Performance and Recovery of Well-Trained Younger and Older Athletes during Different HIIT Protocols


 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Younger Athletes (n = 12) | Older Athletes (n = 12) | p-Values |
|---|---|---|---|
| Age (years) | 24.5 ± 3.7 | 47.3 ± 8.6 | <0.001 |
| Height (m) | 1.76 ± 0.11 | 1.72 ± 0.11 | 0.423 |
| Body mass (kg) | 65.9 ± 10.9 | 70.8 ± 11.0 | 0.281 |
| BMI (kg/m2) | 21.1 ± 1.8 | 23.7 ± 2.2 | 0.004 |
| Body fat (%) | 9.8 ± 6.3 | 14.9 ± 6.1 | 0.011 |
| FFM (kg) | 59.8 ± 12.0 | 59.3 ± 9.5 | 0.901 |
| VO2max (mL/min/kg) | 56.7 ± 7.0 | 49.2 ± 6.4 | 0.011 |
| HRmax (min−1) | 179.2 ± 11.1 | 174.9 ± 11.7 | 0.371 |
| Peak Power (W/kg) | 5.24 ± 0.58 | 4.66 ± 0.43 | 0.011 |
| Peak Power (W/kgFFM) | 5.79 ± 0.47 | 5.60 ± 0.71 | 0.122 |
| VO2max-percentile (%) | 95.4 ± 5.2 | 93.1 ± 5.8 | 0.326 |
| Training (h/week) | 8.73 ± 3.62 | 8.37 ± 2.28 | 0.627 |
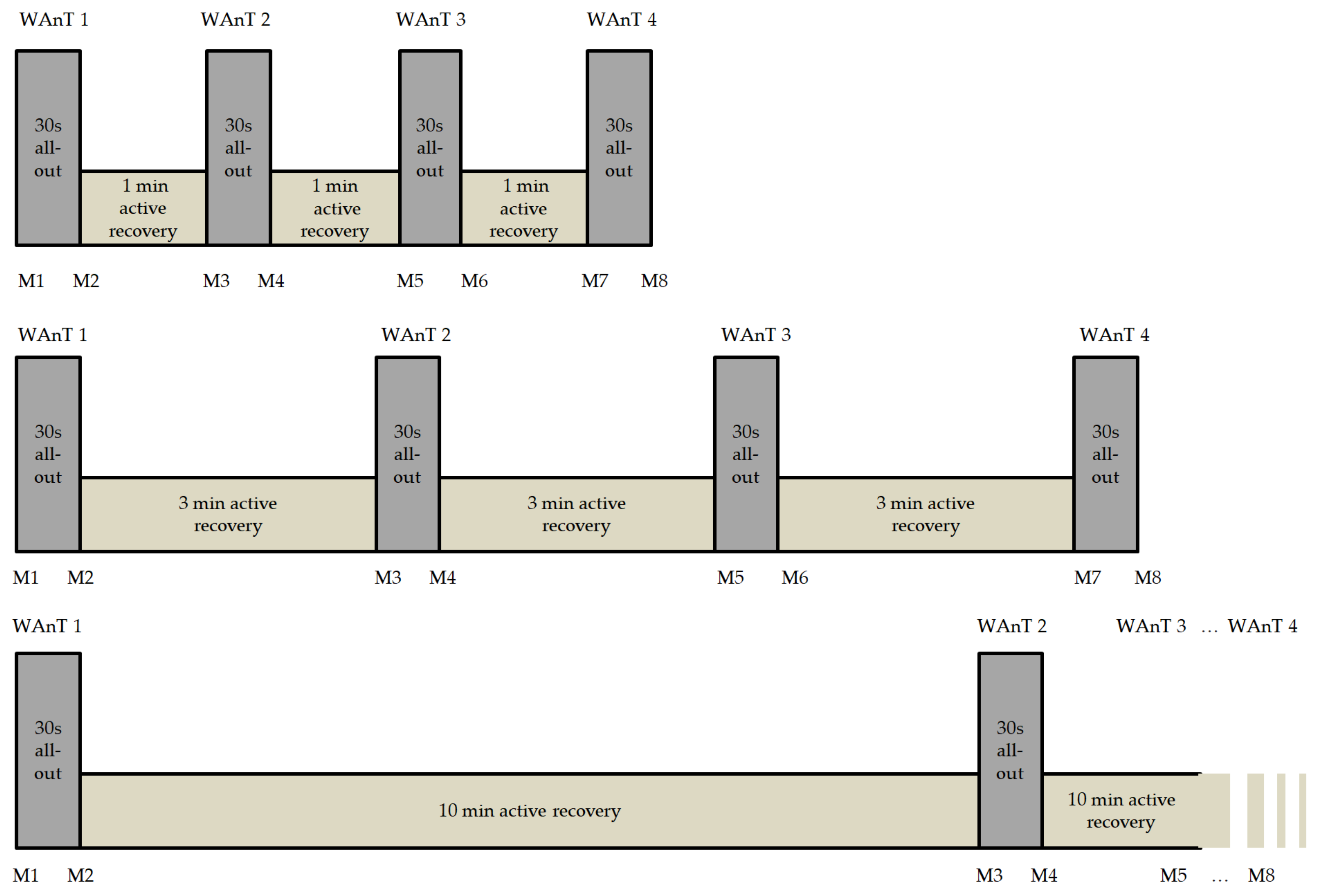
2.2. Test Protocol
2.3. Statistical Analysis
3. Results
3.1. Power
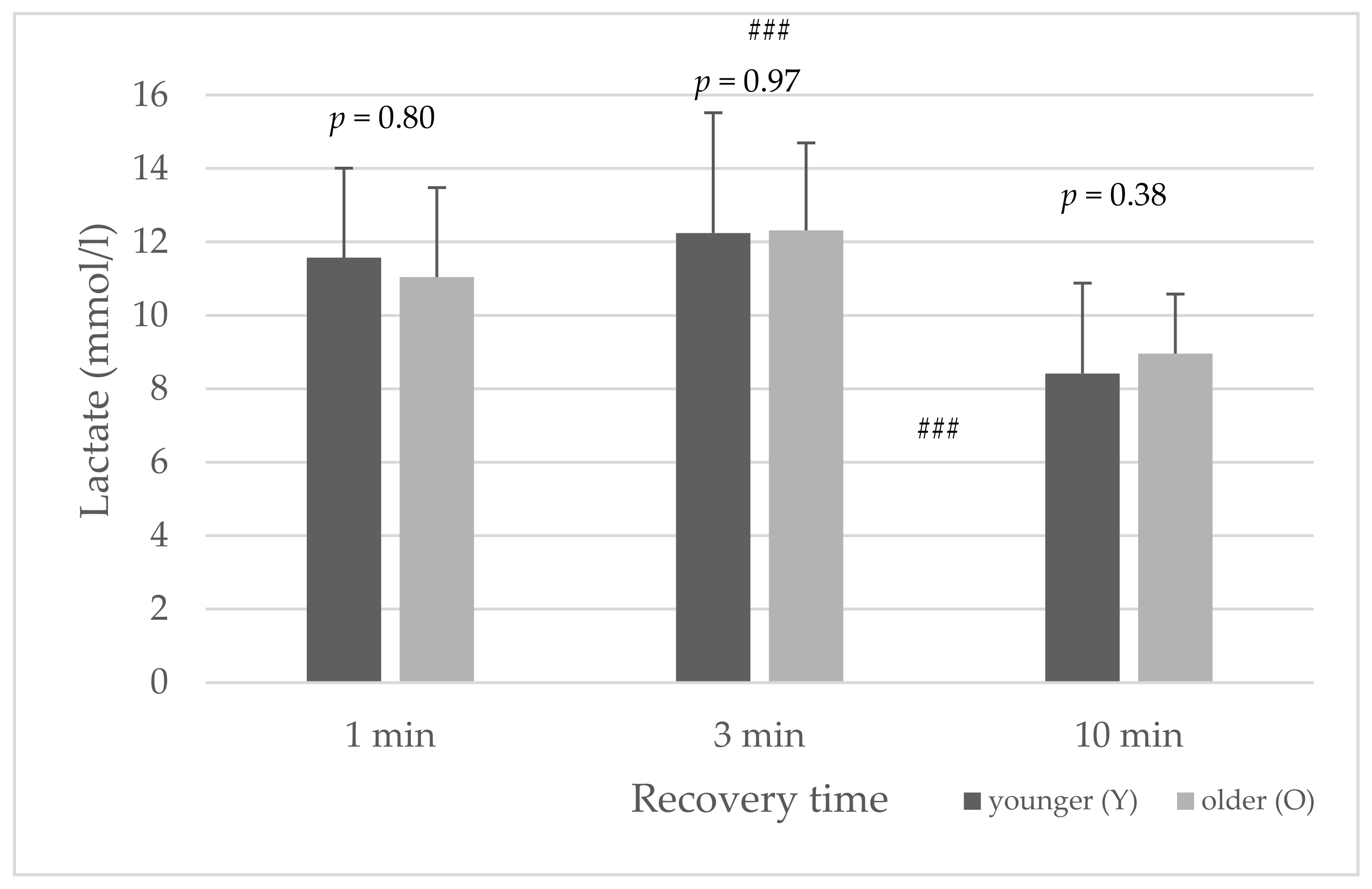
3.2. Lactate
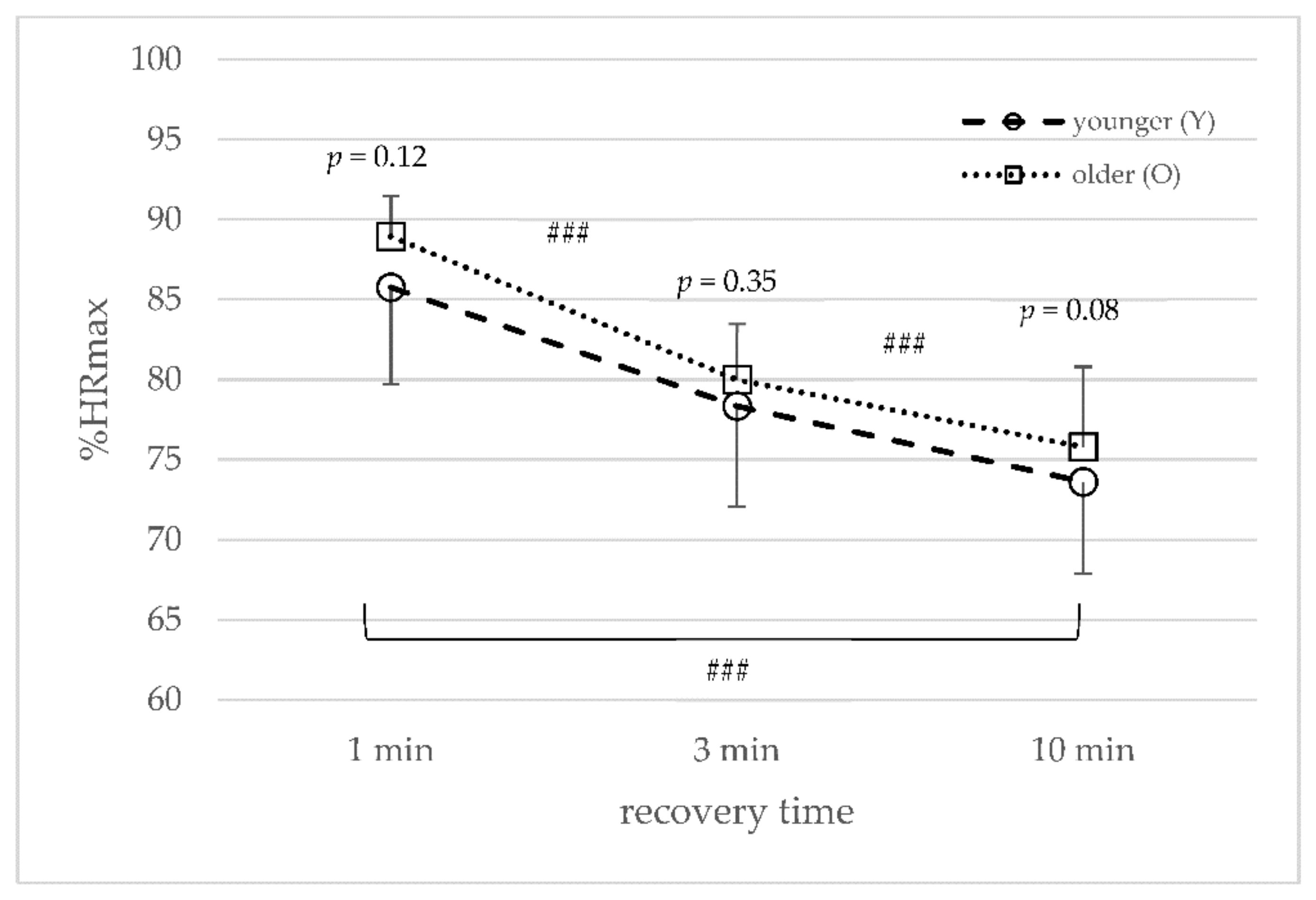
3.3. Heart Rate
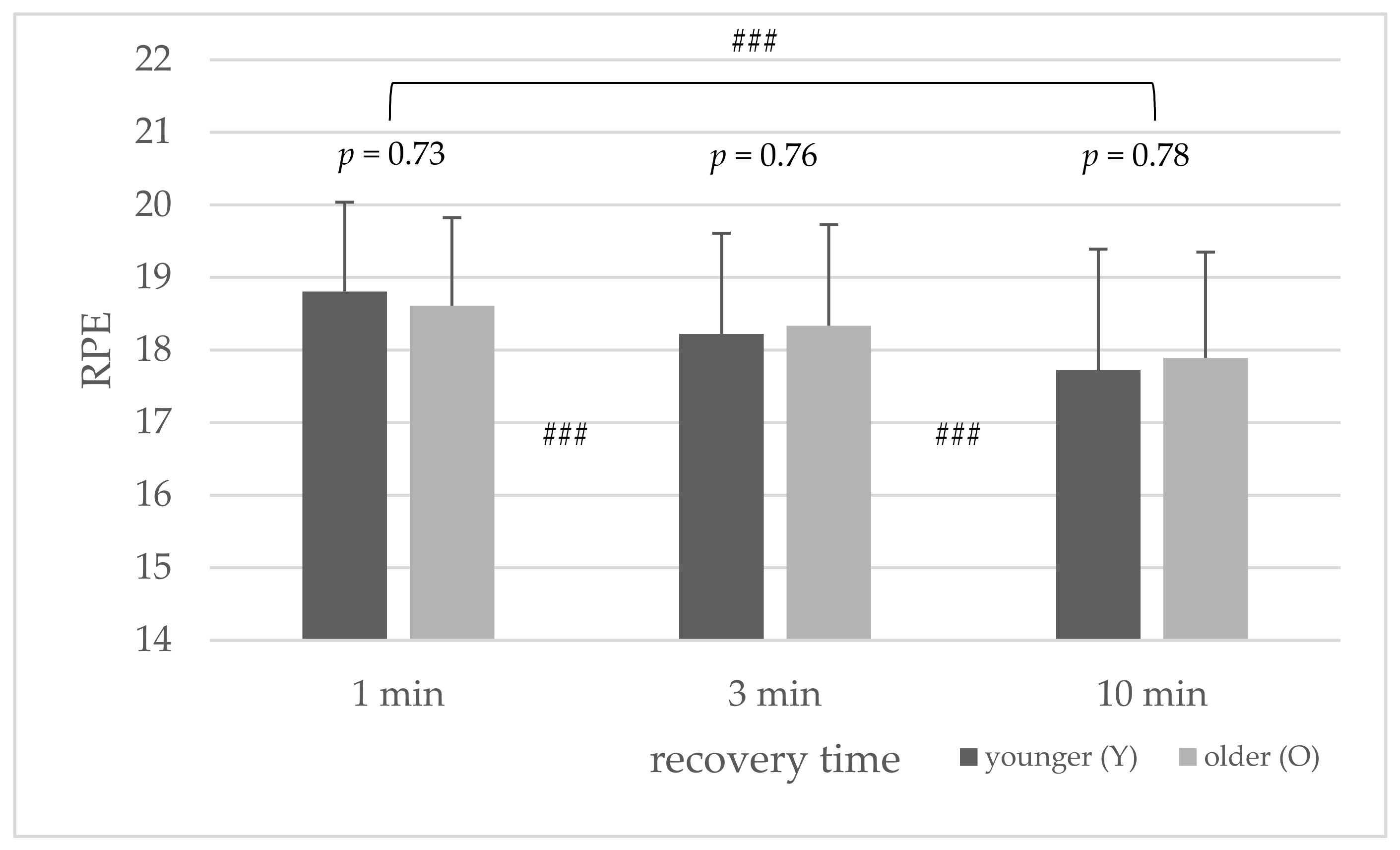
3.4. Subjective Rating of Perceived Exertion (RPE Scale)
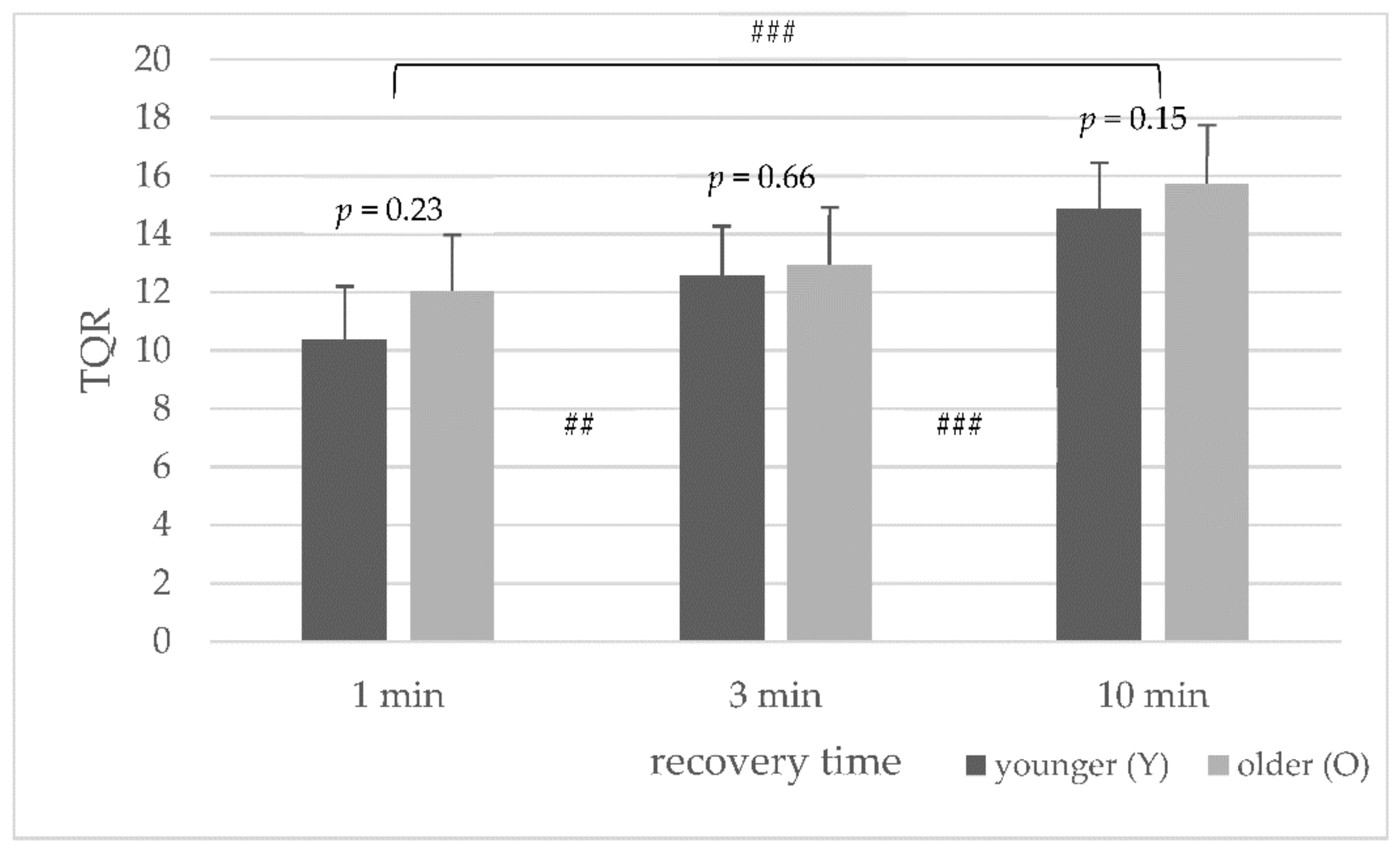
3.5. Subjective Rating of Perceived Recovery (TQR Scale)
3.6. Ventilatory Parameter during Recovery
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Hausswirth, C.; Mujika, I. Recovery for Performance in Sport; Human Kinetics: Champaign, IL, USA, 2013. [Google Scholar]
- Kellmann, M.; Bertollo, M.; Bosquet, L.; Brink, M.; Coutts, A.J.; Duffield, R.; Erlacher, D.; Halson, S.L.; Hecksteden, A.; Heidari, J.; et al. Recovery and Performance in Sport: Consensus Statement. Int. J. Sports Physiol. Perform. 2018, 13, 240–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fell, J.; Williams, A.D. The effect of aging on skeletal-muscle recovery from exercise: Possible implications for aging athletes. J. Aging Phys. Act. 2008, 16, 97–115. [Google Scholar] [CrossRef] [Green Version]
