
Planning for Health Equity: How Municipal Strategic Documents and Project Plans Reflect Intentions Instructed by the Norwegian Public Health Act

 , , , and
, , , and
Abstract
:1. Introduction
1.1. Regional and Local Implementation of Program for Public Health Work in Municipalities
- RQ1: Are the intentions included in municipal and project plans?
- RQ2: How are the intentions described (operationalized) and anchored in municipal and project plans, and are there differences across municipalities in this regard?
- RQ3: How is the relationship between process (knowledge-based approaches, cross-sectoral governance) and outcome (health equity) described in the documents?
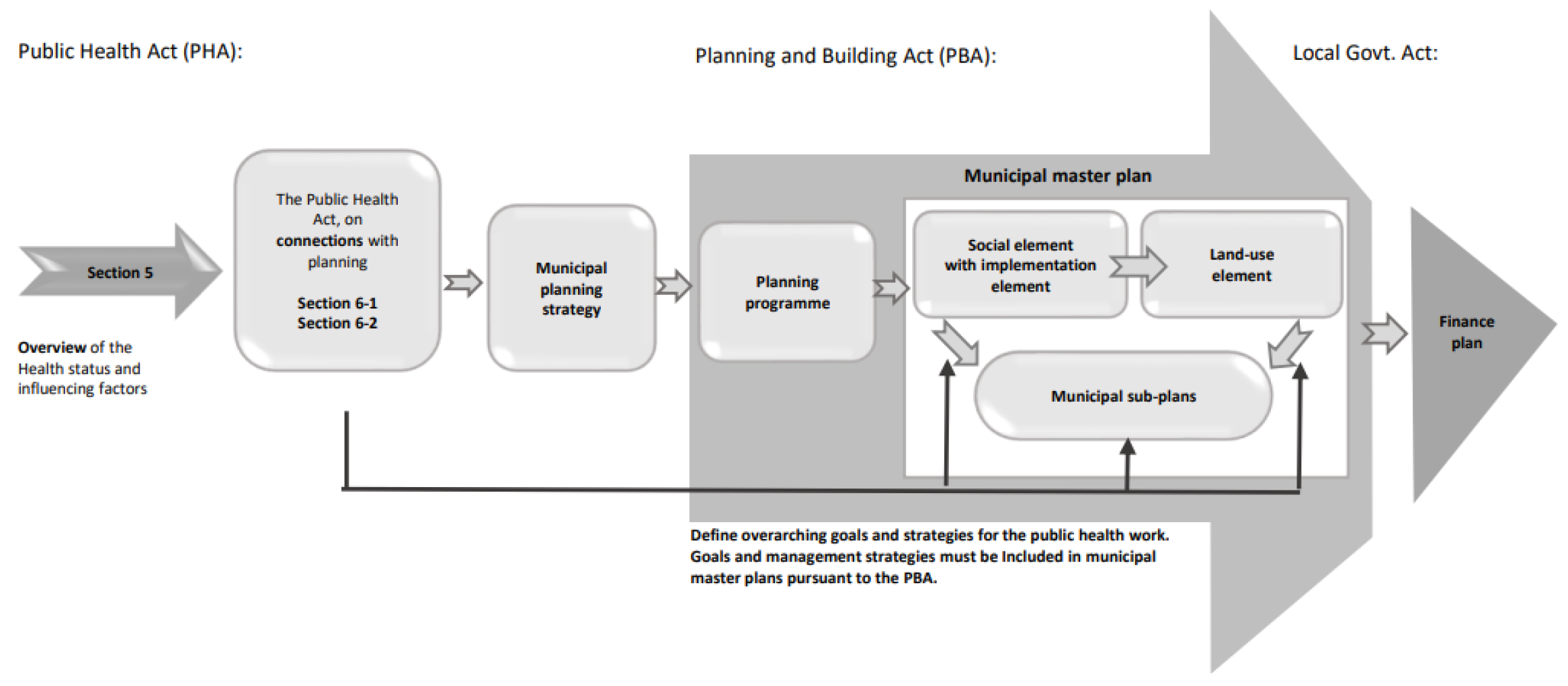
1.2. Municipal Planning
2. Methodology
- 10-year national and regional plan (Central Norway) for Program for Public Health Work in Municipalities 2017–2027 (two documents).
- Applications and municipal project plans related to participation in Program for Public Health work in Municipalities (2017–2027): (eight documents).
