
Speed Matters in Nordic Hamstring Exercise: Higher Peak Knee Flexor Force during Fast Stretch-Shortening Variant Compared to Standard Slow Eccentric Execution in Elite Athletes


Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Approach and Trial Design
2.2. Participants
2.3. Procedures
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maniar, N.; Carmichael, D.S.; Hickey, J.T.; Timmins, R.G.; San Jose, A.J.; Dickson, J.; Opar, D. Incidence and prevalence of hamstring injuries in field-based team sports: A systematic review and meta-analysis of 5952 injuries from over 7 million exposure hours. Br. J. Sports Med. 2023, 57, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Malliaropoulos, N.; Papacostas, E.; Kiritsi, O.; Papalada, A.; Gougoulias, N.; Maffulli, N. Posterior thigh muscle injuries in elite track and field athletes. Am. J. Sports Med. 2010, 38, 1813–1819. [Google Scholar] [CrossRef]
- Kerkhoffs, G.M.; van Es, N.; Wieldraaijer, T.; Sierevelt, I.N.; Ekstrand, J.; van Dijk, C.N. Diagnosis and prognosis of acute hamstring injuries in athletes. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 500–509. [Google Scholar] [CrossRef] [Green Version]
- Ekstrand, J.; Bengtsson, H.; Waldén, M.; Davison, M.; Khan, K.M.; Hägglund, M. Hamstring injury rates have increased during recent seasons and now constitute 24% of all injuries in men’s professional football: The UEFA Elite Club Injury Study from 2001/02 to 2021/22. Br. J. Sports Med. 2022, 57, 292–298. [Google Scholar] [CrossRef] [PubMed]
- De Vos, R.J.; Reurink, G.; Goudswaard, G.J.; Moen, M.H.; Weir, A.; Tol, J.L. Clinical findings just after return to play predict hamstring re-injury, but baseline MRI findings do not. Br. J. Sports Med. 2014, 48, 1377–1384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wangensteen, A.; Tol, J.L.; Witvrouw, E.; Van Linschoten, R.; Almusa, E.; Hamilton, B.; Bahr, R. Hamstring Reinjuries Occur at the Same Location and Early After Return to Sport: A Descriptive Study of MRI-Confirmed Reinjuries. Am. J. Sports Med. 2016, 44, 2112–2121. [Google Scholar] [CrossRef]
