
Neurogenetic and Epigenetic Aspects of Cannabinoids
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Neurogenetic and Epigenetic Aspects of Cannabinoids

{kind=link}
| Genes | Summary Findings | Reference | |
|---|---|---|---|
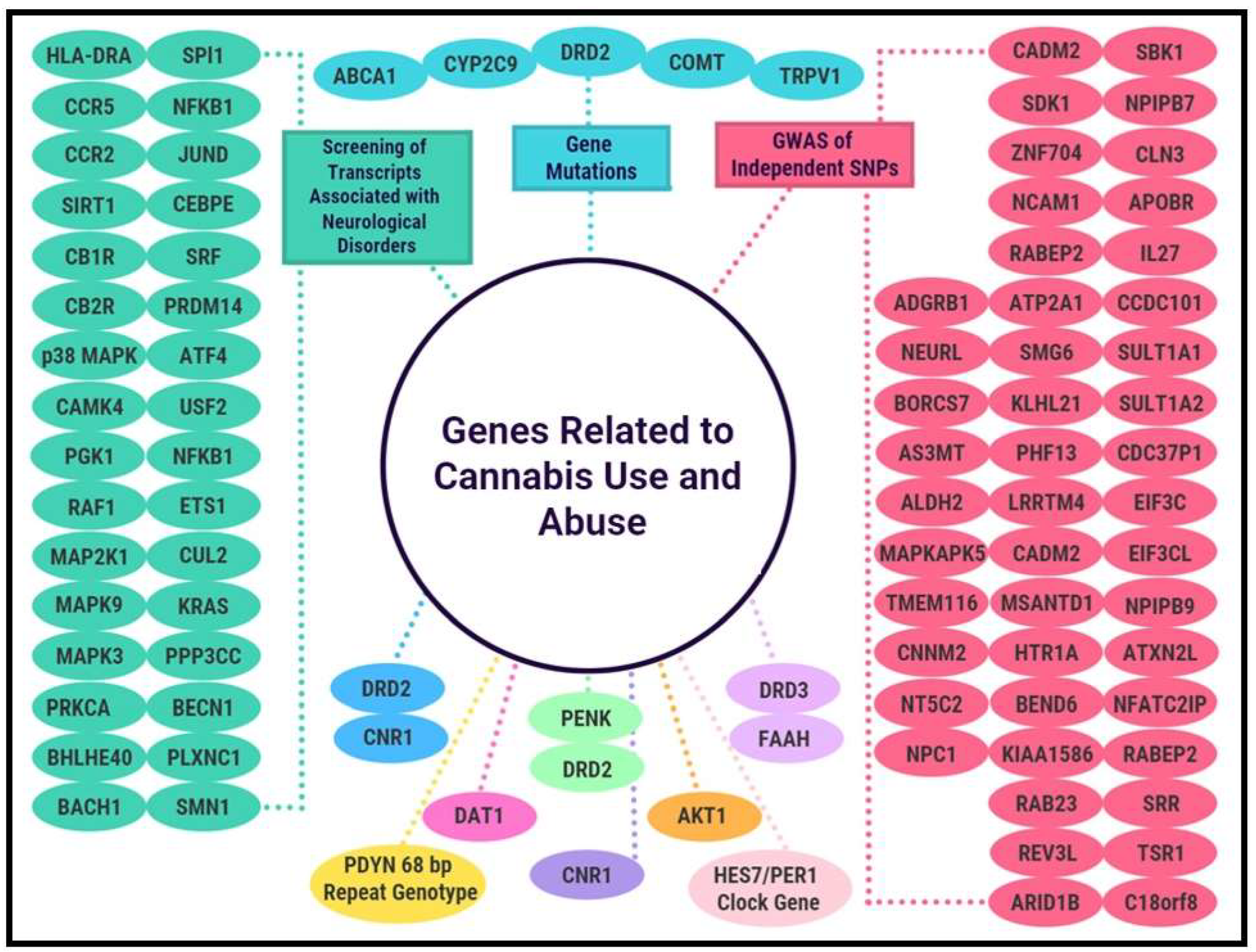
| COMT TRPV1 CYP2C9 DRD2 ABCA1 | Findings in patients included mutations in genes COMT {odds ratio, 12 (95% confidence limit [CL], 1.3–88.1) p = 0.012}, transient receptor potential vanilloid receptor 1 (TRPV1) (odds ratio, 5.8 [95% CL, 1.2–28.4] p = 0.015), CYP2C9 (odds ratio, 7.8 [95% CL, 1.1–70.1] p = 0.043), gene coding dopamine-2 receptor (DRD2) (odds ratio, 6.2 [95% CL, 1.1–34.7] p = 0.031), and ATP-binding cassette transporter gene (ABCA1) (odds ratio, 8.4 [95% CL, 1.5–48.1] p = 0.012). | [58] | |
| HLA-DRA CCR5 CCR2 SIRT1 CB1R CB2R p38 MAPK CAMK4 PGK1 RAF1 MAP2K1 MAPK9 MAPK3 PRKCA BHLHE40 BACH1 | SPl1 NFKB1 JUND CEBPE SRF PRDM14 ATF4 USF2 NFKB1 ETS1 CUL2 KRAS PPP3CC BECN1 PLXNC1 SMN1 | The screening of a large number of transcripts associated with neurological disorders has shown that the effects of cannabis differed drastically between HIV− and HIV+ groups, particularly in gene networks playing a role in inflammation, neurodegeneration, apoptosis, and leukocyte adhesion and transmigration. The results indicate that cannabis, in the context of HIV, may have beneficial effects. However, in individual genes, the authors identified detrimental effects that were associated with polysubstance use as a covariate, particularly methamphetamine. | [59] |
| CADM2 SDK1 ZNF704 NCAM1 RABEP2 ATP2A1 SMG6 KLHL21 PHF13 LRRTM4 CADM2 MSANTD1 HTR1A BEND6 KIAA1586 RAB23 REV3L ARID1B ADGRB1 NEURL BORCS7 AS3MT ALDH2 | SBK1 NPIPB7 CLN3 APOBR IL27 CCDC101 SULT1A1 SULT1A2 CDC37P1 EIF3C EIF3CL NPIPB9 ATXN2L NFATC2IP RABEP2 SRR TSR1 C18orf8 NPC1 TMEM116 CNNM2 NT5C2 MAPKAPK5 | GWAS association results of independent SNPs that are significantly associated with lifetime cannabis use. | [60] |
| DAT1 | These findings suggest that cannabis exposure alters the normal relationship between DAT1 polymorphism and the anatomy of total and subregional hippocampal volumes and that specific hippocampal subregions may be particularly affected. | [36] | |
| HES7/PER1 Clock gene | HES7/PER1 on chromosome 17 may represent a meaningful risk factor in the development of cannabis dependence and its severity. | [61] | |
| DRD2 CNR1 | Results indicate that the increased phenotype of cases requires an individual to be either heterozygous at both loci or homozygous at locus B with homozygous risk factor A1A1 present. We hypothesize that overlapping expressions of CNR1 and DRD2 are the causes of CNR1-DRD2 interactions in cases of substance abuse, and the different polymorphisms of CNR1 and DRD2 genes may have decisive roles in the nature of these interactions in terms of promoting or alleviating the cannabis addiction risk factor of the individual. | [33,34] | |
| AKT1 | Genetic variation in AKT1 may mediate both short-term as well as longer-term effects on psychosis expression associated with the use of cannabis, possibly through a mechanism of cannabinoid-regulated AKT1/GSK-3 signaling downstream of the DRD2 receptor. | [62] | |
| DRD2 PENK | The findings replicated the known association between the rs6277 DRD2 SNP and decisions associated with negative reinforcement outcomes. Moreover, PENK variants (rs2576573 and rs2609997) were significantly related to neuroticism and cannabis dependence. | [63] | |
| FAAH DRD3 | The association of reduced FAAH function with higher dopamine D3 receptors (DRD3) in human and mouse brains provides a mechanistic link between two brain systems that have been implicated in addiction-risk, especially cannabis. | [64] | |
