
Long-Term Exposure of Nitrogen Oxides Air Pollution (NO2) Impact for Coronary Artery Lesion Progression—Pilot Study
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Uni- and Multivariable Analysis for CAD Prediction in Patients’ Living in Cities
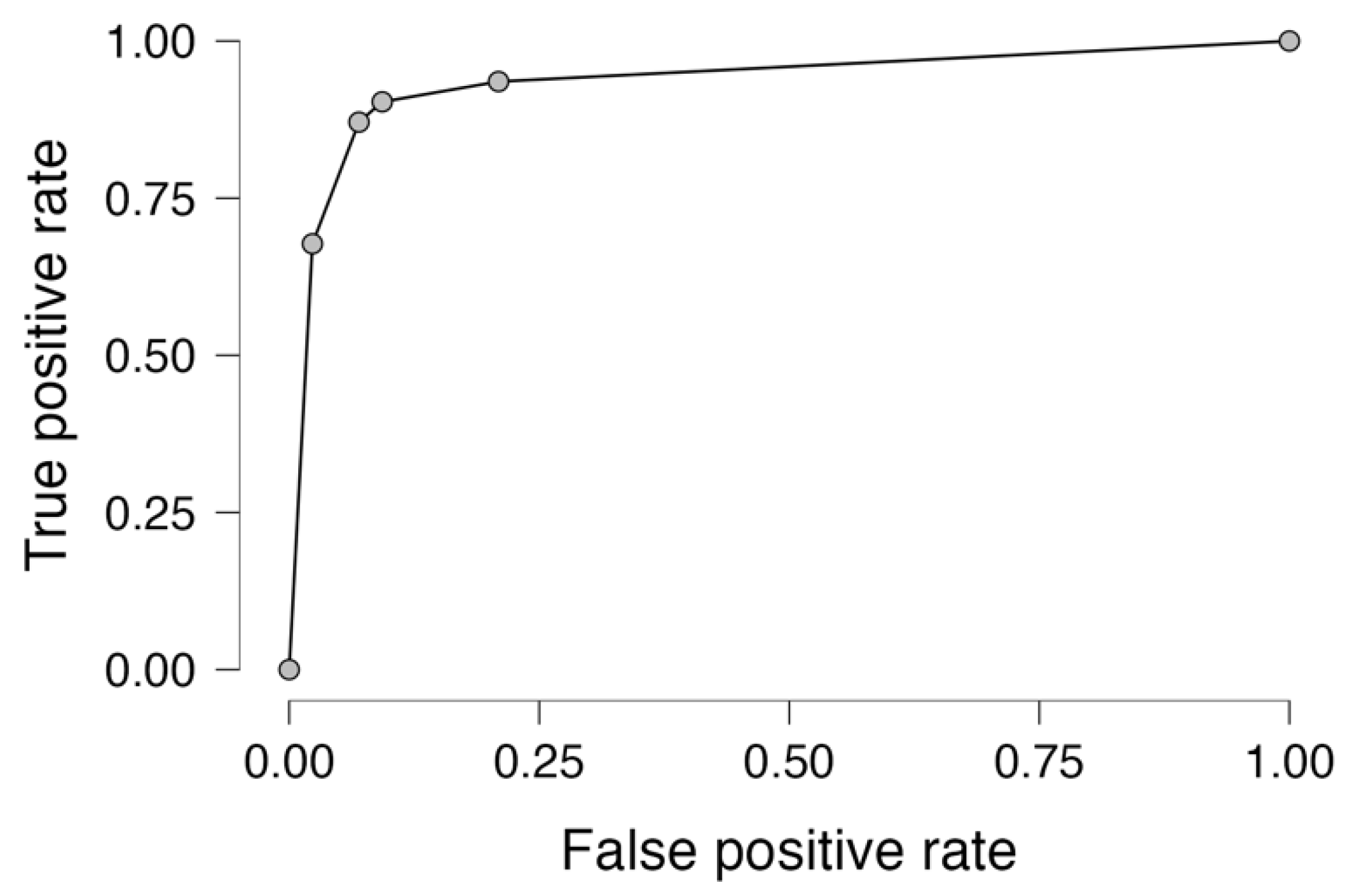
3.2. Receiver-Operator Curve Prediction for Coronary Artery Disease in Patients Living in Cities
4. Discussion
Study Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Duggan, J.P.; Peters, A.S.; Trachiotis, G.D.; Antevil, J.L. Epidemiology of Coronary Artery Disease. Surg. Clin. N. Am. 2022, 102, 499–516. [Google Scholar] [CrossRef] [PubMed]
- Cleven, L.; Krell-Roesch, J.; Nigg, C.R.; Woll, A. The association between physical activity with incident obesity, coronary heart disease, diabetes and hypertension in adults: A systematic review of longitudinal studies published after 2012. BMC Public Health 2020, 20, 726–741. [Google Scholar] [CrossRef] [PubMed]
- Simonetto, C.; Rospleszcz, S.; Kaiser, J.C.; Furukawa, K. Heterogeneity in coronary heart disease risk. Sci. Rep. 2022, 12, 10131–10140. [Google Scholar] [CrossRef] [PubMed]
- Malakar, A.K.; Choudhury, D.; Halder, B.; Paul, P.; Uddin, A.; Chakraborty, S. A review on coronary artery disease, its risk factors, and therapeutics. J. Cell Physiol. 2019, 234, 16812–16823. [Google Scholar] [CrossRef]
- Katta, N.; Loethen, T.; Lavie, C.J.; Alpert, M.A. Obesity and Coronary Heart Disease: Epidemiology, Pathology, and Coronary Artery Imaging. Curr. Probl. Cardiol. 2021, 46, 100655–100681. [Google Scholar] [CrossRef]
- Shufelt, C.L.; Pacheco, C.; Tweet, M.S.; Miller, V.M. Sex-Specific Physiology and Cardiovascular Disease. Adv. Exp. Med. Biol. 2018, 1065, 433–454. [Google Scholar]
- Khamis, R.Y.; Ammari, T.; Mikhail, G.W. Gender differences in coronary heart disease. Heart 2016, 102, 1142–1149. [Google Scholar] [CrossRef]
- Gimenez, M.R.; Scheller, B.; Farah, A.; Ohlow, M.-A.; Mangner, N.; Weilenmann, D.; Wöhrle, J.; Cuculi, F.; Leibundgut, G.; Möbius-Winkler, S.; et al. Sex-specific inequalities in the use of drug-coated balloons for small coronary artery disease: A report from the BASKET-SMALL 2 trial. Clin. Res. Cardiol. 2023. epub ahead of print. [Google Scholar]
