Balance and Fall Risk Assessment in Community-Dwelling Older Adults after Recovery from COVID-19: A Cross-Sectional Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
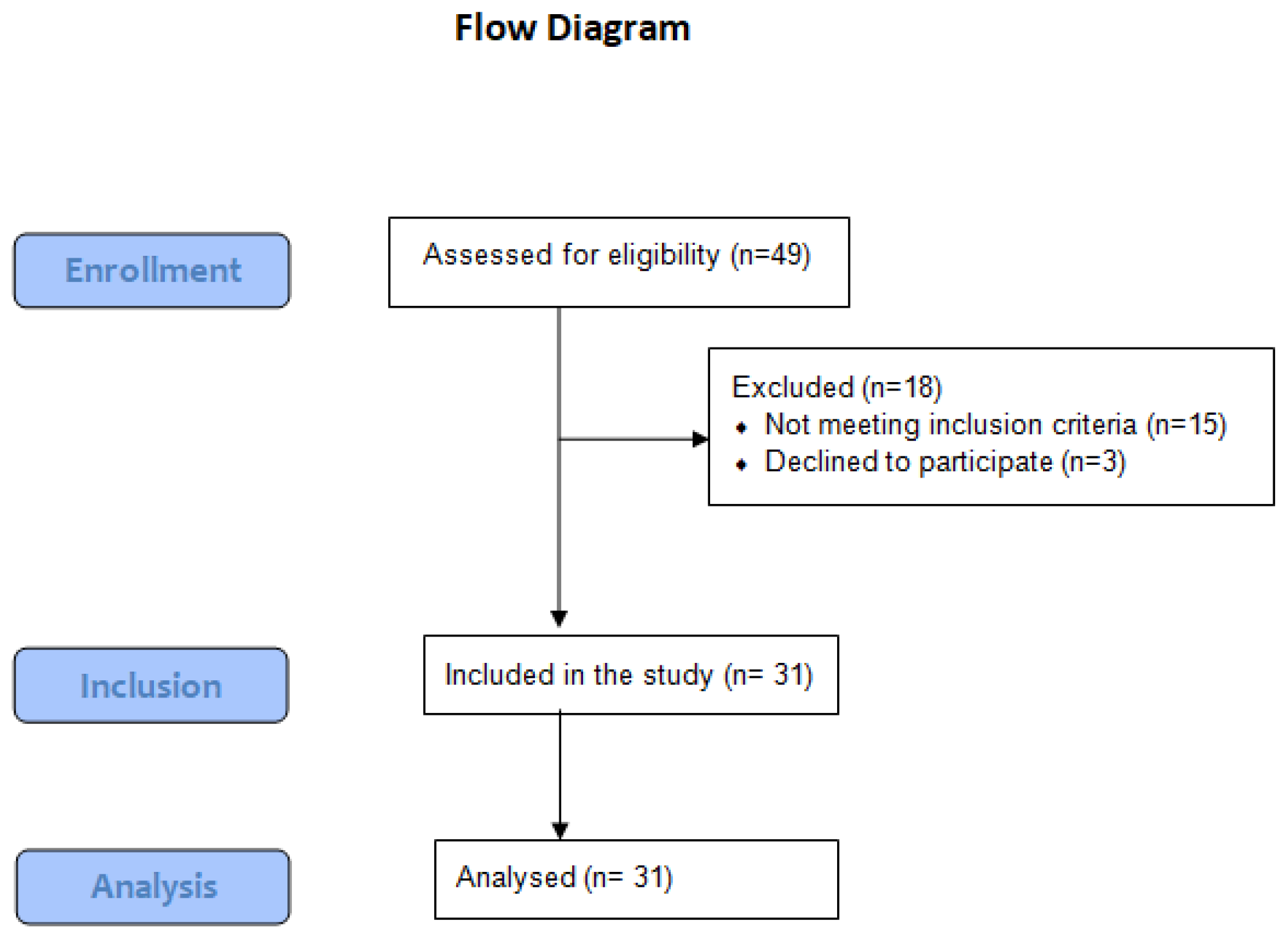
2.2. Participants
2.3. Procedures
2.3.1. Evaluation Procedures
2.3.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yamada, M.; Kimura, Y.; Ishiyama, D.; Otobe, Y.; Suzuki, M.; Koyama, S.; Kikuchi, T.; Kusumi, H.; Arai, H. Effect of the COVID-19 Epidemic on Physical Activity in Community-Dwelling Older Adults in Japan: A Cross-Sectional Online Survey. J. Nutr. Health Aging 2020, 24, 948–950. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-Month Consequences of COVID-19 in Patients Discharged from Hospital: A Cohort Study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Cevik, M.; Kuppalli, K.; Kindrachuk, J.; Peiris, M. Virology, Transmission, and Pathogenesis of SARS-CoV-2. BMJ 2020, 371, m3862. [Google Scholar] [CrossRef] [PubMed]
- Neerland, B.E.; Dobloug, A.; Nore, K.G.; Mikaelsen, E.E.; Halsen, A.; Ahmed, M. V COVID-19 in an Elderly Woman with Acute Functional Decline. Tidsskr. Nor. Laegeforening 2020, 140, 5. [Google Scholar] [CrossRef]
- Olde Rikkert, M.G.M.; Vingerhoets, R.W.; van Geldorp, N.; de Jong, E.; Maas, H.A.A.M. Atypical Clinical Picture of COVID-19 in Older Patients. Ned. Tijdschr. Geneeskd. 2020, 164, D5004. [Google Scholar]
- Norman, R.E.; Stall, N.M.; Sinha, S.K. Typically Atypical: COVID-19 Presenting as a Fall in an Older Adult. J. Am. Geriatr. Soc. 2020, 68, E36–E37. [Google Scholar] [CrossRef]
- Fiani, B.; Covarrubias, C.; Desai, A.; Sekhon, M.; Jarrah, R. A Contemporary Review of Neurological Sequelae of COVID-19. Front. Neurol. 2020, 11, 640. [Google Scholar] [CrossRef]
