conducting observations. The aim was to enter the social world of the HLC and take part as one of the service users in the various groups. The first author participated in the activities, conversations, and interactions, asking questions and following up on topics introduced by others, but avoiding introducing topics herself. The methodological unit under study was the interaction among service users and between service users and HPs.
The data consist of 99 pages of electronically written observation notes, comprising approximately 33,000 words. In PAGs, notes were handwritten immediately after the activity, mainly in the car, in the form of keywords and short sentences that described situations of significance, dialogues, context, number of attendants, and so forth. These ‘rough notes’ were transcribed into more coherent text when the first author returned to the office. In HNGs, routines for writing observation notes differed slightly, as the course resembled a classroom education setting in which all the service users took notes, allowing the researcher to take more comprehensive notes in this setting. These notes also consisted of keywords and short sentences, but they were more elaborate than those from PAGs because they were written during the session. These notes were also transcribed when the first author returned to the office. The observation documents vary in length from two to six written pages each, depending on the duration of the observations (1–3 h) and on the opportunity to take notes during the activity. Following Fangen [
26], the documents were organised into three parts: reflections before observation, observation notes on context and action, and reflections after observation. Reflections can be theoretical, methodological or even analytical [
26], representing empirical analytical reference points [
25] that may contribute to the data analysis.
2.3. Recruitment
The inclusion criterion for this study was an HLC that offered group-based PAGs and HNGs, representing the basic services of HLCs. To be able to participate in HLC activities over several months, the first author also took some practicalities of geographical location into consideration before inviting an HLC to take part in the study. The leader of an HLC located in reasonable geographical proximity was contacted by the first author, and a meeting to discuss the study was arranged. Further, the first author was invited to meet employees to present the project. All employees agreed to invite the first author to conduct participant observation in their group activities.
The service users enrolled in the group activities were informed about the research project orally at the start of every activity and offered written information about the project. They were asked for oral consent to take part in the study. The study was registered at the Norwegian Centre for Research Data (NSD), project number 51816. However, because no personal data were collected in the study, it was not subject to notification.
2.4. Study Context
The participant observations took place in two periods (see
Table 1) in an HLC located in Mid-Norway that offered various group activities, including PAGs and HNGs. The HLC venue was in a public building with multiple functions and services, such as a large social area in the entrance. The indoor PAGs took place mainly in a large hall with direct access to the social area, whereas the HNGs took place in a conference room located elsewhere in the building.
The outdoor PAGs were held on different sites in the nearby area, including a football field, hills for interval running, and hiking trails. The area had a rural feel and was close to nature.
Between five and sixteen service users were present in each of the group activities underlying this study, and seven HPs in total were involved in the different activities.
Even though the first author aimed to position herself as a ’participant as observer´, she noted that there were variations in how she was perceived by the service users and the HPs. The service users predominantly perceived her as a fellow service user, including her in activities and social gatherings, but sometimes also approached her as a researcher. When she was perceived as a researcher, the service users in general expressed positive attitudes towards the HLC and the HPs. In other situations, when the first author was included as one of the service users in social gatherings before or after activities, or in conversations within activities, the attitudes towards the HLC and the HPs were expressed differently, in a more critical and questioning light. The HPs in general approached and involved the first author as a researcher, turning towards her with comments or interpretations of what had been said or done in group activities where the first author also took part. The first author has training and experience in health promotion interventions and personal experience with lifestyle change which may have affected the variety of perceived positions. Together, the three authors have their educational background in both health and social sciences, training and experience in health promotion and health promotion interventions, and experience in research on inclusion, participation, and empowerment.
2.5. Data Analysis
The analysis was based on a constructivist stepwise-deductive inductive approach (SDI), inspired by Tjora [
25]. SDI underlines the importance of inductive coding in the first phases of analysis, anchoring the findings in the empirical data, before research questions and theory inform the analysis in later steps. SDI combines the inductive principle from grounded theory with a strong theoretical motivation [
25].
For the analysis, all data were read thoroughly by the first and third authors, and the first author wrote notes and memos on excerpts from the text. The data were then transferred to the software computer program NVivo 20 in which empirically close coding of the data took place. NVivo is one of many software programs suitable for analytical work in qualitative research, and the use of such software is highly recommended in SDI. This secures a close link between the analytically developed code and the original data. The proximity to the data results in a significant number of codes that the software helps organise [
25]. The text was read line by line, and small sections of text were coded, with the code names taken directly from data excerpts. The observations contain descriptions of situations and context, as well as citations as recalled and noted by the first author. This explains the variation in the codes between more generic descriptions and direct quotes. An example of this phenomenon is the code ‘description of exercise’, which points to 17 references in the data, while the code ‘one more question, then I won’t say anything more today’ has only one reference in the data, as it is a direct quote from a service user. The coding process resulted in 274 inductively based codes.