- Martin, R.L.; Cibulka, M.T.; Bolgla, L.A.; Koc, T.A., Jr.; Loudon, J.K.; Manske, R.C.; Weiss, L.; Christoforetti, J.J.; Heiderscheit, B.C. Hamstring Strain Injury in Athletes. J. Orthop. Sports Phys. Ther. 2022, 52, Cpg1–Cpg44. [Google Scholar] [CrossRef] [PubMed]
- Askling, C.; Tengvar, M.; Saartok, T.; Thorstensson, A. Sports related hamstring strains--two cases with different etiologies and injury sites. Scand. J. Med. Sci. Sports 2000, 10, 304–307. [Google Scholar] [CrossRef]
- Jokela, A.; Valle, X.; Kosola, J.; Rodas, G.; Til, L.; Burova, M.; Pleshkov, P.; Andersson, H.; Pasta, G.; Manetti, P.; et al. Mechanisms of Hamstring Injury in Professional Soccer Players: Video Analysis and Magnetic Resonance Imaging Findings. Clin. J. Sport Med. 2022, 33, 217. [Google Scholar] [CrossRef]
- Askling, C.M.; Koulouris, G.; Saartok, T.; Werner, S.; Best, T.M. Total proximal hamstring ruptures: Clinical and MRI aspects including guidelines for postoperative rehabilitation. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 515–533. [Google Scholar] [CrossRef]
- Cuthbert, M.; Ripley, N.; McMahon, J.J.; Evans, M.; Haff, G.G.; Comfort, P. The Effect of Nordic Hamstring Exercise Intervention Volume on Eccentric Strength and Muscle Architecture Adaptations: A Systematic Review and Meta-analyses. Sports Med. 2020, 50, 83–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Dyk, N.; Behan, F.P.; Whiteley, R. Including the Nordic hamstring exercise in injury prevention programmes halves the rate of hamstring injuries: A systematic review and meta-analysis of 8459 athletes. Br. J. Sports Med. 2019, 53, 1362–1370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCall, A.; Pruna, R.; Van der Horst, N.; Dupont, G.; Buchheit, M.; Coutts, A.J.; Impellizzeri, F.M.; Fanchini, M. Exercise-Based Strategies to Prevent Muscle Injury in Male Elite Footballers: An Expert-Led Delphi Survey of 21 Practitioners Belonging to 18 Teams from the Big-5 European Leagues. Sports Med. 2020, 50, 1667–1681. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, J.; Bengtsson, H.; Walden, M.; Davison, M.; Hagglund, M. Still poorly adopted in male professional football: But teams that used the Nordic Hamstring Exercise in team training had fewer hamstring injuries—A retrospective survey of 17 teams of the UEFA Elite Club Injury Study during the 2020-2021 season. BMJ Open. Sport Exerc. Med. 2022, 8, e001368. [Google Scholar] [CrossRef] [PubMed]