- Ashrafi, M.R.; Azizimalamiri, R.; Badv, R.S.; Tavasoli, A.R.; Nikkhah, A.; Montazerlotfelahi, H.; Vafaee-Shahi, M.; Heidari, M. Coronavirus, Its Neurologic Manifestations, and Complications. Iran. J. Pediatr. 2020, 30, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Carod-Artal, F.J. Neurological Complications of Coronavirus and COVID-19. Rev. Neurol. 2020, 70, 311–322. [Google Scholar]
- Vacchiano, V.; Riguzzi, P.; Volpi, L.; Tappatà, M.; Avoni, P.; Rizzo, G.; Guerra, L.; Zaccaroni, S.; Cortelli, P.; Michelucci, R.; et al. Early Neurological Manifestations of Hospitalized COVID-19 Patients. Neurol. Sci. 2020, 41, 2029–2031. [Google Scholar] [CrossRef] [PubMed]
- Harapan, B.N.; Yoo, H.J. Neurological Symptoms, Manifestations, and Complications Associated with Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and Coronavirus Disease 19 (COVID-19). J. Neurol. 2021, 268, 3059–3071. [Google Scholar] [CrossRef] [PubMed]
- Urbaniak-olejnik, M.; Loba, W.; Stieler, O.; Komar, D.; Majewska, A.; Marcinkowska-gapi, A. Body Balance Analysis in the Visually Impaired Individuals Aged 18–24 Years. Int. J. Environ. Res. Public Health 2022, 19, 14383. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.S.; Kowal, P.; Hestekin, H.; Driscoll, T.O.; Peltzer, K.; Yawson, A. Prevalence, Risk Factors and Disability Associated with Fall-Related Injury in Older Adults in Low- and Middle-Incomecountries: Results from the WHO Study on Global AGEing and Adult Health ( SAGE ). BMC Med. 2015, 13, 147. [Google Scholar] [CrossRef] [Green Version]
- CDC–National Center for Health Statistics. Available online: https://www.cdc.gov/falls/hip-fractures.html (accessed on 17 April 2022).