The next step in the analysis was to group the codes with internal thematic connections and consistency into categories based on both the research interest and the potential of the data. The second author was included in the process at this point, contributing to the code grouping. The first round of groupings resulted in the following three headings for further analysis: interaction, structure, and individual customisation. ‘Structure’ was placed as an overarching theme at this point, and ‘interaction’ and parts of ‘individual customisation’ were further developed in ‘the role of the instructor’. The sorting of codes and continuous analysis went through four rounds, resulting in organising the results into three categories and an overarching theme of ‘ambiguous facilitation’. These three categories, with underlying subcategories, represent contextual dimensions of participation in the HLC and may be understood as aspects of the overarching theme.
Table 2 illustrates the process of grouping the codes into subcategories, categories, and the overarching theme resulting from the analysis.
3. Findings
As illustrated in
Table 2, the analysis resulted in three categories with several subcategories. The categories are interrelated and overlap to some extent, as they are all aspects of the overarching theme.
In our findings, the overarching theme of ‘ambiguous facilitation’ paints the picture of HPs who aim to motivate, create fellowship, and build relations with limited time and resources and shifting professional perspectives. The interaction between HPs and service users in this study seems to be predominantly characterised by a practice of education and giving advice, which affects the conditions for participation in different ways.
Excerpts from the data in this chapter are presented with an identification of the activity they were collected in (HNG for excerpts from the healthy nutrition groups and PAG for excerpts from the physical activity groups, and number of observation).
3.1. Multiple Roles of the HP
Seven HPs are included in these observations, and between five and sixteen service users were present in the activities on which this study is based. The relatively high numbers point to the challenge of simultaneously recognising the individual and managing the group. The following three subcategories that structure the results in this category illustrate the HPs’ act of juggling different roles that affect the conditions for participation in different ways: ‘acknowledging, motivating and creating fellowship’, ‘safeguarding individual needs in group-based activities’, and ‘contrasting aspects: paternalistic structures shining through’.
3.1.1. Acknowledging, Motivating and Creating Fellowship
Despite the occasionally large groups, the HPs played an active motivational role in many situations throughout the observations. For example, the HPs acknowledged the individual struggles the service users went through at the HLC by recognising the genetic component in lifestyle-related diseases and the individual effort involved in lifestyle change, as well as identifying personal virtues, which may have given the service users the experience of being seen as unique individuals. This active motivational role also included affirmations, such as giving service users high fives after completing exercises, instructing them to give each other a ‘thumbs up’ (PAG11) or reflecting together after the exercise (PAG9). In one such reflection after an interval exercise, the HP asked the group if they noticed any difference between the first and the second run up the hill, and three service users replied that the second run was easier. The HP replied, ‘Yes. You knew the hill this time. You knew how far it was to run’ (PAG9). Reflective situations like this seemed valuable and served as a tool for the HPs to create fellowship. This fellowship could also be seen when the HPs included themselves in the struggles the service users went through; as one HP stated when food labelling was discussed, ‘They are trying to fool us all the time. They want to sell their merchandise and try to hide how much sugar it contains. It’s no wonder we get confused!’ (HNG2). This active motivational role seemed valuable in creating safe conditions for service users to participate in these activities.
3.1.2. Safeguarding Individual Needs in Group-Based Activities
The individual needs that had to be tailored in the HLC could be simple or complex. Simple needs could be that physical challenges made it difficult for a service user to participate in strength exercises (PAG5), that hearing challenges prompted a service user to ask the HP to lower the music volume (PAG1), or that a service user showed up for a rigorous outside activity without the appropriate clothing (PAG13). These kinds of needs were mainly met with flexibility from the HPs, who adjusted exercises individually based on physical challenges or presented alternative exercises with varying degrees of difficulty for the service users to choose from. Throughout the observation period, this practice of tailoring to simple needs was regularly noted to positively affect the conditions for participation.