- Urbanowicz, T.; Michalak, M.; Gąsecka, A.; Perek, B.; Rodzki, M.; Bociański, M.; Straburzyńska-Migaj, E.; Jemielity, M. Postoperative Neutrophil to Lymphocyte Ratio as an Overall Mortality Midterm Prognostic Factor following OPCAB Procedures. Clin. Pract. 2021, 11, 587–597. [Google Scholar] [CrossRef]
- Kim, C.; Redberg, R.F.; Pavlic, T.; Eagle, K.A. A systematic review of gender differences in mortality after coronary artery bypass graft surgery and percutaneous coronary interventions. Clin. Cardiol. 2007, 30, 491–495. [Google Scholar] [CrossRef]
- Shahrbaf, M.A.; Akbarzadeh, M.A.; Tabary, M.; Khaheshi, I. Air Pollution and Cardiac Arrhythmias: A Comprehensive Review. Curr. Probl. Cardiol. 2021, 46, 100649–100667. [Google Scholar] [CrossRef] [PubMed]
- de Bont, J.; Jaganathan, S.; Dahlquist, M.; Persson, Å.; Stafoggia, M.; Ljungman, P. Ambient air pollution and cardiovascular diseases: An umbrella review of systematic reviews and meta-analyses. J. Intern. Med. 2022, 291, 779–800. [Google Scholar] [CrossRef] [PubMed]
- Manisalidis, I.; Stavropoulou, E.; Stavropoulos, A.; Bezirtzoglou, E. Environmental and Health Impacts of Air Pollution: A Review. Front. Public Health 2020, 8, 14. [Google Scholar] [CrossRef] [PubMed]
- Franklin, B.A.; Brook, R.; Arden Pope, C., 3rd. Air pollution and cardiovascular disease. Curr. Probl. Cardiol. 2015, 40, 207–238. [Google Scholar] [CrossRef]
- Wang, M.; Zhou, T.; Song, Q.; Ma, H.; Hu, Y.; Heianza, Y.; Qi, L. Ambient air pollution, healthy diet and vegetable intakes, and mortality: A prospective UK Biobank study. Int. J. Epidemiol. 2022, 51, 1243–1253. [Google Scholar] [CrossRef] [PubMed]
- Wolf, K.; Hoffmann, B.; Andersen, Z.J.; Atkinson, R.W.; Bauwelinck, M.; Bellander, T.; Brandt, J.; Brunekreef, B.; Cesaroni, G.; Chen, J.; et al. Long-term exposure to low-level ambient air pollution and incidence of stroke and coronary heart disease: A pooled analysis of six European cohorts within the ELAPSE project. Lancet Planet Health 2021, 5, e620–e632. [Google Scholar] [CrossRef]
- Available online: https://powietrze.gios.gov.pl/pjp/maps/modeling (accessed on 1 July 2023).