| PDYN 68 bp repeat genotype | This study provides the first data on how the PDYN 68 bp genotype is associated with gender-specific patterns of exposure to cannabis. | [65] | |
| CNR1 | The results are consistent with the role of cannabinoid receptors in the modulation of dopamine and cannabinoid reward pathways. | [66] | |
3. Treatment of CUD
4. Use of Cannabis in Medical Therapies
5. Barriers to Cannabis Research
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cannabis. Who. Int. Available online: https://www.who.int/teams/mental-health-and-substance-use/alcohol-drugs-and-addictive-behaviours/drugs-psychoactive/cannabis (accessed on 7 June 2022).
- United Nations: Office on Drugs and Crime. World Drug Report 2021 (Booklet 2); United Nations: New York, NY, USA, 2021. [Google Scholar]
- Key Substance Use and Mental Health Indicators in the United States: Results from the 2020 National Survey on Drug Use and Health. Samhsa. gov. 2021. Available online: https://www.samhsa.gov/data/sites/default/files/reports/rpt35325/NSDUHFFRPDFWHTMLFiles2020/2020NSDUHFFR1PDFW102121.pdf (accessed on 13 June 2022).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR (TM)); American Psychiatric Association Publishing: Arlington, TX, USA, 2022. [Google Scholar]
- Abrams, D.I. The therapeutic effects of Cannabis and cannabinoids: An update from the National Academies of Sciences, Engineering and Medicine report. Eur. J. Intern. Med. 2018, 49, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Hill, K.P.; Gold, M.S.; Nemeroff, C.B.; McDonald, W.; Grzenda, A.; Widge, A.S.; Rodriguez, C.; Kraguljac, N.V.; Krystal, J.H.; Carpenter, L.L. Risks and Benefits of Cannabis and Cannabinoids in Psychiatry. Am. J. Psychiatry 2022, 179, 98–109. [Google Scholar] [CrossRef]
- Figura, M.; Koziorowski, D.; Sławek, J. Cannabis in Parkinson’s Disease—The patient’s perspective versus clinical trials: A systematic literature review. Neurol. Neurochir. Pol. 2022, 56, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Koppel, B.S.; Brust, J.C.; Fife, T.; Bronstein, J.; Youssof, S.; Gronseth, G.; Gloss, D. Systematic review: Efficacy and safety of medical marijuana in selected neurologic disorders: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2014, 82, 1556–1563. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.; See, Y.M.; Lee, J. A Systematic Review of the Effectiveness of Medical Cannabis for Psychiatric, Movement and Neurodegenerative Disorders. Clin. Psychopharmacol. Neurosci. 2017, 15, 301–312. [Google Scholar] [CrossRef]
- Nugent, S.M.; Morasco, B.J.; O’Neil, M.E.; Freeman, M.; Low, A.; Kondo, K.; Elven, C.; Zakher, B.; Motu’Apuaka, M.; Paynter, R.; et al. The Effects of Cannabis among Adults with Chronic Pain and an Overview of General Harms. Ann. Intern. Med. 2017, 167, 319–331. [Google Scholar] [CrossRef]
- Bennici, A.; Mannucci, C.; Calapai, F.; Cardia, L.; Ammendolia, I.; Gangemi, S.; Calapai, G.; Soler, D.G. Safety of Medical Cannabis in Neuropathic Chronic Pain Management. Molecules 2021, 26, 6257. [Google Scholar] [CrossRef]
- Tafelski, S.; Häuser, W.; Schäfer, M. Efficacy, tolerability, and safety of cannabinoids for chemotherapy-induced nausea and vomiting—A systematic review of systematic reviews. Der. Schmerz 2016, 30, 14–24. [Google Scholar] [CrossRef]
- Silins, E.; Horwood, L.J.; Patton, G.C.; Fergusson, D.M.; Olsson, C.A.; Hutchinson, D.M.; Spry, E.; Toumbourou, J.W.; Degenhardt, L.; Swift, W.; et al. Young adult sequelae of adolescent cannabis use: An integrative analysis. Lancet Psychiatry 2014, 1, 286–293. [Google Scholar] [CrossRef]
- Volkow, N.D.; Baler, R.D.; Compton, W.M.; Weiss, S.R. Adverse Health Effects of Marijuana Use. N. Engl. J. Med. 2014, 370, 2219–2227. [Google Scholar] [CrossRef] [Green Version]
