
Persistent Endothelial Lung Damage and Impaired Diffusion Capacity in Long COVID
 , , , , , , , , ,
, , , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics
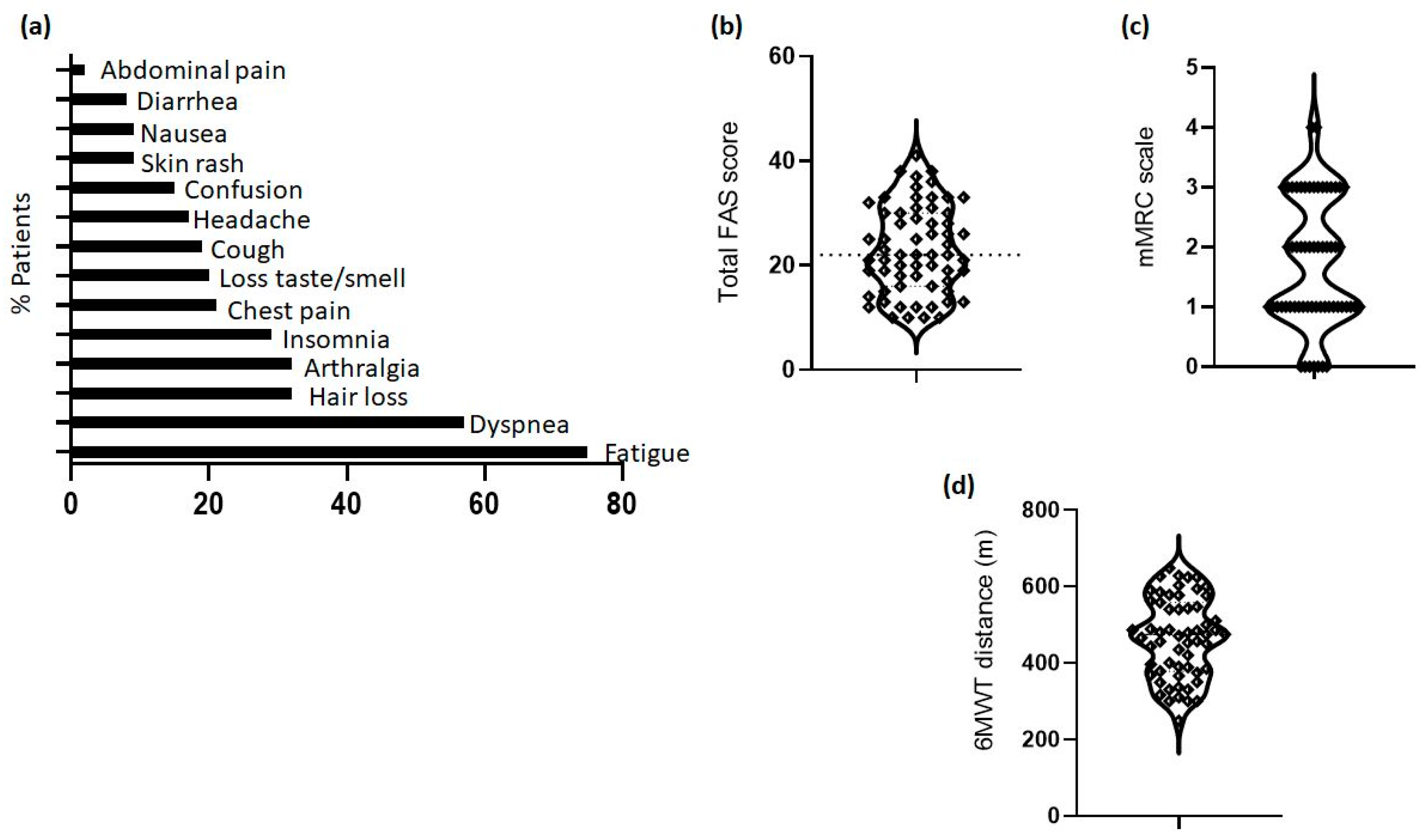
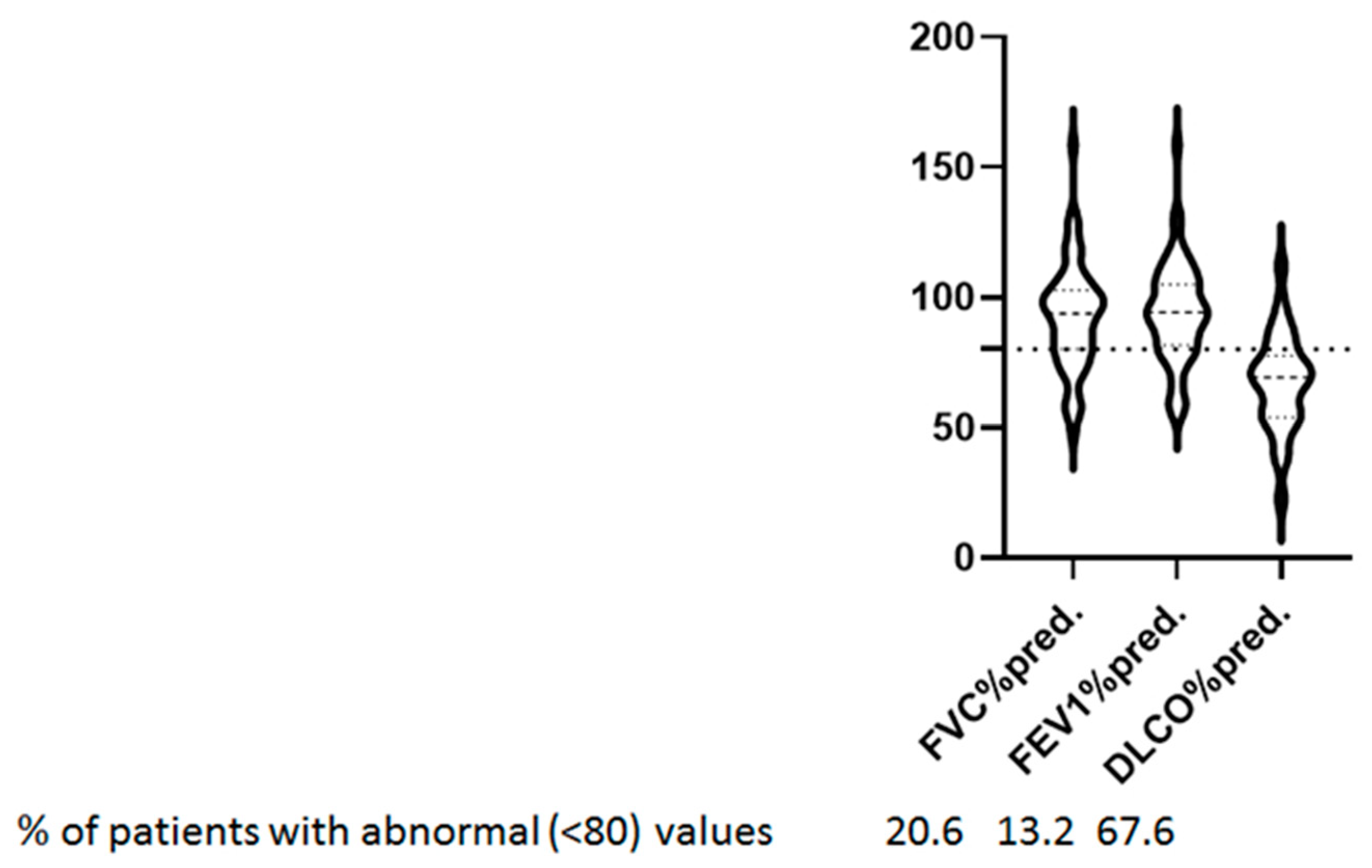
3.2. Long COVID Symptoms, 6-min Walk Test, and Lung Function Tests
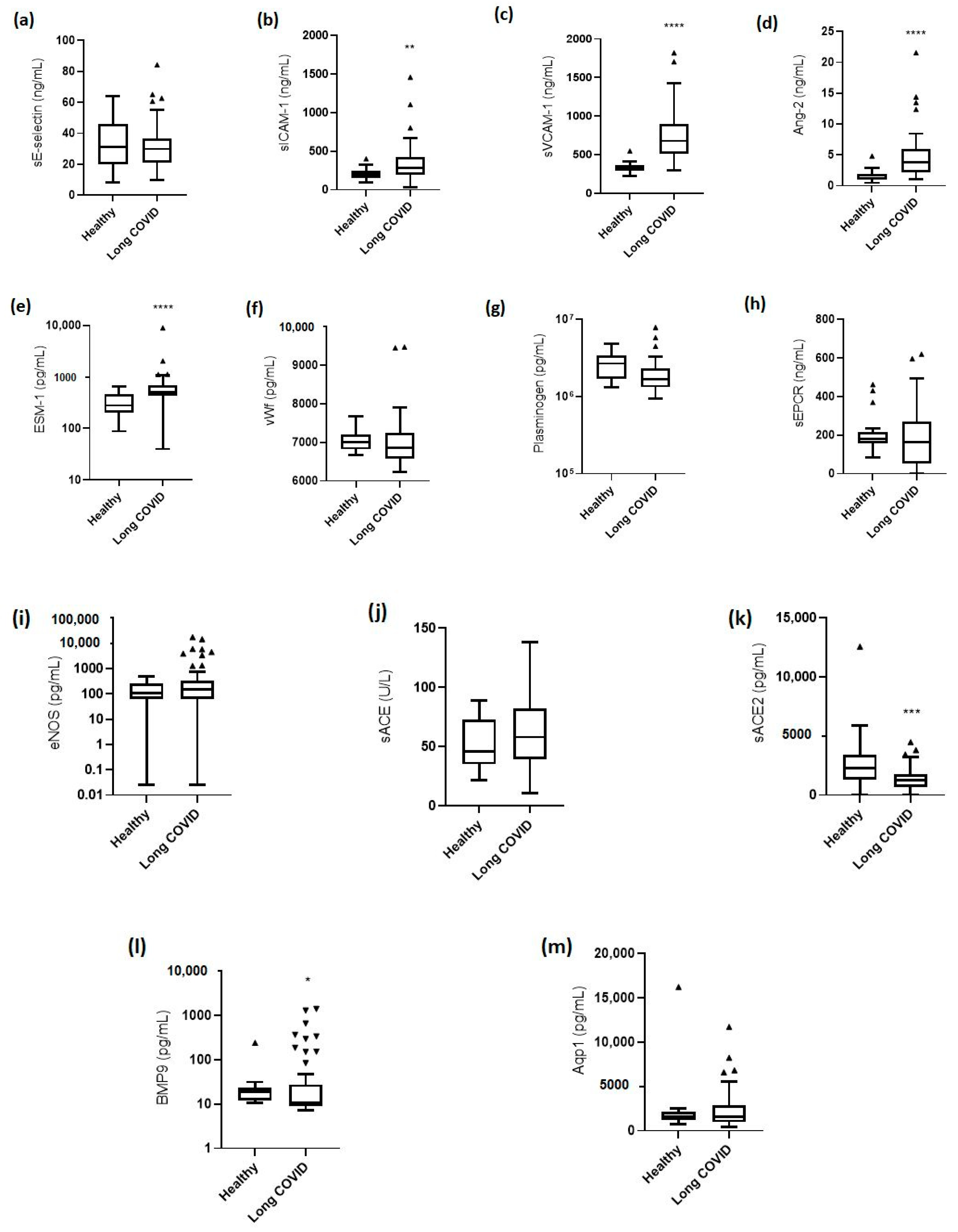
3.3. Levels of Endothelial Biomarkers
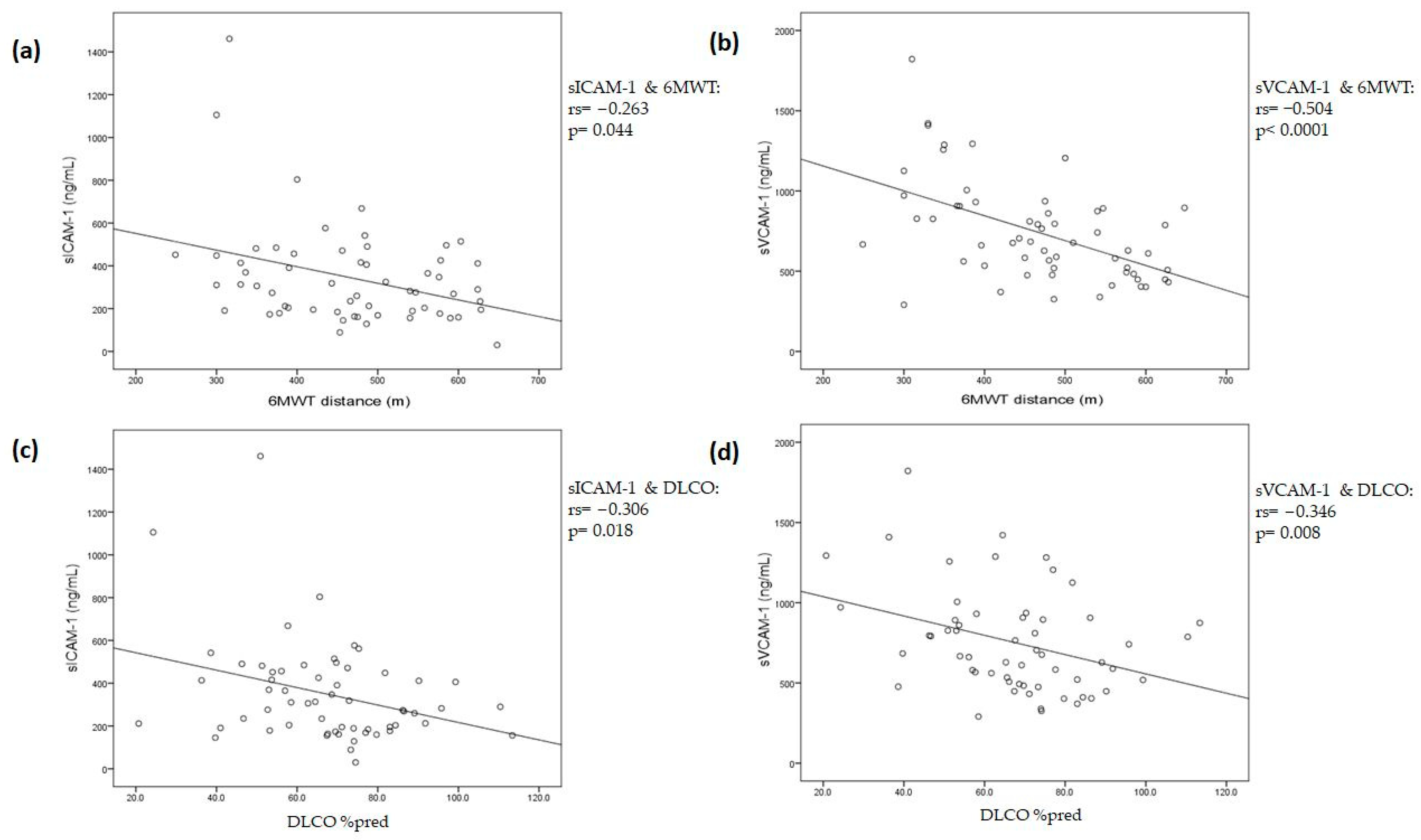
3.4. Associations between Endothelial Biomarkers and Long COVID Symptoms, 6-min Walking Test, and Lung Function Tests
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bonaventura, A.; Vecchié, A.; Dagna, L.; Martinod, K.; Dixon, D.L.; Van Tassell, B.W.; Dentali, F.; Montecucco, F.; Massberg, S.; Levi, M.; et al. Endothelial dysfunction and immunothrombosis as key pathogenic mechanisms in COVID-19. Nat. Rev. Immunol. 2021, 21, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Osuchowski, M.F.; Winkler, M.S.; Skirecki, T.; Cajander, S.; Shankar-Hari, M.; Lachmann, G.; Monneret, G.; Venet, F.; Bauer, M.; Brunkhorst, F.M.; et al. The COVID-19 puzzle: Deciphering pathophysiology and phenotypes of a new disease entity. Lancet Respir. Med. 2021, 9, 622–642. [Google Scholar] [CrossRef] [PubMed]
- Leentjens, J.; van Haaps, T.F.; Wessels, P.F.; Schutgens, R.E.G.; Middeldorp, S. COVID-19-associated coagulopathy and antithrombotic agents-lessons after 1 year. Lancet Haematol. 2021, 8, e524–e533. [Google Scholar] [CrossRef] [PubMed]
- Vassiliou, A.G.; Vrettou, C.S.; Keskinidou, C.; Dimopoulou, I.; Kotanidou, A.; Orfanos, S.E. Endotheliopathy in Acute COVID-19 and Long COVID. Int. J. Mol. Sci. 2023, 24, 8237. [Google Scholar] [CrossRef]
- Cojocaru, C.; Cojocaru, E.; Turcanu, A.M.; Zaharia, D.C. Clinical challenges of SARS-CoV-2 variants (Review). Exp. Ther. Med. 2022, 23, 416. [Google Scholar] [CrossRef]
- Thakur, P.; Thakur, V.; Kumar, P.; Patel, S.K.S. Emergence of novel omicron hybrid variants: BA(x), XE, XD, XF more than just alphabets. Int. J. Surg. 2022, 104, 106727. [Google Scholar] [CrossRef]
