
Time Course of Performance Indexes, Oxidative Stress, Inflammation, and Muscle Damage Markers after a Female Futsal Match
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Measurements
2.3.1. Menstrual Cycle
2.3.2. Anthropometric Assessment
2.3.3. Maximal Oxygen Uptake and Heart Rate
2.3.4. Lower Limb Power and Sprint Performance
2.3.5. Subjective Muscle Soreness and Fatigue Measurements
2.3.6. Blood Sampling and Assays
2.4. Statistical Analyses
3. Results
3.1. Performance Assessments (Figure 2)
3.1.1. Counter Movement Jump

3.1.2. 10 m and 20 m Sprint
3.2. Subjective Muscle Soreness and Fatigue Measurements (Figure 3)
3.2.1. Delayed Onset Muscle Soreness

3.2.2. Rate of Perceived Exertion
3.3. Heart Rate and Blood Lactate Measurements (Figure 4)
3.3.1. Heart Rate

3.3.2. Lactate
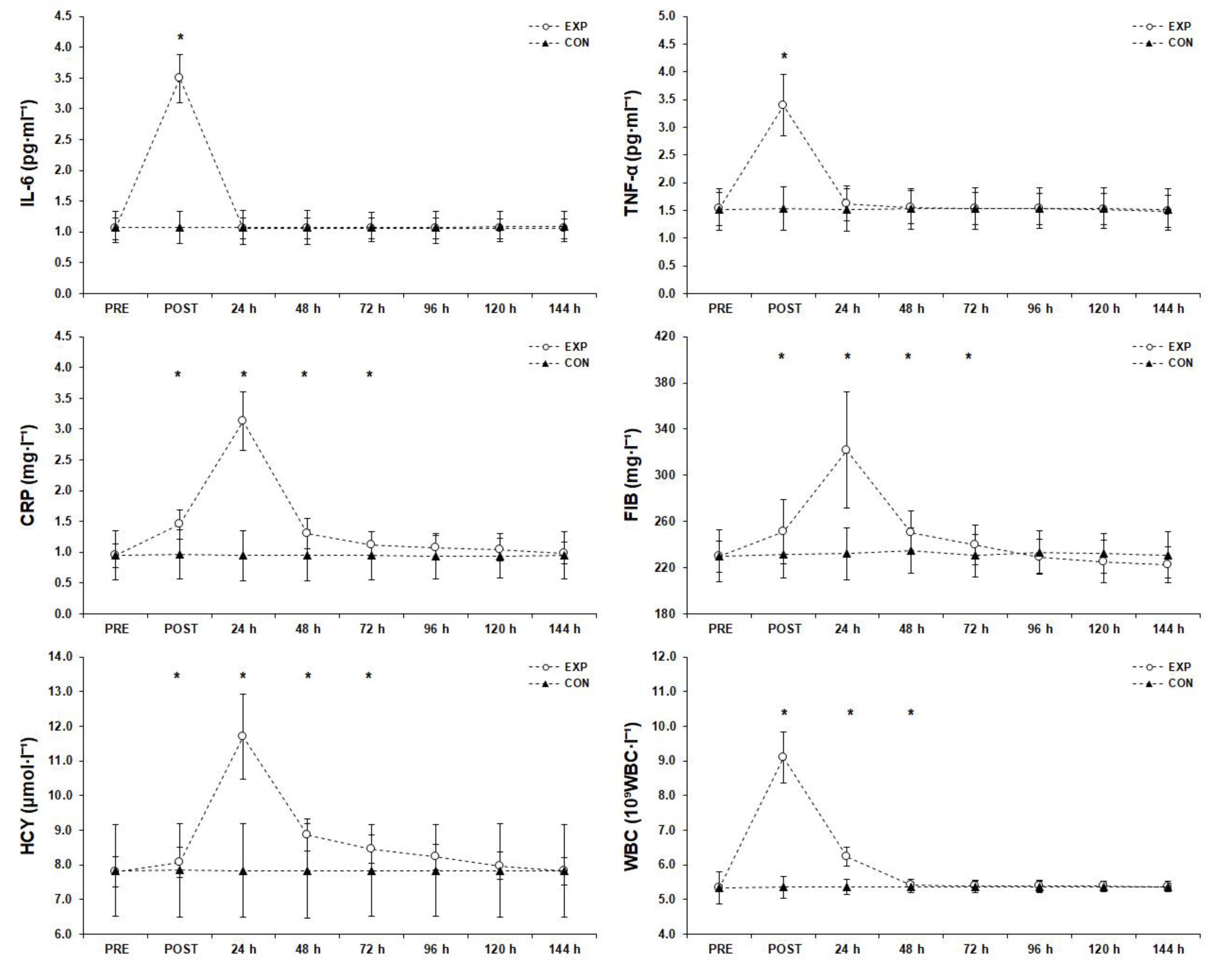
3.4. Inflammatory Responses (Figure 5)
3.4.1. Interleukin-6

3.4.2. Tumor Necrosis Factor alpha
3.4.3. C-Reactive Protein
3.4.4. Fibrinogen
3.4.5. Homocysteine
3.4.6. White Blood Cell Count
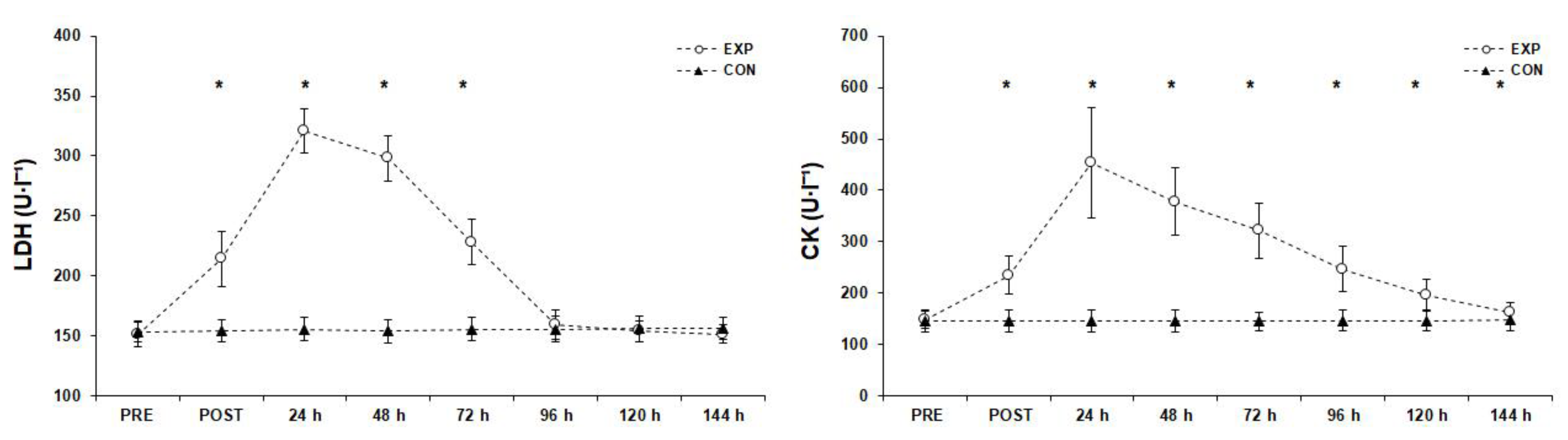
3.5. Muscle Damage Markers (Figure 6)
3.5.1. Lactate Dehydrogenase

3.5.2. Creatine Kinase
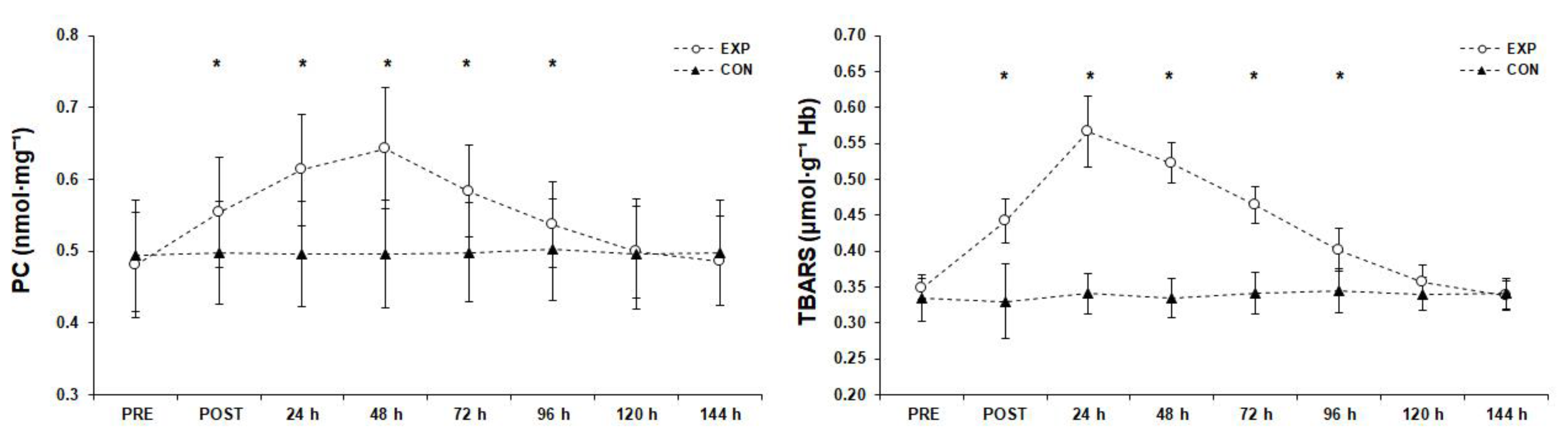
3.6. Oxidative Markers (Figure 7)
3.6.1. Protein Carbonyls

3.6.2. Thiobarbituric Acid Reactive Substances
3.7. Antioxidant Responses (Figure 8)
3.7.1. Reduced Glutathione

3.7.2. Oxidized Glutathione
3.7.3. GSH/GSSG Ratio
3.7.4. Cortisol
3.7.5. Plasma Total Antioxidant Capacity
3.7.6. Catalase
3.7.7. Uric Acid
4. Discussion
Limitations and Recommendations for Future Research, Strengths and Practical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Méndez-Dominguez, C.; Nakamura, F.Y.; Travassos, B. Editorial Futsal Research and Challenges for Sport Development. Front. Psychol. 2022, 20, 856563. [Google Scholar] [CrossRef] [PubMed]
- Beato, M.; Coratella, G.; Schena, F. Brief review of the state of art in Futsal. J. Sport. Med. Phys. Fit. 2016, 56, 428–432. [Google Scholar]
- Barbero-Alvarez, J.C.; Subiela, J.V.; Granda-Vera, J.; Castagna, C.; Gómez, M.; Del Coso, J. Aerobic fitness and performance in elite female futsal players. Biol. Sport 2015, 32, 339–344. [Google Scholar] [CrossRef]
- Makaje, N.; Ruangthai, R.; Arkarapanthu, A.; Yoopat, P. Physiological demands and activity profiles during futsal match play according to competitive level. J. Sports Med. Phys. Fit. 2012, 52, 366–374. [Google Scholar]
- Naser, N.; Ali, A.; Macadam, P. Physical and physiological demands of futsal. J. Exerc. Sci. Fit. 2017, 15, 76–80. [Google Scholar] [CrossRef]
- Castagna, C.; D’Ottavio, S.; Vera, J.G.; Álvarez, J.C.B. Match demands of professional Futsal: A case study. J. Sci. Med. Sport 2009, 12, 490–494. [Google Scholar] [CrossRef]
- Milioni, F.; Vieira, L.H.P.; Barbieri, R.A.; Zagatto, A.M.; Nordsborg, N.B.; Barbieri, F.A.; dos-Santos, J.W.; Santiago, P.R.P.; Papoti, M. Futsal match-related fatigue affects running performance and neuromuscular parameters but not finishing kick speed or accuracy. Front. Physiol. 2016, 7, 518. [Google Scholar] [CrossRef]