- European Air Quality, Copernicus, Atmosphere Monitoring Service. Available online: https://www.regional.atmosphere.copernicus.eu/ (accessed on 27 December 2022).
- Available online: www.kobize.pl/en/article/national-database-on-greenhouse-gases-and-other-substances-emissions/id/1232/general-information (accessed on 19 July 2023).
- Tagaris, E.; Sotiropoulou, R.E.P.; Gounaris, N.; Andronopoulos, S.; Vlachogiannis, D. Effect of the Standard Nomenclature for Air Pollution (SNAP) categories on air quality over Europe. Atmosphere 2015, 6, 1119–1128. [Google Scholar] [CrossRef]
- Gawuc, L.; Szymankiewicz, K.; Kawicka, D.; Mielczarek, E.; Marek, K.; Soliwoda, M.; Maciejewska, J. Bottom–Up Inventory of Residential Combustion Emissions in Poland for National Air Quality Modelling: Current Status and Perspectives. Atmosphere 2021, 12, 1460. [Google Scholar] [CrossRef]
- Kaminski, J.W.; Neary, L.; Struzewska, J.; McConnell, J.C.; Lupu, A.; Jarosz, J.; Toyota, K.; Gong, S.L.; Côté, J.; Liu, X. GEM-AQ, an online global multiscale chemical weather modelling system: Model description and evaluation of gas phase chemistry processes. Atmos. Chem. Phys. 2008, 8, 3255–3281. [Google Scholar] [CrossRef]
- Markevych, I.; Orlov, N.; Grellier, J.; Kaczmarek-Majer, K.; Lipowska, M.; Sitnik-Warchulska, K.; Mysak, Y.; Baumbach, C.; Wierzba-Łukaszyk, M.; Soomro, M.H.; et al. NeuroSmog: Determining the impact of air pollution on the developing brain: Project protocol. Int. J. Environ. Res. Public Health 2022, 19, 310. [Google Scholar] [CrossRef]
- Fraszczyk, M.; Kaczmarek-Majer, K.; Hryniewicz, O.; Skotak, K.; Degorska, A. Expert-in-the-loop Stepwise Regression and its Application in Air Pollution Modeling. In Proceedings of the 2022 IEEE 11th International Conference on Intelligent Systems (IS), Warsaw, Poland, 12–14 October 2022; pp. 1–7. [Google Scholar]
- Chen, R.; Yin, P.; Meng, X.; Liu, C.; Wang, L.; Xu, X.; Ross, J.A.; Tse, L.A.; Zhao, Z.; Kan, H.; et al. Fine Particulate Air Pollution and Daily Mortality. A Nationwide Analysis in 272 Chinese Cities. Am. J. Respir. Crit. Care Med. 2017, 196, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Posadas-Sánchez, R.; Vargas-Alarcón, G.; Cardenas, A.; Texcalac-Sangrador, J.L.; Osorio-Yáñez, C.; Sanchez-Guerra, M. Long-Term Exposure to Ozone and Fine Particulate Matter and Risk of Premature Coronary Artery Disease: Results from Genetics of Atherosclerotic Disease Mexican Study. Biology 2022, 11, 1122. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Mengersen, K.; Tong, S.; Kimlin, M.; Zhou, M.; Wang, L.; Yin, P.; Xu, Z.; Cheng, J.; Zhang, Y.; et al. Short-term association between ambient air pollution and lung cancer mortality. Environ. Res. 2019, 179, 108748–108758. [Google Scholar] [CrossRef] [PubMed]