- Thakur, V.; Bhola, S.; Thakur, P.; Patel, S.K.S.; Kulshrestha, S.; Ratho, R.K.; Kumar, P. Waves and variants of SARS-CoV-2: Understanding the causes and effect of the COVID-19 catastrophe. Infection 2022, 50, 309–325. [Google Scholar] [CrossRef]
- Xu, S.W.; Ilyas, I.; Weng, J.P. Endothelial dysfunction in COVID-19: An overview of evidence, biomarkers, mechanisms and potential therapies. Acta Pharmacol. Sin. 2023, 44, 695–709. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in COVID-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Goshua, G.; Pine, A.B.; Meizlish, M.L.; Chang, C.H.; Zhang, H.; Bahel, P.; Baluha, A.; Bar, N.; Bona, R.D.; Burns, A.J.; et al. Endotheliopathy in COVID-19-associated coagulopathy: Evidence from a single-centre, cross-sectional study. Lancet Haematol. 2020, 7, e575–e582. [Google Scholar] [CrossRef]
- Osiaevi, I.; Schulze, A.; Evers, G.; Harmening, K.; Vink, H.; Kümpers, P.; Mohr, M.; Rovas, A. Persistent capillary rarefication in long COVID syndrome. Angiogenesis 2023, 26, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.A.; Knauer, M.J.; Nicholson, M.; Daley, M.; Van Nynatten, L.R.; Martin, C.; Patterson, E.K.; Cepinskas, G.; Seney, S.L.; Dobretzberger, V.; et al. Elevated vascular transformation blood biomarkers in Long-COVID indicate angiogenesis as a key pathophysiological mechanism. Mol. Med. 2022, 28, 122. [Google Scholar] [CrossRef] [PubMed]
- Pretorius, E.; Vlok, M.; Venter, C.; Bezuidenhout, J.A.; Laubscher, G.J.; Steenkamp, J.; Kell, D.B. Persistent clotting protein pathology in Long COVID/Post-Acute Sequelae of COVID-19 (PASC) is accompanied by increased levels of antiplasmin. Cardiovasc. Diabetol. 2021, 20, 172. [Google Scholar] [CrossRef] [PubMed]
- Katsoularis, I.; Fonseca-Rodríguez, O.; Farrington, P.; Jerndal, H.; Lundevaller, E.H.; Sund, M.; Lindmark, K.; Connolly, A.M.F. Risks of deep vein thrombosis, pulmonary embolism, and bleeding after COVID-19: Nationwide self-controlled cases series and matched cohort study. BMJ 2022, 377, e069590. [Google Scholar] [CrossRef]