2.1. Data Sources and Characteristics of Municipalities
2.2. Operationalisation and Analysis
2.2.1. Step 1
Operationalisation of the Themes for Document Search
Analysis
2.2.2. Step 2
Operationalization
Analysis
3. Results
3.1. RQ1: Are the Intentions Included in Municipal and Project Plans?
3.2. RQ2: How Are the Intentions Described (Operationalized) and Anchored in Municipal and Project Plans, and Are There Differences across Municipalities in This Regard?
“Constant new knowledge and large amounts of information place new demands on employees to keep professionally updated. A goal for all professional practice is that it must be based on the best available knowledge—so-called knowledge-based practice”.
“…it has been decided that the knowledge base on public health (the overview document on public health and influencing factors) shall be used as a basis for the formulation of goals and measures at all levels of the municipality’s planning”.
“In the preparation of this strategy, the public health profile has been an essential document, together with input from business managers and an appointed cross-sectoral administrative project group”.
“Giving children and young people good conditions for growing up will have good effects for decades to come. Child health centres, kindergartens, and schools have a special position in health promotion as they meet all children at an early stage”.
3.3. RQ3: How Is the Relationship between Process (Knowledge-Based Approaches, Cross-Sectoral Governance) and Outcome (Health Equity) Described in the Documents?
“The entire project is based on cross-sectoral collaboration and show priority areas to reduce inequalities in basic social conditions. Measures can provide great benefits here because they can have a positive effect on the entire causal chain—they target the ‘causes of the causes’”.
“Choosing specific measures on the basis of a broad and complex knowledge base is demanding and requires broad collaboration”.
4. Discussion
Methodological Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministry of Health and Care Services. The Norwegian Strategy to Reduce Social Inequalities in Health 2007; Report No. 20 (2006–2007) to the Storting; Ministry of Health and Care Services: Oslo, Norway, 2007; Available online: http://www.regjeringen.no (accessed on 19 November 2022).
- van der Wel, K.A.; Dahl, E.; Bergsli, H. The Norwegian policy to reduce health inequalities: Key challenges. Nord. Welf. Res. 2016, 1, 19–29. [Google Scholar] [CrossRef] [Green Version]
- Dahl, E.; van der Wel, K.A. Nordic Health Inequalities: Patterns, trends and policies. In Health Inequalities: Critical Perspectives; Smith, K.E., Bambra, C., Eds.; Oxford University Press: New York, NY, USA, 2015. [Google Scholar]
- Ministry of Health and Care Services. Norwegian Public Health Act; Ministry of Health and Care Services: Oslo, Norway, 2011; Available online: http://www.regjeringen.no (accessed on 19 November 2022).
- Ministry of Local Government and Modernization. Norwegian Planning and Building Act; Ministry of Local Government and Modernization: Oslo, Norway, 2008; Available online: http://www.regjeringen.no (accessed on 20 November 2022).
- Ministry of Health and Care Services. The Coordination Reform—Proper Treatment—At the Right Place and Right Time; Report No. 47 (2008–2009) to the Storting; Ministry of Health and Care Services: Oslo, Norway, 2009; Available online: http://www.regjeringen.no (accessed on 20 November 2022).
- Ministry of Health and Care Services. Folkehelsemeldingen—Mestring og Muligheter; Report no. 19 (2014–2015) to the Storting; Ministry of Health and Care Services: Oslo, Norway, 2015; Available online: http://www.regjeringen.no (accessed on 20 November 2022).
- Ministry of Local Government and Modernization. The Local Government Act; Ministry of Local Government and Modernization: Oslo, Norway, 1992; Available online: http://www.regjeringen.no (accessed on 19 November 2022).
- Fosse, E.; Helgesen, M.K. Policies to Address the Social Determinants of Health in the Nordic Countries; Nordic Welfare Centre: Stockholm, Sweden, 2019; Available online: https://nordicwelfare.org/wp-content/uploads/2019/10/Rapport_Policies_SocialDeterminants_final.pdf (accessed on 5 August 2022).
- Dahl, E.; Bergsli, H.; van der Wel, K.A. Sosial Ulikhet i Helse. En Norsk Kunnskapsoversikt; Oslo and Akershus University College: Oslo, Norway, 2014; Available online: http://www.hioa.no/helseulikhet (accessed on 5 August 2022).