- Alt, T.; Roos, T.; Nolte, K.; Modenbach, D.; Knicker, A.J.; Jaitner, T. Modulating the Nordic Hamstring Exercise from ‘zero to hero’—A stepwise progression explored in a high-performance athlete. J. Athl. Train. 2022. [Google Scholar] [CrossRef]
- Augustsson, J.; Augustsson, S.R. Development of a Novel Nordic Hamstring Exercise Performance Test Device: A Reliability and Intervention Study. Sports 2022, 10, 26. [Google Scholar] [CrossRef]
- Medeiros, T.M.; Ribeiro-Alvares, J.B.; Fritsch, C.G.; Oliveira, G.S.; Severo-Silveira, L.; Pappas, E.; Baroni, B.M. Effect of Weekly Training Frequency with the Nordic Hamstring Exercise on Muscle-Strain Risk Factors in Football Players: A Randomized Trial. Int. J. Sports Physiol. Perform. 2020, 15, 1026–1033. [Google Scholar] [CrossRef]
- Timmins, R.G.; Ruddy, J.D.; Presland, J.; Maniar, N.; Shield, A.J.; Williams, M.D.; Opar, D.A. Architectural Changes of the Biceps Femoris Long Head after Concentric or Eccentric Training. Med. Sci. Sports Exerc. 2016, 48, 499–508. [Google Scholar] [CrossRef] [Green Version]
- Alegre, L.M.; Jiménez, F.; Gonzalo-Orden, J.M.; Martín-Acero, R.; Aguado, X. Effects of dynamic resistance training on fascicle length and isometric strength. J. Sports Sci. 2006, 24, 501–508. [Google Scholar] [CrossRef]
- Blazevich, A.J.; Giorgi, A. Effect of testosterone administration and weight training on muscle architecture. Med. Sci. Sports Exerc. 2001, 33, 1688–1693. [Google Scholar] [CrossRef] [Green Version]
- Linnamo, V.; Bottas, R.; Komi, P.V. Force and EMG power spectrum during and after eccentric and concentric fatigue. J. Electromyogr. Kinesiol. 2000, 10, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Mayer, F.; Horstmann, T.; Röcker, K.; Heitkamp, H.C.; Dickhuth, H.H. Normal values of isokinetic maximum strength, the strength/velocity curve, and the angle at peak torque of all degrees of freedom in the shoulder. Int. J. Sports Med. 1994, 15 (Suppl. 1), S19–S25. [Google Scholar] [CrossRef] [PubMed]