- Gorog, D.A.; Storey, R.F.; Gurbel, P.A.; Tantry, U.S.; Berger, J.S.; Chan, M.Y.; Duerschmied, D.; Smyth, S.S.; Parker, W.A.E.; Ajjan, R.A.; et al. Current and novel biomarkers of thrombotic risk in COVID-19: A Consensus Statement from the International COVID-19 Thrombosis Biomarkers Colloquium. Nat. Rev. Cardiol. 2022, 19, 475–495. [Google Scholar] [CrossRef]
- Sood, T.; Perrot, N.; Chong, M.; Mohammadi-Shemirani, P.; Mushtaha, M.; Leong, D.; Rangarajan, S.; Hess, S.; Yusuf, S.; Gerstein, H.C.; et al. Biomarkers Associated with Severe COVID-19 Among Populations with High Cardiometabolic Risk: A 2-Sample Mendelian Randomization Study. JAMA Netw Open 2023, 6, e2325914. [Google Scholar] [CrossRef]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef]
- Yang, C.; Tebbutt, S.J. Long COVID: The next public health crisis is already on its way. Lancet Reg. Health Eur. 2023, 28, 100612. [Google Scholar] [CrossRef]
- Katsarou, M.S.; Iasonidou, E.; Osarogue, A.; Kalafatis, E.; Stefanatou, M.; Pappa, S.; Gatzonis, S.; Verentzioti, A.; Gounopoulos, P.; Demponeras, C.; et al. The Greek Collaborative Long COVID Study: Non-Hospitalized and Hospitalized Patients Share Similar Symptom Patterns. J. Pers. Med. 2022, 12, 987. [Google Scholar] [CrossRef]
- Castanares-Zapatero, D.; Chalon, P.; Kohn, L.; Dauvrin, M.; Detollenaere, J.; de Noordhout, C.M.; Primus-de Jong, C.; Cleemput, I.; Van den Heede, K. Pathophysiology and mechanism of long COVID: A comprehensive review. Ann. Med. 2022, 54, 1473–1487. [Google Scholar] [CrossRef]
- Raman, B.; Bluemke, D.A.; Lüscher, T.F.; Neubauer, S. Long COVID: Post-acute sequelae of COVID-19 with a cardiovascular focus. Eur. Heart J. 2022, 43, 1157–1172. [Google Scholar] [CrossRef] [PubMed]