- Easthope, C.S.; Hausswirth, C.; Louis, J.; Lepers, R.; Vercruyssen, F.; Brisswalter, J. Effects of a trail running competition on muscular performance and efficiency in well-trained young and master athletes. Eur. J. Appl. Physiol. 2010, 110, 1107–1116. [Google Scholar] [CrossRef] [Green Version]
- Hottenrott, L.; Ketelhut, S.; Schneider, C.; Wiewelhove, T.; Ferrauti, A. Age-and Sex-Related Differences in Recovery From High-Intensity and Endurance Exercise: A Brief Review. Int. J. Sports Physiol. Perform. 2021, 16, 752–762. [Google Scholar] [CrossRef] [PubMed]
- McCormick, R.; Vasilaki, A. Age-related changes in skeletal muscle: Changes to life-style as a therapy. Biogerontology 2018, 19, 519–536. [Google Scholar] [CrossRef] [Green Version]
- Faulkner, J.A.; Davis, C.S.; Mendias, C.L.; Brooks, S.V. The aging of elite male athletes: Age-related changes in performance and skeletal muscle structure and function. Clin. J. Sport Med. 2008, 18, 501. [Google Scholar] [CrossRef]
- Bieuzen, F.; Hausswirth, C.; Louis, J.; Brisswalter, J. Age-related changes in neuromuscular function and performance following a high-intensity intermittent task in endurance-trained men. Gerontology 2010, 56, 66–72. [Google Scholar] [CrossRef]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-Predicted Maximal Heart Rate Revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef] [Green Version]
- Juel, C.; Klarskov, C.; Nielsen, J.J.; Krustrup, P.; Mohr, M.; Bangsbo, J. Effect of high-intensity intermittent training on lactate and H+ release from human skeletal muscle. Am. J. Physiol. Endocrinol. Metab. 2014, 286, E245–E251. [Google Scholar] [CrossRef] [Green Version]
