
Evaluation of Intraoperative Volumetric Assessment of Breast Volume Using 3D Handheld Stereo Photogrammetric Device

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Study Population
2.2. Patient Selection
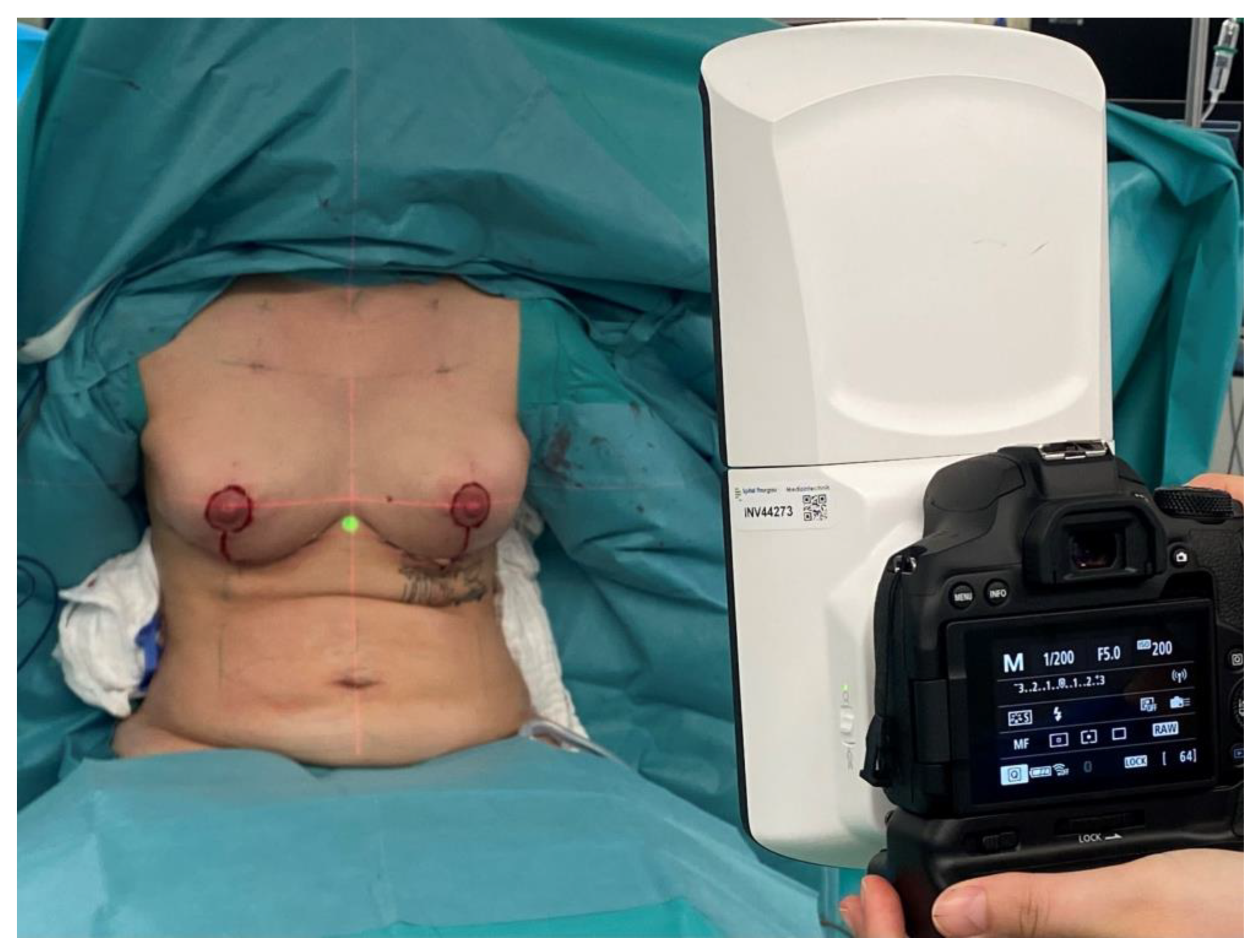
2.3. Surgical Technique
2.4. Three-Dimensional (3D) Volumetric Assessment
2.5. Postoperative Three-Dimensional (3D) Volumetric Assessment
2.6. Data Collection, Statistical Analysis, and Literature Review
3. Results
3.1. Patients and Demographics
3.2. Volumetric Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Onesti, M.G.; Mezzana, P.; Martano, A.; Scuderi, N. Breast asymmetry: A new vision of this malformation. Acta Chir. Plast. 2004, 46, 8–11. [Google Scholar]
- Godden, A.R.; O’connell, R.L.; Barry, P.A.; Krupa, K.C.D.; Wolf, L.M.; Mohammed, K.; Kirby, A.M.; Rusby, J.E. 3-Dimensional objective aesthetic evaluation to replace panel assessment after breast-conserving treatment. Breast Cancer 2020, 27, 1126–1136. [Google Scholar] [CrossRef]
- Cardoso, M.J.; Oliveira, H.; Cardoso, J. Assessing cosmetic results after breast conserving surgery. J. Surg. Oncol. 2014, 110, 37–44. [Google Scholar] [CrossRef]
- Westreich, M. Anthropomorphic breast measurement: Protocol and results in 50 women with aesthetically perfect breasts and clinical application. Plast. Reconstr. Surg. 1997, 100, 468–479. [Google Scholar] [CrossRef]
- Smith, D.J., Jr.; Palin, W.E., Jr.; Katch, V.L.; Bennett, J.E. Breast volume and anthropomorphic measurements: Normal values. Plast. Reconstr. Surg. 1986, 78, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Stark, B.; Olivari, N. Breast asymmetry: An objective analysis of postoperative results. Eur. J. Plast. Surg. 1991, 14, 173–176. [Google Scholar] [CrossRef]
- Loucas, R.; Loucas, M.; Leitsch, S.; Mayer, J.M.; Alberti, A.; Haroon, O.; Petrus, M.; Koban, K.C.; Holzbach, T. How Useful Is the SSN–Nipple Distance? An Analytical Questionnaire Survey on Anthropometric Measurements for the Aesthetically Ideal Positioning of the Nipple–Areolar Complex. J. Clin. Med. 2023, 12, 2494. [Google Scholar] [CrossRef]
- Herold, C.; Reichelt, A.; Stieglitz, L.H.; Dettmer, S.; Knobloch, K.; Lotz, J.; Vogt, P.M. MRI-based breast volumetry—Evaluation of three different software solutions. J. Digit. Imaging 2010, 23, 603–610. [Google Scholar] [CrossRef]
- Neal, A.; Torr, M.; Helyer, S.; Yarnold, J. Correlation of breast dose heterogeneity with breast size using 3D CT planning and dose-volume histograms. Radiother. Oncol. 1995, 34, 210–218. [Google Scholar] [CrossRef]
- Rudolph, R.; Forcier, N. Calculation of silicone breast implant volumes using breast magnetic resonance imaging. Aesthet. Surg. J. 2009, 29, 310–313. [Google Scholar] [CrossRef]