- Gyöngyösi, M.; Alcaide, P.; Asselbergs, F.W.; Brundel, B.; Camici, G.G.; Martins, P.D.C.; Ferdinandy, P.; Fontana, M.; Girao, H.; Gnecchi, M.; et al. Long COVID and the cardiovascular system-elucidating causes and cellular mechanisms in order to develop targeted diagnostic and therapeutic strategies: A joint Scientific Statement of the ESC Working Groups on Cellular Biology of the Heart and Myocardial and Pericardial Diseases. Cardiovasc. Res. 2023, 119, 336–356. [Google Scholar] [PubMed]
- Michielsen, H.J.; De Vries, J.; Van Heck, G.L. Psychometric qualities of a brief self-rated fatigue measure: The Fatigue Assessment Scale. J. Psychosom. Res. 2003, 54, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, C.M.; Elmes, P.C.; Fairbairn, A.S.; Wood, C.H. The significance of respiratory symptoms and the diagnosis of chronic bronchitis in a working population. Br. Med. J. 1959, 2, 257–266. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am. J. Respir. Crit. Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef]
- Graham, B.L.; Brusasco, V.; Burgos, F.; Cooper, B.G.; Jensen, R.; Kendrick, A.; MacIntyre, N.R.; Thompson, B.R.; Wanger, J. 2017 ERS/ATS standards for single-breath carbon monoxide uptake in the lung. Eur. Respir. J. 2017, 49, 1600016. [Google Scholar] [CrossRef]
- Keskinidou, C.; Vassiliou, A.G.; Zacharis, A.; Jahaj, E.; Gallos, P.; Dimopoulou, I.; Orfanos, S.E.; Kotanidou, A. Endothelial, Immunothrombotic, and Inflammatory Biomarkers in the Risk of Mortality in Critically Ill COVID-19 Patients: The Role of Dexamethasone. Diagnostics 2021, 11, 1249. [Google Scholar] [CrossRef]
- Vassiliou, A.G.; Keskinidou, C.; Jahaj, E.; Gallos, P.; Dimopoulou, I.; Kotanidou, A.; Orfanos, S.E. ICU Admission Levels of Endothelial Biomarkers as Predictors of Mortality in Critically Ill COVID-19 Patients. Cells 2021, 10, 186. [Google Scholar] [CrossRef]
- Vassiliou, A.G.; Zacharis, A.; Keskinidou, C.; Jahaj, E.; Pratikaki, M.; Gallos, P.; Dimopoulou, I.; Kotanidou, A.; Orfanos, S.E. Soluble Angiotensin Converting Enzyme 2 (ACE2) Is Upregulated and Soluble Endothelial Nitric Oxide Synthase (eNOS) Is Downregulated in COVID-19-induced Acute Respiratory Distress Syndrome (ARDS). Pharmaceuticals 2021, 14, 695. [Google Scholar] [CrossRef]