- Ünlü, G.; Çevikol, C.; Melekoğlu, T. Comparison of the Effects of Eccentric, Concentric, and Eccentric-Concentric Isotonic Resistance Training at Two Velocities on Strength and Muscle Hypertrophy. J. Strength. Cond. Res. 2020, 34, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Augustsson, J.; Andersson, H. Differences in Peak Knee Flexor Force between Eccentric-Only and Combined Eccentric-Concentric Nordic Hamstring Exercise. Sports 2023, 11, 41. [Google Scholar] [CrossRef]
- Haeger, R.M.; Rassier, D.E. Force enhancement after stretch of isolated myofibrils is increased by sarcomere length non-uniformities. Sci. Rep. 2020, 10, 21590. [Google Scholar] [CrossRef]
- Groeber, M.; Reinhart, L.; Kornfeind, P.; Baca, A. The Contraction Modalities in a Stretch-Shortening Cycle in Animals and Single Joint Movements in Humans: A Systematic Review. J. Sports Sci. Med. 2019, 18, 604–614. [Google Scholar] [PubMed]
- Mjolsnes, R.; Arnason, A.; Osthagen, T.; Raastad, T.; Bahr, R. A 10-week randomized trial comparing eccentric vs. concentric hamstring strength training in well-trained soccer players. Scand. J. Med. Sci. Sports 2004, 14, 311–317. [Google Scholar] [CrossRef]
- Salci, Y.; Yildirim, A.; Celik, O.; Ak, E.; Kocak, S.; Korkusuz, F. The effects of eccentric hamstring training on lower extremity strength and landing kinetics in recreational female athletes. Isokinet. Exerc. Sci. 2013, 21, 11–18. [Google Scholar] [CrossRef]
- Sebelien, C.; Stiller, C.H.; Maher, S.F.; Qu, X. Effects of implementing Nordic hamstring exercises for semi-professional soccer players in Akershus, Norway. Orthop. Phys. Ther. Prac. 2014, 26, 90–97. [Google Scholar]
- Wiesinger, H.P.; Gressenbauer, C.; Kosters, A.; Scharinger, M.; Muller, E. Device and method matter: A critical evaluation of eccentric hamstring muscle strength assessments. Scand. J. Med. Sci. Sports 2020, 30, 217–226. [Google Scholar] [CrossRef]
- Alt, T.; Komnik, I.; Severin, J.; Nodler, Y.T.; Benker, R.; Knicker, A.J.; Bruggemann, G.P.; Struder, H.K. Swing Phase Mechanics of Maximal Velocity Sprints-Does Isokinetic Lower-Limb Muscle Strength Matter? Int. J. Sports Physiol. Perform. 2021, 16, 974–984. [Google Scholar] [CrossRef] [PubMed]