- Shakhov, V.; Materukhin, A.; Sokolova, O.; Koo, I. Optimizing Urban Air Pollution Detection Systems. Sensors 2022, 22, 4767. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Huang, J.; Li, G.; Wang, W.; Wang, K.; Wang, J.; Wei, C.; Li, Y.; Deng, F.; Baccarelli, A.; et al. Ozone pollution and hospital admissions for cardiovascular events. Eur. Heart J. 2023, 44, 1622–1632. [Google Scholar] [CrossRef]
- Chen, R.; Jiang, Y.; Hu, J.; Chen, H.; Li, H.; Meng, X.; Ji, J.S.; Gao, Y.; Wang, W.; Liu, C.; et al. Hourly Air Pollutants and Acute Coronary Syndrome Onset in 1.29 Million Patients. Circulation 2022, 145, 1749–1760. [Google Scholar] [CrossRef]
- Biondi-Zoccai, G.; Frati, G.; Gaspardone, A.; Mariano, E.; Di Giosa, A.D.; Bolignano, A.; Giudici, A.D.; Calcagno, S.; Scappaticci, M.; Sciarretta, S.; et al. Impact of environmental pollution and weather changes on the incidence of ST-elevation myocardial infarction. Eur. J. Prev. Cardiol. 2021, 28, 1501–1507. [Google Scholar] [CrossRef]
- Kuźma, Ł.; Wańha, W.; Kralisz, P.; Kazmierski, M.; Bachórzewska-Gajewska, H.; Wojakowski, W.; Dobrzycki, S. Impact of short-term air pollution exposure on acute coronary syndrome in two cohorts of industrial and non-industrial areas: A time series regression with 6,000,000 person-years of follow-up (ACS—Air Pollution Study). Environ. Res. 2021, 197, 111154–111165. [Google Scholar] [CrossRef]
- Kim, J.S.; Chen, Z.; Alderete, T.L.; Toledo-Corral, C.; Lurmann, F.; Berhane, K.; Gilliland, F.D. Associations of air pollution, obesity and cardiometabolic health in young adults: The Meta-AIR study. Environ. Int. 2019, 133, 105180–105205. [Google Scholar] [CrossRef]
- Tian, F.; Cai, M.; Li, H.; Qian, Z.M.; Chen, L.; Zou, H.; Zhang, Z.; Wang, C.; Xian, H.; McMillin, S.E.; et al. Air Pollution Associated with Incident Stroke, Poststroke Cardiovascular Events, and Death: A Trajectory Analysis of a Prospective Cohort. Neurology 2022, 99, e2474–e2484. [Google Scholar] [CrossRef]
- Dominski, F.H.; Lorenzetti Branco, J.H.; Buonanno, G.; Stabile, L.; Gameiro da Silva, M.; Andrade, A. Effects of air pollution on health: A mapping review of systematic reviews and meta-analyses. Environ. Res. 2021, 201, 111487–111501. [Google Scholar] [CrossRef] [PubMed]
- Münzel, T.; Gori, T.; Al-Kindi, S.; Deanfield, J.; Lelieveld, J.; Daiber, A.; Rajagopalan, S. Effects of gaseous and solid constituents of air pollution on endothelial function. Eur. Heart J. 2018, 39, 3543–3550. [Google Scholar] [CrossRef] [PubMed]
- Bevan, G.H.; Al-Kindi, S.G.; Brook, R.; Rajagopalan, S. Ambient Air Pollution and Atherosclerosis: Recent Updates. Curr. Atheroscler. Rep. 2021, 23, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Utell, M.J.; Frampton, M.W.; Zareba, W.; Devlin, R.B.; Cascio, W.E. Cardiovascular effects associated with air pollution: Potential mechanisms and methods of testing. Inhal. Toxicol. 2002, 14, 1231–1247. [Google Scholar] [CrossRef]