- Karila, L.; Roux, P.; Rolland, B.; Benyamina, A.; Reynaud, M.; Aubin, H.-J.; Lancon, C. Acute and Long-Term Effects of Cannabis Use: A Review. Curr. Pharm. Des. 2014, 20, 4112–4118. [Google Scholar] [CrossRef]
- Crean, R.D.; Crane, N.; Mason, B.J. An Evidence-Based Review of Acute and Long-Term Effects of Cannabis Use on Executive Cognitive Functions. J. Addict. Med. 2011, 5, 1–8. [Google Scholar] [CrossRef]
- Ryan, S.A.; Ammerman, S.D.; O’Connor, M.E.; Gonzalez, L.; Patrick, S.W.; Quigley, J.; Walker, L.R.; Meek, J.Y.; Johnston, M.; Stellwagen, L.; et al. Marijuana Use During Pregnancy and Breastfeeding: Implications for Neonatal and Childhood Outcomes. Pediatrics 2018, 142, e20181889. [Google Scholar] [CrossRef]
- Campolongo, P.; Trezza, V.; Cassano, T.; Gaetani, S.; Morgese, M.G.; Ubaldi, M.; Soverchia, L.; Antonelli, T.; Ferraro, L.; Massi, M.; et al. Perinatal exposure to delta-9-tetrahydrocannabinol causes enduring cognitive deficits associated with alteration of cortical gene expression and neurotransmission in rats. Addict. Biol. 2007, 12, 485–495. [Google Scholar] [CrossRef]
- Fergusson, D.M.; Boden, J. Cannabis use and later life outcomes. Addiction 2008, 103, 969–976. [Google Scholar] [CrossRef]
- Brook, J.S.; Lee, J.Y.; Finch, S.J.; Seltzer, N.; Brook, D.W. Adult Work Commitment, Financial Stability, and Social Environment as Related to Trajectories of Marijuana Use Beginning in Adolescence. Subst. Abus. 2013, 34, 298–305. [Google Scholar] [CrossRef]
- Blum, K.; Wood, R.C.; Braverman, E.R.; Chen, T.J.; Sheridan, P.J. The D2 dopamine receptor gene as a predictor of compulsive disease: Bayes’ theorem. Funct. Neurol. 1995, 10, 37–44. [Google Scholar]
- Blum, K.; McLaughlin, T.; Bowirrat, A.; Modestino, E.J.; Baron, D.; Gomez, L.L.; Ceccanti, M.; Braverman, E.R.; Thanos, P.K.; Cadet, J.L.; et al. Reward Deficiency Syndrome (RDS) Surprisingly Is Evolutionary and Found Everywhere: Is It “Blowin’ in the Wind”? J. Pers. Med. 2022, 12, 321. [Google Scholar] [CrossRef]
- Johnson, E.C.; Demontis, D.; Thorgeirsson, T.E.; Walters, R.K.; Polimanti, R.; Hatoum, A.S.; Sanchez-Roige, S.; Paul, S.E.; Wendt, F.R.; Clarke, T.-K.; et al. A large-scale genome-wide association study meta-analysis of cannabis use disorder. Lancet Psychiatry 2020, 7, 1032–1045. [Google Scholar] [CrossRef]
- Verweij, K.J.H.; Zietsch, B.; Lynskey, M.T.; Medland, S.; Neale, M.C.; Martin, N.; Boomsma, D.I.; Vink, J.M. Genetic and environmental influences on cannabis use initiation and problematic use: A meta-analysis of twin studies. Addiction 2010, 105, 417–430. [Google Scholar] [CrossRef]
- Hodgson, K.; Coleman, J.R.I.; Hagenaars, S.; Purves, K.L.; Glanville, K.; Choi, S.W.; O’Reilly, P.; Breen, G.; Lewis, C.M. Major Depressive Disorder Working Group of the Psychiatric Genomics Consortium Cannabis use, depression and self-harm: Phenotypic and genetic relationships. Addiction 2020, 115, 482–492. [Google Scholar] [CrossRef] [PubMed]
- Blum, K.; Gold, M.S.; Febo, M.; Baron, D.; Modestino, E.J.; Elman, I.; Badgaiyan, R.D. Molecular role of dopamine in anhedonia linked to reward deficiency syndrome RDS and anti-reward systems. Front. Biosci. 2018, 10, 309–325. [Google Scholar] [CrossRef] [PubMed]
- Blum, K.; Morgan, J.; Cadet, J.L.; Baron, D.; Carney, P.R.; Khalsa, J.; Badgaiyan, R.D.; Gold, M.S. Psychoactive Drugs Like Cannabis-Induce Hypodopaminergic Anhedonia and Neuropsychological Dysfunction in Humans: Putative Induction of Dopamine Homeostasis via Coupling of Genetic Addiction Risk Severity (GARS) testing and Precision Pro-dopamine Regulation (KB220). Neurology (E-Cronicon) 2021, 13, 86–92. [Google Scholar]