- Berthelot, G.; Bar-Hen, A.; Marck, A.; Foulonneau, V.; Douady, S.; Noirez, P.; Toussaint, J.F. An integrative modeling approach to the age-performance relationship in mammals at the cellular scale. Sci Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef]
- Korhonen, M.T.; Suominen, H.; Mero, A. Age and sex differences in blood lactate response to sprint running in elite master athletes. Can. J. Appl. Physiol. 2005, 30, 647–665. [Google Scholar] [CrossRef] [PubMed]
- Hunter, G.R.; Newcomer, B.R.; Weinsier, R.L.; Karapondo, D.L.; Larson-Meyer, D.E.; Joanisse, D.R.; Bamman, M.M. Age is independently related to muscle metabolic capacity in premenopausal women. J. Appl. Physiol. 2002, 93, 70–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, J.L.; Mazzeo, R.S.; Podolin, D.A.; Cartee, G.D.; Stanley, W.C. Exercise training does not compensate for age-related decrease in myocardial GLUT-4 content. J. Appl. Physiol. 1994, 76, 328–332. [Google Scholar] [CrossRef]
- Cicioni-Kolsky, D.; Lorenzen, C.; Williams, M.D.; Kemp, J.G. Endurance and sprint benefits of high-intensity and supramaximal interval training. Eur. J. Sport Sci. 2013, 13, 304–311. [Google Scholar] [CrossRef]
- Milanović, Z.; Sporiš, G.; Weston, M. Effectiveness of High-Intensity Interval Training (HIT) and Continuous Endurance Training for VO2max Improvements: A Systematic Review and Meta-Analysis of Controlled Trials. Sports Med. 2015, 45, 1469–1481. [Google Scholar] [CrossRef]