- Jeon, Y.J.; Kim, G.M. Comparison of the Berg Balance Scale and Fullerton Advanced Balance Scale to Predict Falls in Community-Dwelling Adults. J. Phys. Ther. Sci. 2017, 29, 232–234. [Google Scholar] [CrossRef] [Green Version]
- Ban, B.; Sevšek, F.; Rugelj, D. A Comparison of the Ceiling Effect between Berg Balance Scale and Mini-BESTest in a Group of Balance Trained Community-Dwelling Older Adults. Physiother. Q. 2017, 25, 3–9. [Google Scholar] [CrossRef]
- Pickerill, M.L.; Harter, R.A. Validity and Reliability of Limits-of-Stability Testing: A Comparison of 2 Postural Stability Evaluation Devices. J. Athl. Train. 2011, 46, 600–606. [Google Scholar] [CrossRef] [Green Version]
- Cho, K.; Lee, K.; Lee, B.; Lee, H.; Lee, W. Relationship between Postural Sway and Dynamic Balance in Stroke Patients. J. Phys. Ther. Sci. 2014, 26, 1989–1992. [Google Scholar] [CrossRef] [Green Version]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients with Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [Green Version]
- Almufarrij, I.; Uus, K.; Munro, K.J. Does Coronavirus Affect the Audio-Vestibular System? A Rapid Systematic Review. Int. J. Audiol. 2020, 59, 487–491. [Google Scholar] [CrossRef]
- Ghahramani, M. Fall Risk Assessment in Older People. Int. J. Eng. Sci. 2016, 5, 1–14. [Google Scholar] [CrossRef]
- Park, S.H. Tools for Assessing Fall Risk in the Elderly: A Systematic Review and Meta-Analysis. Aging Clin. Exp. Res. 2018, 30, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Halaweh, H.; Dahlin-Ivanoff, S.; Svantesson, U.; Willén, C. Perspectives of Older Adults on Aging Well: A Focus Group Study. J. Aging Res. 2018, 2018, 9858252. [Google Scholar] [CrossRef] [Green Version]
- COVID-19 Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/ (accessed on 8 March 2022).
- Markotegi, M.; Irazusta, J.; Sanz, B.; Rodriguez-Larrad, A. Effect of the COVID-19 Pandemic on the Physical and Psychoaffective Health of Older Adults in a Physical Exercise Program. Exp. Gerontol. 2021, 155, 111580. [Google Scholar] [CrossRef] [PubMed]
- Kang, H. Sample Size Determination and Power Analysis Using the G * Power Software. J. Educ. Eval. Health Prof. 2021, 18, 17. [Google Scholar] [CrossRef] [PubMed]
- Prometti, P.; Olivares, A.; Gaia, G.; Bonometti, G.; Comini, L.; Scalvini, S. Biodex Fall Risk Assessment in the Elderly with Ataxia: A New Age-Dependent Derived Index in Rehabilitation: An Observational Study. Medicine 2016, 95, e2977. [Google Scholar] [CrossRef]
- Abdel Ghafar, M.A.; Abdelraouf, O.R.; Abdelgalil, A.A.; Seyam, M.K.; Radwan, R.E.; El-Bagalaty, A.E. Quantitative Assessment of Sensory Integration and Balance in Children with Autism Spectrum Disorders: Cross-Sectional Study. Children 2022, 9, 353. [Google Scholar] [CrossRef]
- Portney, L.G.; Watkins Mary, P. Foundations of Clinical Research: Applications to Practice, 3rd ed.; Pearson/Prentice Hall: Hoboken, NJ, USA, 2009; ISBN 9780131716407. [Google Scholar]
- Viola, P.; Ralli, M.; Pisani, D.; Malanga, D.; Sculco, D.; Messina, L.; Laria, C.; Aragona, T.; Leopardi, G.; Ursini, F.; et al. Tinnitus and Equilibrium Disorders in COVID-19 Patients: Preliminary Results. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 3725–3730. [Google Scholar] [CrossRef]