- Stanojevic, S.; Kaminsky, D.A.; Miller, M.R.; Thompson, B.; Aliverti, A.; Barjaktarevic, I.; Cooper, B.G.; Culver, B.; Derom, E.; Hall, G.L.; et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur. Respir. J. 2022, 60, 2101499. [Google Scholar] [CrossRef]
- Sonnweber, T.; Sahanic, S.; Pizzini, A.; Luger, A.; Schwabl, C.; Sonnweber, B.; Kurz, K.; Koppelstätter, S.; Haschka, D.; Petzer, V.; et al. Cardiopulmonary recovery after COVID-19: An observational prospective multicentre trial. Eur. Respir. J. 2021, 57, 2003481. [Google Scholar] [CrossRef]
- Liu, K.; Zhang, W.; Yang, Y.; Zhang, J.; Li, Y.; Chen, Y. Respiratory rehabilitation in elderly patients with COVID-19: A randomized controlled study. Complement Ther. Clin. Pract. 2020, 39, 101166. [Google Scholar] [CrossRef]
- Pellegrino, R.; Viegi, G.; Brusasco, V.; Crapo, R.O.; Burgos, F.; Casaburi, R.; Coates, A.; van der Grinten, C.P.; Gustafsson, P.; Hankinson, J.; et al. Interpretative strategies for lung function tests. Eur. Respir. J. 2005, 26, 948–968. [Google Scholar] [CrossRef] [PubMed]
- Langleben, D.; Orfanos, S.E.; Giovinazzo, M.; Hirsch, A.; Baron, M.; Senécal, J.L.; Armaganidis, A.; Catravas, J.D. Pulmonary capillary endothelial metabolic dysfunction: Severity in pulmonary arterial hypertension related to connective tissue disease versus idiopathic pulmonary arterial hypertension. Arthritis Rheum. 2008, 58, 1156–1164. [Google Scholar] [CrossRef] [PubMed]
- Blanco, J.R.; Cobos-Ceballos, M.J.; Navarro, F.; Sanjoaquin, I.; Arnaiz de Las Revillas, F.; Bernal, E.; Buzon-Martin, L.; Viribay, M.; Romero, L.; Espejo-Perez, S.; et al. Pulmonary long-term consequences of COVID-19 infections after hospital discharge. Clin. Microbiol. Infect. 2021, 27, 892–896. [Google Scholar] [CrossRef]