- Sloth, M.; Sloth, D.; Overgaard, K.; Dalgas, U. Effects of Sprint Interval Training on VO2max and Aerobic Exercise Performance: A Systematic Review and Meta-Analysis. Scand J. Med. Sci. Sports 2013, 23, e341–e352. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M.; Laursen, P.B. High-Intensity Interval Training, Solutions to the Programming Puzzle: Part I: Cardiopulmonary Emphasis. Sports Med. 2013, 43, 313–338. [Google Scholar] [CrossRef]
- Buchheit, M.; Laursen, P. Science and application of high-intensity interval training: Solutions to the programming puzzle. In Physiological Targets of HIIT; Laursen, P., Buchheit, M., Eds.; Human Kinetics: Champaign, IL, USA, 2018; pp. 33–50. [Google Scholar]
- Mujika, I. Quantification of Training and Competition Loads in Endurance Sports: Methods and Applications. Int. J. Sports Physiol. Perform. 2017, 12, S2–S9. [Google Scholar] [CrossRef] [PubMed]
- Hebestreit, H.; Mimura, K.; Bar-Or, O. Recovery of muscle power after high-intensity short-term exercise: Comparing boys and men. J. Appl. Physiol. 1993, 74, 2875–2880. [Google Scholar] [CrossRef]
- Laursen, P.; Buchheit, M.; Vollmer, J.C. Science and application of high-intensity interval training: Solutions to the programming puzzle. In Genesis and Evolution of High-Intensity Interval Training; Laursen, P., Buchheit, M., Eds.; Human Kinetics: Champaign, IL, USA, 2018; pp. 3–15. [Google Scholar]
- Hottenrott, L.; Möhle, M.; Ide, A.; Ketelhut, S.; Stoll, O.; Hottenrott, K. Recovery from Different High-Intensity Interval Training Protocols: Comparing Well-Trained Women and Men. Sports 2021, 9, 34. [Google Scholar] [CrossRef]
- Ohuchi, H.; Suzuki, H.; Yasuda, K.; Arakaki, Y.; Echigo, S.; Kamiya, T. Heart rate recovery after exercise and cardiac autonomic nervous activity in children. Pediatr. Res. 2000, 47, 329. [Google Scholar] [CrossRef] [Green Version]