- Oliva-Lozano, J.M.; Muyor, J.M.; Puche Ortuño, D.; Rico-González, M.; Pino-Ortega, J. Analysis of key external and internal load variables in professional female futsal players: A longitudinal study. Res. Sport. Med. 2021, 1–10. [Google Scholar] [CrossRef]
- Beato, M.; Coratella, G.; Schena, F.; Hulton, A.T. Evaluation of the external and internal workload in female futsal players. Biol. Sport 2017, 34, 227–231. [Google Scholar] [CrossRef]
- Ruiz-Pérez, I.; López-Valenciano, A.; Jiménez-Loaisa, A.; Elvira, J.L.L.; De Ste Croix, M.; Ayala, F. Injury incidence, characteristics and burden among female sub-elite futsal players: A prospective study with three-year follow-up. PeerJ 2019, 7, e7989. [Google Scholar] [CrossRef]
- Ispirlidis, I.; Fatouros, I.G.; Jamurtas, A.Z.; Nikolaidis, M.G.; Michailidis, I.; Douroudos, I.; Margonis, K.; Chatzinikolaou, A.; Kalistratos, E.; Katrabasas, I.; et al. Time-course of changes in inflammatory and performance responses following a soccer game. Clin. J. Sport Med. 2008, 18, 423–431. [Google Scholar] [CrossRef]
- Wilke, J.; Behringer, M. Is “delayed onset muscle soreness” a false friend? The potential implication of the fascial connective tissue in post-exercise discomfort. Int. J. Mol. Sci. 2021, 22, 9482. [Google Scholar] [CrossRef]
- Hitzschke, B.; Wiewelhove, T.; Raeder, C.; Ferrauti, A.; Meyer, T.; Pfeiffer, M.; Kellmann, M.; Kölling, S. Evaluation of psychological measures for the assessment of recovery and stress during a shock-microcycle in strength and high-intensity interval training. Perform. Enhanc. Health 2017, 5, 147–157. [Google Scholar] [CrossRef]
- Brancaccio, P.; Maffulli, N.; Buonauro, R.; Limongelli, F.M. Serum Enzyme Monitoring in Sports Medicine. Clin. Sport. Med. 2008, 27, 1–18. [Google Scholar] [CrossRef]
- Philippou, A.; Bogdanis, G.; Maridaki, M.; Halapas, A.; Sourla, A.; Koutsilieris, M. Systemic cytokine response following exercise-induced muscle damage in humans. Clin. Chem. Lab. Med. 2009, 47, 777–782. [Google Scholar] [CrossRef]
- Philippou, A.; Maridaki, M.; Tenta, R.; Koutsilieris, M. Hormonal responses following eccentric exercise in humans. Hormones 2017, 16, 405–413. [Google Scholar] [CrossRef]
- Silva, J.R.; Ascensão, A.; Marques, F.; Seabra, A.; Rebelo, A.; Magalhães, J. Neuromuscular function, hormonal and redox status and muscle damage of professional soccer players after a high-level competitive match. Eur. J. Appl. Physiol. 2013, 113, 2193–2201. [Google Scholar] [CrossRef]
- De Moura, N.R.; Borges, L.S.; Santos, V.C.; Joel, G.B.; Bortolon, J.R.; Hirabara, S.M.; Cury-Boaventura, M.F.; Pithon-Curi, T.C.; Curi, R.; Hatanaka, E. Muscle lesions and inflammation in futsal players according to their tactical positions. J. Strength Cond. Res. 2013, 27, 2612–2618. [Google Scholar] [CrossRef]
- Philippou, A.; Maridaki, M.; Theos, A.; Koutsilieris, M. Cytokines in muscle damage. Adv. Clin. Chem. 2012, 58, 49–87. [Google Scholar] [CrossRef]