- Fosse, E.; Helgesen, M.K. How can local governments level the social gradient in health among families with children? The case of Norway. Int. J. Child Youth Fam. Stud. 2015, 6, 328–346. [Google Scholar] [CrossRef]
- Hagen, S.; Torp, S.; Helgesen, M.; Fosse, E. Promoting health by addressing living conditions in Norwegian municipalities. Health Promot. Int. 2016, 32, 977–987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fosse, E.; Sherriff, N.; Helgesen, M. Leveling the Social Gradient in Health at the Local Level: Applying the Gradient Equity Lens to Norwegian Local Public Health Policy. Int. J. Health Serv. 2019, 49, 538–554. [Google Scholar] [CrossRef] [PubMed]
- Dahl, E.; Elstad, J.I. Sosial Ulikhet Tar Liv; Rapport Nasjonalforeningen for Folkehelsen 9/2022; ETN Grafisk: Oslo, Norway, 2022. [Google Scholar]
- Arntzen, A.; Bøe, T.; Dahl, E.; Drange, N.; Eikemo, T.A.; Elstad, I.; Fosse, E.; Krokstad, S.; Syse, A.; Sletten, M.A.; et al. 29 recommendations to combat social inequalities in health. The Norwegian Council on Social Inequalities in Health. Scand. J. Public Health 2019, 47, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Goldblatt, P.; Castedo, A.; Allen, J.; Lionello, L.; Bell, R.; Marmot, M.; von Heimburg, D.; Ness, O. Rapid Review of Inequalities in Health and Wellbeing in Norway Since 2014; Report 3/2023; Institute of Health Equity, UCL Educational Media: London, UK, 2023. [Google Scholar]
- Office of the Auditor General of Norway. Riksrevisjonens Undersøkelse av Offentlig Folkehelsearbeid; Dokument 3:11 (2014–2015); Fagbokforlaget: Bergen, Norway, 2015; Available online: http://www.riksrevisjonen.no (accessed on 1 July 2022)ISBN 978-82-8229-322-8.
- Program for Public Health Work in Municipalities. Available online: https://www.helsedirektoratet.no/tema/folkehelsearbeid-i-kommunen/program-for-folkehelsearbeid-i-kommunene (accessed on 1 July 2022).
- Program for Public Health Work in Trøndelag. Available online: https://www.trondelagfylke.no/programmet (accessed on 1 July 2022).
- Lillefjell, M.; Magnus, E.; Knudtsen, M.S.; Wist, G.; Horghagen, S.; Espnes, G.A.; Maass, R.E.K.; Anthun, K.S. Governance for Public Health and Health Equity—The Tröndelag Model for Public Health Work. Scand. J. Public Health 2018, 46 (Suppl. S22), 37–47. [Google Scholar] [CrossRef] [PubMed]
- Lillefjell, M.; Anthun, S.S.; Maass, R.E.K.; Innstrand, S.T.; Espnes, G.A. A Salutogenic, Participatory and Settings-Based Model of Research for the Development and Evaluation of Complex Interventions: The Trøndelag Model for Public Health Work. In Global Handbook of Health Promotion Research; Innstrand, S.T., Potvin, L., Jourdan, D., Eds.; Springer: Cham, Switzerland, 13 May 2022; Volume 1. [Google Scholar]
- Lillefjell, M.; Maass, R.E.K. Involvement and Multi-Sectoral Collaboration: Applying Principles of Health Promotion during the Implementation of Local Policies and Measures—A Case Study. Societies 2022, 12, 5. [Google Scholar] [CrossRef]
- World Health Organization. WHO The Helsinki statement on health in all policies. In Proceedings of the 8th Global Conference on Health Promotion, Helsinki, Finland, 10–14 June 2013. Available online: https://www.who.int/publications/i/item/9789241506908 (accessed on 1 July 2022).
- World Health Organization (WHO). The Shanghai declaration on health promotion. In Proceedings of the 9th Global Conference on Health Promotion, Shanghai, China, 15–31 October 2016. Available online: https://www.who.int/publications/i/item/WHO-NMH-PND-17.8 (accessed on 1 July 2022).
- The Norwegian Directorate of Health. Available online: https://www.helsedirektoratet.no/veiledere/systematisk-folkehelsearbeid (accessed on 1 July 2022).
- Norwegian Planning and Building Act. 2008. Available online: https://www.regjeringen.no/en/dokumenter/planning-building-act/id570450/ (accessed on 1 July 2022).
- Bowen, G.A. Document Analysis as a Qualitative Research Method. Qual. Res. J. 2009, 9, 27–40. [Google Scholar] [CrossRef] [Green Version]
- Statistics Norway. Sentralitetsindeksen. Available online: https://www.ssb.no/befolkning/artikler-og-publikasjoner/_attachment/413602?_ts=17085d29f50 (accessed on 5 December 2022).