- Birat, A.; Bourdier, P.; Piponnier, E.; Blazevich, A.J.; Maciejewski, H.; Duché, P.; Ratel, S. Metabolic and fatigue profiles are comparable between prepubertal children and well-trained adult endurance athletes. Front. Physiol. 2018, 9, 387. [Google Scholar] [CrossRef] [Green Version]
- Buchheit, M.; Duche, P.; Laursen, P.B.; Ratel, S. Postexercise heart rate recovery in children: Relationship with power output, blood pH, and lactate. Appl. Physiol. Nutr. Metab. 2010, 35, 142–150. [Google Scholar] [CrossRef]
- Kappenstein, J.; Fernández-Fernández, J.; Engel, F.; Ferrauti, A. Effects of active and passive recovery on blood lactate and blood pH after a repeated sprint protocol in children and adults. Pediatr. Exerc Sci. 2015, 27, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Chamari, K.; Ahmaidi, S.; Ayoub, J.; Merzouk, A.; Laparidis, C.; Choquet, D.; Mercier, J.; Préfaut, C. Effects of aging on cardiorespiratory responses to brief and intense intermittent exercise in endurance-trained athletes. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, 537–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandewalle, H.; Pérès, G.; Monod, H. Standard Anaerobic Exercise Tests. Sports Med. 1987, 4, 268–289. [Google Scholar] [CrossRef] [PubMed]
- Bar-Or, O. The Wingate Anaerobic Test: An Update on Methodology, Reliability and Validity. Sports Med. 1987, 4, 381–394. [Google Scholar] [CrossRef]
- Inbar, O.; Bar-Or, O.; Skinner, J.S. The Development of the Wingate Anaerobic Test. In The Wingate Anaerobic Test; Human Kinetics: Champaign, IL, USA, 1996; pp. 1–7. [Google Scholar]
- Patton, J.F.; Duggan, A. An evaluation of tests of anaerobic power. Aviat. Space Environ. Med. 1987, 58, 237–242. [Google Scholar]
- Lovell, D.; Mason, D.; Delphinus, E.; Eagles, A.; Shewring, S.; McLellan, C. Does Upper Body Strength and Power Influence Upper Body Wingate Performance in Men and Women? Int. J. Sports Med. 2011, 32, 771–775. [Google Scholar] [CrossRef]
