
Framing Patellar Instability: From Diagnosis to the Treatment of the First Episode

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Classification of Patellofemoral Disorders
- Objective patellar instability: Patients have experienced at least one episode of patellar dislocation and present at least one or more principal factors of instability. Patellar dislocation can occur during high-energy activities such as sports and is frequently associated with hemarthrosis.
- Potential patellar instability: Patients never experienced a true patellar dislocation, although they report a rather generic feeling of instability. It may occur daily during low-demand activities, such as walking and climbing stairs. These patients present one or more principal factors of instability.
- Patellofemoral pain syndrome: Pain is the main symptom, and it is mostly attributed to cartilage wear on either the patellar or femoral side. Imaging does not show any evident factor of instability, nor can a clinical episode of patellar dislocation be identified. In subjects suffering from patellofemoral pain (PFP) syndrome, exercise therapy should be considered the first-line treatment option as it is considered the “treatment of choice” and is supported by high-level evidence. Such therapy should include exercises for strengthening the hip and knee; these exercises can be performed through kinetic chain exercises (either weight-bearing or non-weight-bearing). Additionally, joint mobilization targeted at the knee, patellofemoral taping, and neuromuscular training have also been suggested as second-line treatment options to be used in conjunction with exercise therapy [8].
3. Principal Factors of Instability
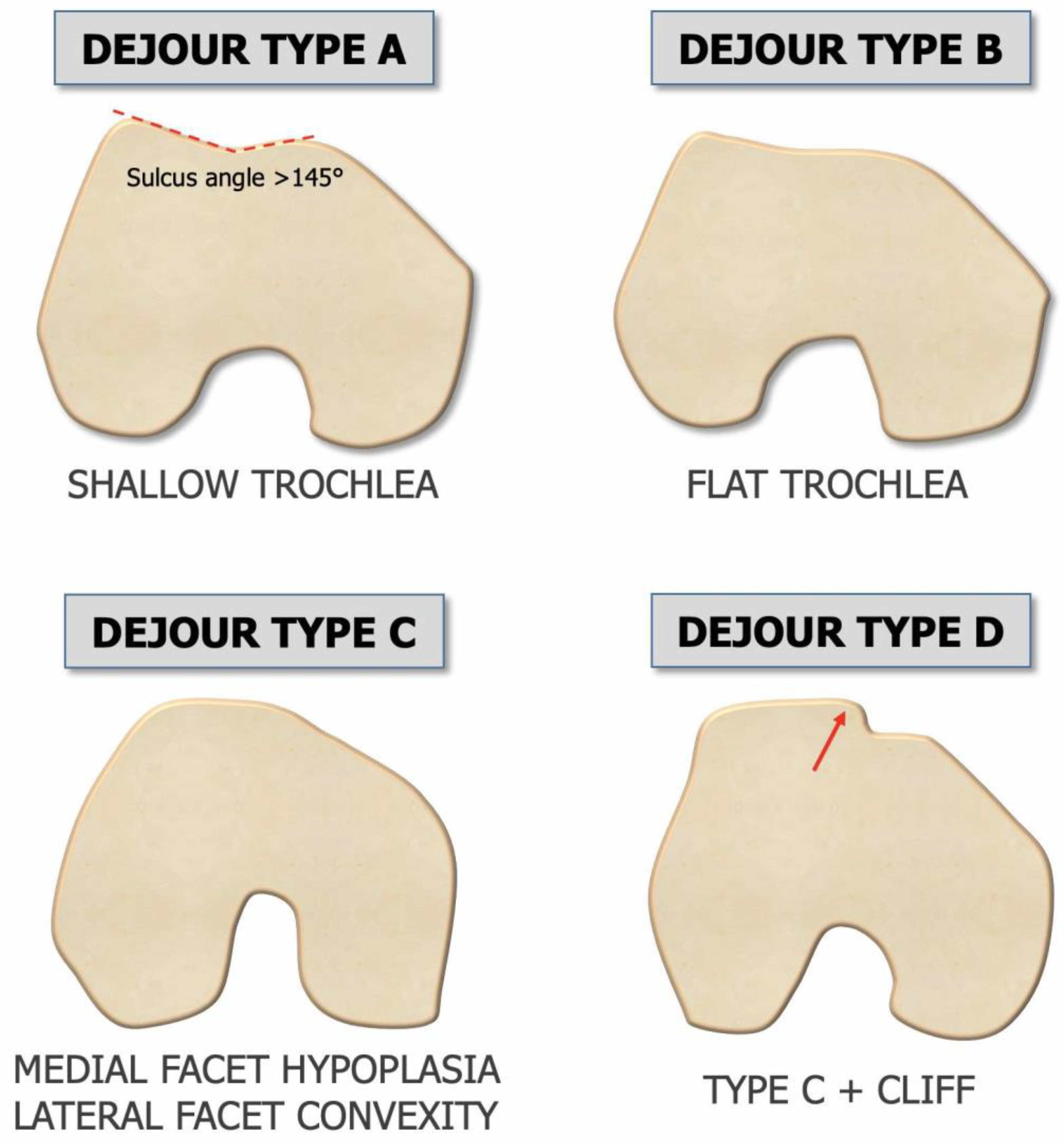
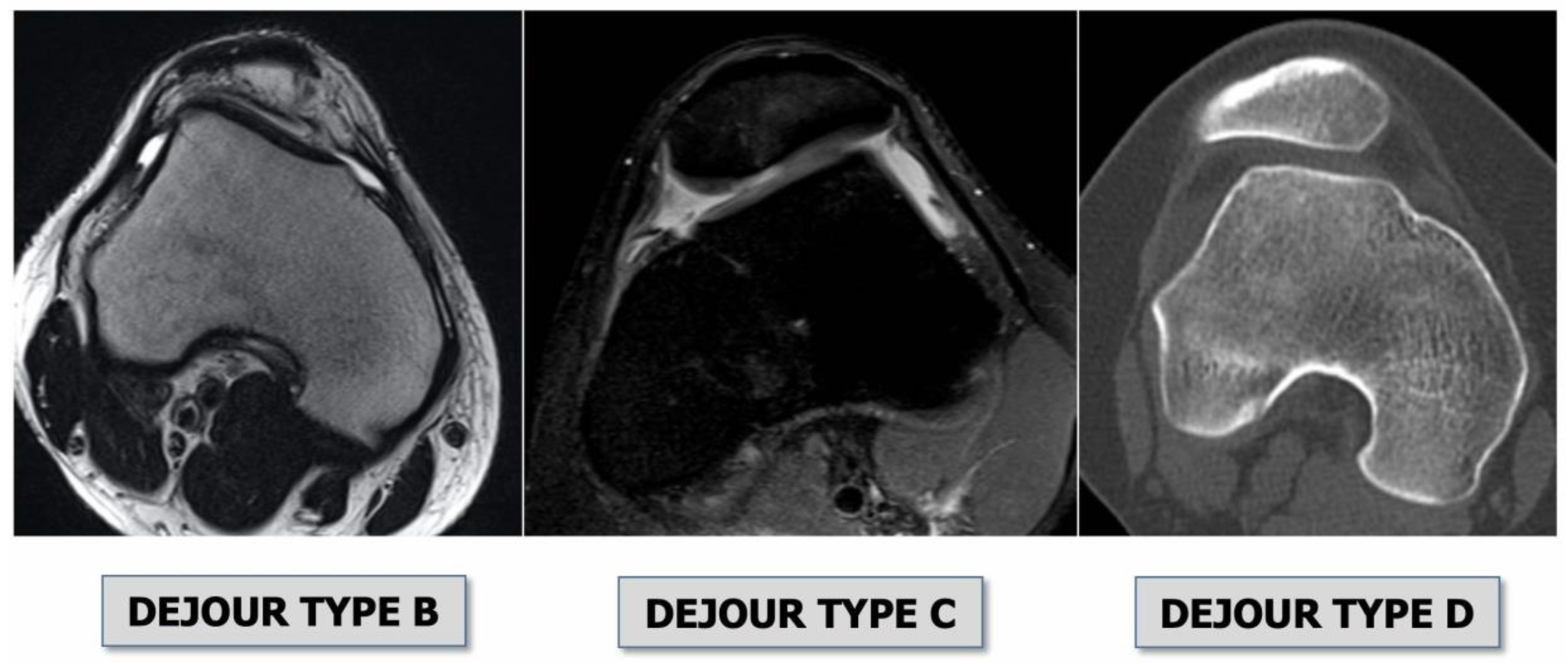
- Trochlear dysplasia indicates whether the femoral trochlea is flat or convex (instead of concave), causing abnormal patellar tracking and a loss of joint congruence (Figure 1 and Figure 2). Dejour classified trochlear dysplasia into four groups [9]. This classification system requires an accurate lateral X-ray (congruent posterior condyles) and confirmation via axial imaging of the knee (CT scan or MRI). A certain degree of trochlear dysplasia was found in up to 96% of patients with objective or potential patellar instability [7].