- Green, A.I.; Zimmet, S.V.; Straus, R.D.; Schildkraut, J.J. Clozapine for Comorbid Substance Use Disorder and Schizophrenia: Do Patients with Schizophrenia Have a Reward-Deficiency Syndrome That Can Be Ameliorated by Clozapine? Harv. Rev. Psychiatry 1999, 6, 287–296. [Google Scholar] [CrossRef]
- Johnson, E.C.; Hatoum, A.S.; Deak, J.D.; Polimanti, R.; Murray, R.M.; Edenberg, H.J.; Gelernter, J.; Di Forti, M.; Agrawal, A. The relationship between cannabis and schizophrenia: A genetically informed perspective. Addiction 2021, 116, 3227–3234. [Google Scholar] [CrossRef]
- Berman, M.O.; Blum, K.; Chen, T.J.; Braverman, E.R.; Waite, R.L.; Downs, B.W.; Arcuri, V.; Notaro, A.; Palomo, T.; Comings, D.E. Attention-deficit-hyperactivity disorder and reward deficiency syndrome. Neuropsychiatr. Dis. Treat. 2008, 4, 893–917. [Google Scholar] [CrossRef]
- Song, P.; Zha, M.; Yang, Q.; Zhang, Y.; Li, X.; Rudan, I. The prevalence of adult attention-deficit hyperactivity disorder: A global systematic review and meta-analysis. J. Glob. Health 2021, 11, 04009. [Google Scholar] [CrossRef]
- Artigas, M.S.; Sánchez-Mora, C.; Rovira, P.; Richarte, V.; Martínez, I.G.; Pagerols, M.; Demontis, D.; Stringer, S.; Vink, J.M.; Børglum, A.D.; et al. Attention-deficit/hyperactivity disorder and lifetime cannabis use: Genetic overlap and causality. Mol. Psychiatry 2019, 25, 2493–2503. [Google Scholar] [CrossRef]
- Isir, A.B.; Baransel, C.; Nacak, M. An Information Theoretical Study of the Epistasis between the CNR1 1359 G/A Polymorphism and the Taq1A and Taq1B DRD2 Polymorphisms: Assessing the Susceptibility to Cannabis Addiction in a Turkish Population. J. Mol. Neurosci. 2016, 58, 456–460. [Google Scholar] [CrossRef]
- Blum, K.; Noble, E.; Sheridan, P.; Montgomery, A.; Ritchie, T.; Ozkaragoz, T.; Fitch, R.; Wood, R.; Finley, O.; Sadlack, F. Genetic predisposition in alcoholism: Association of the D2 dopamine receptor TaqI B1 RFLP with severe alcoholics. Alcohol 1993, 10, 59–67. [Google Scholar] [CrossRef]
- Ermis, A.; Erkiran, M.; Dasdemir, S.; Turkcan, A.S.; Ceylan, M.E.; Bireller, E.S.; Cakmakoglu, B. The relationship between catechol-O-methyltransferase gene Val158Met (COMT) polymorphism and premorbid cannabis use in Turkish male patients with schizophrenia. Vivo 2015, 29, 129–132. [Google Scholar]
- Batalla, A.; Lorenzetti, V.; Chye, Y.; Yücel, M.; Soriano-Mas, C.; Bhattacharyya, S.; Torrens, M.; Crippa, J.A.; Martín-Santos, R. The Influence of DAT1, COMT, and BDNF Genetic Polymorphisms on Total and Subregional Hippocampal Volumes in Early Onset Heavy Cannabis Users. Cannabis Cannabinoid Res. 2018, 3, 1–10. [Google Scholar] [CrossRef]
- Gerra, M.C.; Manfredini, M.; Cortese, E.; Antonioni, M.C.; Leonardi, C.; Magnelli, F.; Somaini, L.; Jayanthi, S.; Cadet, J.L.; Donnini, C. Genetic and Environmental Risk Factors for Cannabis Use: Preliminary Results for the Role of Parental Care Perception. Subst. Use Misuse 2019, 54, 670–680. [Google Scholar] [CrossRef]
- Grzywacz, A.; Chmielowiec, J.; Chmielowiec, K.; Mroczek, B.; Masiak, J.; Suchanecka, A.; Sipak-Szmigiel, O.; Szumilas, K.; Trybek, G. The Ankyrin Repeat and Kinase Domain Containing 1 Gene Polymorphism (ANKK1 Taq1A) and Personality Traits in Addicted Subjects. Int. J. Environ. Res. Public Health 2019, 16, 2687. [Google Scholar] [CrossRef]
- Neville, M.J.; Johnstone, E.C.; Walton, R. Identification and characterization of ANKK1: A novel kinase gene closely linked to DRD2 on chromosome band 11q23.1. Hum. Mutat. 2004, 23, 540–545. [Google Scholar] [CrossRef]
- Adedeji, O.H.; Akinniyi, O.A.; Abiola, M.O.; Abayomi, O.M. Association of dopamine receptor D2 Taq I A polymorphism and cannabis use disorder in Lagos, Nigeria. Psych J. 2014, 3, 93–100. [Google Scholar] [CrossRef]