- van der Sar-van der Brugge, S.; Talman, S.; Boonman-de Winter, L.; de Mol, M.; Hoefman, E.; van Etten, R.W.; De Backer, I.C. Pulmonary function and health-related quality of life after COVID-19 pneumonia. Respir. Med. 2021, 176, 106272. [Google Scholar] [CrossRef] [PubMed]
- Guler, S.A.; Ebner, L.; Aubry-Beigelman, C.; Bridevaux, P.O.; Brutsche, M.; Clarenbach, C.; Garzoni, C.; Geiser, T.K.; Lenoir, A.; Mancinetti, M.; et al. Pulmonary function and radiological features 4 months after COVID-19: First results from the national prospective observational Swiss COVID-19 lung study. Eur. Respir. J. 2021, 57, 2003690. [Google Scholar] [CrossRef] [PubMed]
- Sibila, O.; Perea, L.; Albacar, N.; Moises, J.; Cruz, T.; Mendoza, N.; Solarat, B.; Lledo, G.; Espinosa, G.; Barbera, J.A.; et al. Elevated plasma levels of epithelial and endothelial cell markers in COVID-19 survivors with reduced lung diffusing capacity six months after hospital discharge. Respir. Res. 2022, 23, 37. [Google Scholar] [CrossRef] [PubMed]
- Fan, B.E.; Wong, S.W.; Sum, C.L.L.; Lim, G.H.; Leung, B.P.; Tan, C.W.; Ramanathan, K.; Dalan, R.; Cheung, C.; Lim, X.R.; et al. Hypercoagulability, endotheliopathy, and inflammation approximating 1 year after recovery: Assessing the long-term outcomes in COVID-19 patients. Am. J. Hematol. 2022, 97, 915–923. [Google Scholar] [CrossRef]
- Kozlowski, P.; Smiarowski, M.; Przyborska, W.; Zemlik, K.; Malecka-Gieldowska, M.; Leszczynska, A.; Garley, M.; Ciepiela, O. Mild-to-Moderate COVID-19 Convalescents May Present Pro-Longed Endothelium Injury. J. Clin. Med. 2022, 11, 6461. [Google Scholar] [CrossRef]
- Mitrović-Ajtić, O.; Djikić, D.; Subotički, T.; Bižić-Radulović, S.; Beleslin-Čokić, B.; Dragojević, T.; Živković, E.; Miljatović, S.; Čokić, V. Sex Difference in the Cytokine Profile among Patients Hospitalized for COVID-19 and during Their Recovery: Predominance of Females in Adhesion Molecules and Males in Oxidative Stress. 2022; Pre-Print. Available online: https://assets.researchsquare.com/files/rs-2355363/v1/03b2c2d3-7717-473c-aedb-01abcbba5a93.pdf?c=1674560543(accessed on 20 June 2023).