- Graves, R.S.; Mahnken, J.D.; Perea, R.D.; Billinger, S.A.; Vidoni, E.D. Modeling Percentile Rank of Cardiorespiratory Fitness Across the Lifespan. Cardiopulm. Phys. Ther. J. 2015, 26, 108–113. [Google Scholar] [CrossRef] [Green Version]
- Midgley, A.W.; Carroll, S.; Marchant, D.; McNaughton, L.R.; Siegler, J. Evaluation of true maximal oxygen uptake based on a novel set of standardized criteria. Appl. Physiol. Nutr. Metabolism. 2009, 34, 115–123. [Google Scholar] [CrossRef] [Green Version]
- Beltz, N.M.; Gibson, A.L.; Janot, J.M.; Kravitz, L.; Mermier, C.M.; Dalleck, L.C. Graded exercise testing protocols for the determination of VO2max: Historical perspectives, progress, and future considerations. J. Sports Med. 2016, 2016, 3968393. [Google Scholar] [CrossRef] [Green Version]
- Borg, G.; Hassmén, P.; Lagerström, M. Perceived exertion related to heart rate and blood lactate during arm and leg exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1987, 56, 679–685. [Google Scholar] [CrossRef]
- Kenttä, G.; Hassmén, P. Overtraining and recovery. A conceptual model. Sports Med. 1998, 26, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.A.; Quinney, H.A. Determination of resistance settings for anaerobic power testing. Can. J. Appl. Sport Sci. J. Can. Sci. Appl. Sport. 1981, 6, 53–56. [Google Scholar]
- Hopkins, W.G. Spreadsheets for analysis of controlled trials, with adjustment for a subject characteristic. Sport Sci. 2006, 10, 46–50. [Google Scholar]
- Lievens, E.; Klass, M.; Bex, T.; Derave, W. Muscle Fiber Typology Substantially Influences Time to Recover from High-Intensity Exercise. J. Appl. Physiol. 2020, 128, 648–659. [Google Scholar] [CrossRef]