- Liang, S.; Zhang, J.; Ning, R.; Du, Z.; Liu, J.; Batibawa, J.W.; Duan, J.; Sun, Z. The critical role of endothelial function in fine particulate matter-induced atherosclerosis. Part Fibre Toxicol. 2020, 17, 61–85. [Google Scholar] [CrossRef]
- Zhang, H.; Yi, M.; Wang, Y.; Zhang, Y.; Xiao, K.; Si, J.; Shi, N.; Sun, L.; Miao, Z.; Zhao, T.; et al. Air pollution and recurrence of cardiovascular events after ST-segment elevation myocardial infarction. Atherosclerosis 2022, 342, 1–8. [Google Scholar] [CrossRef]
- Ain, N.U.; Qamar, S.U.R. Particulate Matter-Induced Cardiovascular Dysfunction: A Mechanistic Insight. Cardiovasc. Toxicol. 2021, 21, 505–516. [Google Scholar] [CrossRef]
- Chen, S.Y.; Hwang, J.S.; Chan, C.C.; Wu, C.F.; Wu, C.; Su, T.C. Urban Air Pollution and Subclinical Atherosclerosis in Adolescents and Young Adults. J. Adolesc. Health. 2022, 71, 233–238. [Google Scholar] [CrossRef]
- Brunekreef, B.; Strak, M.; Chen, J.; Andersen, Z.J.; Atkinson, R.; Bauwelinck, M.; Bellander, T.; Boutron, M.-C.; Brandt, J.; Carey, I.; et al. Mortality and Morbidity Effects of Long-Term Exposure to Low-Level PM2.5, BC, NO2, and O3: An Analysis of European Cohorts in the ELAPSE Project. Res. Rep. Health Eff. Inst. 2021, 208, 1–127. [Google Scholar]
- Rus, A.A.; Mornoş, C. The Impact of Meteorological Factors and Air Pollutants on Acute Coronary Syndrome. Curr. Cardiol. Rep. 2022, 24, 1337–1349. [Google Scholar] [CrossRef]
- Kaluzna-Oleksy, M.; Aunan, K.; Rao-Skirbekk, S.; Kjellstrom, T.; Ezekowitz, J.A.; Agewall, S.; Atar, D. Impact of climate and air pollution on acute coronary syndromes: An update from the European Society of Cardiology Congress 2017. Scand Cardiovasc. J. 2018, 52, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Chirón, L.; Negral, L.; Megido, L.; Suárez-Peña, B.; Domínguez-Rodríguez, A.; Rodríguez, S.; Abreu-Gonzalez, P.; Pascual, I.; Moris, C.; Avanzas, P. Relationship Between Exposure to Sulphur Dioxide Air Pollution, White Cell Inflammatory Biomarkers and Enzymatic Infarct Size in Patients With ST-segment Elevation Acute Coronary Syndromes. Eur. Cardiol. 2021, 16, e50–e55. [Google Scholar] [CrossRef] [PubMed]
- Coelho, S.; Ferreira, J.; Rodrigues, V.; Lopes, M. Source apportionment of air pollution in European urban areas: Lessons from the ClairCity project. J. Environ. Manag. 2022, 320, 115899–115909. [Google Scholar] [CrossRef] [PubMed]
- Kiesewetter, G.; Borken-Kleefeld, J.; Schöpp, W.; Heyes, C.; Thunis, P.; Bessagnet, B.; Terrenoire, E.; Gsella, A.; Amann, M. Modelling NO2 concentrations at the street level in the GAINS integrated assessment model: Projections under current legislation. Atmos. Chem. Phys. 2014, 14, 813–829. [Google Scholar] [CrossRef]