- Pedersen, B.K. Exercise and cytokines. Immunol. Cell Biol. 2000, 78, 532–535. [Google Scholar] [CrossRef]
- Owen, A.L.; Djaoui, L.; Dellal, A.; Ates, O.; Mendes, B.; Lyon, C. Biochemical Response Comparisons of a Competitive Microcycle Vs. Congested Fixture Periods in Elite Level European Champions League Soccer Players. J. Complement. Med. Altern. Healthc. 2019, 10, 555778. [Google Scholar] [CrossRef]
- Oliveira, R.S.; Leicht, A.S.; Bishop, D.; Barbero-Álvarez, J.C.; Nakamura, F.Y. Seasonal changes in physical performance and heart rate variability in high level futsal players. Int. J. Sport. Med. 2013, 34, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, V.M.; Ramos, G.P.; Mendes, T.T.; Cabido, C.E.; Melo, E.S.; Condessa, L.A.; Coelho, D.B.; Garcia, E.S. Intensity of official Futsal matches. J. Strength Cond. Res. 2011, 25, 2482–2487. [Google Scholar] [CrossRef] [PubMed]
- Leite, W.S.S. Physiological Demands in Footbal, Futsal, and Beach Soccer: A Brief Review. Eur. J. Phys. Educ. Sport Sci. 2016, 2, 1–10. [Google Scholar] [CrossRef]
- Fatouros, I.G.; Chatzinikolaou, A.; Douroudos, I.I.; Nikolaidis, M.G.; Kyparos, A.; Margonis, K.; Michailidis, Y.; Vantarakis, A.; Taxildaris, K.; Katrabasas, I.; et al. Time-course of changes in oxidative stress and antioxidant status responses following a soccer game. J. Strength Cond. Res. 2010, 24, 3278–3286. [Google Scholar] [CrossRef]
- Souglis, A.; Bogdanis, G.C.; Chryssanthopoulos, C.; Apostolidis, N.; Geladas, N.D. Time course of oxidative stress, inflammation, and muscle damage markers for 5 days after a soccer match: Effects of sex and playing position. J. Strength Cond. Res. 2018, 32, 2045–2054. [Google Scholar] [CrossRef]
- Souglis, A.; Travlos, A.K. The influence of competitive activity on selected biochemical and haematological parameters of amateur soccer athletes. J. Phys. Educ. Sport 2015, 15, 24–31. [Google Scholar] [CrossRef]
- Bekris, E.; Bourdas, D.I.; Mylonis, E.; Ispirlidis, I.; Zacharakis, E.D.; Katis, A. Effect of 3 vs. 3 Soccer Small-Sided Game on Various Performance, Inflammatory, Muscle Damage and Hormonal Indicators in Semi-Professional Players. Sports 2022, 10, 102. [Google Scholar] [CrossRef]
- Da Costa, C.S.C.; Palma, A.; Pedrosa, C.M.; Pierucci, A.P.T.R. Female Futsal Players’ Profile and Biochemical Alterations through Intermittent High-Intensity Exercise Training. Food Nutr. Sci. 2012, 3, 110–116. [Google Scholar] [CrossRef]
- Stålnacke, B.M.; Ohlsson, A.; Tegner, Y.; Sojka, P. Serum concentrations of two biochemical markers of brain tissue damage S-100B and neurone specific enolase are increased in elite female soccer players after a competitive game. Br. J. Sport. Med. 2006, 40, 313–316. [Google Scholar] [CrossRef]
- Bassett, A.J.; Ahlmen, A.; Rosendorf, J.M.; Romeo, A.A.; Erickson, B.J.; Bishop, M.E. The biology of sex and sport. JBJS Rev. 2020, 8, e0140. [Google Scholar] [CrossRef]