- Fell, J.; Haseler, L.; Gaffney, P.; Reaburn, P.; Harrison, G. Performance during consecutive days of laboratory time-trials in young and veteran cyclists. J. Sports Med. Phys. Fitness 2006, 46, 395–402. [Google Scholar]
- Fell, J.; Reaburn, P.; Harrison, G.J. Altered perception and report of fatigue and recovery in veteran athletes. J. Sports Med. Phys. Fitness 2008, 48, 272. [Google Scholar]
- Silverman, H.G.; Mazzeo, R.S. Hormonal responses to maximal and submaximal exercise in trained and untrained men of various ages. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1996, 51, B30–B37. [Google Scholar] [CrossRef] [PubMed]
- Darr, K.C.; Bassett, D.R.; Morgan, B.J.; Thomas, D.P. Effects of age and training status on heart rate recovery after peak exercise. Am. J. Physiol. 1988, 254, H340–H343. [Google Scholar] [CrossRef] [PubMed]
- Laursen, P.; Buchheit, M. Science and Application of High-Intensity Interval Training; Human Kinetics: Champaign, IL, USA, 2019; pp. 68–69. [Google Scholar]






| Parameter | Recovery | Age | WAnT 1 | WAnT 2 | WAnT 3 | WAnT 4 | T1–T4 |
|---|---|---|---|---|---|---|---|
| Peak Power (W) | 1 min | Y | 734.8 ± 225.4 | 583.5 ± 157.3 *** | 554.4 ± 140.3 * | 530.5 ± 131.7 | p < 0.001 |
| O | 724.1 ± 181.2 | 579.8 ± 145.4 *** | 550.3 ± 135.3 | 533.7 ± 145.5 | p < 0.001 | ||
| Av. Power (W) | Y | 535.8 ± 192.3 | 454.8 ± 157.5 *** | 422.4 ± 141.3 *** | 410.1 ± 135.3 * | p < 0.001 | |
| O | 485.8 ± 126.3 | 418.4 ± 110.2 *** | 402.3 ± 109.5 * | 395.3 ± 119.0 | p < 0.001 | ||
| Fatigue (%) | Y | 27.3 ± 12.1 | 23.3 ± 9.8 * | 25.1 ± 9.0 | 23.6 ± 10.9 | p = 0.11 | |
| O | 32.7 ± 9.0 | 27.7 ± 9.6 * | 26.8 ± 12.0 | 26.4 ± 8.2 | p = 0.01 | ||
| Peak Power (W) | 3 min | Y | 739.4 ± 218.5 | 663.8 ± 183.4 ** | 637.3 ± 188.8 * | 608.8 ± 160.7 * | p < 0.001 |
