
Graft-Derived Cell-Free DNA Quantification following Liver Transplantation Using Tissue-Specific DNA Methylation and Donor-Specific Genotyping Techniques: An Orthogonal Comparison Study
 , , and
, , and
Abstract
:1. Background
2. Materials and Methods
2.1. Patient Recruitment
2.2. Sample Collection, Processing and Storage
2.3. DNA Extraction and Bisulfite Modification
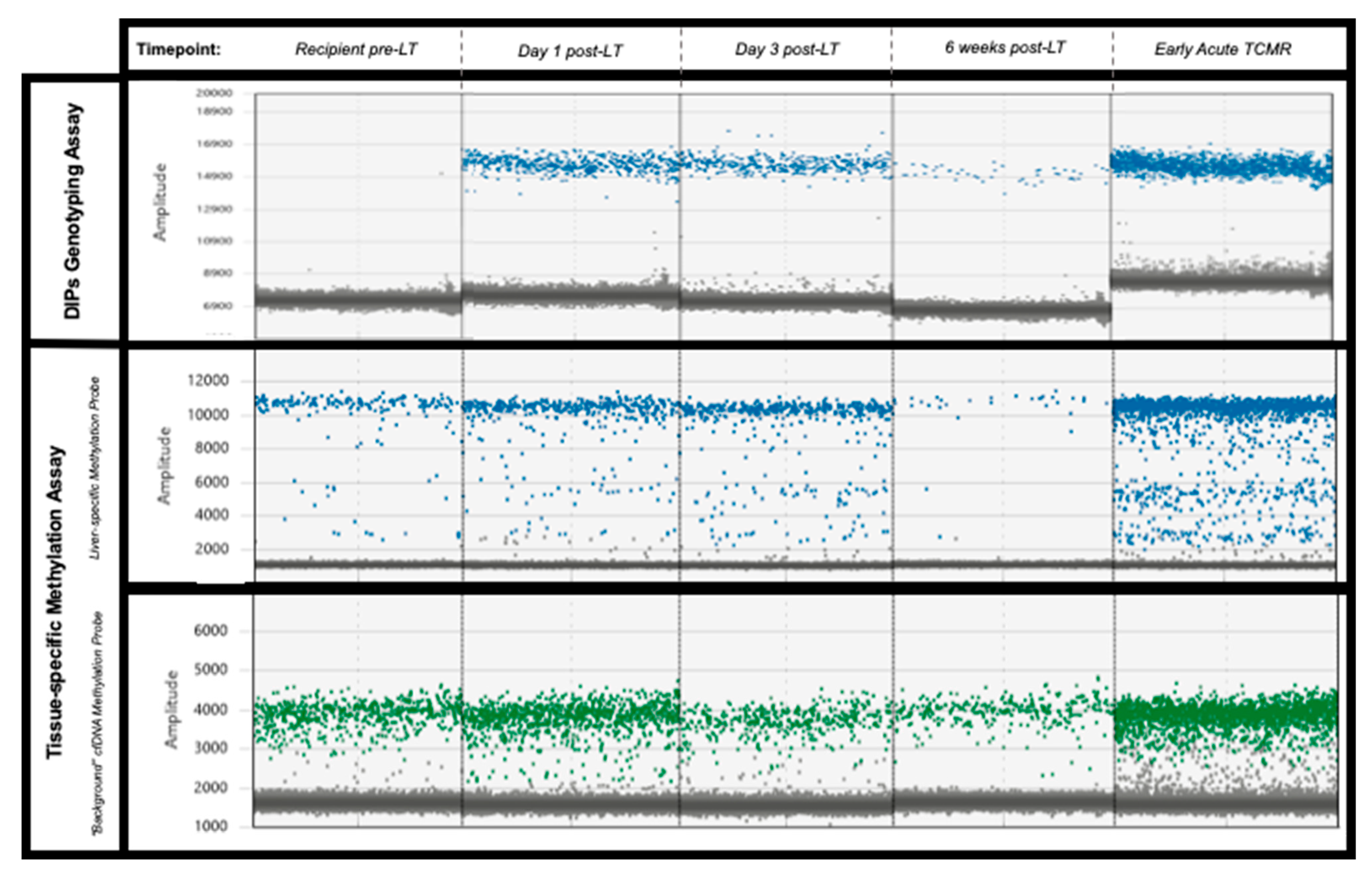
2.4. gdcfDNA Quantification: Donor-Specific Genetic Polymorphism Technique
2.4.1. Genotyping for Identification of Informative Deletion/Insertion Genetic Polymorphisms
2.4.2. Monitoring gdcfDNA Post-LT Using Insertion/Deletion Genetic Polymorphisms
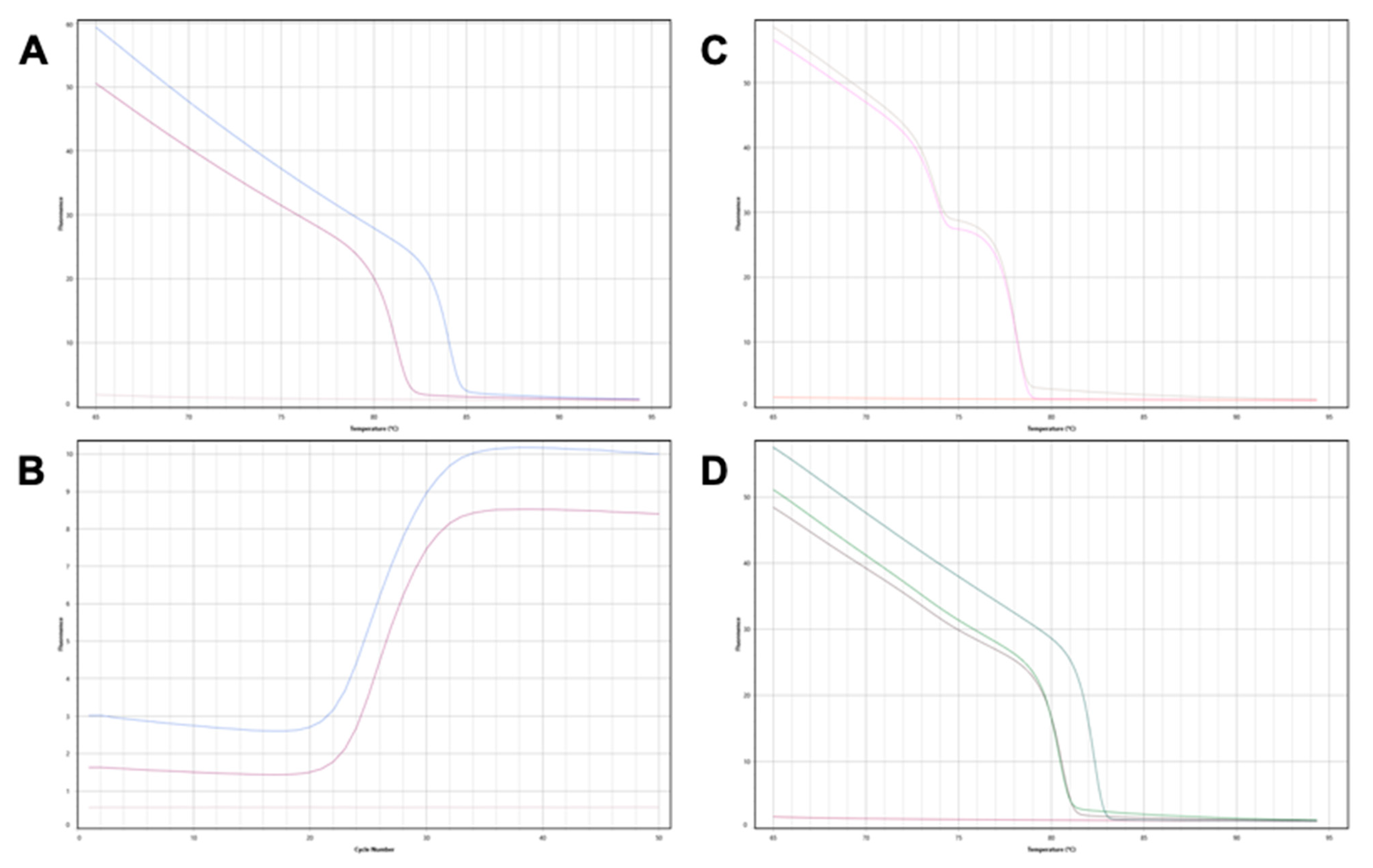
2.5. gdcfDNA Quantification: Tissue-Specific DNA Methylation Technique
2.6. Outcomes and Data Collection
2.7. Statistical Analysis
3. Results
3.1. Patient Outcomes
3.2. gdcfDNA Analysis
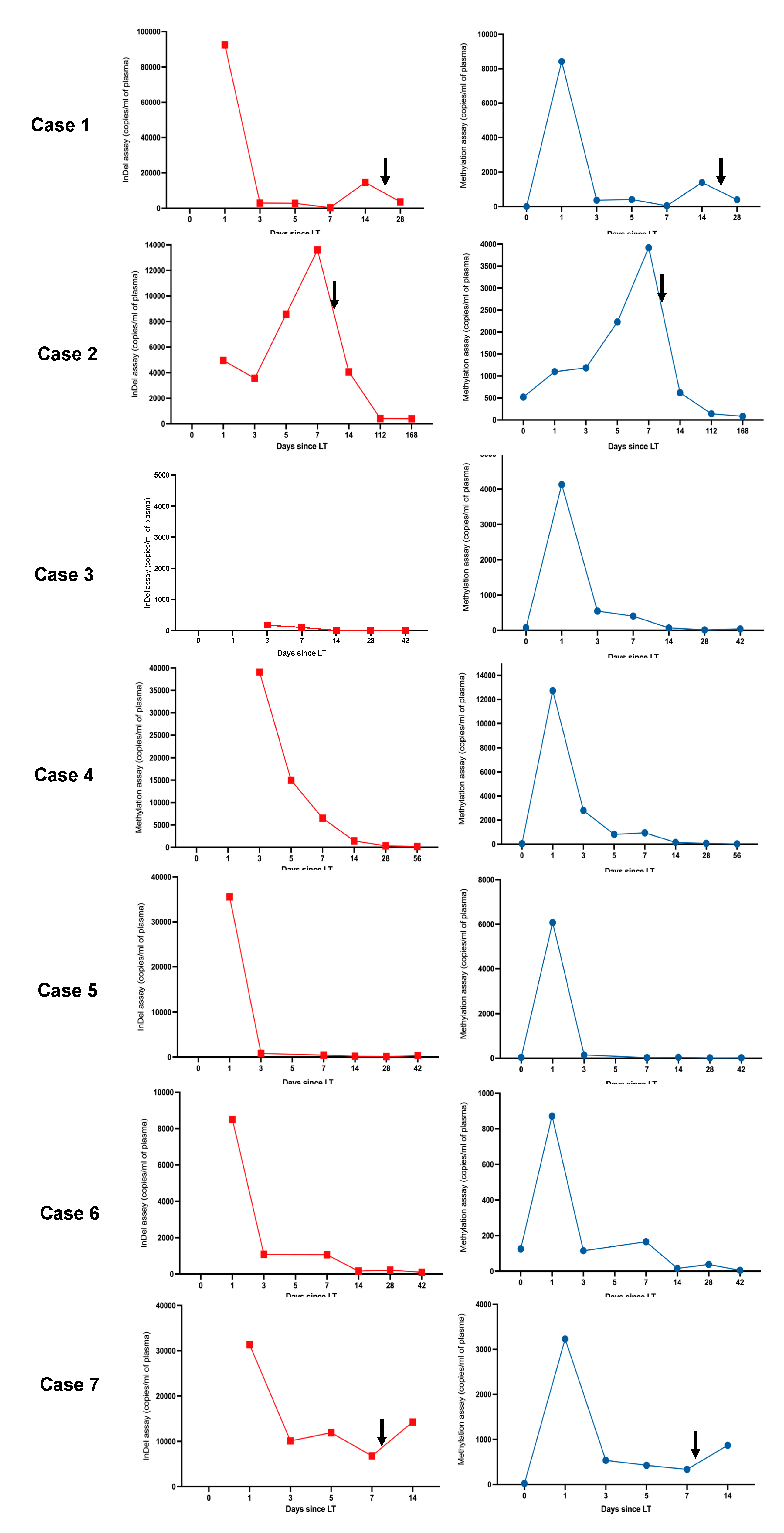
3.2.1. gdcfDNA Results: Genetic Polymorphism Technique
3.2.2. gdcfDNA Results: Tissue-Specific DNA Methylation Technique
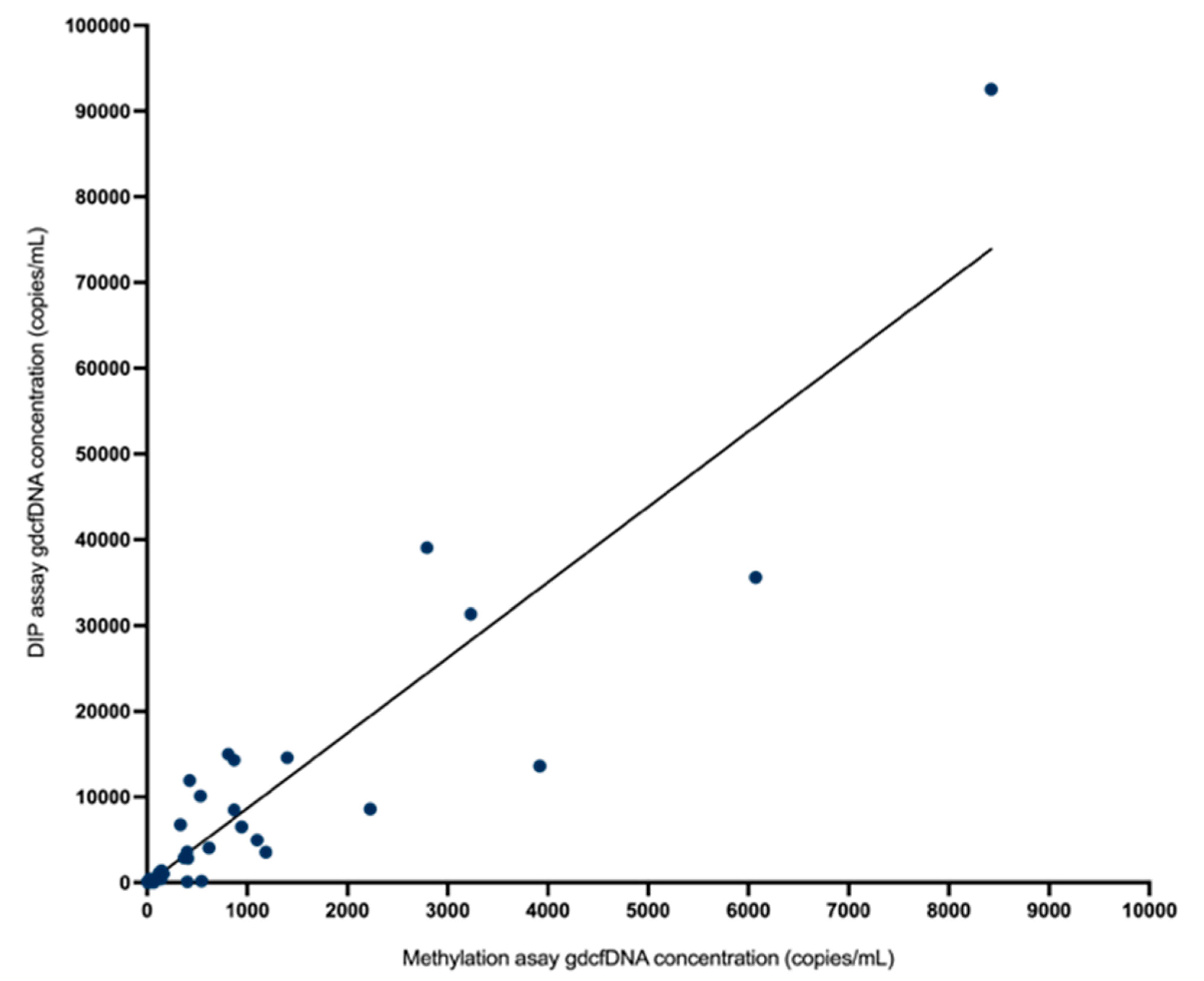
3.3. Comparative Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Shaked, A.; Ghobrial, R.M.; Merion, R.M.; Shearon, T.H.; Emond, J.C.; Fair, J.H.; Fisher, R.A.; Kulik, L.M.; Pruett, T.L.; Terrault, N.A. Incidence and Severity of Acute Cellular Rejection in Recipients Undergoing Adult Living Donor or Deceased Donor Liver Transplantation. Am. J. Transplant. 2009, 9, 301–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guiral, S.; Segundo, D.S.; Irure, J.; Casafont, F.; Fortea, J.I.; Puente, Á.; Fabrega, E. Number of Antibody-verified Eplet in HLA-C Locus as an Independent Factor of T-cell–Mediated Rejection After Liver Transplantation. Transplantation 2020, 104, 562–567. [Google Scholar] [CrossRef] [PubMed]
- Levitsky, J.; Goldberg, D.; Smith, A.R.; Mansfield, S.A.; Gillespie, B.W.; Merion, R.M.; Lok, A.S.; Levy, G.; Kulik, L.; Abecassis, M.; et al. Acute Rejection Increases Risk of Graft Failure and Death in Recent Liver Transplant Recipients. Clin. Gastroenterol. Hepatol. 2017, 15, 584–593.e2. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Perálvarez, M.; Germani, G.; Tsochatzis, E.; Rolando, N.; Luong, T.V.; Dhillon, A.P.; Thorburn, D.; O’beirne, J.; Patch, D.; Burroughs, A.K. Predicting severity and clinical course of acute rejection after liver transplantation using blood eosinophil count. Transpl. Int. 2012, 25, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Wiesner, R.H.; Demetris, A.J.; Belle, S.H.; Seaberg, E.C.; Lake, J.R.; Zetterman, R.K.; Everhart, J.; Detre, K.M. Acute hepatic allograft rejection: Incidence, risk factors, and impact on outcome. Hepatology 1998, 28, 638–645. [Google Scholar] [CrossRef]
- Demetris, A.J.; Bellamy, C.; Hübscher, S.G.; O’Leary, J.; Randhawa, P.S.; Feng, S.; Neil, D.; Colvin, R.B.; McCaughan, G.; Fung, J.J.; et al. 2016 Comprehensive Update of the Banff Working Group on Liver Allograft Pathology: Introduction of Antibody-Mediated Rejection. Am. J. Transplant. 2016, 16, 2816–2835. [Google Scholar] [CrossRef] [Green Version]
- Van Ha, T. Liver Biopsy in Liver Transplant Recipients. Semin. Interv. Radiol. 2004, 21, 271–274. [Google Scholar] [CrossRef] [Green Version]
- Tie, J.; Cohen, J.D.; Lahouel, K.; Lo, S.N.; Wang, Y.; Kosmider, S.; Wong, R.; Shapiro, J.; Lee, M.; Harris, S.; et al. Circulating Tumor DNA Analysis Guiding Adjuvant Therapy in Stage II Colon Cancer. N. Engl. J. Med. 2022, 386, 2261–2272. [Google Scholar] [CrossRef]
- Mathios, D.; Johansen, J.S.; Cristiano, S.; Medina, J.E.; Phallen, J.; Larsen, K.R.; Bruhm, D.C.; Niknafs, N.; Ferreira, L.; Adleff, V.; et al. Detection and characterization of lung cancer using cell-free DNA fragmentomes. Nat. Commun. 2021, 12, 5060. [Google Scholar] [CrossRef]
- Stokowski, R.; Wang, E.; White, K.; Batey, A.; Jacobsson, B.; Brar, H.; Balanarasimha, M.; Hollemon, D.; Sparks, A.; Nicolaides, K.; et al. Clinical performance of non-invasive prenatal testing (NIPT) using targeted cell-free DNA analysis in maternal plasma with microarrays or next generation sequencing (NGS) is consistent across multiple controlled clinical studies. Prenat. Diagn. 2015, 35, 1243–1246. [Google Scholar] [CrossRef] [Green Version]