- Newell, K.; Kartsonaki, C.; Lam, K.B.H.; Kurmi, O. Cardiorespiratory health effects of gaseous ambient air pollution exposure in low and middle income countries: A systematic review and meta-analysis. Environ. Health 2018, 17, 41–55. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Wang, W.; Fecht, D.; Beevers, S.; Gulliver, J. Predicting daily concentrations of nitrogen dioxide, particulate matter and ozone at fine spatial scale in Great Britain. Atmos. Pollut. Res. 2022, 13, 101506–101512. [Google Scholar] [CrossRef]
- Liu, C.; Chen, R.; Sera, F.; Vicedo-Cabrera, A.M.; Guo, Y.; Tong, S.; Coelho, M.S.Z.S.; Saldiva, P.H.N.; Lavigne, E.; Matus, P.; et al. Ambient Particulate Air Pollution and Daily Mortality in 652 Cities. N. Engl. J. Med. 2019, 381, 705–715. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | Group 1 | Group 2 | p |
|---|---|---|---|
| n = 90 | n = 58 | ||
| Sex (male (%)/female (%)) | 66 (73)/24 (27) | 36 (62)/22 (38) | 0.657 |
| Age (years) (median (Q1–Q3)) | 68 (57–73) | 72 (65–77) | 0.074 |
| Weight (kg) (median (Q1–Q3)) | 93 (92–94) | 90 (67–94) | 0.434 |
| Height (cm) (median (Q1–Q3)) | 168 (162–175) | 171 (161–176) | 0.703 |
| Body mass index (median (Q1–Q3)) | 29.7 (27.2–33.8) | 29.1 (25.7–31.5) | 0.398 |
| Co-morbidities: | |||
| Arterial hypertension (n(%)) | 47 (52) | 34 (59) | 0.445 |
| Diabetes mellitus (n(%)) | 26 (29) | 14 (24) | 0.525 |
| Hypercholesterolemia (n(%)) | 48 (53) | 30 (52) | 0.848 |
| COPD (n(%)) | 5 (6) | 3 (5) | 0.919 |
| Thyroid disease (n(%)) | 10 (11) | 5 (9) | 0.624 |
| Atrial fibrillation (n(%)) | 8 (9) | 4 (7) | 0.665 |
| Current nicotinism (n(%)) | 3 (3) | 1 (2) | 0.556 |
| Stroke (n(%)) | 3 (3) | 3 (5) | 0.58 |
| PAD (n(%)) | 9 (10) | 5 (9) | 0.78 |
| Current nicotinism (n(%)) | 3 (3) | 1 (2) | 0.556 |
| Echocardiographic results | |||
| Left ventricular diameter (mm) (median (Q1–Q3)) | 40 (38–43) | 47 (44–50) | 0.044 * |
| Left atrium diameter (mm) (median (Q1–Q3)) | 35 (30–37) | 39 (37–42) | 0.137 |
| Left ventricular ejection fraction (%)(median (Q1–Q3)) | 65 (60–65) | 55 (55–60) | 0.199 |
| Laboratory results | |||
| WBC (×109/L) (median (Q1–Q3)) | 7.48 (7.29–8.41) | 7.44 (6.13–8.67) | 0.669 |
| Neutrophils (×109/L) (median (Q1–Q3)) | 5.28 (4.90–5.64) | 4.14 (3.54–5.58) | 0.269 |
| Lymphocyte (×109/L) (median (Q1–Q3)) | 1.70 (1.54–2.11) | 1.98 (1.45–2.20) | 0.88 |
| Monocyte (×109/L) (median (Q1–Q3)) | 0.50 (0.42–0.52) | 0.46 (0.41–0.57) | 0.801 |
| Platelets (×109/L) (median (Q1–Q3)) | 218 (216–231) | 218 (178–255) | 0.88 |
| Hemoglobin (mmol/L) (median (Q1–Q3)) | 7.70 (7.55–8.30) | 8.60 (8.25–8.98) | 0.19 |
| Hematocrit (%) (median (Q1–Q3)) | 36 (35–40) | 38 (34–43) | 0.21 |
| MPV (fl) (median (Q1–Q3)) | 9.1 (8.5–9.4) | 8.4 (7.9–9.2) | 0.58 |
| MCV (median (Q1–Q3)) | 90 (89–92) | 93 (90–97) | 0.313 |
| MCHC (mmol/L) (median (Q1–Q3)) | 20.87 (20.82–20.97) | 20.96 (20.59–21.40) | 0.802 |
| RDW (%) (median (Q1–Q3)) | 12.60 (12.55–12.90) | 13.80 (13.18–14.18) | 0.030 * |
| Creatinine (median (Q1–Q3)) | 90 (83–108) | 92 (71–108) | 0.725 |
| GFR (umol/l) (median (Q1–Q3)) | 59 (57–65) | 74 (60–86) | 0.242 |