| O | 731.0 ± 130.5 | 671.8 ± 151.0 ** | 629.1 ± 137.7 * | 617.6 ± 129.5 | p < 0.001 | ||
| Av. Power (W) | Y | 537.7 ± 202.6 | 498.4 ± 180.7 ** | 476.8 ± 172.0 *** | 465.3 ± 166.2 ** | p < 0.001 | |
| O | 499.8 ± 134.4 | 471.2 ± 125.7 *** | 447.3 ± 117.4 ** | 445.8 ± 115.3 | p < 0.001 | ||
| Fatigue (%) | Y | 28.4 ± 11.1 | 26.0 ± 11.9 | 26.3 ± 9.7 | 25.0 ± 11.0 | p = 0.09 | |
| O | 32.4 ± 10.7 | 29.9 ± 11.7 | 29.4 ± 8.8 | 28.1 ± 10.6 | p = 0.06 | ||
| Peak Power (W) | 10 min | Y | 749.8 ± 217.3 | 692.0 ± 207.0 ** | 682.1 ± 216.9 | 678.2 ± 194.4 | p < 0.001 |
| O | 728.8 ± 187.6 | 709.6 ± 156.9 | 691.1 ± 149.7 | 672.8 ± 150.3 | p = 0.04 | ||
| Av. Power (W) | Y | 536.2 ± 202.1 | 526.0 ± 193.2 | 523.2 ± 193.3 | 520.1 ± 188.9 | p = 0.03 | |
| O | 500.4 ± 141.4 | 504.0 ± 131.8 | 499.3 ± 130.7 | 493.3 ± 129.5 | p = 0.43 | ||
| Fatigue (%) | Y | 29.7 ± 10.6 | 25.1 ± 9.6 ** | 24.3 ± 8.3 | 24.7 ± 9.5 | p < 0.001 | |
| O | 31.3 ± 10.1 | 29.2 ± 9.6 | 28.1 ± 9.1 | 26.6 ± 11.8 | p = 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hottenrott, L.; Möhle, M.; Feichtinger, S.; Ketelhut, S.; Stoll, O.; Hottenrott, K. Performance and Recovery of Well-Trained Younger and Older Athletes during Different HIIT Protocols. Sports 2022, 10, 9. https://doi.org/10.3390/sports10010009
Hottenrott L, Möhle M, Feichtinger S, Ketelhut S, Stoll O, Hottenrott K. Performance and Recovery of Well-Trained Younger and Older Athletes during Different HIIT Protocols. Sports. 2022; 10(1):9. https://doi.org/10.3390/sports10010009
Chicago/Turabian StyleHottenrott, Laura, Martin Möhle, Sarah Feichtinger, Sascha Ketelhut, Oliver Stoll, and Kuno Hottenrott. 2022. "Performance and Recovery of Well-Trained Younger and Older Athletes during Different HIIT Protocols" Sports 10, no. 1: 9. https://doi.org/10.3390/sports10010009