- Kataria, A.; Kumar, D.; Gupta, G. Donor-derived Cell-free DNA in Solid-organ Transplant Diagnostics: Indications, Limitations, and Future Directions. Transplantation 2021, 105, 1203–1211. [Google Scholar] [CrossRef] [PubMed]
- McClure, T.; Goh, S.K.; Cox, D.; Muralidharan, V.; Dobrovic, A.; Testro, A.G. Donor-specific cell-free DNA as a biomarker in liver transplantation: A review. World J. Transplant. 2020, 10, 307–319. [Google Scholar] [CrossRef] [PubMed]
- Knight, S.R.; Thorne, A.; Lo Faro, M.L. Donor-specific Cell-free DNA as a Biomarker in Solid Organ Transplantation. Syst. Rev. Transplant. 2019, 103, 273–283. [Google Scholar]
- Legendre, C.; Gooden, G.C.; Johnson, K.; Martinez, R.A.; Liang, W.S.; Salhia, B. Whole-genome bisulfite sequencing of cell-free DNA identifies signature associated with metastatic breast cancer. Clin. Epigenetics 2015, 7, 100. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.C.; Oxnard, G.R.; Klein, E.A.; Swanton, C.; Seiden, M.V.; CCGA Consortium. Sensitive and specific multi-cancer detection and localization using methylation signatures in cell-free DNA. Ann. Oncol. 2020, 31, 745–759. [Google Scholar] [CrossRef]
- Moss, J.; Magenheim, J.; Neiman, D.; Zemmour, H.; Loyfer, N.; Korach, A.; Samet, Y.; Maoz, M.; Druid, H.; Arner, P.; et al. Comprehensive human cell-type methylation atlas reveals origins of circulating cell-free DNA in health and disease. Nat. Commun. 2018, 9, 5068. [Google Scholar] [CrossRef] [Green Version]
- Lehmann-Werman, R.; Neiman, D.; Zemmour, H.; Moss, J.; Magenheim, J.; Vaknin-Dembinsky, A.; Rubertsson, S.; Nellgard, B.; Blennow, K.; Zetterberg, H.; et al. Identification of tissue-specific cell death using methylation patterns of circulating DNA. Proc. Natl. Acad. Sci. USA 2016, 113, E1826–E1834. [Google Scholar] [CrossRef] [Green Version]
- Jiang, P.; Chan, K.A.; Lo, Y.D. Liver-derived cell-free nucleic acids in plasma: Biology and applications in liquid biopsies. J. Hepatol. 2019, 71, 409–421. [Google Scholar] [CrossRef] [Green Version]
- Lehmann-Werman, R.; Magenheim, J.; Moss, J.; Neiman, D.; Abraham, O.; Piyanzin, S.; Zemmour, H.; Fox, I.; Dor, T.; Grompe, M.; et al. Monitoring liver damage using hepatocyte-specific methylation markers in cell-free circulating DNA. J. Clin. Investig. 2018, 3, e120687. [Google Scholar] [CrossRef] [Green Version]