- Comings, D.E.; MacMurray, J.P. Molecular Heterosis: A Review. Mol. Genet. Metab. 2000, 71, 19–31. [Google Scholar] [CrossRef]
- Noble, E.P. Allelic Association of the D2 Dopamine Receptor Gene with Receptor-Binding Characteristics in Alcoholism or Gene ism. Arch. Gen. Psychiatry 1991, 48, 648–654. [Google Scholar] [CrossRef]
- Schacht, J.P.; Selling, R.E.; Hutchison, K.E. Intermediate cannabis dependence phenotypes and the FAAH C385A variant: An exploratory analysis. Psychopharmacology 2008, 203, 511–517. [Google Scholar] [CrossRef]
- Smith, A.; Kaufman, F.; Sandy, M.S.; Cardenas, A. Cannabis Exposure During Critical Windows of Development: Epigenetic and Molecular Pathways Implicated in Neuropsychiatric Disease. Curr. Environ. Health Rep. 2020, 7, 325–342. [Google Scholar] [CrossRef]
- Goldschmidt, L.; Day, N.L.; Richardson, G.A. Effects of prenatal marijuana exposure on child behavior problems at age 10. Neurotoxicol. Teratol. 2000, 22, 325–336. [Google Scholar] [CrossRef]
- Goldschmidt, L.; Richardson, G.A.; Willford, J.A.; Severtson, S.G.; Day, N.L. School achievement in 14-year-old youths prenatally exposed to marijuana. Neurotoxicol. Teratol. 2012, 34, 161–167. [Google Scholar] [CrossRef]
- Noland, J.S.; Singer, L.; Short, E.J.; Minnes, S.; Arendt, R.E.; Kirchner, H.L.; Bearer, C. Prenatal drug exposure and selective attention in preschoolers. Neurotoxicol. Teratol. 2005, 27, 429–438. [Google Scholar] [CrossRef]
- Leech, S.L.; Larkby, C.A.; Day, R.; Day, N.L. Predictors and Correlates of High Levels of Depression and Anxiety Symptoms among Children at Age 10. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 223–230. [Google Scholar] [CrossRef]
- Conner, S.N.; Bedell, V.; Lipsey, K.; Macones, G.A.; Cahill, A.G.; Tuuli, M.G. Maternal Marijuana Use and Adverse Neonatal Outcomes. Obstet. Gynecol. 2016, 128, 713–723. [Google Scholar] [CrossRef]
- Leemaqz, S.Y.; Dekker, G.A.; McCowan, L.M.; Kenny, L.C.; Myers, J.E.; Simpson, N.A.; Poston, L.; Roberts, C.T. Maternal marijuana use has independent effects on risk for spontaneous preterm birth but not other common late pregnancy complications. Reprod. Toxicol. 2016, 62, 77–86. [Google Scholar] [CrossRef]
- Jaques, S.C.; Kingsbury, A.M.; Henshcke, P.; Chomchai, C.; Clews, S.; Falconer, J.; Abdel-Latif, M.E.; Feller, J.M.; Oei, J.L. Cannabis, the pregnant woman and her child: Weeding out the myths. J. Perinatol. 2014, 34, 417–424. [Google Scholar] [CrossRef]
- Vargish, G.A.; Pelkey, K.A.; Yuan, X.; Chittajallu, R.; Collins, D.; Fang, C.; McBain, C.J. Persistent inhibitory circuit defects and disrupted social behaviour following in utero exogenous cannabinoid exposure. Mol. Psychiatry 2017, 22, 56–67. [Google Scholar] [CrossRef]
- Melas, P.; Scherma, M.; Fratta, W.; Cifani, C.; Fadda, P. Cannabidiol as a Potential Treatment for Anxiety and Mood Disorders: Molecular Targets and Epigenetic Insights from Preclinical Research. Int. J. Mol. Sci. 2021, 22, 1863. [Google Scholar] [CrossRef]
- DiNieri, J.A.; Wang, X.; Szutorisz, H.; Spano, S.M.; Kaur, J.; Casaccia, P.; Dow-Edwards, D.; Hurd, Y.L. Maternal Cannabis Use Alters Ventral Striatal Dopamine D2 Gene Regulation in the Offspring. Biol. Psychiatry 2011, 70, 763–769. Available online: https://www.biologicalpsychiatryjournal.com/article/S0006-3223(11)00672-X/fulltext (accessed on 4 August 2022). [CrossRef] [PubMed]
- Hurd, Y.L.; Manzoni, O.J.; Pletnikov, M.V.; Lee, F.S.; Bhattacharyya, S.; Melis, M. Cannabis and the Developing Brain: Insights into Its Long-Lasting Effects. J. Neurosci. 2019, 39, 8250–8258. [Google Scholar] [CrossRef] [PubMed]