However, more complex individual needs were often met quite differently. In an outdoor session, a service user in need of assistance from a companion ended up far behind the rest of the group right from the start of PAG9 and stayed far behind for the rest of the activity. The HP stood at the top of the hill, giving high fives to the service users reaching the top but started downwards long before the assisted service user reached the top. When meeting this service user, who was still on the way up, the HP invited them to join the group back down, but the assisted service user refused, saying, ‘No. I want to run my part, too!’ This led to exclusion from the rest of the activity as well. In several sessions, there were examples of non-native service users with linguistic challenges that made it difficult for them to fully participate in activities, especially in some PAGs in which the instructions for certain exercises were quite complicated (PAG3, PAG7). This was acknowledged by one HP in PAG7, who expressed frustration with this challenge and explained that she met it by choosing exercises that she could illustrate rather than explain. However, she experienced specific communication issues with some non-native service users that she recognised as barriers to participation. Thus, safeguarding individual needs in group activities seemed to be unproblematic in cases with simple needs but more challenging for service users with more complex needs.
3.1.3. Contrasting Aspects: Paternalistic Structures Shining Through
In contrast to the motivating and flexible type of HPs, as depicted above, some HPs could also take a more traditional expert role, as the following statement illustrates: ‘We know what works; we know what has to be done’ (PAG14). Whereas the findings mentioned above show how the HPs created fellowship with the service users, this subcategory represents findings in which the HPs seem to have stereotypical assumptions about the service users as a group.
On several occasions, the group leaders in PAGs pointed to the weather as the main reason for low attendance rates, such as ‘Surprisingly many people texted me to say that they were ill or at home with sick children today. I knew it would be that way this morning when I looked out and saw it was raining’ (PAG6). Such assumptions about the service users may explain the following situation, in which the HP did not seem to acknowledge the service users’ stories in the first session after a festive holiday.
The session started with a conversation around the table. All service users present reported that they were happy about sticking to the plan they had made about restricting unhealthy eating and snacks during the holiday. After this round of success stories, the HP introduced the theme of the day, which was blood sugar regulation, by saying, ‘The holiday is just over, and many of you may have gone wild eating snacks…’ (HNG2). Nobody answered, maybe because everybody just reported the exact opposite.
The statement may indicate that the HP had not listened to or did not believe the service users or that the HP was following a predefined plan in which this statement was in line with how the topic was normally introduced. Either way, it may reveal underlying assumptions about the service users, which emerged on a regular basis through comments such as ‘So you’re going to go home to eat unhealthy food now?’ (PAG4) or, when the HP talked about the price of snacks, ‘You don’t have to buy snacks even though they are on sale. Those who sell them are the winners, and we are the losers getting diabetes. Don’t you agree?’ (PAG14). None of the service users answered this question, and the HP turned to the researcher, saying, ‘Nobody dares to disagree’.
3.2. The Process of Goal Setting
According to the HLC guidelines, the services should build upon an individual mapping of needs, challenges, and goals, which are important aspects of the process of goal setting. The findings in this category suggested that goal setting was a continuous, nonlinear process in the group activities throughout the programme, and that there seemed to be a lack of shared understanding between actors involved in the process. The findings in this category are divided into two subcategories, representing the starting and end points of the goal-setting process.
3.2.1. Where to Start
The findings in this subcategory are all drawn from HNGs. Through observations in several sessions, the first author recognised predefined course content that provided little room for individual experiences and challenges. Sometimes this rigidity seemed to lead to faltering conversation between the service users and HPs and the lack of a shared understanding of the problem, as illustrated in the following excerpt:
In the first session of the HNG, there is a round where the service users are asked about their different challenges related to food. A man said that his biggest struggle was overeating. The HP responded to this by talking about a Japanese custom about not eating until you are completely full but stopping when you are 80% full because it takes some time before the brain recognises the sensation of being full. The service user reacted to this information with, ‘But … that is no help to me when my problem is that I can’t even know when I am full, then how can I know when I am 80% full? I only know … stuffed!’ The HP responded that this is a question about frequency and quantity and talked about how much food makes a portion using different methods, among others, a method where you can use your hand to decide a portion: ‘If you imagine the palm of your hand, only the palm without the fingers … everybody’s hands are proportional to the rest of the body, so everybody can use this method […]. If you imagine eating a steak or similar, it should be the size of your palm and as thick as your hand and eat it with rice or potato the size of your fist.’ When the HP said this, another service user looked startled, raised his eyebrows, studied his hand before looking around the room, as if he was looking for some reaction from the other service users (HNG1).
In this situation, the HP seemed to acknowledge neither the nonverbally nor verbally communicated frustration of the service users. This lack of acknowledgement of communicated frustration was visible in several situations throughout the course, such as when the HP made smoothies for the service users to taste (HNG6). One of the smoothies was all green, and a couple of service users wrinkled their noses looking at it. One said that it looked like vomit. When asked about the taste, one service user said that it tasted strange. The HP responded that it is all a question of habit and that one can learn to like new things, after which nothing more was said about it.