- Gallo, V.; Egger, M.; McCormack, V.; Farmer, P.B.; Ioannidis, J.P.A.; Kirsch-Volders, M.; Matullo, G.; Phillips, D.H.; Schoket, B.; Stromberg, U.; et al. STrengthening the Reporting of OBservational studies in Epidemiology—Molecular Epidemiology (STROBE-ME): An extension of the STROBE statement. Eur. J. Clin. Investig. 2011, 42, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Kerachian, M.A.; Azghandi, M.; Mozaffari-Jovin, S.; Thierry, A.R. Guidelines for pre-analytical conditions for assessing the methylation of circulating cell-free DNA. Clin. Epigenetics 2021, 13, 193. [Google Scholar] [CrossRef] [PubMed]
- Goh, S.K.; Muralidharan, V.; Christophi, C.; Do, H.; Dobrovic, A. Probe-Free Digital PCR Quantitative Methodology to Measure Donor-Specific Cell-Free DNA after Solid-Organ Transplantation. Clin. Chem. 2017, 63, 742–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gai, W.; Ji, L.; Lam, W.J.; Sun, K.; Jiang, P.; Chan, A.W.; Wong, J.; Lai, P.B.; Ng, S.S.; Ma, B.B.; et al. Liver- and Colon-Specific DNA Methylation Markers in Plasma for Investigation of Colorectal Cancers with or without Liver Metastases. Clin. Chem. 2018, 64, 1239–1249. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Ren, J.; Luo, N.; Guo, H.; Zheng, Y.; Li, J.; Tang, F.; Wen, L.; Peng, J. Comprehensive DNA methylation analysis of tissue of origin of plasma cell-free DNA by methylated CpG tandem amplification and sequencing (MCTA-Seq). Clin. Epigenetics 2019, 11, 93. [Google Scholar] [CrossRef]
- Schütz, E.; Fischer, A.; Beck, J.; Harden, M.; Koch, M.; Wuensch, T.; Stockmann, M.; Nashan, B.; Kollmar, O.; Matthaei, J.; et al. Graft-derived cell-free DNA, a noninvasive early rejection and graft damage marker in liver transplantation: A prospective, observational, multicenter cohort study. PLoS Med. 2017, 14, e1002286. [Google Scholar] [CrossRef] [Green Version]
