
Resting Blood Pressure in Master Athletes: Immune from Hypertension?

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Approval and Survey
2.2. Biometrics Classifications
2.3. National Comparative Data
2.4. Statistical Analyses
3. Results
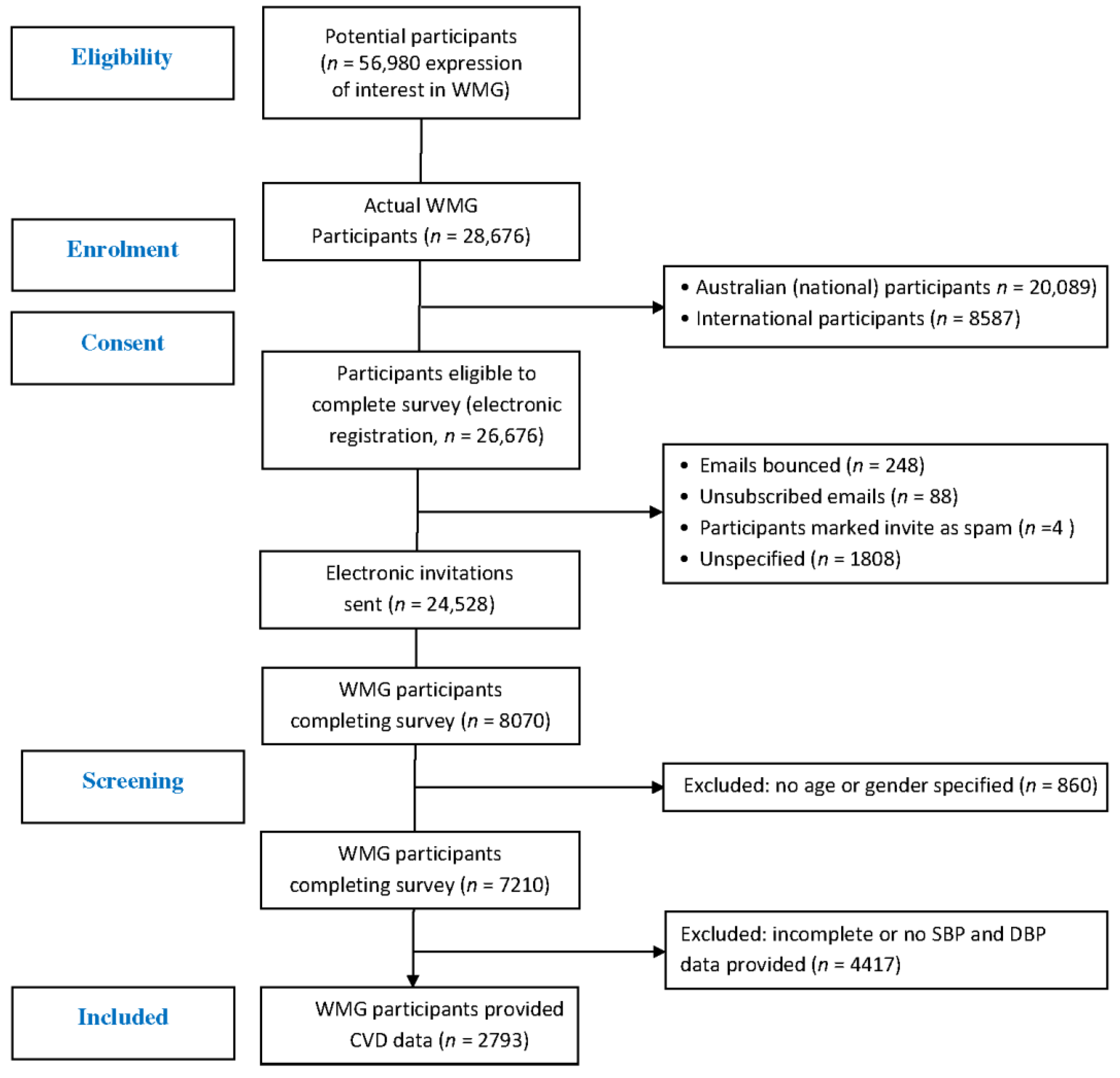