- Yılmaz, O.; Mutlu, B.Ö.; Yaman, H.; Bayazıt, D.; Demirhan, H.; Bayazıt, Y.A. Assessment of Balance after Recovery from COVID-19 Disease. Auris Nasus Larynx 2022, 49, 291–298. [Google Scholar] [CrossRef]
- Iwasaki, S.; Yamasoba, T. Dizziness and Imbalance in the Elderly: Age-Related Decline in the Vestibular System. Aging Dis. 2015, 6, 38–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mustafa, M.; Taya, U. Vestibular Evoked Myogenic Potentials of Asymptomatic COVID-19 PCR-Positive Cases. Glob. J. Otolaryngol. 2020, 22, 00135–00138. [Google Scholar] [CrossRef]
- Ralli, M.; Campo, F.; Angeletti, D.; Minni, A.; Artico, M.; Greco, A.; Polimeni, A.; de Vincentiis, M. Pathophysiology and Therapy of Systemic Vasculitides. EXCLI J. 2020, 19, 817–854. [Google Scholar]
- Motaqi, M.; Hatef, B.; Ashtiani, A.A.; Ghanjal, A. Musculoskeletal Problems in Patients with COVID-19: A Review Study. Asian J. Sports Med. 2021, 12, e111040. [Google Scholar] [CrossRef]
- Margitić, S.E.; Inouye, S.K.; Thomas, J.L.; Cassel, C.K.; Regenstreif, D.I.; Kowal, J. Hospital Outcomes Project for the Elderly (HOPE): Rationale and Design for a Prospective Pooled Analysis. J. Am. Geriatr. Soc. 1993, 41, 258–267. [Google Scholar] [CrossRef] [PubMed]
- Lakhan, P.; Jones, M.; Wilson, A.; Courtney, M.; Hirdes, J.; Leonard, C. A Prospective Cohort Study of Geriatric Syndromes among Older Medical Patients Admitted to Acute Care Hospitals. J. Am. Geriatr. Soc. 2011, 59, 2001–2008. [Google Scholar] [CrossRef] [PubMed]
- WHO Guidlines on Physical Activity and Sedentary Behavior. Available online: https://apps.who.int/iris/bitstream/handle/10665/337001/9789240014886-eng.pdf (accessed on 28 November 2022).
- World Health Organization #HealthyAtHome—Physical Activity. WHO. Healthy At Home—Physical Activity. Available online: https://www.who.int/news-room/campaigns/connecting-the-world-to-combat-coronavirus/healthyathome/healthyathome---physical-activity (accessed on 15 October 2022).
- Narici, M.; De Vito, G.; Franchi, M.; Paoli, A.; Moro, T.; Marcolin, G.; Grassi, B.; Baldassarre, G.; Zuccarelli, L.; Biolo, G.; et al. Impact of Sedentarism Due to the COVID-19 Home Confinement on Neuromuscular, Cardiovascular and Metabolic Health: Physiological and Pathophysiological Implications and Recommendations for Physical and Nutritional Countermeasures. Eur. J. Sport Sci. 2021, 21, 614–635. [Google Scholar] [CrossRef]
- Parsa, M.; Rahimi, A.; Noorizadeh Dehkordi, S. Studying the Correlation between Balance Assessment by Biodex Stability System and Berg Scale in Stroke Individuals. J. Bodyw. Mov. Ther. 2019, 23, 850–854. [Google Scholar] [CrossRef]
- Murphy, M.A.; Roberts-Warrior, D. A Review of Motor Performance Measures and Treatment Interventions for Patients with Stroke. Top. Geriatr. Rehabil. 2003, 19, 3–42. [Google Scholar] [CrossRef]
- Elwishy, A. Effect of Sensorimotor Integration Balance Program in Patients with Multiple Sclerosis: A Single Blinded Randomized Controlled Study. Med. J. Cairo. Univ. 2012, 80, 85–93. [Google Scholar]