- Pozzobon, A.V.; Neto, M.S.; Veiga, D.F.; Abla, L.E.F.; Pereira, J.B.; Biasi, T.L.; Ferreira, L.M.; Yamashita, L.A.; Kawano, F.; Nakano, E.M.; et al. Magnetic resonance images and linear measurements in the surgical treatment of breast asymmetry. Aesthet. Plast. Surg. 2009, 33, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Tezel, E.; Numanoglu, A. Practical do-it-yourself device for accurate volume measurement of breast. Plast. Reconstr. Surg. 2000, 105, 1019–1023. [Google Scholar] [CrossRef] [PubMed]
- Wilkie, T.; Ship, A.G. Volumetric breast measurement during surgery. Aesthet. Plast. Surg. 1976, 1, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Tegtmeier, R.E. A quick, accurate mammometer. Ann. Plast. Surg. 1978, 1, 625–626. [Google Scholar] [CrossRef]
- Holzbach, T. Laser Level Projection: A Helpful Tool for Preoperative Markings. Plast. Reconstr. Surg. 2023, 151, 348e–350e. [Google Scholar] [CrossRef]
- Holzbach, T.; Linder, S.; Leitsch, S.; Loucas, R.; Loucas, M.; Giunta, R.E.; Mayer, J. Improving symmetry of nipple–areola complex (NAC) position in reduction mammoplasty using laser level projection. J. Plast. Reconstr. Aesthet. Surg. 2023, 77, 284–290. [Google Scholar] [CrossRef]
- Campaigne, B.; Katch, V.; Freedson, P.; Sady, S.; Katch, F. Measurement of breast volume in females: Description of a reliable method. Ann. Hum. Biol. 1979, 6, 363–367. [Google Scholar] [CrossRef]
- Edsander-Nord, Å.; Wickman, M.; Jurell, G. Measurement of breast volume with thermoplastic casts. Scand. J. Plast. Reconstr. Surg. Hand Surg. 1996, 30, 129–132. [Google Scholar] [CrossRef]
- Kovacs, L.; Eder, M.; Hollweck, R. Comparison between breast volume measurement using 3D surface imaging and classical techniques. Breast 2006, 6, 137–145. [Google Scholar] [CrossRef]
- Kovacs, L.; Yassouridis, A.; Zimmermann, A.; Brockmann, G.; Wöhnl, A.; Blaschke, M.; Eder, M.; Schwenzer-Zimmerer, K.; Rosenberg, R.; Papadopulos, N.A.; et al. Optimization of 3-dimensional imaging of the breast region with 3-dimensional laser scanners. Ann. Plast. Surg. 2006, 56, 229–236. [Google Scholar] [CrossRef]
- Losken, A.; Seify, H.; Denson, D.D.; Paredes, A.A.; Carlson, G.W. Validating three-dimensional imaging of the breast. Ann. Plast. Surg. 2005, 54, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Nahabedian, M.Y.; Galdino, G. Symmetrical breast reconstruction: Is there a role for three-dimensional digital photography? Plast. Reconstr. Surg. 2003, 112, 1582–1590. [Google Scholar] [CrossRef]