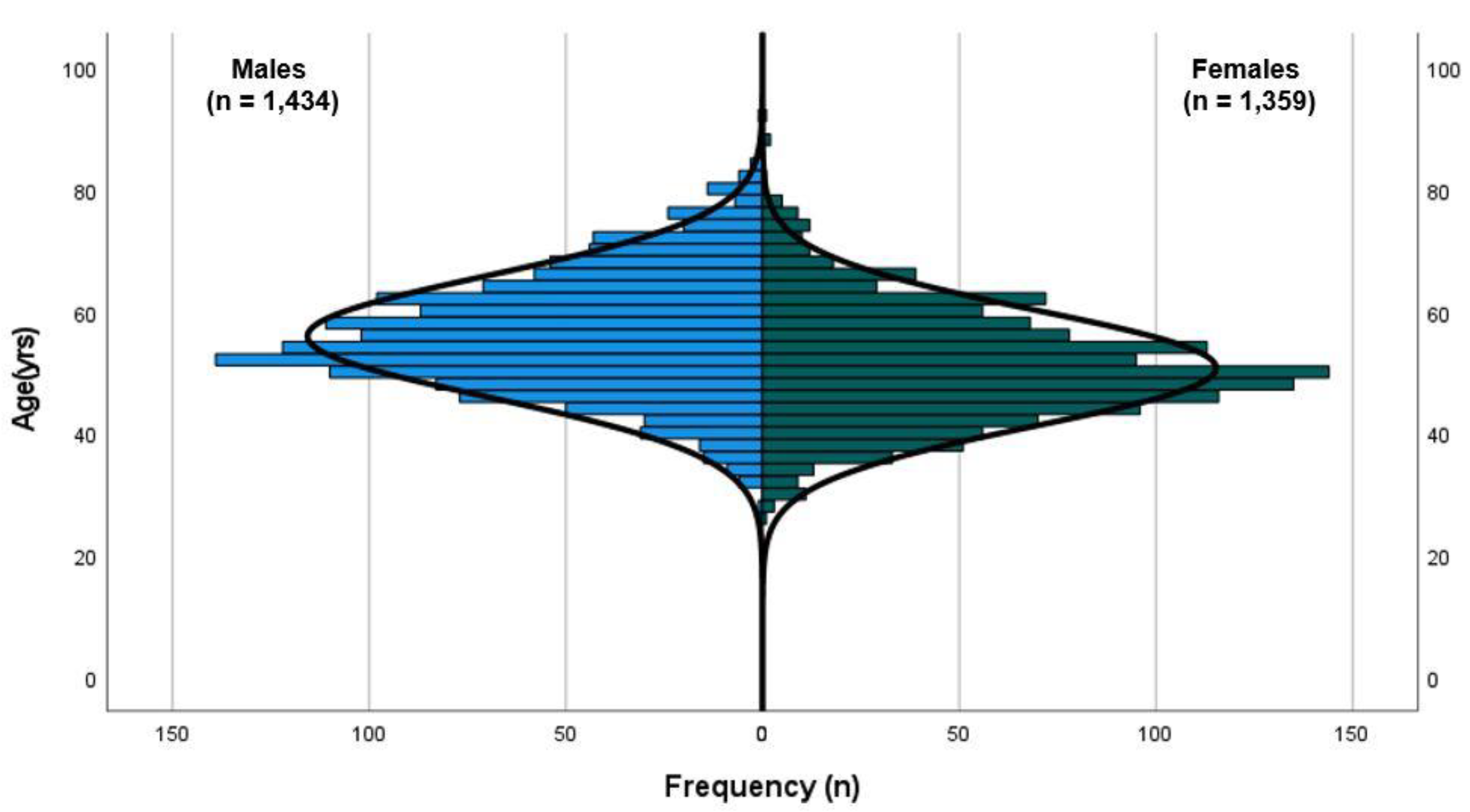
3.1. Study Participants
3.2. Indicators of Obesity
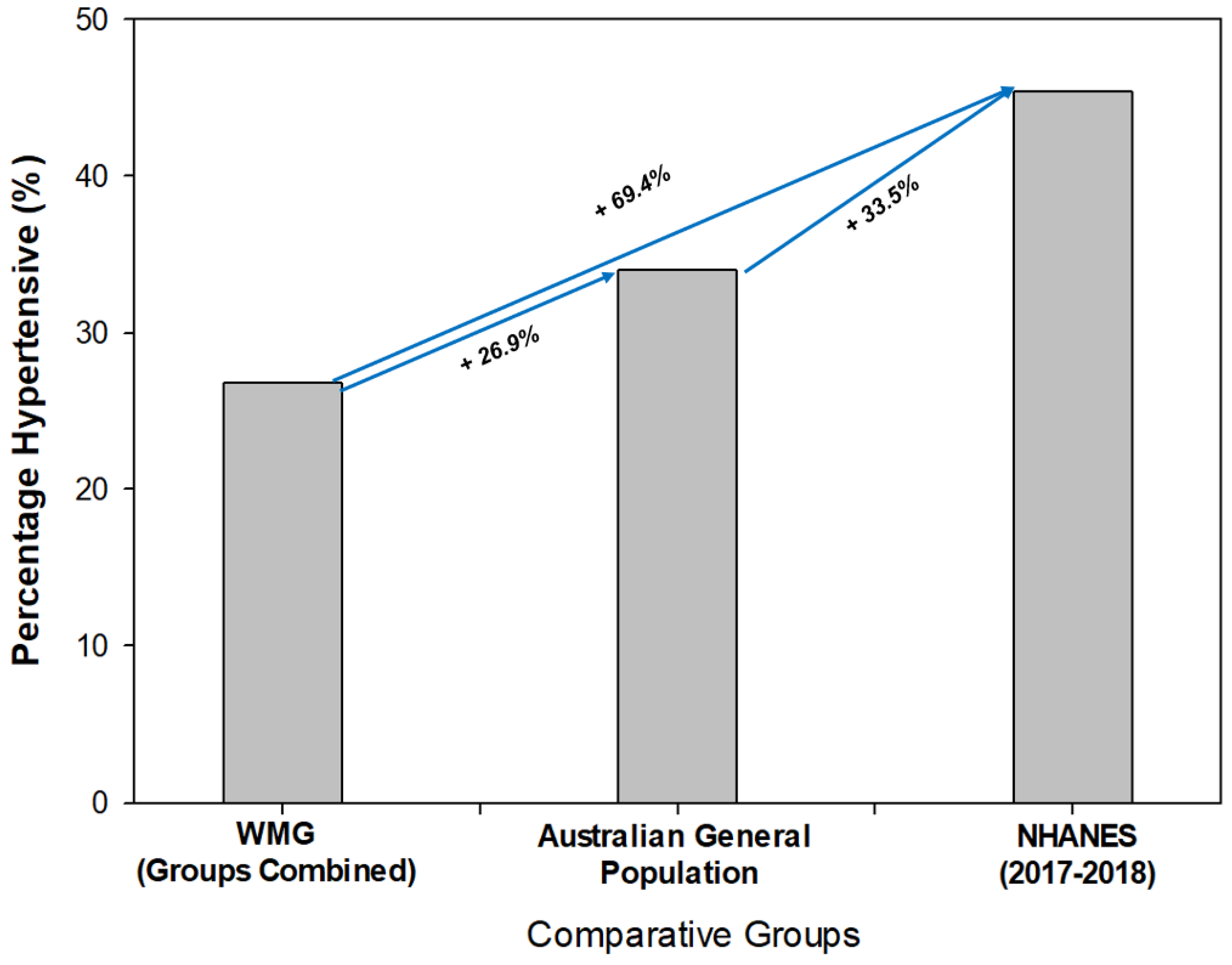
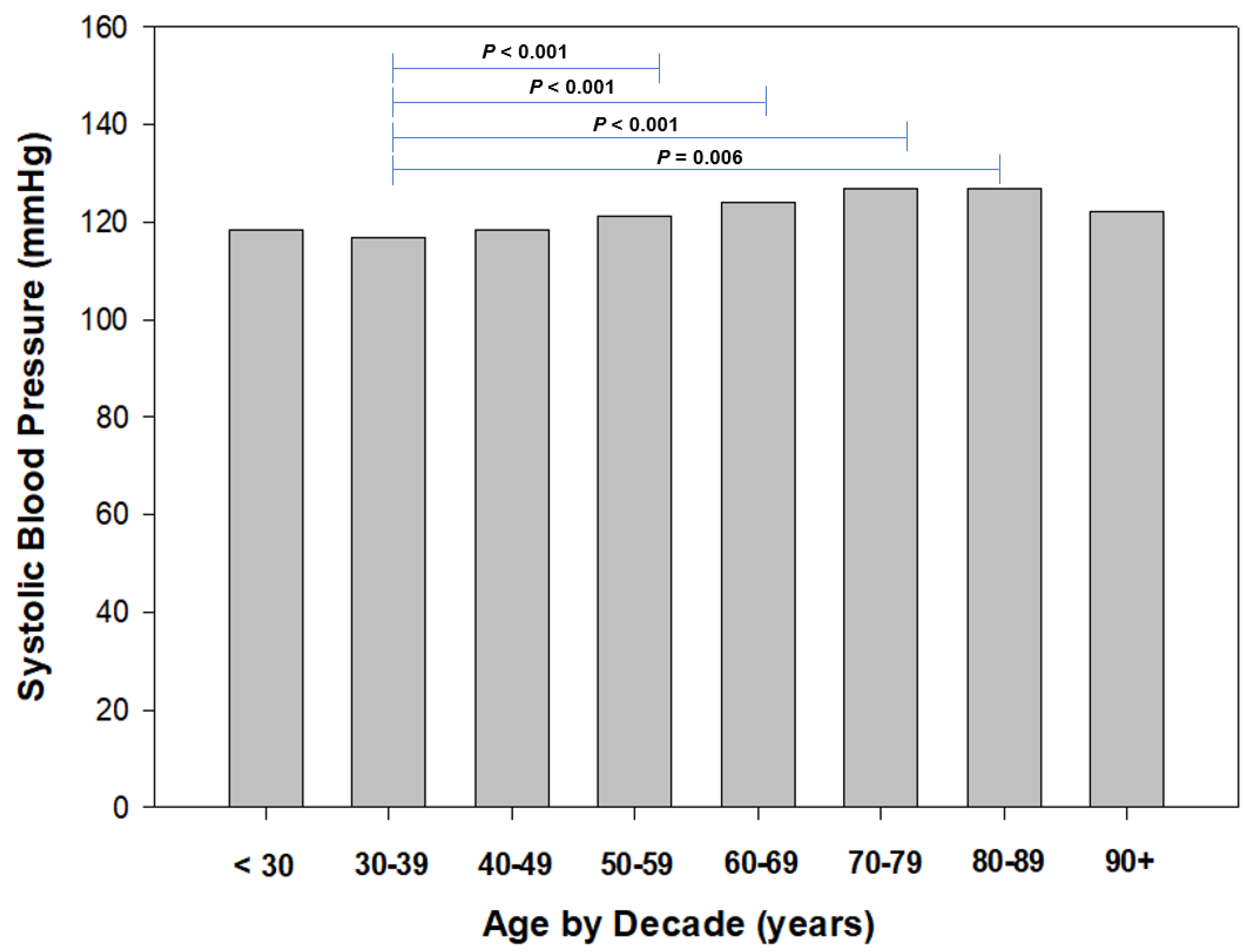
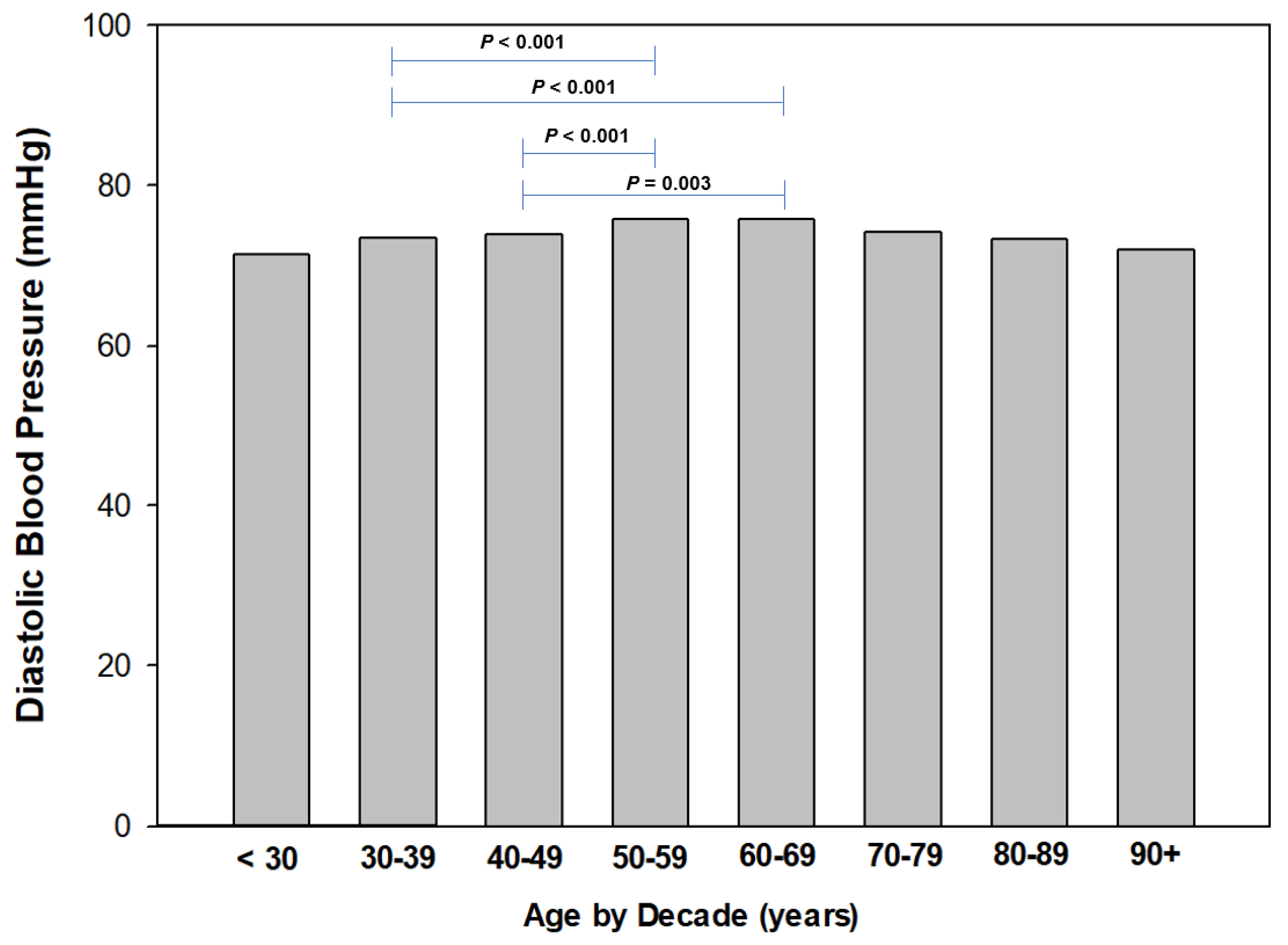
3.3. Resting Systolic and Diastolic Blood Pressure
4. Discussion
4.1. Strengths of the Study
4.2. Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rapsomaniki, E.; Timmis, A.; George, J.; Pujades-Rodriguez, M.; Shah, A.D.; Denaxas, S.; White, I.R.; Caulfield, M.J.; Deanfield, J.E.; Smeeth, L.; et al. Blood pressure and incidence of twelve cardiovascular diseases: Lifetime risks, healthy life-years lost, and age-specific associations in 1·25 million people. Lancet 2014, 383, 1899–1911. [Google Scholar] [CrossRef]
- World Health Organization. Cardiovascular Diseases (CVDs). Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 18 February 2023).