- Oyaci, Y.; Aytac, H.M.; Pasin, O.; Aydin, P.C.; Pehlivan, S. Detection of altered methylation of MB-COMT promotor and DRD2 gene in cannabinoid or synthetic cannabinoid use disorder regarding gene variants and clinical parameters. J. Addict. Dis. 2021, 39, 526–536. [Google Scholar] [CrossRef] [PubMed]
- Burgdorf, C.E.; Jing, D.; Yang, R.; Huang, C.; Hill, M.N.; Mackie, K.; Milner, T.A.; Pickel, V.M.; Lee, F.S.; Rajadhyaksha, A.M. Endocannabinoid genetic variation enhances vulnerability to THC reward in adolescent female mice. Sci. Adv. 2020, 6, eaay1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russo, E.B.; Spooner, C.; May, L.; Leslie, R.; Whiteley, V.L. Cannabinoid Hyperemesis Syndrome Survey and Genomic Investigation. Cannabis Cannabinoid Res. 2022, 7, 336–344. [Google Scholar] [CrossRef]
- Basova, L.V.; Lukkes, S.E.; Milner, R.; Ellis, R.J.; Cherner, M.; Iudicello, J.; Marcondes, M.C.G. Polygenic networks in peripheral leukocytes indicate patterns associated with HIV infection and context-dependent effects of cannabis use. Brain Behav. Immun.-Health 2022, 20, 100414. [Google Scholar] [CrossRef]
- Pasman, J.A.; Verweij, K.J.H.; Gerring, Z.; Stringer, S.; Sanchez-Roige, S.; Treur, J.L.; Abdellaoui, A.; Nivard, M.G.; Baselmans, B.M.L.; Ong, J.-S.; et al. GWAS of lifetime cannabis use reveals new risk loci, genetic overlap with psychiatric traits, and a causal effect of schizophrenia liability. Nat. Neurosci. 2018, 21, 1161–1170. [Google Scholar] [CrossRef]
- Saffroy, R.; Lafaye, G.; Desterke, C.; Ortiz-Tudela, E.; Amirouche, A.; Innominato, P.; Pham, P.; Benyamina, A.; Lemoine, A. Several clock genes polymorphisms are meaningful risk factors in the development and severity of cannabis addiction. Chrono. Int. 2019, 36, 122–134. [Google Scholar] [CrossRef]
- Van Winkel, R. Family-Based Analysis of Genetic Variation Underlying Psychosis-Inducing Effects of CannabisSibling Analysis and Proband Follow-upGenetic Variation Underlying Cannabis Effects. Arch. Gen. Psychiatry 2011, 68, 148–157. [Google Scholar] [CrossRef]
- Jutras-Aswad, D.; Jacobs, M.M.; Yiannoulos, G.; Roussos, P.; Bitsios, P.; Nomura, Y.; Liu, X.; Hurd, Y.L. Cannabis-Dependence Risk Relates to Synergism between Neuroticism and Proenkephalin SNPs Associated with Amygdala Gene Expression: Case-Control Study. PLoS ONE 2012, 7, e39243. [Google Scholar] [CrossRef]
- Mansouri, E.; Nobrega, J.N.; Hill, M.N.; Tyndale, R.F.; Lee, F.S.; Hendershot, C.S.; Best, L.M.; Di Ciano, P.; Balsevich, G.; Sloan, M.E.; et al. D3 dopamine receptors and a missense mutation of fatty acid amide hydrolase linked in mouse and men: Implication for addiction. Neuropsychopharmacology 2020, 45, 745–752. [Google Scholar] [CrossRef]
- Yuferov, V.; Butelman, E.R.; Kreek, M.J. Gender-specific association of functional prodynorphin 68 bp repeats with cannabis exposure in an African American cohort. Neuropsychiatr. Dis. Treat. 2018, 14, 1025–1034. [Google Scholar] [CrossRef] [PubMed]
- Comings, D.E.; Muhleman, D.; Gade, R.; Johnson, P.; Verde, R.; Saucier, G.; MacMurray, J. Cannabinoid receptor gene (CNR1): Association with IV drug use. Mol. Psychiatry 1997, 2, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Stephens, R.S.; Walker, R.; DeMarce, J.; Lozano, B.E.; Rowland, J.; Walker, D.; Roffman, R.A. Treating cannabis use disorder: Exploring a treatment as needed model with 34-month follow-up. J. Subst. Abus. Treat. 2020, 117, 108088. [Google Scholar] [CrossRef] [PubMed]
- Schettino, J.; Leuschner, F.; Kasten, L.; Tossmann, P.; Hoch, E.; Ferri, M.; Guarita, B.; Simon, R. Treatment of Cannabis-Related Disorders in Europe. Europa.eu. 2015. Available online: https://www.emcdda.europa.eu/system/files/publications/1014/TDXD14017ENN.pdf (accessed on 13 June 2022).