- Tong, M.; Yan, X.; Jiang, Y.; Jin, Z.; Zhu, S.; Zou, L.; Liu, Y.; Zheng, Q.; Chen, G.; Gu, R.; et al. Endothelial Biomarkers in Patients Recovered from COVID-19 One Year after Hospital Discharge: A Cross-Sectional Study. Mediterr. J. Hematol. Infect. Dis. 2022, 14, e2022033. [Google Scholar] [CrossRef]
- Haffke, M.; Freitag, H.; Rudolf, G.; Seifert, M.; Doehner, W.; Scherbakov, N.; Hanitsch, L.; Wittke, K.; Bauer, S.; Konietschke, F.; et al. Endothelial dysfunction and altered endothelial biomarkers in patients with post-COVID-19 syndrome and chronic fatigue syndrome (ME/CFS). J. Transl. Med. 2022, 20, 138. [Google Scholar] [CrossRef]
- Belli, S.; Balbi, B.; Prince, I.; Cattaneo, D.; Masocco, F.; Zaccaria, S.; Bertalli, L.; Cattini, F.; Lomazzo, A.; Dal Negro, F.; et al. Low physical functioning and impaired performance of activities of daily life in COVID-19 patients who survived hospitalisation. Eur. Respir. J. 2020, 56, 2002096. [Google Scholar] [CrossRef]
- Gloeckl, R.; Leitl, D.; Jarosch, I.; Schneeberger, T.; Nell, C.; Stenzel, N.; Vogelmeier, C.F.; Kenn, K.; Koczulla, A.R. Benefits of pulmonary rehabilitation in COVID-19: A prospective observational cohort study. ERJ Open Res. 2021, 7, 00108-2021. [Google Scholar] [CrossRef] [PubMed]
- Camarri, B.; Eastwood, P.R.; Cecins, N.M.; Thompson, P.J.; Jenkins, S. Six minute walk distance in healthy subjects aged 55–75 years. Respir. Med. 2006, 100, 658–665. [Google Scholar] [CrossRef] [PubMed]
- Newton, D.J.; Kennedy, G.; Chan, K.K.; Lang, C.C.; Belch, J.J.; Khan, F. Large and small artery endothelial dysfunction in chronic fatigue syndrome. Int. J. Cardiol. 2012, 154, 335–336. [Google Scholar] [CrossRef] [PubMed]
- Dunmore, B.J.; Upton, P.D.; Auckland, K.; Samanta, R.J.; Lyons, P.A.; Smith, K.G.C.; Gräf, S.; Summers, C.; Morrell, N.W.; CITIID-NIHR BioResource COVID-19 Collaboration; et al. Reduced circulating BMP9 and pBMP10 in hospitalized COVID-19 patients. Pulm. Circ. 2023, 13, e12192. [Google Scholar] [CrossRef]
- Vitiello, A.; Ferrara, F. Correlation between renin-angiotensin system and Severe Acute Respiratory Syndrome Coronavirus 2 infection: What do we know? Eur. J. Pharmacol. 2020, 883, 173373. [Google Scholar] [CrossRef]
- Spadaro, S.; Fogagnolo, A.; Campo, G.; Zucchetti, O.; Verri, M.; Ottaviani, I.; Tunstall, T.; Grasso, S.; Scaramuzzo, V.; Murgolo, F.; et al. Markers of endothelial and epithelial pulmonary injury in mechanically ventilated COVID-19 ICU patients. Crit. Care 2021, 25, 74. [Google Scholar] [CrossRef]
- Fogarty, H.; Ward, S.E.; Townsend, L.; Karampini, E.; Elliott, S.; Conlon, N.; Dunne, J.; Kiersey, R.; Naughton, A.; Gardiner, M.; et al. Sustained VWF-ADAMTS-13 axis imbalance and endotheliopathy in long COVID syndrome is related to immune dysfunction. J. Thromb. Haemost. 2022, 20, 2429–2438. [Google Scholar] [CrossRef] [PubMed]
- Turner, S.; Naidoo, C.A.; Usher, T.J.; Kruger, A.; Venter, C.; Laubscher, G.J.; Khan, M.A.; Kell, D.B.; Pretorius, E. Increased Levels of Inflammatory and Endothelial Biomarkers in Blood of Long COVID Patients Point to Thrombotic Endothelialitis. Semin. Thromb. Hemost. 2023. [Google Scholar] [CrossRef] [PubMed]
- Bayraktar, N.; Bayraktar, M.; Ozturk, A.; Ibrahim, B. Evaluation of the Relationship Between Aquaporin-1, Hepcidin, Zinc, Copper, and İron Levels and Oxidative Stress in the Serum of Critically Ill Patients with COVID-19. Biol. Trace Elem. Res. 2022, 200, 5013–5021. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Endothelial Biomarkers | Intra-Assay Coefficient of Variability (CV) (%) | Detection Limit | Manufacturer |
|---|---|---|---|
| sE-selectin | 5.9 | 0.027 ng/mL | R&D Systems Inc., Thermofisher scientific, Waltham, MA, USA |
| Ang-2 | 5.9 | 21.3 pg/mL | R&D Systems Inc., Thermofisher scientific, Waltham, MA, USA |
| sICAM-1 | 4.6 | 0.254 ng/mL | R&D Systems Inc., Thermofisher scientific, Waltham, MA, USA |
| sVCAM-1 | 3.1 | 1.26 ng/mL | R&D Systems Inc., Thermofisher scientific, Waltham, MA, USA |
| sEPCR | 5.8 | 0.3 ng/mL | R&D Systems Inc., Thermofisher scientific, Waltham, MA, USA |
| eNOS | 4.2 | 25 pg/mL | R&D Systems Inc., Thermofisher scientific, Waltham, MA, USA |