- Australian Government Department of Health and Aged Care. What We’re Doing about Cardiovascular Conditions. Available online: https://www.health.gov.au/topics/chronic-conditions/what-were-doing-about-chronic-conditions/what-were-doing-about-cardiovascular-conditions (accessed on 18 February 2023).
- Centers for Disease Control and Prevention. Heart Disease and Stroke: Risk Factors and CDC’s Response. Available online: https://www.cdc.gov/chronicdisease/resources/publications/factsheets/heart-disease-stroke.htm (accessed on 18 February 2023).
- American College of Cardiology. New ACC/AHA High Blood Pressure Guidelines Lower Definition of Hypertension. Available online: https://www.acc.org/latest-in-cardiology/articles/2017/11/08/11/47/mon-5pm-bp-guideline-aha-2017 (accessed on 7 February 2023).
- Fuchs, F.D.; Whelton, P.K. High Blood Pressure and Cardiovascular Disease. Hypertension 2020, 75, 285–292. [Google Scholar] [CrossRef]
- Wu, C.Y.; Hu, H.Y.; Chou, Y.J.; Huang, N.; Chou, Y.C.; Li, C.P. High Blood Pressure and All-Cause and Cardiovascular Disease Mortalities in Community-Dwelling Older Adults. Medicine 2015, 94, e2160. [Google Scholar] [CrossRef]
- Kahan, T. Focus on blood pressure as a major risk factor. Lancet 2014, 383, 1866–1868. [Google Scholar] [CrossRef]
- World Health Organization. Hypertension. Available online: https://www.who.int/news-room/fact-sheets/detail/hypertension (accessed on 18 February 2023).
- GBD 2017 Risk Factor Collaborators. Global, Regional, and National Comparative Risk Assessment of 84 Behavioural, Environmental and Occupational, and Metabolic Risks or Clusters of Risks for 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar] [CrossRef]
- Grillo, A.; Salvi, L.; Coruzzi, P.; Salvi, P.; Parati, G. Sodium Intake and Hypertension. Nutrients 2019, 11, 1970. [Google Scholar] [CrossRef]
- Flippini, T.; Malavolti, M.; Vinceti, M. Blood Pressure Effects of Sodium Reduction. Circulation 2021, 143, 1542–1567. [Google Scholar] [CrossRef]
- Tsai, S.Y.; Huang, W.H.; Chan, H.L.; Hwang, L.C. The role of smoking cessation programs in lowering blood pressure: A retrospective cohort study. Tob. Induc. Dis. 2021, 19, 82. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Ghadieh, A.S.; Saab, B. Evidence for exercise training in the management of hypertension in adults. Can. Fam. Phys. 2015, 61, 233–239. [Google Scholar]
- Dimeo, F.; Pagonas, N.; Seibert, F.; Arndt, R.; Zidek, W.; Westhoff, T.H. Aerobic exercise reduces blood pressure in resistant hypertension. Hypertension 2012, 60, 653–658. [Google Scholar] [CrossRef]
- de Barcelos, G.T.; Heberle, I.; Coneglian, J.C.; Vieira, B.A.; Delevatti, R.S.; Gerage, A.M. Effects of Aerobic Training Progression on Blood Pressure in Individuals With Hypertension: A Systematic Review With Meta-Analysis and Meta-Regression. Front. Sport. Act. Living 2022, 4, 719063. [Google Scholar] [CrossRef] [PubMed]
- Lemes, Í.R.; Ferreira, P.H.; Linares, S.N.; Machado, A.F.; Pastre, C.M.; Netto, J.J. Resistance training reduces systolic blood pressure in metabolic syndrome: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sport. Med. 2016, 50, 1438–1442. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.; Heazlewood, I.T.; Climstein, M. Body Mass Index in Master Athletes: Review of the Literature. J. Lifestyle Med. 2018, 8, 79–98. [Google Scholar] [CrossRef] [PubMed]
- Federation Internationle De Natation. FINA Master Rules 2017–2021. Available online: https://resources.fina.org/fina/document/2021/02/19/9998a198-f2ac-47c6-a36f-72e3aad37ca8/2017_2021_masters_11102017_new.pdf (accessed on 19 February 2023).
- United States Athletic Track and Field. Welcome to the USATF Masters Track & Field. Available online: https://usatfmasters.org/about/ (accessed on 19 February 2023).