- Prakash, K.; Aggarwal, S.; Bhardwaj, S.; Ramakrishna, G.; Pandey, C.K. Serial perioperative cell-free DNA levels in donors and recipients undergoing living donor liver transplantation. Acta Anaesthesiol. Scand. 2017, 61, 1084–1094. [Google Scholar] [CrossRef]
- Fernández-Galán, E.; Badenas, C.; Fondevila, C.; Jiménez, W.; Navasa, M.; Puig-Butillé, J.A.; Brunet, M. Monitoring of Donor-Derived Cell-Free DNA by Short Tandem Repeats: Concentration of Total Cell-Free DNA and Fragment Size for Acute Rejection Risk Assessment in Liver Transplantation. Liver Transplant. 2022, 28, 257–268. [Google Scholar] [CrossRef]
- Zhao, D.; Zhou, T.; Luo, Y.; Wu, C.; Xu, D.; Zhong, C.; Cong, W.; Liu, Q.; Zhang, J.; Xia, Q. Preliminary clinical experience applying donor-derived cell-free DNA to discern rejection in pediatric liver transplant recipients. Sci. Rep. 2021, 11, 1138. [Google Scholar] [CrossRef]
- Goh, S.K.; Do, H.; Testro, A.; Pavlovic, J.; Vago, A.; Lokan, J.; Jones, R.M.; Christophi, C.; Dobrovic, A.; Muralidharan, V. The Measurement of Donor-Specific Cell-Free DNA Identifies Recipients with Biopsy-Proven Acute Rejection Requiring Treatment After Liver Transplantation. Transplant. Direct 2019, 5, e462. [Google Scholar] [CrossRef]
- Beck, J.; Bierau, S.; Balzer, S.; Andag, R.; Kanzow, P.; Schmitz, J.; Gaedcke, J.; Moerer, O.; Slotta, J.E.; Walson, P.; et al. Digital Droplet PCR for Rapid Quantification of Donor DNA in the Circulation of Transplant Recipients as a Potential Universal Biomarker of Graft Injury. Clin. Chem. 2013, 59, 1732–1741. [Google Scholar] [CrossRef] [Green Version]
- Macher, H.C.; García-Fernández, N.; Adsuar-Gómez, A.; Porras-López, M.; González-Calle, A.; Noval-Padillo, J.; Guerrero, J.M.; Molinero, P.; Borrego-Domínguez, J.M.; Herruzo-Avilés, Á.; et al. Donor-specific circulating cell free DNA as a noninvasive biomarker of graft injury in heart transplantation. Clin. Chim. Acta 2019, 495, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Dengu, F. Next-generation sequencing methods to detect donor-derived cell-free DNA after transplantation. Transplant. Rev. 2020, 34, 100542. [Google Scholar] [CrossRef] [PubMed]