Learning to like new things was also a challenge for a non-native service user who expressed frustration about adopting the Norwegian healthy diet in his daily life based on cultural heritage and habits from his earlier home country. He sighed and shook his head, saying, ‘It’s difficult. I’m hungry. My wife is hungry. My kids don’t like it…’ (HNG5), but nothing more was said about this either.
One service user raised a question about whether services that are not attuned to individual needs will lead to any change at all: ‘You would think in this kind of service, that you’d start slowly … but it is tough. Too tough for many of us. There are many people striving to keep up. I keep up in a way but know that I won’t continue this practice when my time here is done’ (HNG6).
3.2.2. Where to Aim
Setting goals was a frequent topic in both HNGs and PAGs and seemed challenging for several service users. Every session of the HNG started with a conversation about the goals the service users had set the previous week and ended with what they wanted to focus on for the following week. These discussions were characterised by differing understandings and expectations between the service users and HPs about how to formulate a goal, as well as what goals to aim for. The topic of goal setting revealed a striking discrepancy between the attention it was given, its stated importance, and the service users’ confusion about it throughout the course. This was apparent in the last session of the HNG, which was led by two substitute HPs who did not know the service users present. Wanting to repeat key messages from the course content, the substitutes invited the service users to repeat the specifications of SMART (specific, measurable, achievable, relevant and time bound) goals, which none of the service users recognised. This led to a debate among the service users about whether they had gone through this topic earlier, which they agreed that they had not. To complete the course, the two substitute HPs distributed a paper form for the service users to fill in and return before going home. The form had columns in which the service users were expected to evaluate their own effort in the course in relation to their personal goals, main goal and intermediate goals and the dates by which they should be attained. One service user clearly struggled with this task. She sat by herself, saying out loud, ‘What is this? What are the main goal and intermediate goals? And why are they dated?’ (HNG6).
In this final session, a quiz was presented to review knowledge gained in the course. The quiz was complicated, and neither the service users nor the two substitute HPs knew the answers to the questions. This led to visible resignation among the service users while the substitute HPs discussed the questions among themselves, making statements like ‘I have studied nutrition for years. I still don’t know the answers to these questions’ (HNG6). When the two substitute HPs and service users discussed the answers as a group, the two substitute HPs did not reach consensus on several questions, so they moved on without presenting an answer. Therefore, the final goal of the HNG in terms of specific knowledge gained from the course was unclear, even in the final session.
There was also confusion about which goals to set in PAGs. On two occasions, balancing tests were presented, which were intended to predict whether one would reach a certain age. One service user reacted to this with a question: ‘So that is our goal? To never die? I don’t dare to find out…’ (PAG15). Another service user named the test ‘The doomsday prophecy’ (PAG14). None of the service users, including the researcher, passed the test. The two different HPs gave instructions but did not complete the test themselves and did not respond to the reactions to the test, and nothing more was said about the test after it was completed.
3.3. Time Frames and Physical Context
In this category, the results were organised into three subcategories: ‘temporal predictability’, ‘rhythm and time schedules’ and ‘physical context’. The findings in this category point to how dialogue and participation are affected by these three features.
3.3.1. Temporal Predictability
The topic of the time frames for the services came up on a regular basis in informal conversations among service users. The HLC prescription, as the basic services of the HLC are called, runs for 12 weeks, but the service users displayed various understandings of the time frames, varying from 10 to 36 weeks. Many service users talked about three HLC prescriptions—that is, 36 weeks—as ‘my period’. One service user in PAG10 stated that he was in the middle of his second HLC prescription and hoped to be granted one more; he expressed frustration that he was not given a clear answer when he asked for clarification about this. Another service user empathised with his frustration, saying that there had been a four-week break in her period because of an injury she had in a PAG, but that she had not been given an answer about whether she would have these weeks added to her stay (PAG10). In the same session, a service user wondered whether his period would be prolonged because a holiday had fallen during his period. When talking to each other and the researcher, many service users dwelt on confusion about the HLC’s unpredictable time frames.
Unpredictability also characterised some of the oral and written information given in the HLC, resulting in an experience of hastiness and shifting information. The time frames for the HNGs were unclear from the start, and information about the duration of each session varied from two to three-and-a-half hours, which caused reactions in the first session of the course. In one situation, the time for the HNG changed, and a service user arrived at the first appointed time only to find that the session was over due to the new timetable. She had to cancel her attendance for the rest of the HNG because she had an agreement with her workplace based on the original timetable that could not be changed on short notice (HNG3). The need for predictability was expressed several times during the HNG, and one HP acknowledged this, saying, ‘I understand the need to know, and I have been telling them that it isn’t only me who needs to know, that it is important for you, too, to be able to plan the days and work and all. I do understand’ (HNG4).