- Cury-Boaventura, M.F.; Gorjão, R.; de Moura, N.R.; Santos, V.C.; Bortolon, J.R.; Murata, G.M.; da Silva Borges, L.; Momesso, C.M.; Dermargos, A.; Pithon-Curi, T.C.; et al. The effect of a competitive futsal match on T Lymphocyte surface receptor signaling and functions. Front. Physiol. 2018, 9, 202. [Google Scholar] [CrossRef]
- Bourdas, D.I.; Zacharakis, E.D. Impact of COVID-19 Lockdown on Physical Activity in a Sample of Greek Adults. Sports 2020, 8, 139. [Google Scholar] [CrossRef]
- Bourdas, D.I.; Zacharakis, E.D. Evolution of changes in physical activity over lockdown time: Physical activity datasets of four independent adult sample groups corresponding to each of the last four of the six COVID-19 lockdown weeks in Greece. Data Br. 2020, 32, 106301. [Google Scholar] [CrossRef]
- Warburton, D.; Jamnik, V.; Bredin, S.; Gledhill, N. The 2018 Physical Activity Readiness Questionnaire for Everyone (PAR-Q+) and electronic Physical Activity Readiness Medical Examination (ePARmed-X+). Health Fit. J. Can. 2018, 11, 31–34. [Google Scholar] [CrossRef]
- Bourdas, D.I.; Zacharakis, E.D.; Travlos, A.K.; Souglis, A.; Georgali, T.I.; Gofas, D.C.; Ktistakis, I.E.; Deltsidou, A. Impact of lockdown on smoking and sleeping in the early COVID-19 presence: Datasets of Greek Adults sample. Data Br. 2021, 39, 107480. [Google Scholar] [CrossRef]
- McKay, A.K.A.; Stellingwerff, T.; Smith, E.S.; Martin, D.T.; Mujika, I.; Goosey-Tolfrey, V.L.; Sheppard, J.; Burke, L.M. Defining Training and Performance Caliber: A Participant Classification Framework. Int. J. Sport. Physiol. Perform. 2022, 17, 317–331. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services; Healthier.gov. Physical Activity Guidelines for Americans; U.S. Department of Health and Human Services: Washington, DC, USA, 2008.
- Speroff, L.; Vande Wiele, R.L. Regulation of the human menstrual cycle. Am. J. Obstet. Gynecol. 1971, 109, 234–247. [Google Scholar] [CrossRef]
- Carmichael, M.A.; Thomson, R.L.; Moran, L.J.; Wycherley, T.P. The impact of menstrual cycle phase on athletes’ performance: A narrative review. Int. J. Environ. Res. Public Health 2021, 18, 1667. [Google Scholar] [CrossRef]
- World Medical Association Declaration of Helsinki, Ethical Principles for Scientific Requirements and Research Protocols. 2013. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 1 October 2022).
- Cadegiani, F.A.; Kater, C.E. Novel insights of overtraining syndrome discovered from the EROS study. BMJ Open Sport Exerc. Med. 2019, 5, e000542. [Google Scholar] [CrossRef]
- Bourdas, D.I.; Souglis, A.; Zacharakis, E.D.; Geladas, N.D.; Travlos, A.K. Meta-Analysis of Carbohydrate Solution Intake during Prolonged Exercise in Adults: From the Last 45+ Years’ Perspective. Nutrients 2021, 13, 4223. [Google Scholar] [CrossRef] [PubMed]
- Deltsidou, A.; Zarikas, V.; Mastrogiannis, D.; Kapreli, E.; Bourdas, D.; Raftopoulos, V.; Noula, M.; Lykeridou, K. Data on advanced glycation end-products concentrations and haemodynamic parameters following caffeine and nicotine consumption in nursing students. Data Br. 2020, 32, 106063. [Google Scholar] [CrossRef] [PubMed]