- Lajoie, Y.; Girard, A.; Guay, M. Comparison of the Reaction Time, the Berg Scale and the ABC in Non-Fallers and Fallers. Arch. Gerontol. Geriatr. 2002, 35, 215–225. [Google Scholar] [CrossRef] [PubMed]
- Tyson, S.; DeSouza, L. A Systematic Review of Methods to Measure Balance and Walking Post-Stroke. Part 1: Ordinal Scales. Phys. Ther. Rev. 2002, 7, 173–186. [Google Scholar] [CrossRef]
- Lajoie, Y.; Gallagher, S.P. Predicting Falls within the Elderly Community: Comparison of Postural Sway, Reaction Time, the Berg Balance Scale and the Activities-Specific Balance Confidence (ABC) Scale for Comparing Fallers and Non-Fallers. Arch. Gerontol. Geriatr. 2004, 38, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Leroux, A.; Pinet, H.; Nadeau, S. Task-Oriented Intervention in Chronic Stroke: Changes in Clinical and Laboratory Measures of Balance and Mobility. Am. J. Phys. Med. Rehabil. 2006, 85, 820–830. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Groups | SARS-CoV-2 Group n = 31 | Control Group n = 33 | p-Value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Age (years) | 69.79 ± 3.21 | 70.89 ± 4.63 | 0.542 a |
| Height (m) | 1.62 ± 0.12 | 1.65 ± 0.17 | 0.680 a |
| Weight (kg) | 75.39 ± 9.38 | 77.54 ± 10.27 | 0.286 a |
| BMI | 28.67 ± 2.67 | 30.13± 5.54 | 0.135 a |
| Gender distribution (Male/Female) | (22/9) | (23/10) | 0.796 b |
| Health conditions | |||
| Hypertension | 25/31 | 22/33 | 0.045 * b |
| Cardiopathies | 24/31 | 20/33 | 0.041 * b |
| Diabetes | 17/31 | 19/33 | 0.634 b |
| Falls | 9/31 | 10/33 | 0.721 b |
| Socioeconomic Factors | |||
| Living at home with family | 25/31 | 24/33 | 0.673 b |
| Living at home alone | 6/31 | 9/33 | 0.598 b |
| Smoking | 12/31 | 13/33 | 0.726 b |
| Groups | SARS-CoV-2 Group n = 31 Mean ± SD | Control Group n = 33 Mean ± SD | p-Value | |
|---|---|---|---|---|
| Biodex Balance indices | APSI | 3.05 ± 0.42 | 2.26 ± 0.31 | 0.013 * |
| MLSI | 2.17 ± 0.28 | 1.43 ± 0.2 | 0.018 * | |
| OSI | 3.25 ± 0.45 | 2.16 ± 0.32 | 0.011 * | |
| FRI | 5.32 ± 0.79 | 3.86 ± 0.46 | 0.008 * | |
| Berg Balance Scale score | 41.92 ± 5.64 | 50.02 ± 4.64 | 0.003 * | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Bagalaty, A.E.; Mohamed, M.E.-S.; Abdelraouf, O.R.; Abdel Ghafar, M.A.; Abdelaal, A.K.; Abdelgalil, A.A.; Mousa, G.S. Balance and Fall Risk Assessment in Community-Dwelling Older Adults after Recovery from COVID-19: A Cross-Sectional Study. Sports 2023, 11, 28. https://doi.org/10.3390/sports11020028
El-Bagalaty AE, Mohamed ME-S, Abdelraouf OR, Abdel Ghafar MA, Abdelaal AK, Abdelgalil AA, Mousa GS. Balance and Fall Risk Assessment in Community-Dwelling Older Adults after Recovery from COVID-19: A Cross-Sectional Study. Sports. 2023; 11(2):28. https://doi.org/10.3390/sports11020028
Chicago/Turabian StyleEl-Bagalaty, Amira E., Mariam El-Sayed Mohamed, Osama R. Abdelraouf, Mohamed A. Abdel Ghafar, Alshaimaa K. Abdelaal, Abdelgalil A. Abdelgalil, and Gihan S. Mousa. 2023. "Balance and Fall Risk Assessment in Community-Dwelling Older Adults after Recovery from COVID-19: A Cross-Sectional Study" Sports 11, no. 2: 28. https://doi.org/10.3390/sports11020028