- Alt, T.; Schmidt, M. The ANHEQ Evaluation Criteria: Introducing Reliable Rating Scales for Assessing Nordic Hamstring Exercise Quality. Sports Med. Open 2021, 7, 91. [Google Scholar] [CrossRef] [PubMed]
- Alt, T.; Nodler, Y.T.; Severin, J.; Knicker, A.J.; Strüder, H.K. Velocity-specific and time-dependent adaptations following a standardized Nordic Hamstring Exercise training. Scand. J. Med. Sci. Sports 2018, 28, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; L. Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef] [PubMed]
- Lodge, C.; Tobin, D.; O’Rourke, B.; Thorborg, K. Reliability and Validity of a New Eccentric Hamstring Strength Measurement Device. Arch. Rehabil. Res. Clin. Trans. 2020, 2, 100034. [Google Scholar] [CrossRef]
- Presland, J.D.; Opar, D.A.; Williams, M.D.; Hickey, J.T.; Maniar, N.; Lee Dow, C.; Bourne, M.N.; Timmins, R.G. Hamstring strength and architectural adaptations following inertial flywheel resistance training. J. Sci. Med. Sport. 2020, 23, 1093–1099. [Google Scholar] [CrossRef]
- Brazier, J.; Maloney, S.; Bishop, C.; Read, P.J.; Turner, A.N. Lower Extremity Stiffness: Considerations for Testing, Performance Enhancement, and Injury Risk. J. Strength. Cond. Res. 2019, 33, 1156–1166. [Google Scholar] [CrossRef] [Green Version]
- Sarabon, N.; Marusic, J.; Markovic, G.; Kozinc, Z. Kinematic and electromyographic analysis of variations in Nordic hamstring exercise. PLoS ONE 2019, 14, e0223437. [Google Scholar] [CrossRef] [Green Version]
- Marušič, J.; Sarabon, N. Comparison of electromyographic activity during Nordic hamstring exercise and exercise in lengthened position. Eur. J. Transl. Myol. 2020, 30, 8957. [Google Scholar] [CrossRef]
- Marušič, J.; Vatovec, R.; Markovic, G.; Sarabon, N. Effects of eccentric training at long-muscle length on architectural and functional characteristics of the hamstrings. Scand. J. Med. Sci. Sports 2020, 30, 2130–2142. [Google Scholar] [CrossRef]