- Khush, K.K.; Patel, J.; Pinney, S.; Kao, A.; Alharethi, R.; DePasquale, E.; Ewald, G.; Berman, P.; Kanwar, M.; Hiller, D.; et al. Noninvasive detection of graft injury after heart transplant using donor-derived cell-free DNA: A prospective multicenter study. Am. J. Transplant. 2019, 19, 2889–2899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goh, S.K.; Muralidharan, V.; Christophi, C.; Dobrovic, A. Fresh Frozen Plasma Transfusion Can Confound the Analysis of Circulating Cell-Free DNA. Clin. Chem. 2018, 64, 749–751. [Google Scholar] [CrossRef] [PubMed]
- Cox, D.R.A.; Low, N.; Goh, S.K.; Lee, E.; Vago, A.; Jackett, L.; Lokan, J.; Braat, S.; Jones, R.; Testro, A.; et al. Low Levels of Hepatocyte-Specific Methylation in Cell-Free DNA Are a Strong Negative Predictor for Acute T Cell–Mediated Rejection Requiring Treatment Following Liver Transplantation. Liver Transplant. 2022, 28, 1024–1038. [Google Scholar] [CrossRef]
- Ørntoft, M.-B.W.; Jensen, S.; Hansen, T.B.; Bramsen, J.B.; Andersen, C.L. Comparative analysis of 12 different kits for bisulfite conversion of circulating cell-free DNA. Epigenetics 2017, 12, 626–636. [Google Scholar] [CrossRef] [Green Version]
- Bundo, M.; Sunaga, F.; Ueda, J.; Kasai, K.; Kato, T.; Iwamoto, K. A systematic evaluation of whole genome amplification of bisulfite-modified DNA. Clin. Epigenetics 2012, 4, 22. [Google Scholar] [CrossRef] [Green Version]
- Cox, D.R.; Wong, B.K.L.; Lee, E.; Testro, A.; Muralidharan, V.; Dobrovic, A.; Goh, S.K. Evaluating DNA recovery efficiency following bisulphite modification from plasma samples submitted for cell-free DNA methylation analysis. Epigenetics 2022, 17, 1956–1960. [Google Scholar] [CrossRef]
- Devonshire, A.S.; Whale, A.S.; Gutteridge, A.; Jones, G.; Cowen, S.; Foy, C.A.; Huggett, J. Towards standardisation of cell-free DNA measurement in plasma: Controls for extraction efficiency, fragment size bias and quantification. Anal. Bioanal. Chem. 2014, 406, 6499–6512. [Google Scholar] [CrossRef] [Green Version]
- Mikeska, T.; Candiloro, I.L.; Dobrovic, A. The implications of heterogeneous DNA methylation for the accurate quantification of methylation. Epigenomics 2010, 2, 561–573. [Google Scholar] [CrossRef] [Green Version]