| Plasminogen | <8 | 46.875 pg/mL | Fine Biotech Co., Wuhan, China |
| ESM-1 | 6.3 | <10 pg/mL | OriGene Technologies, Inc., Rockville, MD, USA |
| vWf | 5.2 | <50 pg/mL | OriGene Technologies, Inc., Rockville, MD, USA |
| sACE2 | 4.8 | <10 pg/mL | OriGene Technologies, Inc., Rockville, MD, USA |
| BMP9 | 4.8 | <10 pg/mL | OriGene Technologies, Inc., Rockville, MD, USA |
| Aqp1 | 4.5 | 75 pg/mL | Assay Genie, Dublin, Ireland |
| sACE | 1.4 | 2.4 U/L | Sentinel Diagnostics, Milan, Italy |
| Characteristics | Long COVID Patients |
|---|---|
| Number of patients, N | 68 |
| Age (years), (median, IQR) | 56 (46–63) |
| Sex, N (%) | |
| Male | 38 (55.9%) |
| Female | 30 (44.1%) |
| Days after positive-test, (median, IQR) | 139 (86–350) |
| Hospitalized, N (%) | |
| ICU | 35 (51.5%) |
| Mechanical ventilation | 32 (91.4%) |
| High-flow oxygen therapy | 3 (8.6%) |
| Ward | 15 (22.0%) |
| Outpatients | 18 (26.5%) |
| Hospitalization days, (median, IQR) | 33 (19–55) |
| BMI (kg/m2), (median, IQR) | 29.0 (24.9–33.1) |
| Smoking/Ex-smoking habit, N (%) | |
| Yes | 20 (29.4%) |
| No | 48 (70.6%) |
| Comorbidities, N (%) | 32 (47.1%) |
| Hyperlipidemia | 13 |
| Hypertension | 10 |
| Diabetes | 7 |
| COPD | 7 |
| Coronary artery disease | 3 |
| Chronic renal failure | 1 |
| Symptoms during acute COVID-19, N (%) | |
| Fever | 61 (89.7%) |
| Cough | 35 (51.4%) |
| Dyspnea | 24 (35.3%) |
| Fatigue | 20 (29.4%) |
| Arthralgia/Myalgia | 17 (25.0%) |
| Loss of taste/smell | 15 (22.1%) |
| Diarrhea | 14 (20.6%) |
| Headache | 14 (20.6%) |
| Laboratory data | |
| CRP (mg/dL), (median, IQR) | 0.2 (0.1–0.3) |
| D-dimers (µg/mL), (median, IQR) | 0.32 (0.24–0.57) |
| LDH (U/L), (median, IQR) | 183 ± 36 |
| Creatinine (mg/dL), (median, IQR) | 0.8 (0.7–0.9) |
| Platelets (per μL), (median, IQR) | 241,000 (207,000–270,000 |
| White blood cell count (per μL), (mean ± SD) | 6116 ± 1615 |
| Neutrophils (%), (mean ± SD) | 55.5 ± 7.9 |
| Lymphocytes (%), (mean ± SD) | 34.4 ± 7.4 |
| Fatigue, dyspnea, 6-min walk, diffusion capacity, and spirometry | |
| FAS scale, (median, IQR) | 22 (16–30) |
| mMRC dyspnea scale (median, IQR) | 2 (1–3) |
| 6MWT (meters), (median, IQR) | 474 (378–558) |
| DLCO %pred., (mean ± SD) | 67 ± 18.6% |
| FEV1 %pred., (median, IQR) | 94.3 (81.6–105.0) |
| FVC %pred., (median, IQR) | 93.8 (80.1–102.7) |
| FEV-1/FVC (median, IQR) | 84.0 (81.1–87.4) |
| Endothelial biomarkers | |
| sE-selectin (ng/mL), (median, IQR) | 29.9 (21.2–36.7) |
| sICAM-1 (ng/mL), (median, IQR) | 286.3 (191.9–428.1) |
| sVCAM-1 (ng/mL), (median, IQR) | 676.1 (507.6–901.0) |
| Ang-2 (ng/mL), (median, IQR) | 3.8 (2.2–5.9) |
| ESM-1 (pg/mL), (median, IQR) | 501.4 (426.6–693.9) |
| vWf (pg/mL), (median, IQR) | 6862 (6574–7241) |
| Plasminogen (pg/mL), (median, IQR) | 1,680,182 (1,312,186–2,309,512) |
| sEPCR (ng/mL), (median, IQR) | 164.8 (54.2–268.5) |
| eNOS (pg/mL), (median, IQR) | 149.8 (62.9–338.0) |
| sACE (U/l), (median, IQR) | 58 (39–83) |
| sACE2 (pg/mL), (median, IQR) | 1219 (661–1710) |
| BMP9 (pg/mL), (median, IQR) | 10.6 (8.8–27.8) |
| Aqp1 (pg/mL), (median, IQR) | 1622 (956–2837) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asimakos, A.T.; Vassiliou, A.G.; Keskinidou, C.; Spetsioti, S.; Antonoglou, A.; Vrettou, C.S.; Mourelatos, P.; Diamantopoulos, A.; Pratikaki, M.; Athanasiou, N.; et al. Persistent Endothelial Lung Damage and Impaired Diffusion Capacity in Long COVID. J. Pers. Med. 2023, 13, 1351. https://doi.org/10.3390/jpm13091351
Asimakos AT, Vassiliou AG, Keskinidou C, Spetsioti S, Antonoglou A, Vrettou CS, Mourelatos P, Diamantopoulos A, Pratikaki M, Athanasiou N, et al. Persistent Endothelial Lung Damage and Impaired Diffusion Capacity in Long COVID. Journal of Personalized Medicine. 2023; 13(9):1351. https://doi.org/10.3390/jpm13091351
Chicago/Turabian StyleAsimakos, Andreas T., Alice G. Vassiliou, Chrysi Keskinidou, Stavroula Spetsioti, Archontoula Antonoglou, Charikleia S. Vrettou, Panagiotis Mourelatos, Aristidis Diamantopoulos, Maria Pratikaki, Nikolaos Athanasiou, and et al. 2023. "Persistent Endothelial Lung Damage and Impaired Diffusion Capacity in Long COVID" Journal of Personalized Medicine 13, no. 9: 1351. https://doi.org/10.3390/jpm13091351