- Havenetidis, K.; Bourdas, D. Creatine supplementation: Effects on urinary excretion and anaerobic performance. J. Sport. Med. Phys. Fit. 2003, 43, 347–355. [Google Scholar]
- Nevill, A.M.; Metsios, G.S.; Jackson, A.S.; Wang, J.; Thornton, J.; Gallagher, D. Can we use the Jackson and Pollock equations to predict body density/fat of obese individuals in the 21st century? Int. J. Body Compos. Res. 2008, 6, 114–121. [Google Scholar] [PubMed]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Riebe, D., Ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2018; ISBN 9781496339065. [Google Scholar]
- Clemente, F.M.; Nikolaidis, P.T.; Rosemann, T.; Knechtle, B. Dose-response relationship between external load variables, body composition, and fitness variables in professional soccer players. Front. Physiol. 2019, 10, 443. [Google Scholar] [CrossRef]
- Van Melick, N.; Meddeler, B.M.; Hoogeboom, T.J.; Nijhuis-van der Sanden, M.W.G.; van Cingel, R.E.H. How to determine leg dominance: The agreement between self-reported and observed performance in healthy adults. PLoS ONE 2017, 12, e0189876. [Google Scholar] [CrossRef]
- Nosaka, K.; Sacco, P.; Mawatari, K. Effects of amino acid supplementation on muscle soreness and damage. Int. J. Sport Nutr. Exerc. Metab. 2006, 16, 620–635. [Google Scholar] [CrossRef]
- Borg, G.A.V. Psychophysical bases of perceived exertion. Med. Sci. Sport. Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Reddy, Y.N.; Murthy, S.V.; Krishna, D.R.; Prabhakar, M.C. Role of Free Radicals and Antioxidants in Tuberculosis Patients. Indian J. Tuberc. 2004, 51, 213–218. [Google Scholar]
- Tietze, F. Enzymic method for quantitative determination of nanogram amounts of total and oxidized glutathione: Applications to mammalian blood and other tissues. Anal. Biochem. 1969, 27, 502–522. [Google Scholar] [CrossRef]
- Suen, K.F.K.; Lee, G.R.; Finnegan, M.; Halton, K.; Borovickova, I.; Trench, C.; Fitzgibbon, M.C. Total plasma homocysteine measurement: Evaluation of the Abbott immunoassay, comparison with the JEOL ion exchange chromatography and investigation of its clinical utility. Pract. Lab. Med. 2022, 32, e00295. [Google Scholar] [CrossRef]
- Myint, P.K.; Luben, R.N.; Wareham, N.J.; Welch, A.A.; Bingham, S.A.; Khaw, K.T. Physical activity and fibrinogen concentrations in 23,201 men and women in the EPIC-Norfolk population-based study. Atherosclerosis 2008, 198, 419–425. [Google Scholar] [CrossRef]
- Clauss, A. Gerinnungsphysiologische Schnellmethode zur Bestimmung des Fibrinogens [Rapid physiological coagulation method in determination of fibrinogen]. Acta Haematol. 1954, 17, 237–246. [Google Scholar] [CrossRef]
- Janaszewska, A.; Bartosz, G. Assay of total antioxidant capacity: Comparison of four methods as applied to human blood plasma. Scand. J. Clin. Lab. Investig. 2002, 62, 231–236. [Google Scholar] [CrossRef]
- Aebi, H. Catalase in vitro. Methods Enzymol. 1984, 105, 121–126. [Google Scholar] [CrossRef]