| Ureic acid (median (Q1–Q3)) | 296 (272–352) | 363 (317–403) | 0.634 |
| Group 1 | Group 2 | p | |
|---|---|---|---|
| n = 90 | n = 58 | ||
| First angiographic results | |||
| 1. Disease (>30% stenosis): | |||
| 1. LMCA disease (n,%) | 6 (7) | 4 (7) | 0.96 |
| 2. LAD disease (n,%) | 52 (58) | 33 (57) | 0.918 |
| 3. Cx disease (n,%) | 29 (32) | 16 (28) | 0.552 |
| 4. RCA disease (n,%) | 42 (47) | 23 (40) | 0.404 |
| 2. Normal angiogram (n,%) | 21 (23) | 11 (19) | 0.532 |
| 3. Culprit lesion > 70% (n,%) | 75 (83) | 56 (97) | 0.179 |
| 4. Performed procedures: | |||
| 1. Single PCIs (n,%) | 55 (61) | 37 (64) | 0.645 |
| 2. Two stents (n,%) | 10 (11) | 7 (12) | 0.773 |
| 3. On bifurcation (n,%) | 5 (6) | 5 (9) | 0.84 |
| Second angiographic results | |||
| 1. Disease (>30% stenosis): | |||
| 1. LMCA disease (n,%) | 7 (8) | 5 (9) | 0.858 |
| 2. LAD disease (n,%) | 41 (46) | 26 (45) | 0.933 |
| 3. Cx disease (n,%) | 29 (32) | 11 (19) | 0.078 |
| 4. RCA disease (n,%) | 33 (37) | 26 (45) | 0.325 |
| 2. Normal angiogram (n,%) | 3 (3) | 1 (2) | 0.079 |
| 3. Culprit lesion >70% (n,%) | 46 (51) | 55 (9) | 0.049 * |
| 4. Performed procedures: | |||
| 1. Single PCIs (n,%) | 44 (49) | 26 (45) | 0.732 |
| 2. Two stents (n,%) | 1 (1) | 11 (19) | 0.021 * |
| 3. Bifurcation (n,%) | 0 (0) | 7 (12) | 0.023 * |
| 5. Culprit lesion change (%) | 55 (10–90) | 68 (15–97) | 0.383 |
| Parameter | Group 1 | Group 2 | p |
|---|---|---|---|
| n = 90 | n = 58 | ||
| Particulate Matter < 2.5 (PM < 2.5) | |||
| Mean exposure in 2019 (median (Q1–Q3)) | 17.5 (15.5–19.1) | 17.5 (16.6–18.7) | 0.736 |
| Mean exposure in 2020 (median (Q1–Q3)) | 12.6 (11.0–15.1) | 16.4 (14.7–19.1) | <0.001 |
| Mean exposure in 2021 (median (Q1–Q3)) | 14.6 (13.4–16.3) | 17.7 (15.8–19.2) | <0.001 |
| Mean exposure 2019–2021 (median (Q1–Q3)) | 15.8 (13.6–16.6) | 17.2 (16.0–18.9) | <0.001 |
| Maximal exposure (median (Q1–Q3)) | 18 (15.5–19.3) | 18.9 (16.9–20.0) | 0.269 |
| Particulate Matter < 10 (PM < 10) | |||
| Mean exposure in 2019 (median (Q1–Q3)) | 23.4 (21.8–25.0) | 26.4 (24.6 28.6) | <0.001 |
| Mean exposure in 2020 (median (Q1–Q3)) | 20.2 (18.4–22.0) | 23.7 (21.9–28.1) | <0.001 |
| Mean exposure in 2021 (median (Q1–Q3)) | 23.3 (22.1–28.1) | 25.9 (23.6–29.7) | <0.001 |
| Mean exposure 2019–2021 (median (Q1–Q3)) | 22.2 (21.5–23.5) | 25.4 (23.6 28.7) | <0.001 |
| Maximal exposure (median (Q1–Q3)) | 24.0 (22.6–26.00) | 26.6 (25.2–30.1) | <0.001 |
| Nitrogen Oxides (NO2) | |||
| Mean exposure in 2019 (median (Q1–Q3)) | 12.2 (10.5–14.2) | 22.4 (19.4–24.00) | <0.001 |
| Mean exposure in 2020 (median (Q1–Q3)) | 11.2 (10.2–13.1) | 17.8 (16.5–18.7) | <0.001 |
| Mean exposure in 2021 (median (Q1–Q3)) | 12.6 (12.00–13.8) | 18.1 (17.0–19.5) | <0.001 |
| Mean exposure 2019–2021 (median (Q1–Q3)) | 12.1 (11.0–13.6) | 19.4 (17.8–20.7) | <0.001 |