- Tepper, O.M.; Small, K.; Rudolph, L.; Choi, M.; Karp, N. Virtual 3-dimensional modeling as a valuable adjunct to aesthetic and reconstructive breast surgery. Am. J. Surg. 2006, 192, 548–551. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Rokohl, A.C.; Guo, Y.; Li, S.; Hou, X.; Fan, W.; Formuzal, M.; Lin, M.; Heindl, L.M. Reliability of Stereophotogrammetry for Area Measurement in the Periocular Region. Aesthet. Plast. Surg. 2021, 45, 1601–1610. [Google Scholar] [CrossRef]
- Guridi, R.; Rodriguez, J.R. A Step-by-Step Approach to a Successful Cosmetic Breast Reduction. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2117. [Google Scholar] [CrossRef]
- Tebbetts, J.B. A process for quantifying aesthetic and functional breast surgery: I. Quantifying optimal nipple position and vertical and horizontal skin excess for mastopexy and breast reduction. Plast. Reconstr. Surg. 2013, 132, 65–73. [Google Scholar] [CrossRef]
- O’connell, R.L.; Di Micco, R.; Khabra, K.; Wolf, L.; Desouza, N.; Roche, N.; Barry, P.A.; Kirby, A.M.; Rusby, J.E. The potential role of three-dimensional surface imaging as a tool to evaluate aesthetic outcome after Breast Conserving Therapy (BCT). Breast Cancer Res. Treat. 2017, 164, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Henseler, H.; Khambay, B.S.; Bowman, A.; Smith, J.; Siebert, J.P.; Oehler, S.; Ju, X.; Ayoub, A.; Ray, A.K. Investigation into accuracy and reproducibility of a 3D breast imaging system using multiple stereo cameras. J. Plast. Reconstr. Aesthet. Surg. 2011, 64, 577–582. [Google Scholar] [CrossRef]
- Koch, M.C.; Adamietz, B.; Jud, S.M.; Fasching, P.A.; Haeberle, L.; Karbacher, S.; Veit, K.; Schulz-Wendtland, R.; Uder, M.; Beckmann, M.W.; et al. Breast Volumetry Using a Three-Dimensional Surface Assessment Technique. Aesthet. Plast. Surg. 2011, 35, 847–855. [Google Scholar] [CrossRef]
- Lewis, P.; Mattison, G.; Kim, H.; Gupta, S. Evaluation of 3D photographic imaging to measure differential volumes in reconstructed breast tissue. In Journal of Investigative Medicine; Lippincott Williams & Wilkins 530 Walnut St.: Philadelphia, PA, USA, 2014. [Google Scholar]
- Veitch, D.; Burford, K.; Dench, P.; Dean, N.; Griffin, P. Measurement of breast volume using body scan technology(computer-aided anthropometry). Work 2012, 41 (Suppl. S1), 4038–4045. [Google Scholar] [CrossRef]
- Yip, J.M.; Mouratova, N.; Jeffery, R.M.; Veitch, D.E.; Woodman, R.J.; Dean, N.R. Accurate assessment of breast volume: A study comparing the volumetric gold standard (direct water displacement measurement of mastectomy specimen) with a 3D laser scanning technique. Ann. Plast. Surg. 2012, 68, 135–141. [Google Scholar] [CrossRef]