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Kyngäs, H.; Kaakinen, P. Deductive Content Analysis. In The Application of Content Analysis in Nursing Science Research; Kyngäs, H., Mikkonen, K., Kääriäinen, M., Eds.; Springer Nature: Cham, Switzerland, 2020. [Google Scholar] [CrossRef]
- Wagner, P.M.; Torney, D.; Ylä-Anttila, T. Governing a multilevel and cross-sectoral climate policy implementation network. Environ. Policy Gov. 2021, 31, 417–431. [Google Scholar] [CrossRef]
- Bryson, J.M.; Crosby, B.C.; Stone, M.M. The design and implementation of cross-sector collaborations: Propositions from the literature. Public Adm. Rev. 2006, 66, 44–55. [Google Scholar] [CrossRef]
- Bryson, J.M.; Crosby, B.C.; Stone, M.M. Designing and Implementing Cross-Sector Collaborations: Needed and Challenging. Public Adm. Rev. 2015, 75, 647–663. [Google Scholar] [CrossRef]


{kind=link}
| Municipalities | M1 | M2 | M3 | M4 |
|---|---|---|---|---|
| Population class pr. 1 January 2022 * | 1 | 1 | 2 | 3 |
| Area class ** | 1 | 5 | 1 | 2 |
| Residents living in urban areas on 1 January 2022 (%) | 32 | 62 | 87 | 72 |
| Centrality class *** | 6 | 5 | 3 | 3 |
| Average age per 1 January 2022 | 40.2 | 42.7 | 38.5 | 40.8 |
| Population 0–17 years old 1 January 2022 (%) | 19 | 20 | 24 | 22 |
| Population 80+ years old 1 January 2022 (%) | 4 | 6 | 4 | 5 |
| Population age 0–17 in persistently low income in the period 2018–2020 (%) | 7 | 8 | 5 | 11 |
| Population age 16+ with secondary school or higher education 2021 (%) | 24 | 27 | 38 | 29 |
| Population age 16+ with primary school as their highest education 2021 (%) | 33 | 26 | 21 | 24 |
| Type of Document | Search Theme | ||
|---|---|---|---|
| Systematic Knowledge-Based | Cross-Sectoral Governance | Health Equity | |
| Municipality I | |||
| Application 1 | 5 | 5 | 0 |
| Project plan | 6 | 3 | 4 |
| MPS * | 10 | 0 | 0 |
| MMP ** | 3 | 1 | 0 |
| MAP *** | N/A | N/A | N/A |
| Municipality II | |||
| Application | 13 | 7 | 0 |
| Project plan | 22 | 1 | 2 |
| MPS * | 1 | 1 | 2 |
| MMP ** | 3 | 2 | 0 |
| MAP *** | 0 | 0 | 1 |
| Municipality III | |||
| Application | 5 | 2 | 1 |
| Project plan | 10 | 2 | 2 |
| MPS * | 20 | 2 | 2 |
| MMP ** | 3 | 5 | 3 |
| MAP *** | 36 | 6 | 4 |
| Municipality IV | |||
| Application | 37 | 4 | 0 |
| Project plan | 24 | 1 | 0 |
| MPS * | 7 | 2 | 0 |
| MMP ** | 4 | 0 | 2 |
| MAP *** | 10 | 3 | 23 |
| Frequency across documents and municipalities | 219 | 47 | 46 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lillefjell, M.; Hope, S.; Anthun, K.S.; Hermansen, E.; Vik, J.T.; Sund, E.R.; Aasan, B.E.V.; Sylte, M.; Maass, R. Planning for Health Equity: How Municipal Strategic Documents and Project Plans Reflect Intentions Instructed by the Norwegian Public Health Act. Societies 2023, 13, 74. https://doi.org/10.3390/soc13030074
Lillefjell M, Hope S, Anthun KS, Hermansen E, Vik JT, Sund ER, Aasan BEV, Sylte M, Maass R. Planning for Health Equity: How Municipal Strategic Documents and Project Plans Reflect Intentions Instructed by the Norwegian Public Health Act. Societies. 2023; 13(3):74. https://doi.org/10.3390/soc13030074
Chicago/Turabian StyleLillefjell, Monica, Siren Hope, Kirsti Sarheim Anthun, Eirin Hermansen, John Tore Vik, Erik R. Sund, Bodil Elisabeth Valstad Aasan, Mari Sylte, and Ruca Maass. 2023. "Planning for Health Equity: How Municipal Strategic Documents and Project Plans Reflect Intentions Instructed by the Norwegian Public Health Act" Societies 13, no. 3: 74. https://doi.org/10.3390/soc13030074