- Patsoukis, N.; Zervoudakis, G.; Panagopoulos, N.T.; Georgiou, C.D.; Angelatou, F.; Matsokis, N.A. Thiol redox state (TRS) and oxidative stress in the mouse hippocampus after pentylenetetrazol-induced epileptic seizure. Neurosci. Lett. 2004, 357, 83–86. [Google Scholar] [CrossRef]
- Keles, M.S.; Taysi, S.; Sen, N.; Aksoy, H.; Akçay, F. Effect of corticosteroid therapy on serum and CSF malondialdehyde and antioxidant proteins in multiple sclerosis. Can. J. Neurol. Sci. 2001, 28, 141–143. [Google Scholar] [CrossRef]
- Keppel, G.; Wickens, T.D. Design and Analysis: A Researcher’s Handbook, 4th ed.; Pearson Education, Inc.: Upper Saddle River, NJ, USA, 2004; ISBN 978-0135159415. [Google Scholar]
- Meyers, L.S.; Gamst, G.; Guarino, A.J. Applied Multivariate Research Design and Interpretation, 3rd ed.; SAGE Publications Inc.: Newbury Park, CA, USA, 2016; ISBN 978-1506329765. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Nemčić, T.; Calleja-González, J. Evidence-based recovery strategies in futsal: A narrative review. Kinesiology 2021, 1, 131–140. [Google Scholar] [CrossRef]
- Andersson, H.; Karlsen, A.; Blomhoff, R.; Raastad, T.; Kadi, F. Plasma antioxidant responses and oxidative stress following a soccer game in elite female players. Scand. J. Med. Sci. Sport 2010, 20, 600–608. [Google Scholar] [CrossRef]
- Steensberg, A.; Fischer, C.P.; Keller, C.; Møller, K.; Pedersen, B.K. IL-6 enhances plasma IL-1ra, IL-10, and cortisol in humans. Am. J. Physiol. Endocrinol. Metab. 2003, 285, 433–437. [Google Scholar] [CrossRef]
- Florini, J.R. Hormonal control of muscle growth. Muscle Nerve 1987, 10, 577–598. [Google Scholar] [CrossRef] [PubMed]
- Impellizzeri, F.M.; Rampinini, E.; Coutts, A.J.; Sassi, A.; Marcora, S.M. Use of RPE-based training load in soccer. Med. Sci. Sport. Exerc. 2004, 36, 1042–1047. [Google Scholar] [CrossRef] [PubMed]
- Miloski, B.; Moreira, A.; Caetano, F.; Nogueira, D.A.; Freitas, V. De Do physical fitness measures influence internal training load responses in high-level futsal players? J. Sport Med. Phys. Fit. 2014, 54, 588–594. [Google Scholar]
- Paulsen, G.; Mikkelsen, U.R.; Raastad, T.; Peake, J.M. Leucocytes, cytokines and satellite cells: What role do they play in muscle damage and regeneration following eccentric exercise? Exerc. Immunol. Rev. 2012, 18, 42–97. [Google Scholar]
- Chatzinikolaou, A.; Christoforidis, C.; Avloniti, A.; Draganidis, D.; Jamurtas, A.Z.; Stampoulis, T.; Ermidis, G.; Sovatzidis, A.; Papassotiriou, I.; Kambas, A.; et al. A Microcycle of Inflammation Following a Team Handball Game. J. Strength Cond. Res. 2014, 28, 1981–1994. [Google Scholar] [CrossRef]
- Malm, C.; Nyberg, P.; Engstrom, M.; Sjodim, B.; Lenkei, R.; Ekblom, B.; Lundberg, I. Immunological changes in human skeletal muscle and blood after eccentric exercise and multiple biopsies. J. Physiol. 2000, 529, 243–262. [Google Scholar] [CrossRef]
- Devrnja, A.; Matković, B.R. The effects of a soccer match on muscle damage indicators. Kinesiology 2018, 50, 112–123. [Google Scholar] [CrossRef]