- Harnett, J.; Climstein, M.; Walsh, J.; Gifford, J. The Use of Medications and Dietary Supplements by Masters Athletes—A Review. Curr. Nutr. Rep. 2022, 11, 253–262. [Google Scholar] [CrossRef]
- Climstein, M.; Walsh, J.; Heazlewood, T.; Meir, R. Chapter 5: An Overview of Risk Factors for Disease in Masters Athletes; Taylor & Francis Group: Abingdon, UK, 2021; p. 216. [Google Scholar]
- Climstein, M.; Walsh, J.; Heazlewood, I.; DeBeliso, M. Endurance masters athletes: A model of successful ageing with clinically superior BMI? Sport J. 2019, 21, 1–11. [Google Scholar]
- Debeliso, M.; Sevene, T.; Walsh, J.; Adams, K.; Kettunen, J.; Heazlewood, I.; M, C. Body Mass Index of North American Participants at the World Masters Games. J. Sport. Sci. 2014, 2, 189–194. [Google Scholar]
- Walsh, J.; Climstein, M.; Heazlewood, I.T.; Burke, S.; Kettunen, J.; Adams, K.; DeBeliso, M. Body mass index for Australian athletes participating in rugby union, soccer and touch football at the World Masters Games. World Acad. Sci. Eng. Technol. 2011, 7, 1119–1122. [Google Scholar]
- Walsh, J.; Climstein, M.; Heazlewood, I.T.; DeBeliso, M.; Adams, K.; Burke, S.; Kettunen, J. Body mass index of masters basketball players. Med. Sport. J. Rom. Sport. Med. Soc. 2011, 7, 1700–1705. [Google Scholar]
- Walsh, J.; Climstein, M.; Burke, S.; Kettunen, J.; Heazlewood, I.T.; DeBeliso, M.; Adams, K. Obesity prevalence for athletes participating in soccer at the World Masters Games. Int. Sport. J. 2012, 13, 76–84. [Google Scholar]
- Walsh, J.; Climstein, M.; Heazlewood, I.T.; Kettunen, J.; Burke, S.; Debeliso, M.; Adams, K. Body mass index for athletes participating in swimming at the World Masters Games. J. Sport. Med. Phys. Fit. 2013, 53, 162–168. [Google Scholar]
- Walsh, J.; Heazelwood, I.; DeBeliso, M.; Climstein. Comparison of Obesity Prevalence Across 28 World Masters Games Sports. Sport Sci. Int. Sci. J. Kinesiol. 2018, 21, 30–36. [Google Scholar]
- Climstein, M.; Walsh, J.; Debeliso, M.; Heazlewood, T.; Sevene, T.; Adams, K. Cardiovascular risk profiles of world masters games participants. J. Sport. Med. Phys. Fit. 2018, 58, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Climstein, M.; Walsh, J.; Adams, K.; Sevene, T.; Heazlewood, T.; DeBeliso, M. Prevalence of hyperglycemia in masters athletes. PeerJ 2022, 10, e13389. [Google Scholar] [CrossRef]
- Hernelahti, M.; Kujala, U.M.; Kaprio, J.; Karjalainen, J.; Sarna, S. Hypertension in master endurance athletes. J. Hypertens. 1998, 16, 1573–1577. [Google Scholar] [CrossRef]
- Parry-Williams, G.; Obaid, D.; Moser, J.; Vlahos, I.; Bulleros, P.; Fanton, Z.; Basu, J.; Miles, C.; MacLachlan, H.; Moreira-Accame, M.; et al. Low grade hypertension an ccoronary atherosclerosis in male master enduance athletes. Heart 2021, 107, A142. [Google Scholar]
- Hawkins, S.A.; Wiswell, R.A.; Marcell, T.J. Exercise and the master athlete--a model of successful aging? J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, 1009–1011. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Booker, Q.S.; Austin, J.D.; Balasubramanian, B.A. Survey strategies to increase participant response rates in primary care research studies. Fam. Pract. 2021, 38, 699–702. [Google Scholar] [CrossRef]
- Royal Australian College of General Practitioners. Red Book: Introduction. Available online: https://www.racgp.org.au/clinical-resources/clinical-guidelines/key-racgp-guidelines/view-all-racgp-guidelines/guidelines-for-preventive-activities-in-general-pr/preamble/introduction (accessed on 12 February 2023).
- Perone, F.; Pingitore, A.; Conte, E.; Halasz, G.; Ambrosetti, M.; Peruzzi, M.; Cavarretta, E. Obesity and Cardiovascular Risk: Systematic Intervention Is the Key for Prevention. Healthcare 2023, 11, 902. [Google Scholar] [CrossRef] [PubMed]
- Flack, J.M.; Adekola, B. Blood pressure and the new ACC/AHA hypertension guidelines. Trends Cardiovasc. Med. 2020, 30, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Ostchega, Y.; Hughes, J.P.; Kit, B.; Chen, T.C.; Nwankwo, T.; Commodore-Mensah, Y.; Graber, J.E.; Nguyen, D.T. Differences in Hypertension and Stage II Hypertension by Demographic and Risk Factors, Obtained by Two Different Protocols in US Adults: National Health and Nutrition Examination Survey, 2017–2018. Am. J. Hypertens. 2022, 35, 619–626. [Google Scholar] [CrossRef]
- The British Academy: Centre for Multilevel Modelling. SPSS: Checking for Normality Practice. Available online: https://www.bristol.ac.uk/cmm/media/research/ba-teaching-ebooks/pdf/Normality%20-%20Practical.pdf (accessed on 7 February 2023).