- Hidalgo, D.A.; Sinno, S. Current Trends and Controversies in Breast Augmentation. Plast. Reconstr. Surg. 2016, 137, 1142–1150. [Google Scholar] [CrossRef] [PubMed]
- O’connell, R.L.; Khabra, K.; Bamber, J.C.; Desouza, N.; Meybodi, F.; Barry, P.A.; Rusby, J.E. Validation of the Vectra XT three-dimensional imaging system for measuring breast volume and symmetry following oncological reconstruction. Breast Cancer Res. Treat. 2018, 171, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Mu, D.; Xu, B.; Li, W.; Zhang, X.; Lin, Y.; Li, H. An Intraoperative Measurement Method of Breast Symmetry Using Three-Dimensional Scanning Technique in Reduction Mammaplasty. Aesthet. Plast. Surg. 2021, 45, 2135–2145. [Google Scholar] [CrossRef]
- Bai, L.; Lundström, O.; Johansson, H.; Meybodi, F.; Arver, B.; Sandelin, K.; Wickman, M.; Brandberg, Y. Clinical assessment of breast symmetry and aesthetic outcome: Can 3D imaging be the gold standard? J. Plast. Surg. Hand Surg. 2023, 57, 145–152. [Google Scholar] [CrossRef]
- Lopez, X.; Panton, J.; Nagarkar, P.; Preston, S.; Abramowitz, J.; Amirlak, B. Initial Assessment of VECTRA Three-Dimensional Imaging to Accurately Simulate Breast Volume Changes in Transfeminine Patients: A Mannequin Study. Aesthet. Surg. J. Open Forum 2023, 5, ojad015. [Google Scholar] [CrossRef]
- Adham, M.; Sawan, K.; Lovelace, C.; Jaeger, N.J.; Adham, C. Unfavorable outcomes with vertical reduction mammaplasty: Part II. Aesthet. Surg. J. 2011, 31, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Garcia, O. Management of Asymmetry After Breast Reduction. Clin. Plast. Surg. 2016, 43, 373–382. [Google Scholar] [CrossRef]
- Eder, M.; Waldenfels, F.V.; Sichtermann, M.; Schuster, T.; Papadopulos, N.A.; Machens, H.-G.; Biemer, E.; Kovacs, L. Three-dimensional evaluation of breast contour and volume changes following subpectoral augmentation mammaplasty over 6 months. J. Plast. Reconstr. Aesthet. Surg. 2011, 64, 1152–1160. [Google Scholar] [CrossRef]
- Creasman, C.N.; Mordaunt, D.; Liolios, T.; Chiu, C.; Gabriel, A.; Maxwell, G.P. Four-dimensional breast imaging, part II: Clinical implementation and validation of a computer imaging system for breast augmentation planning. Aesthet. Surg. J. 2011, 31, 925–938. [Google Scholar] [CrossRef]