- Souglis, A.G.; Papapanagiotou, A.; Bogdanis, G.C.; Travlos, A.K.; Apostolidis, N.G.; Geladas, N.D. Comparison of inflammatory responses to a soccer match between elite male and female players. J. Strength Cond. Res. 2015, 29, 1227–1233. [Google Scholar] [CrossRef]
- De Moura, N.R.; Cury-Boaventura, M.F.; Santos, V.C.; Levada-Pires, A.C.; Bortolon, J.R.; Fiamoncini, J.; Pithon-Curi, T.C.; Curi, R.; Hatanaka, E. Inflammatory response and neutrophil functions in players after a futsal match. J. Strength Cond. Res. 2012, 26, 2507–2514. [Google Scholar] [CrossRef]
- Reihmane, D.; Dela, F. Interleukin-6: Possible biological roles during exercise. Eur. J. Sport Sci. 2014, 14, 242–250. [Google Scholar] [CrossRef]
- Da Rocha, A.L.; Pinto, A.P.; Kohama, E.B.; Pauli, J.R.; de Moura, L.P.; Cintra, D.E.; Ropelle, E.R.; da Silva, A.S.R. The proinflammatory effects of chronic excessive exercise. Cytokine 2019, 119, 57–61. [Google Scholar] [CrossRef]
- Ghafourian, M.; Ashtary-Larky, D.; Chinipardaz, R.; Eskandary, N.; Mehavaran, M. Inflammatory biomarkers’ response to two different intensities of a single bout exercise among soccer players. Iran. Red Crescent Med. J. 2016, 18, 2–9. [Google Scholar] [CrossRef]
- Jamurtas, A.Z.; Fatouros, I.G.; Deli, C.K.; Georgakouli, K.; Poulios, A.; Draganidis, D.; Papanikolaou, K.; Tsimeas, P.; Chatzinikolaou, A.; Avloniti, A.; et al. The effects of acute low-volume HIIT and aerobic exercise on leukocyte count and redox status. J. Sport Sci. Med. 2018, 17, 501–508. [Google Scholar]
- Simioni, C.; Zauli, G.; Martelli, A.M.; Vitale, M.; Sacchetti, G.; Gonelli, A.; Neri, L.M. Oxidative stress: Role of physical exercise and antioxidant nutraceuticals in adulthood and aging. Oncotarget 2018, 9, 17181–17198. [Google Scholar] [CrossRef]
- Bogdanis, G.C.; Stavrinou, P.; Fatouros, I.G.; Philippou, A.; Chatzinikolaou, A.; Draganidis, D.; Ermidis, G.; Maridaki, M. Short-term high-intensity interval exercise training attenuates oxidative stress responses and improves antioxidant status in healthy humans. Food Chem. Toxicol. 2013, 61, 171–177. [Google Scholar] [CrossRef]
- Goodwin, M.L.; Harris, J.E.; Hernández, A.; Gladden, L.B. Blood lactate measurements and analysis during exercise: A guide for clinicians. J. Diabetes Sci. Technol. 2007, 1, 558–569. [Google Scholar] [CrossRef]
- Romero-Parra, N.; Alfaro-Magallanes, V.M.; Rael, B.; Cupeiro, R.; Rojo-Tirado, M.A.; Benito, P.J.; Peinado, A.B. IronFEMME Study Group Indirect Markers of Muscle Damage Throughout the Menstrual Cycle. Int. J. Sport. Physiol. Perform. 2021, 16, 190–198. [Google Scholar] [CrossRef]
- Romero-Parra, N.; Cupeiro, R.; Alfaro-Magallanes, V.M.; Rael, B.; Rubio-Arias, J.Á.; Peinado, A.B.; Benito, P.J. IronFEMME Study Group Exercise-Induced Muscle Damage During the Menstrual Cycle: A Systematic Review and Meta-Analysis. J. Strength Cond. Res. 2021, 35, 549–561. [Google Scholar] [CrossRef]