- Australian Institute of Health and Welfare. High Blood Pressure. Available online: https://www.aihw.gov.au/reports/risk-factors/high-blood-pressure/data (accessed on 7 February 2023).
- National Health and Nutrition Examination Survey National. National Center for Health Statistics: National Health and Nutrition Examination Survey Fact Sheet. Available online: https://www.cdc.gov/nchs/data/factsheets/factsheet_nhanes.pdf (accessed on 12 February 2023).
- Climstein, M.; Walsh, J.; Best, J.; Heazlewood, I.T.; Burke, S.; Kettunen, J.; Adams, K.; DeBeliso, M. Physiological and pathology demographics of veteran rugby athletes: Golden Oldies Rugby Festival. World Acad. Sci. Eng. Technol. 2011, 77, 1123–1128. [Google Scholar]
- Schweiger, V.; Niederseer, D.; Schmied, C.; Attenhofer-Jost, C.; Caselli, S. Athletes and Hypertension. Curr. Cardiol. Rep. 2021, 23, 176. [Google Scholar] [CrossRef]
- Guzman, H.; Rouseff, M.; Tran, T.T.; Nasir, K.; Bou-Khalil, J.; Mora, J.; Das, J.; Brown, D.; Santiago, J.; Ochoa, T. Clinically Significant Blood Pressure Reduction among Participants of a Lifestyle Intervention Improvement Program Strongly Associated with Reduced Systemic Inflammation in a High Risk Working Population. Available online: https://www.ahajournals.org/doi/10.1161/circ.129.suppl_1.p391 (accessed on 17 February 2023).
- Blood Pressure Lowering Treatment Trialists’ Collaboration. Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: An individual participant-level data meta-analysis. Lancet 2021, 397, 1625–1636. [Google Scholar] [CrossRef]
- Chan, L.S. Minimal clinically important difference (MCID)—Adding meaning to statistical inference. Am. J. Public Health 2013, 103, e24–e25. [Google Scholar] [CrossRef]
- Berge, H.M.; Isern, C.B.; Berge, E. Blood pressure and hypertension in athletes: A systematic review. Br. J. Sport. Med. 2015, 49, 716–723. [Google Scholar] [CrossRef]
- Naci, H.; Salcher-Konrad, M.; Dias, S.; Blum, M.R.; Sahoo, S.A.; Nunan, D.; Ioannidis, J.P.A. How does exercise treatment compare with antihypertensive medications? A network meta-analysis of 391 randomised controlled trials assessing exercise and medication effects on systolic blood pressure. Br. J. Sport. Med. 2019, 53, 859–869. [Google Scholar] [CrossRef]
- Castillo-Garcia, A.; Naci, H.; Valenzuela, P.L.; Salcher-Konrad, M.; Dias, S.; Blum, M.R.; Sahoo, S.A.; Nunan, D.; Morales, J.S.; Lucia, A.; et al. Infographic. How does exercise treatment compare with antihypertensive medications? Br. J. Sport. Med. 2020, 54, 746–747. [Google Scholar] [CrossRef]
- Slomski, A. Polypill for Initial Hypertension Treatment Is Promising. JAMA 2021, 326, 1572. [Google Scholar] [CrossRef] [PubMed]
- Paczkowska-Walendowska, M.; Sip, S.; Staszewski, R.; Cielecka-Piontek, J. Single-Pill Combination to Improve Hypertension Treatment: Pharmaceutical Industry Development. Int. J. Environ. Res. Public Health 2022, 19, 4156. [Google Scholar] [CrossRef] [PubMed]
- Perrone, V.; Veronesi, C.; Gambera, M.; Nati, G.; Perone, F.; Tagliabue, P.F.; Degli Esposti, L.; Volpe, M. Treatment with Free Triple Combination Therapy of Atorvastatin, Perindopril, Amlodipine in Hypertensive Patients: A Real-World Population Study in Italy. High Blood Press. Cardiovasc. Prev. 2019, 26, 399–404. [Google Scholar] [CrossRef]
- Gaciong, Z. Preference and Adherence to a Fixed-Dose Combination of Bisoprolol-Aspirin and Blood Pressure Control: Results of an Open-Label, Multicentre Study. J. Clin. Med. 2022, 12, 17. [Google Scholar] [CrossRef]