| Maximal exposure (median (Q1–Q3)) | 13.0 (12.0–14.2) | 22.5 (19.7–24.0) | <0.001 |
| Univariable | Multivariable | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | |
| Demographical factors: | - | - | - | |||
| Sex | 1.24 | 0.42–1.84 | <0.001 * | |||
| Age | 1.05 | 0.10–1.13 | 0.055 | |||
| Co-morbidities | - | - | - | |||
| Arterial hypertension | 5.43 | 0.42–29.63 | 0.009 * | |||
| DM | 2.83 | 0.01–2.92 | 0.073 | |||
| Hyperlipidemia | 2.65 | 0.50–14.55 | <0.001 * | |||
| Thyroid disease | 1.99 | 0.14–1.15 | 0.418 | |||
| Laboratory results: | - | - | - | |||
| WBC | 0.66 | 0.03–0.21 | 0.197 | |||
| Hemoglobin | 2.06 | 0.61–2.05 | 0.286 | |||
| NLR | 1.09 | 0.77–1.09 | 0.557 | |||
| MLR | 4.83 | 1.67–4.82 | 0.342 | |||
| SIRI | 2.23 | 1.14–2.74 | 0.42 | |||
| MCHC | 0.77 | 0.61–2.43 | 0.243 | |||
| Creatinine | 1.01 | 0.03–0.53 | 0.486 | |||
| Ureic acid | 1 | 0.03–1.02 | 0.734 | |||
| Air pollution—PM < 2.5 | - | - | - | |||
| PM < 2.5 in 2019 | 0.98 | 0.796–1.722 | 0.859 | |||
| PM < 2.5 in 2020 | 4.13 | 0.23–6.42 | <0.001 | |||
| PM < 2.5 in 2021 | 1.53 | 0.20–6.58 | <0.001 | |||
| Mean PM < 2.5 exposure | 1.44 | 0.21–5.17 | <0.001 | |||
| Max PM < 2.5 exposure | 1.15 | 0.01–2.76 | 0.033 | |||
| Air pollution—PM < 10 | - | - | - | |||
| PM < 10 in 2019 | 1.39 | 0.20–4.55 | <0.001 | |||
| PM < 10 in 2020 | 1.43 | 0.23–4.87 | <0.001 | |||
| PM < 10 in 2021 | 1.28 | 0.13–3.55 | <0.001 | |||
| Mean PM < 10 exposure | 1.44 | 0.23–5.01 | <0.001 | |||
| Max PM < 10 exposure | 1.33 | 0.17–4.04 | <0.001 | |||
| Air pollution—NO2 | ||||||
| NO2 in 2019 | 1.57 | 0.33–5.80 | <0.001 | |||
| NO2 in 2020 | 1.99 | 0.49–8.80 | <0.001 | |||
| NO2 in 2021 | 2.35 | 0.61–1.10 | <0.001 | |||
| Mean | 1.93 | 0.48–8.45 | <0.001 | 2 | 0.41–9.62 | <0.001 |
| Max | 1.76 | 0.41–7.27 | <0.001 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urbanowicz, T.; Skotak, K.; Filipiak, K.J.; Olasińska-Wiśniewska, A.; Szczepański, K.; Wyrwa, M.; Sikora, J.; Tykarski, A.; Jemielity, M. Long-Term Exposure of Nitrogen Oxides Air Pollution (NO2) Impact for Coronary Artery Lesion Progression—Pilot Study. J. Pers. Med. 2023, 13, 1376. https://doi.org/10.3390/jpm13091376
Urbanowicz T, Skotak K, Filipiak KJ, Olasińska-Wiśniewska A, Szczepański K, Wyrwa M, Sikora J, Tykarski A, Jemielity M. Long-Term Exposure of Nitrogen Oxides Air Pollution (NO2) Impact for Coronary Artery Lesion Progression—Pilot Study. Journal of Personalized Medicine. 2023; 13(9):1376. https://doi.org/10.3390/jpm13091376
Chicago/Turabian StyleUrbanowicz, Tomasz, Krzysztof Skotak, Krzysztof J. Filipiak, Anna Olasińska-Wiśniewska, Krystian Szczepański, Michał Wyrwa, Jędrzej Sikora, Andrzej Tykarski, and Marek Jemielity. 2023. "Long-Term Exposure of Nitrogen Oxides Air Pollution (NO2) Impact for Coronary Artery Lesion Progression—Pilot Study" Journal of Personalized Medicine 13, no. 9: 1376. https://doi.org/10.3390/jpm13091376