- Edwards, R.L.; Takach, J.E.; McAndrew, M.J.; Menteer, J.; Lestz, R.M.; Whitman, D.; Baxter-Lowe, L.A. 216.17: Multiplex Digital PCR for the Detection of Donor-derived Cell-free DNA. Transplantation 2022, 106, S60. [Google Scholar] [CrossRef]
- Gaňová, M.; Zhang, H.; Zhu, H.; Korabečná, M.; Neužil, P. Multiplexed digital polymerase chain reaction as a powerful diagnostic tool. Biosens. Bioelectron. 2021, 181, 113155. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Sex | Age (Years) | Indication for LT | Associated HCC? | TCMR (Day) | Details | Other Significant Post-Operative Complications |
|---|---|---|---|---|---|---|---|
| 1 | F | 48 | Alcohol and A1AT deficiency cirrhosis | No | Yes (20) | Mild rejection RAI 3. | Nil |
| 2 | M | 30 | PSC cirrhosis | No | Yes (10) | Moderate-Severe rejection RAI 7-8. | Nil |
| 3 | M | 55 | Acutely Decompensated HBV cirrhosis | No | No | N/A | Nil |
| 4 | M | 54 | HCV cirrhosis + HCC | Yes | No | N/A | Return to operating theatre day 1 for suspected HAT. |
| 5 | M | 61 | HCV cirrhosis + HCC | Yes | No | N/A | Nil |
| 6 | M | 34 | PSC cirrhosis | No | No | Nil | Nil |
| 7 | M | 21 | PSC cirrhosis | No | Yes (8) | Moderate-Severe RAI 8/9. No concerning changes in LFTs until Day 7. Serendipitous rapid access to ultrasound guided biopsy. | Nil |
| gdcfDNA Results | Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | Patient 7 | |
|---|---|---|---|---|---|---|---|---|
| Pre-operative sample | DIPs | n/a | n/a | n/a | n/a | n/a | n/a | n/a |
| Meth | 7 | 519 | 75 | 40 | 37 | 126 | 22 | |
| Meth% | 0.2 | 31 | 1 | 1 | 4 | 12 | 3 | |
| Day 1 post-op | DIPs | 92,538 | 4964 | - | - | 35,578 | 8498 | 31,350 |
| Meth | 8422 | 1100 | 4133 | 12,719 | 6073 | 871 | 3231 | |
| Meth% | 80 | 41 | 296 | 508 | 300 | 50 | 111 | |
| Day 3 post-op | DIPs | 2901 | 3561 | 180 | 39,050 | 815 | 1084 | 10,106 |
| Meth | 371 | 1186 | 546 | 2795 | 146 | 115 | 536 | |
| Meth% | 24 | 114 | 38 | 51 | 21 | 21 | 44 | |
| Day 5 post-op | DIPs | 2846 | 8580 | - | 14,988 | - | - | 11,921 |
| Meth | 409 | 2228 | - | 811 | - | - | 426 | |
| Meth% | 17 | 28 | - | 8 | - | - | 19 | |
| Day 7 post-op | DIPs | 349 | 13,599 | 105 | 6518 | 442 | 1062 | 6779 |