- Laine, M.K.; Kujala, U.M.; Eriksson, J.G.; Wasenius, N.S.; Kaprio, J.; Bäckmand, H.M.; Peltonen, M.; Heinonen, O.; Jula, A.; Sarna, S. Former male elite athletes and risk of hypertension in later life. J. Hypertens. 2015, 33, 1549–1554. [Google Scholar] [CrossRef]
- Nessler, K.; Krztoń-Królewiecka, A.; Suska, A.; Mann, M.R.; Nessler, M.B.; Windak, A. The reliability of patient blood pressure self-assessments—A cross-sectional study. BMC Prim. Care 2023, 24, 2. [Google Scholar] [CrossRef]
- Gabb, G.M.; Mangoni, A.A.; Arnolda, L. Guideline for the diagnosis and management of hypertension in adults—2016. Med. J. Aust. 2017, 206, 141. [Google Scholar] [CrossRef]
- Liu, C.; Zheng, H.; Griffiths, C.; Murray, A. Comparison of Repeatability of Blood Pressure Measurements between Oscillometric and Auscultatory Methods. Comput. Cardiol. 2015, 42, 1073–1076. [Google Scholar] [CrossRef]
- O’Sullivan, I.; Orbell, S.; Rakow, T.; Parker, R. Prospective research in health service settings: Health psychology, science and the ‘Hawthorne’ effect. J. Health Psychol. 2004, 9, 355–359. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Males | Females | |
|---|---|---|---|
| (n = 2793) | (n = 1434) | (n = 1359) | |
| •Age (yr) | 53.3 ± 9.9 | 55.8 ± 9.8 | 50.6 ± 9.4 * < 0.001 |
| (52.9–53.7) | (55.3–56.3) | (50.1–51.1) | |
| •Smoking status | |||
| -Non-smoker (%) | 77.3 | 78.5 | 75.9 |
| -Ex-smoker (%) | 19.9 | 20 | 19.9 |
| -Smoker (%) | 2.8 | 1.5 | 4.2 |
| •Drinking status | |||
| -Non-drinker (%) | 16.4 | 16 | 16.7 |
| -Ex-drinker (%) | 0.8 | 1.3 | 0.6 |
| -Drinker (%) | 82.7 | 82.7 | 82.7 |
| -Drinks/wk (n) | 6.8 ± 6.4 | 8.0 ± 7.2 | 5.3 ± 5.1 |
| •Mass (kg) | 76.7 ± 14.9 | 83.8 ± 12.9 | 69.2 ± 13.0 * < 0.001 |
| (76.2–77.3) | (83.1–84.5) | (68.5–69.9) | |
| •BMI (kg/m2) | 25.7 ± 4.2 | 26.2 ± 3.6 | 25.1 ± 4.6 |
| (25.5–25.4) | (26.0–26.4) | (24.8–25.3) | |
| •BMI Classification | |||
| -Underweight (%) | 0.08 | 0.1 | 1.5 |
| -Normal (%) | 49.8 | 41.9 | 56.8 |
| -Overweight (%) | 36.8 | 44.6 | 27.6 |
| -Obese (%) | 12.5 | 12.6 | 12.1 |
| •Waist circumference | 85.4 ± 11.9 | 89.8 ± 10.4 | 80.0 ± 11.5 * < 0.001 |
| classification | (84.9–85.9) | (89.2–90.4) | (79.3–80.7) |
| -Normal (%) | 61.7 | 68.9 | 52.7 |
| -Increased risk (%) | 22.4 | 20 | 25.3 |
| -High risk (%) | 15.9 | 11.1 | 22 |
| •Resting SBP (mmHg) | 120.9 ± 12.6 | 124.6 ± 11.5 | 117.0 ± 12.5 * < 0.001 |
| (120.4–121.4) | (124.0–125.2) | (116.4–117.7) | |
| •SBP Classification | |||
| -Normal (%) | 34.3 | 19.9 | 49.7 |
| -Elevated (%) | 39.0 | 43.8 | 34.1 |
| -HTN stage 1 (%) | 17.6 | 24.3 | 10.6 |
| -HTN stage 2 (%) | 8.8 | 11.9 | 5.5 |
| •HTN crisis (%) | 0.4 | 0.04 | 0.02 |
| •Resting DBP (mmHg) | 74.9 ± 9.2 | 77.1 ± 8.4 | 72.7 ± 9.5 * < 0.001 |
| Classification | (74.6–75.3) | (76.6–77.5) | (72.2–73.2) |
| -Normal (%) | 55.9 | 46.2 | 66.1 |
| -HTN stage 1 (%) | 37.5 | 45.7 | 29 |
| -HTN stage 2 (%) | 6.5 | 8 | 4.8 |
| -HTN crisis (%) | <0.001 | <0.001 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Climstein, M.; Walsh, J.; DeBeliso, M.; Heazlewood, T.; Sevene, T.; Del Vecchio, L.; Adams, K. Resting Blood Pressure in Master Athletes: Immune from Hypertension? Sports 2023, 11, 85. https://doi.org/10.3390/sports11040085
Climstein M, Walsh J, DeBeliso M, Heazlewood T, Sevene T, Del Vecchio L, Adams K. Resting Blood Pressure in Master Athletes: Immune from Hypertension? Sports. 2023; 11(4):85. https://doi.org/10.3390/sports11040085
Chicago/Turabian StyleClimstein, Mike, Joe Walsh, Mark DeBeliso, Tim Heazlewood, Trish Sevene, Luke Del Vecchio, and Kent Adams. 2023. "Resting Blood Pressure in Master Athletes: Immune from Hypertension?" Sports 11, no. 4: 85. https://doi.org/10.3390/sports11040085