- Calomarde-Gómez, C.; Jiménez-Fernández, B.; Balcells-Oliveró, M.; Gual, A.; López-Pelayo, H. Motivational Interviewing for Cannabis Use Disorders: A Systematic Review and Meta-Analysis. Eur. Addict. Res. 2021, 27, 413–427. [Google Scholar] [CrossRef]
- Gray, K.M.; Carpenter, M.J.; Baker, N.L.; DeSantis, S.M.; Kryway, E.; Hartwell, K.J.; McRae-Clark, A.L.; Brady, K.T. A Double-Blind Randomized Controlled Trial of N-Acetylcysteine in Cannabis-Dependent Adolescents. Am. J. Psychiatry 2012, 169, 805–812. [Google Scholar] [CrossRef]
- Mason, B.J.; Crean, R.; Goodell, V.; Light, J.M.; Quello, S.; Shadan, F.; Buffkins, K.; Kyle, M.; Adusumalli, M.; Begovic, A.; et al. A Proof-of-Concept Randomized Controlled Study of Gabapentin: Effects on Cannabis Use, Withdrawal and Executive Function Deficits in Cannabis-Dependent Adults. Neuropsychopharmacology 2012, 37, 1689–1698. [Google Scholar] [CrossRef]
- Lintzeris, N.; Bhardwaj, A.; Mills, L.; Dunlop, A.; Copeland, J.; Mcgregor, I.; Bruno, R.; Gugusheff, J.; Phung, N.; Montebello, M.; et al. Nabiximols for the Treatment of Cannabis Dependence. JAMA Intern. Med. 2019, 179, 1242–1253. [Google Scholar] [CrossRef]
- Lintzeris, N.; Mills, L.; Dunlop, A.; Copeland, J.; Mcgregor, I.; Bruno, R.; Kirby, A.; Montebello, M.; Hall, M.; Jefferies, M.; et al. Cannabis use in patients 3 months after ceasing nabiximols for the treatment of cannabis dependence: Results from a placebo-controlled randomised trial. Drug Alcohol Depend. 2020, 215, 108220. [Google Scholar] [CrossRef]
- Freeman, T.P.; Hindocha, C.; Baio, G.; Shaban, N.D.C.; Thomas, E.M.; Astbury, D.; Freeman, A.M.; Lees, R.; Craft, S.; Morrison, P.D.; et al. Cannabidiol for the treatment of cannabis use disorder: A phase 2a, double-blind, placebo-controlled, randomised, adaptive Bayesian trial. Lancet Psychiatry 2020, 7, 865–874. [Google Scholar] [CrossRef]
- McRae-Clark, A.L.; Gray, K.M.; Baker, N.L.; Sherman, B.J.; Squeglia, L.; Sahlem, G.L.; Wagner, A.; Tomko, R. Varenicline as a treatment for cannabis use disorder: A placebo-controlled pilot trial. Drug Alcohol Depend. 2021, 229, 109111. [Google Scholar] [CrossRef]
- Gray, K.M.; Sonne, S.C.; McClure, E.A.; Ghitza, U.E.; Matthews, A.G.; McRae-Clark, A.L.; Carroll, K.M.; Potter, J.S.; Wiest, K.; Mooney, L.J.; et al. A randomized placebo-controlled trial of N-acetylcysteine for cannabis use disorder in adults. Drug Alcohol Depend. 2017, 177, 249–257. [Google Scholar] [CrossRef]
- Trigo, J.M.; Soliman, A.; Quilty, L.C.; Fischer, B.; Rehm, J.; Selby, P.; Barnes, A.J.; Huestis, M.A.; George, T.P.; Streiner, D.L.; et al. Nabiximols combined with motivational enhancement/cognitive behavioral therapy for the treatment of cannabis dependence: A pilot randomized clinical trial. PLoS ONE 2018, 13, e0190768. [Google Scholar] [CrossRef]
- Bahji, A.; Meyyappan, A.C.; Hawken, E.R.; Tibbo, P.G. Pharmacotherapies for cannabis use disorder: A systematic review and network meta-analysis. Int. J. Drug Policy 2021, 97, 103295. [Google Scholar] [CrossRef]
- Pagano, C.; Navarra, G.; Coppola, L.; Avilia, G.; Bifulco, M.; Laezza, C. Cannabinoids: Therapeutic Use in Clinical Practice. Int. J. Mol. Sci. 2022, 23, 3344. [Google Scholar] [CrossRef]
- Legare, C.A.; Raup-Konsavage, W.M.; Vrana, K.E. Therapeutic Potential of Cannabis, Cannabidiol, and Cannabinoid-Based Pharmaceuticals. Pharmacology 2022, 107, 131–149. [Google Scholar] [CrossRef]
- Ben Amar, M. Cannabinoids in medicine: A review of their therapeutic potential. J. Ethnopharmacol. 2006, 105, 1–25. [Google Scholar] [CrossRef]
- Rong, C.; Lee, Y.; Carmona, N.E.; Cha, D.S.; Ragguett, R.-M.; Rosenblat, J.D.; Mansur, R.B.; Ho, R.C.; McIntyre, R.S. Cannabidiol in medical marijuana: Research vistas and potential opportunities. Pharmacol. Res. 2017, 121, 213–218. [Google Scholar] [CrossRef]
- Pisanti, S.; Malfitano, A.M.; Ciaglia, E.; Lamberti, A.; Ranieri, R.; Cuomo, G.; Abate, M.; Faggiana, G.; Proto, M.C.; Fiore, D.; et al. Cannabidiol: State of the art and new challenges for therapeutic applications. Pharmacol. Ther. 2017, 175, 133–150. [Google Scholar] [CrossRef]
- Chayasirisobhon, S. Cannabis and Neuropsychiatric Disorders: An Updated Review. Acta Neurol. Taiwan 2019, 28, 27–39. [Google Scholar]
- Chayasirisobhon, S. The Role of Cannabidiol in Neurological Disorders. Perm. J. 2021, 25, 1. [Google Scholar] [CrossRef]
- Parker, L.A.; Rock, E.M.; Limebeer, C.L. Regulation of nausea and vomiting by cannabinoids. J. Cereb. Blood Flow Metab. 2011, 163, 1411–1422. [Google Scholar] [CrossRef]