- Blandford, L.; Theis, N.; Charvet, I.; Mahaffey, R. Is neuromuscular inhibition detectable in elite footballers during the Nordic hamstring exercise? Clin. Biomech. 2018, 58, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Monajati, A.; Larumbe-Zabala, E.; Goss-Sampson, M.; Naclerio, F. Analysis of the Hamstring Muscle Activation During two Injury Prevention Exercises. J. Hum. Kinet. 2017, 60, 29–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kruse, A.; Rivares, C.; Weide, G.; Tilp, M.; Jaspers, R.T. Stimuli for Adaptations in Muscle Length and the Length Range of Active Force Exertion—A Narrative Review. Front. Physiol. 2021, 12, 742034. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n | Mean ± SD |
|---|---|---|
| Female | 10 | |
| Male | 12 | |
| Football players | 5 | |
| Track and field athletes | 17 | |
| Age, year | 20 ± 4 | |
| Height, cm | 178 ± 8 | |
| Body mass, kg | 72 ± 8 | |
| Practice, hours per week | 11 ± 3 |
| Test Parameters | NHEECC | NHESSC | p-Value | Effect Size |
|---|---|---|---|---|
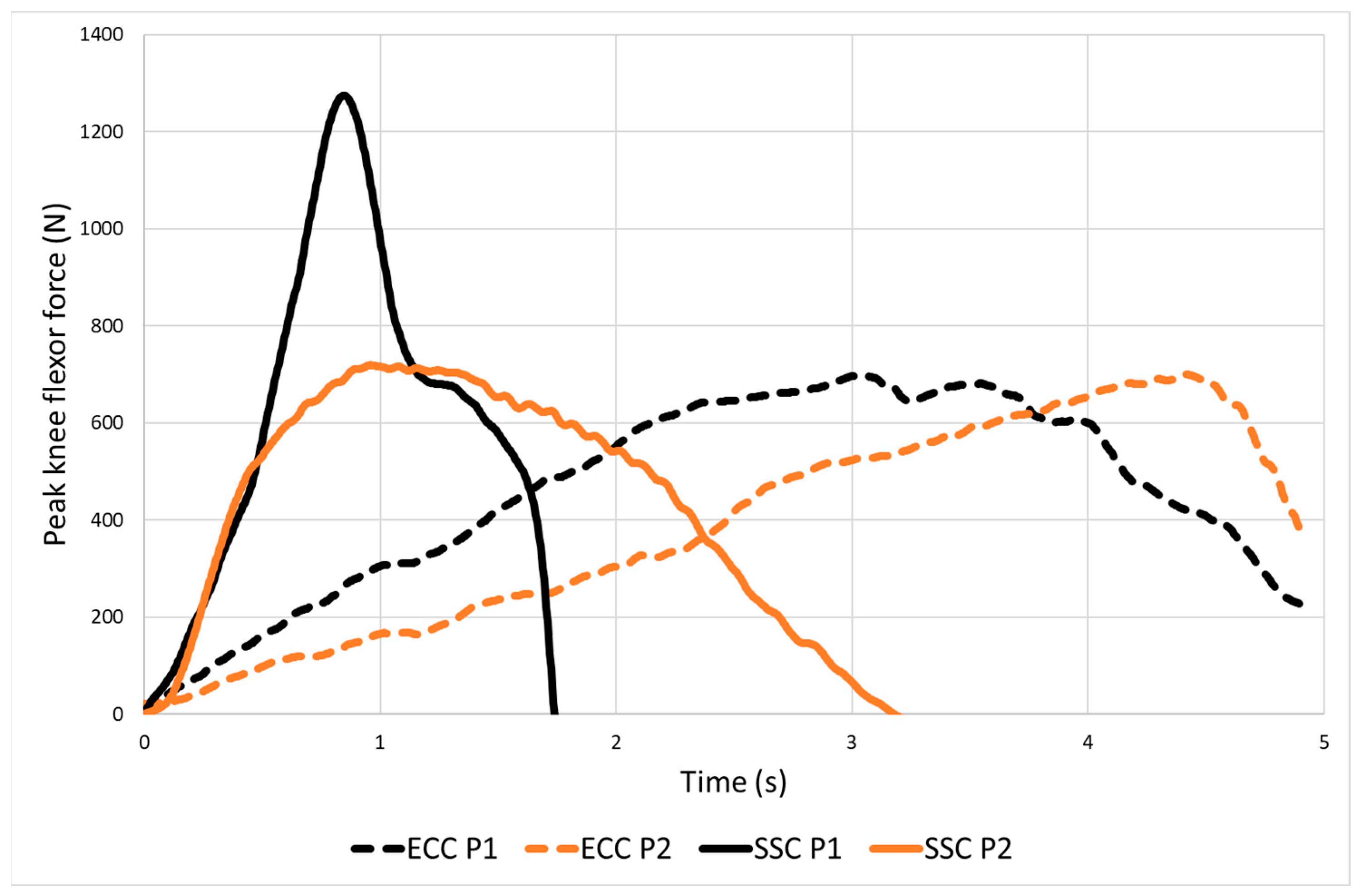
| Bilateral peak knee flexor force (N) | 726 ± 150 | 822 ± 204 | 0.008 | 0.54 |
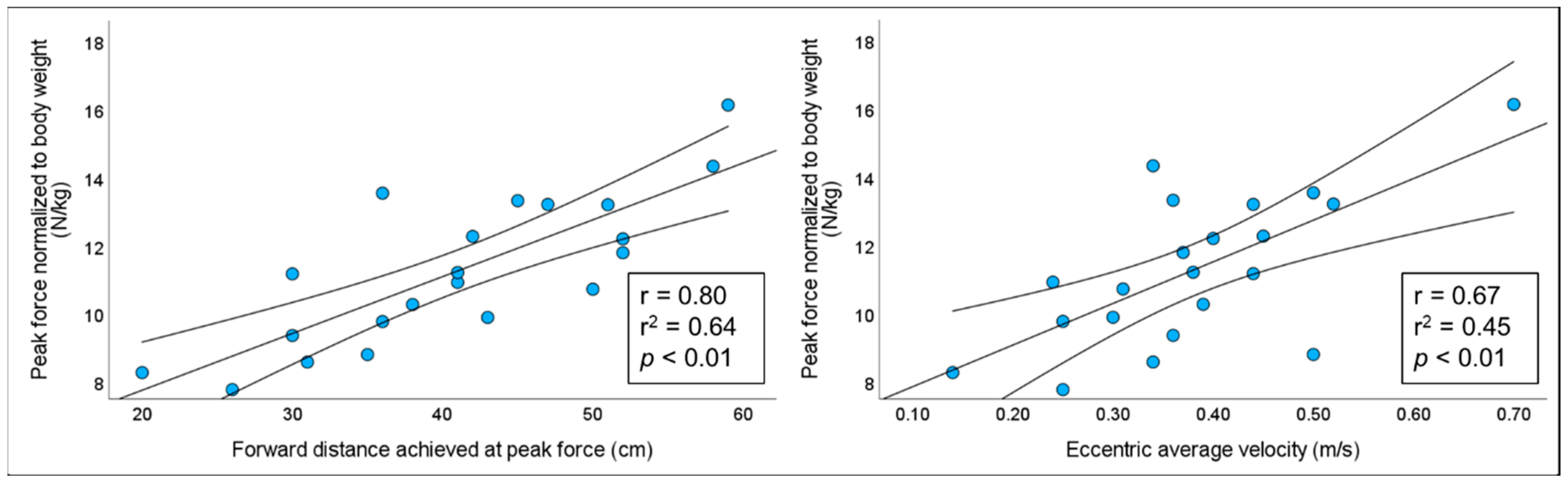
| Hip forward distance at peak force (cm) | 54 ± 9 | 41 ± 10 | 0.001 | 1.37 |
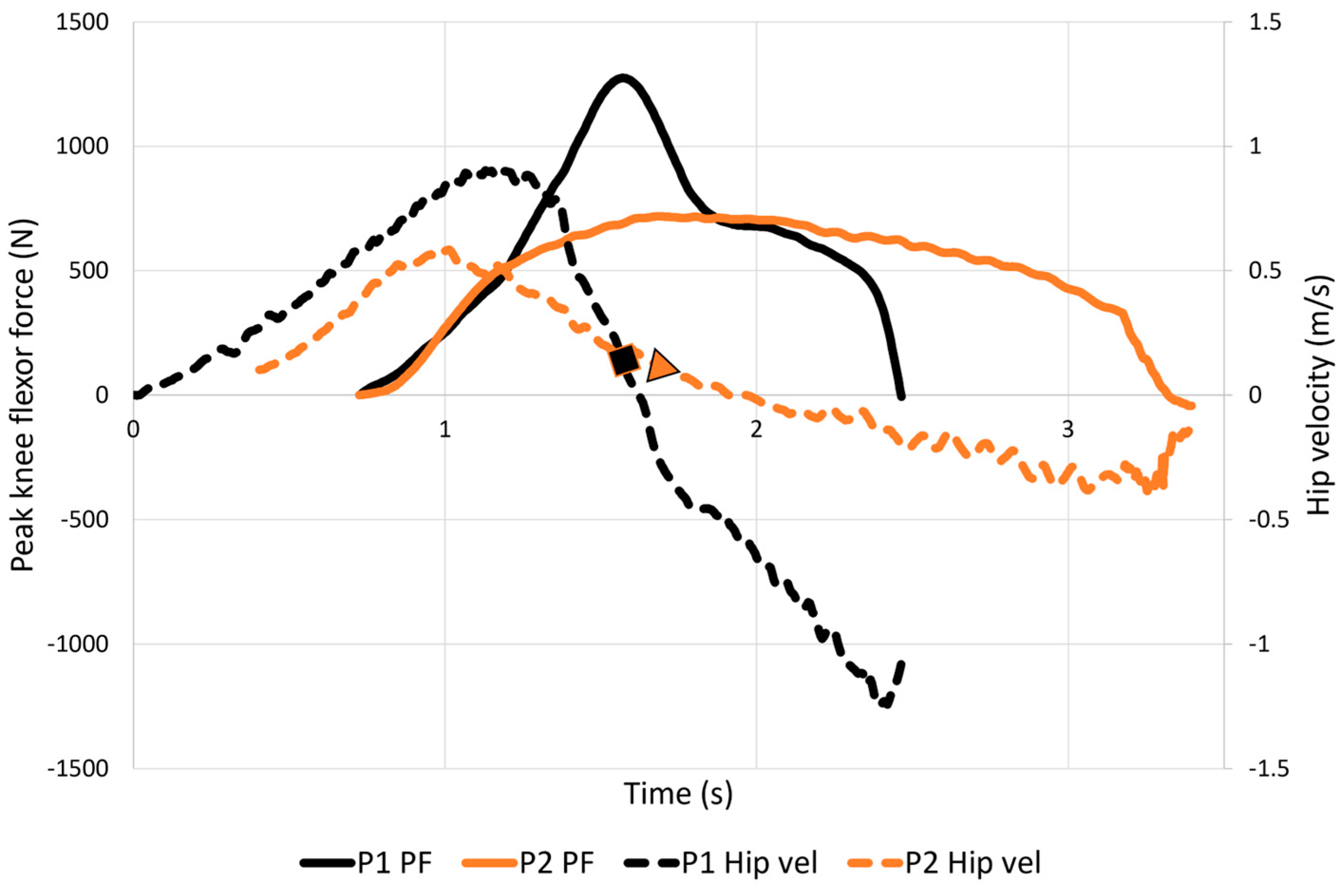
| Eccentric average velocity (m/s) | 0.12 ± 0.04 | 0.38 ± 0.12 | 0.001 | 3.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Augustsson, J.; Alt, T.; Andersson, H. Speed Matters in Nordic Hamstring Exercise: Higher Peak Knee Flexor Force during Fast Stretch-Shortening Variant Compared to Standard Slow Eccentric Execution in Elite Athletes. Sports 2023, 11, 130. https://doi.org/10.3390/sports11070130
Augustsson J, Alt T, Andersson H. Speed Matters in Nordic Hamstring Exercise: Higher Peak Knee Flexor Force during Fast Stretch-Shortening Variant Compared to Standard Slow Eccentric Execution in Elite Athletes. Sports. 2023; 11(7):130. https://doi.org/10.3390/sports11070130
Chicago/Turabian StyleAugustsson, Jesper, Tobias Alt, and Håkan Andersson. 2023. "Speed Matters in Nordic Hamstring Exercise: Higher Peak Knee Flexor Force during Fast Stretch-Shortening Variant Compared to Standard Slow Eccentric Execution in Elite Athletes" Sports 11, no. 7: 130. https://doi.org/10.3390/sports11070130