- McNulty, K.L.; Elliott-Sale, K.J.; Dolan, E.; Swinton, P.A.; Ansdell, P.; Goodall, S.; Thomas, K.; Hicks, K.M. The Effects of Menstrual Cycle Phase on Exercise Performance in Eumenorrheic Women: A Systematic Review and Meta-Analysis. Sport Med. 2020, 50, 1813–1827. [Google Scholar] [CrossRef]
- Queiroga, M.R.; da Silva, D.F.; Ferreira, S.A.; Weber, V.M.R.; Fernandes, D.Z.; Cavazzotto, T.G.; Portela, B.S.; Tartaruga, M.P.; Nascimento, M.A.; Vieira, E.R. Characterization of Reproductive and Morphological Variables in Female Elite Futsal Players. Front. Psychol. 2021, 12, 625354. [Google Scholar] [CrossRef]
- Matsuda, T.; Ogata, H.; Kanno, M.; Ishikawa, A.; Yamada, M.; Sakamaki-Sunaga, M. Effects of the menstrual cycle on oxidative stress and antioxidant response to high-intensity intermittent exercise until exhaustion in healthy women. J. Sport Med. Phys. Fit. 2020, 60, 1335–1341. [Google Scholar] [CrossRef] [PubMed]
- Bourdas, D.I.; Zacharakis, E.D.; Travlos, A.K.; Souglis, A. Return to Basketball Play Following COVID-19 Lockdown. Sports 2021, 9, 81. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Experimental | Control |
|---|---|---|
| Age (y) | 22.6 ± 2.1 [21.9–23.3] | 22.3 ± 2.6 [21.4–23.3] |
| Height (cm) | 167.4 ± 3.6 [166.1–168.6] | 166.6 ± 4.6 [164.9–168.2] |
| Body mass (kg) | 57.5 ± 3.0 [56.5–58.5] | 56.8 ± 3.4 [55.6–58.0] |
| Body fat (%) | 16.9 ± 0.8 [16.6–17.1] | 16.6 ± 1 [16.2–16.9] |
| ⩒O2max (ml·kg−1·min−1) | 54.6 ± 1.5 [54.1–55.2] | 54.0 ± 1.4 [53.5–54.5] |
| Training period (y) | 12.5 ± 2.3 [11.7–13.3] | 12.4 ± 2.3 [11.6–13.3] |
| Training volume (min·week−1) | 285.0 ± 36.3 [272.8–297.2] | 274.7 ± 34.7 [262.2–287.1] |
| Training frequency (times·week−1) | 5.3 ± 0.8 [5.0–5.6] | 5.2 ± 0.9 [4.8–5.5] |
| Menarche age (y) | 13.1 ± 1.0 [12.7–13.4] | 13.0 ± 1.1 [12.6–13.4] |
| Menstrual cycle (d) | 28.1 ± 1.3 [27.7–28.6] | 28.4 ± 1.6 [27.8–29.0] |
| Intervention (d of menstrual cycle) | 4.6 ± 1.8 [4.0–5.2] | 4.7 ± 1.8 [4.0–5.4] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Souglis, A.; Bourdas, D.I.; Gioldasis, A.; Ispirlidis, I.; Philippou, A.; Zacharakis, E.; Apostolidis, A.; Efthymiou, G.; Travlos, A.K. Time Course of Performance Indexes, Oxidative Stress, Inflammation, and Muscle Damage Markers after a Female Futsal Match. Sports 2023, 11, 127. https://doi.org/10.3390/sports11070127
Souglis A, Bourdas DI, Gioldasis A, Ispirlidis I, Philippou A, Zacharakis E, Apostolidis A, Efthymiou G, Travlos AK. Time Course of Performance Indexes, Oxidative Stress, Inflammation, and Muscle Damage Markers after a Female Futsal Match. Sports. 2023; 11(7):127. https://doi.org/10.3390/sports11070127
Chicago/Turabian StyleSouglis, Athanasios, Dimitrios I. Bourdas, Aristotelis Gioldasis, Ioannis Ispirlidis, Anastassios Philippou, Emmanouil Zacharakis, Alexandros Apostolidis, Georgios Efthymiou, and Antonios K. Travlos. 2023. "Time Course of Performance Indexes, Oxidative Stress, Inflammation, and Muscle Damage Markers after a Female Futsal Match" Sports 11, no. 7: 127. https://doi.org/10.3390/sports11070127