- Grimison, P.; Mersiades, A.; Kirby, A.; Lintzeris, N.; Morton, R.; Haber, P.; Olver, I.; Walsh, A.; McGregor, I.; Cheung, Y.; et al. Oral THC:CBD cannabis extract for refractory chemotherapy-induced nausea and vomiting: A randomised, placebo-controlled, phase II crossover trial. Ann. Oncol. 2020, 31, 1553–1560. [Google Scholar] [CrossRef]
- Simon, L.; Baldwin, C.; Kalea, A.Z.; Slee, A. Cannabinoid interventions for improving cachexia outcomes in cancer: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2022, 13, 23–41. [Google Scholar] [CrossRef]
- Breijyeh, Z.; Jubeh, B.; Bufo, S.; Karaman, R.; Scrano, L. Cannabis: A Toxin-Producing Plant with Potential Therapeutic Uses. Toxins 2021, 13, 117. [Google Scholar] [CrossRef]
- Kondrad, E.C.; Reed, A.J.; Simpson, M.J.; Nease, N.E. Lack of Communication about Medical Marijuana Use between Doctors and Their Patients. J. Am. Board Fam. Med. 2018, 31, 805–808. [Google Scholar] [CrossRef]
- Choi, N.G.; DiNitto, D.M.; Marti, C.N. Nonmedical versus medical marijuana use among three age groups of adults: Associations with mental and physical health status. Am. J. Addict. 2017, 26, 697–706. [Google Scholar] [CrossRef]
- Kim, J.; Coors, M.E.; Young, S.E.; Raymond, K.M.; Hopfer, C.J.; Wall, T.L.; Corley, R.P.; Brown, S.A.; Sakai, J.T. Cannabis use disorder and male sex predict medical cannabis card status in a sample of high risk adolescents. Drug Alcohol Depend. 2018, 183, 25–33. [Google Scholar] [CrossRef]
- Kahan, M.; Srivastava, A.; Clarke, S. Cannabis industry and medical cannabis clinics need regulation. Can. Fam. Physi. 2019, 65, 864–868. [Google Scholar]
- Chiu, V.; Leung, J.; Hall, W.; Stjepanović, D.; Degenhardt, L. Public health impacts to date of the legalisation of medical and recreational cannabis use in the USA. Neuropharmacology 2021, 193, 108610. Available online: https://www.sciencedirect.com/science/article/pii/S0028390821001647 (accessed on 4 August 2022). [CrossRef]
- National Academies of Sciences, Engineering; and Medicine, Health and Medicine Division; Board on Population Health and Public Health Practice. Challenges and Barriers in Conducting Cannabis Research; National Academies Press: Washington, DC, USA, 2017. [Google Scholar]
- Cooper, Z.D.; Abrams, D.I.; Gust, S.; Salicrup, A.; Throckmorton, D.C. Challenges for Clinical Cannabis and Cannabinoid Research in the United States. J. Natl. Cancer Inst. Monogr. 2021, 2021, 114–122. Available online: https://academic.oup.com/jncimono/article/2021/58/114/6446199 (accessed on 4 August 2022). [CrossRef]
- Purcell, J.M.; Passley, T.M.; Leheste, J.R. The cannabidiol and marijuana research expansion act: Promotion of scientific knowledge to prevent a national health crisis. Lancet Reg. Health Am. 2022, 14, 100325. Available online: https://www.thelancet.com/journals/lanam/article/PIIS2667-193X(22)00142-9/fulltext (accessed on 4 August 2022). [CrossRef]
- Moss, M.K. Results—A Billion Dollars for Cannabis Research; Createspace Independent Publishing Platform: North Charleston, SC, USA, 2019; Available online: https://hellth.com/#/cannabis/initial-results (accessed on 4 August 2022).
- O’Grady, C. Cannabis research data reveals a focus on harms of the drug. Science 2020, 369, 1155. [Google Scholar] [CrossRef] [PubMed]
- Jaeger, K. Top Federal Drug Agency Wants to Create a National Medical Marijuana Registry to Track How Patients Use Cannabis. Marijuana Moment. 2022. Available online: https://www.marijuanamoment.net/top-federal-drug-agency-wants-to-create-a-national-medical-marijuana-registry-to-track-how-patients-use-cannabis/ (accessed on 4 August 2022).
- Moss, M.K. Results—Funding by Research Area; Createspace Independent Publishing Platform: North Charleston, SC, USA, 2019; Available online: https://hellth.com/#/cannabis/classification-results (accessed on 4 August 2022).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dennen, C.A.; Blum, K.; Bowirrat, A.; Khalsa, J.; Thanos, P.K.; Baron, D.; Badgaiyan, R.D.; Gupta, A.; Braverman, E.R.; Gold, M.S. Neurogenetic and Epigenetic Aspects of Cannabinoids. Epigenomes 2022, 6, 27. https://doi.org/10.3390/epigenomes6030027
Dennen CA, Blum K, Bowirrat A, Khalsa J, Thanos PK, Baron D, Badgaiyan RD, Gupta A, Braverman ER, Gold MS. Neurogenetic and Epigenetic Aspects of Cannabinoids. Epigenomes. 2022; 6(3):27. https://doi.org/10.3390/epigenomes6030027
Chicago/Turabian StyleDennen, Catherine A., Kenneth Blum, Abdalla Bowirrat, Jag Khalsa, Panayotis K. Thanos, David Baron, Rajendra D. Badgaiyan, Ashim Gupta, Eric R. Braverman, and Mark S. Gold. 2022. "Neurogenetic and Epigenetic Aspects of Cannabinoids" Epigenomes 6, no. 3: 27. https://doi.org/10.3390/epigenomes6030027