| Meth | 52 | 3919 | 403 | 945 | 24 | 166 | 334 | |
| Meth% | 4 | 72 | 24 | 16 | 3 | 24 | 48 | |
| Day 14 post-op | DIPs | 14,575 | 4070 | 6 | 1416 | 208 | 165 | 14,300 |
| Meth | 1399 | 619 | 68 | 146 | 41 | 16 | 870 | |
| Meth% | 19 | 51 | 3 | 2 | 9 | 3 | 44 | |
| Day 28 post-op | DIPs | 3589 | - | 2 | 330 | 132 | 214 | - |
| Meth | 402 | - | 10 | 66 | 18 | 38 | - | |
| Meth% | 27 | - | 2 | 4 | 4 | 4 | - | |
| Day 42 post-op | DIPs | - | - | 10 | - | 329 | 103 | - |
| Meth | - | - | 37 | - | 23 | 5 | - | |
| Meth% | - | - | 6 | - | 7 | 1 | - | |
| Day 56 post-op | DIPs | - | - | - | 188 | - | - | - |
| Meth | - | - | - | 20 | - | - | - | |
| Meth% | - | - | - | 2 | - | - | - | |
| Day 112 post-op | DIPs | - | 418 | - | - | - | - | - |
| Meth | - | 141 | - | - | - | - | - | |
| Meth% | - | 12 | - | - | - | - | - | |
| Day 168 post-op | DIPs | - | 404 | - | - | - | - | - |
| Meth | - | 84 | - | - | - | - | - | |
| Meth% | - | 10 | - | - | - | - | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cox, D.R.A.; McClure, T.; Zhang, F.; Wong, B.K.L.; Testro, A.; Goh, S.K.; Muralidharan, V.; Dobrovic, A. Graft-Derived Cell-Free DNA Quantification following Liver Transplantation Using Tissue-Specific DNA Methylation and Donor-Specific Genotyping Techniques: An Orthogonal Comparison Study. Epigenomes 2023, 7, 11. https://doi.org/10.3390/epigenomes7020011
Cox DRA, McClure T, Zhang F, Wong BKL, Testro A, Goh SK, Muralidharan V, Dobrovic A. Graft-Derived Cell-Free DNA Quantification following Liver Transplantation Using Tissue-Specific DNA Methylation and Donor-Specific Genotyping Techniques: An Orthogonal Comparison Study. Epigenomes. 2023; 7(2):11. https://doi.org/10.3390/epigenomes7020011
Chicago/Turabian StyleCox, Daniel R. A., Tess McClure, Fan Zhang, Boris Ka Leong Wong, Adam Testro, Su Kah Goh, Vijayaragavan Muralidharan, and Alexander Dobrovic. 2023. "Graft-Derived Cell-Free DNA Quantification following Liver Transplantation Using Tissue-Specific DNA Methylation and Donor-Specific Genotyping Techniques: An Orthogonal Comparison Study" Epigenomes 7, no. 2: 11. https://doi.org/10.3390/epigenomes7020011