3.3.2. Rhythm and Time Schedules
The findings showed a tendency in the HLC to deliver large amounts of information within limited time frames, making little room for the service users’ questions and reflections. This seemed to create an uneven rhythm in the group activities, which affected participation. This was especially visible in HNGs, in which some service users seemed to excuse themselves for asking questions through comments such as ‘…one more question, and then I won’t say anything more in this course’ (HNG4); in another session, a service user kept saying ‘sorry’ after asking questions (HNG5). Questions and reflections did not appear to be appreciated or encouraged, even though nothing was said about this explicitly. Service users may have perceived this discouragement through body language or the perceived availability of the HPs, as in the case where the HP, after talking in great detail about cholesterol, asked if there were any questions while wrinkling her nose (HNG5). Several times, the HPs ended the session with a comment about how tight the schedule was and that so much more had been planned. The tight schedule was also noticeable in that every break throughout the HNG was filled with assignments for the service users to complete. This practice seemed to make it difficult for the service users to socialise much in the HNG course, where the degree of social interaction among service users was noticeably lower than in PAGs.
Having a large amount of content and too little time may have contributed to the HPs’ confusion about what had been said and done in earlier sessions, such as when the HP in HNG2 talked about intermediate goals, asking the service users to repeat what they had discussed about intermediate goals last session. None of the service users reacted to this, and the observation notes revealed that the topic had not been mentioned in the previous session.
3.3.3. Physical Context
Although both HNGs and PAGs took place in the same building, the physical contexts for the two activities were quite different. The PAGs took place in a hall with direct access to the social area in the building’s entrance. Quite early in the observation period for PAGs, the researcher decided to arrive at least 15 min before the scheduled activity because the participants seemed to have a habit of meeting up early to socialise, with topics of conversation ranging from sports, TV programmes, and the weather to experiences of participation in the PAGs. Occasionally, service users even met up to socialise before PAGs without participating in the actual activity. The atmosphere in the social area was experienced as welcoming and stimulating (by the researcher) due to paintings and other artworks as well as a piano, which was occasionally played. The outside area was equally stimulating, with a tidy garden with statues.
The HNGs were held in different surroundings—in a conference room on a corridor on the second floor of the building. A large table took most of the room, with a narrow passage on both sides of the table. In the back of the room was a small table with cups and glasses, thermoses of coffee and tea, and two jugs of water, one with slices of cucumber and one with red pepper. At the far end of the room was a lectern with a computer for PowerPoint presentations on the blackboard on the wall. On the wall between the door and the blackboard was an information board with a poster illustrating the effects of quitting nicotine use.
The uncertainty surrounding the HNGs, described in
Section 3.3.1, was additionally affected by venue-related challenges. It was not clear to the service users or the researcher until the last session of the HNGs whether this would be the last session or not because of continuous uncertainty surrounding securing a venue for a planned practical cooking event. Because this planned event could not be carried out, the course length was reduced by several weeks.
5. Conclusions and Contribution to the Field
While other studies have examined participation from the perspectives of different actors in HLCs, this study explored participation through context-specific institutional dynamics within this setting. This focus has contributed to a broader understanding of how participation is affected by interactions and context in group activities in a Norwegian HLC.
The proposed ambiguity in facilitating participation within the HLC may be explained by understanding new approaches, such as health promotion and salutogenesis, as add-ons to a fixed, originally clinical agenda, as other studies have found [
16,
27,
28,
29]. This may result in remnants of the traditional role of the biomedically oriented HP as an expert, even though the same HP also acted as health-promoting and resource-oriented. The ambiguity was not understood as the HPs’ preferred practice, but as a result of contrasting and competing underlying values and ideals which are part of the conflict between the preventive model and the empowerment model within health promotion [
6]. The current HLC practice in Norway may be labelled secondary prevention, which is originally outside the scope of health promotion, and is considered a distraction for practitioners in the field [
49]. This ambiguous practice may lead to an unintended continuation of practice within the biomedical paradigm. However, the HLC model has been considered an innovation in health services and could be a potential contribution to reoriented health services, which is an important goal for health promotion. For such a reorientation to happen, a clarification of the underlying values and ideologies within health promotion will have to happen first. New efforts may therefore be necessary within the model of the HLC programme to increase service users’ participation in this setting. These efforts should be founded on a thorough understanding of salutogenesis and health promotion, in which participation is a core concept.




{kind=link}