- Eder, M.; Waldenfels, F.V.; Swobodnik, A.; Klöppel, M.; Pape, A.-K.; Schuster, T.; Raith, S.; Kitzler, E.; Papadopulos, N.A.; Machens, H.-G.; et al. Objective breast symmetry evaluation using 3-D surface imaging. Breast 2012, 21, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Krois, W.; Romar, A.K.; Wild, T.; Dubsky, P.; Exner, R.; Panhofer, P.; Jakesz, R.; Gnant, M.; Fitzal, F. Objective breast symmetry analysis with the breast analyzing tool (BAT): Improved tool for clinical trials. Breast Cancer Res. Treat. 2017, 164, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, M.J.; Cardoso, J.; Amaral, N.; Azevedo, I.; Barreau, L.; Bernardo, M.; Christie, D.; Costa, S.; Fitzal, F.; Fougo, J.L.; et al. Turning subjective into objective: The BCCT. core software for evaluation of cosmetic results in breast cancer conservative treatment. Breast 2007, 16, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, J.S.; Cardoso, M.J. Towards an intelligent medical system for the aesthetic evaluation of breast cancer conservative treatment. Artif. Intell. Med. 2007, 40, 115–126. [Google Scholar] [CrossRef]
- De Stefani, A.; Barone, M.; Alamdari, S.H.; Barjami, A.; Baciliero, U.; Apolloni, F.; Gracco, A.; Bruno, G. Validation of Vectra 3D Imaging Systems: A Review. Int. J. Environ. Res. Public Health 2022, 19, 8820. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patients Mean ± Std (Min, Max) | |
|---|---|
| Age at surgery | 48.34 ± 14.73 (20; 89), n = 103 |
| Gender | 103 Female |
| Side (Uni/Bilateral) | 103 Bilateral |
| Body Mass Index | 24.65 ± 3.88 (16.52; 38.26), n = 103 |
| Diabetes | 6/103 |
| Patients | p Value | |
|---|---|---|
| Intraoperative three-dimensional (3D) volumetric measurement | 507.11 ± 206.29 cc n = 103 | - |
| Postoperative three-dimensional (3D) volumetric measurement | 504.24 ± 276.61 cc n = 103 | - |
| Mean absolute volume difference between intraoperative simulations and postoperative results | 27.1 ± 20.7 (0.9; 83.5) n = 103 | 0.68 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loucas, R.; Loucas, M.; Leitsch, S.; Danuser, K.; Reichard, G.; Haroon, O.; Mayer, J.M.; Koban, K.; Holzbach, T. Evaluation of Intraoperative Volumetric Assessment of Breast Volume Using 3D Handheld Stereo Photogrammetric Device. J. Pers. Med. 2023, 13, 1262. https://doi.org/10.3390/jpm13081262
Loucas R, Loucas M, Leitsch S, Danuser K, Reichard G, Haroon O, Mayer JM, Koban K, Holzbach T. Evaluation of Intraoperative Volumetric Assessment of Breast Volume Using 3D Handheld Stereo Photogrammetric Device. Journal of Personalized Medicine. 2023; 13(8):1262. https://doi.org/10.3390/jpm13081262
Chicago/Turabian StyleLoucas, Rafael, Marios Loucas, Sebastian Leitsch, Katarina Danuser, Gabriela Reichard, Omar Haroon, Julius Michael Mayer, Konstantin Koban, and Thomas Holzbach. 2023. "Evaluation of Intraoperative Volumetric Assessment of Breast Volume Using 3D Handheld Stereo Photogrammetric Device" Journal of Personalized Medicine 13, no. 8: 1262. https://doi.org/10.3390/jpm13081262