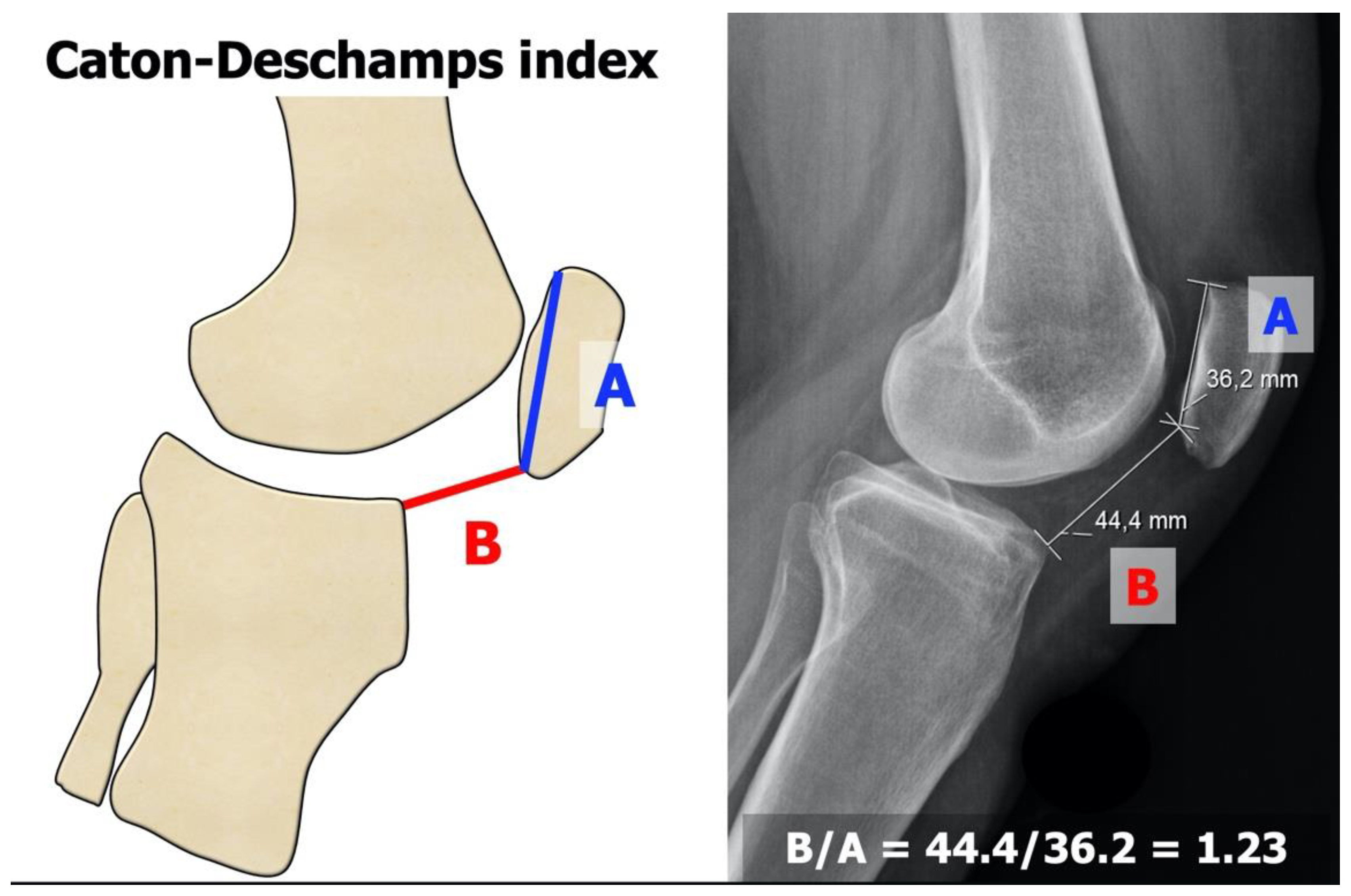
- Patella alta is defined as an excessive patellar height that prevents or limits patellar engagement on the trochlea during flexion, thus predisposing the patient to patellofemoral instability. It is easily measured using the Caton–Deschamps Index (CDI) on an accurate lateral knee X-ray [10,11]. It is pathological when the CDI is greater than or equal to 1.2 (Figure 3). It is present in 30% of patellar dislocations [12].
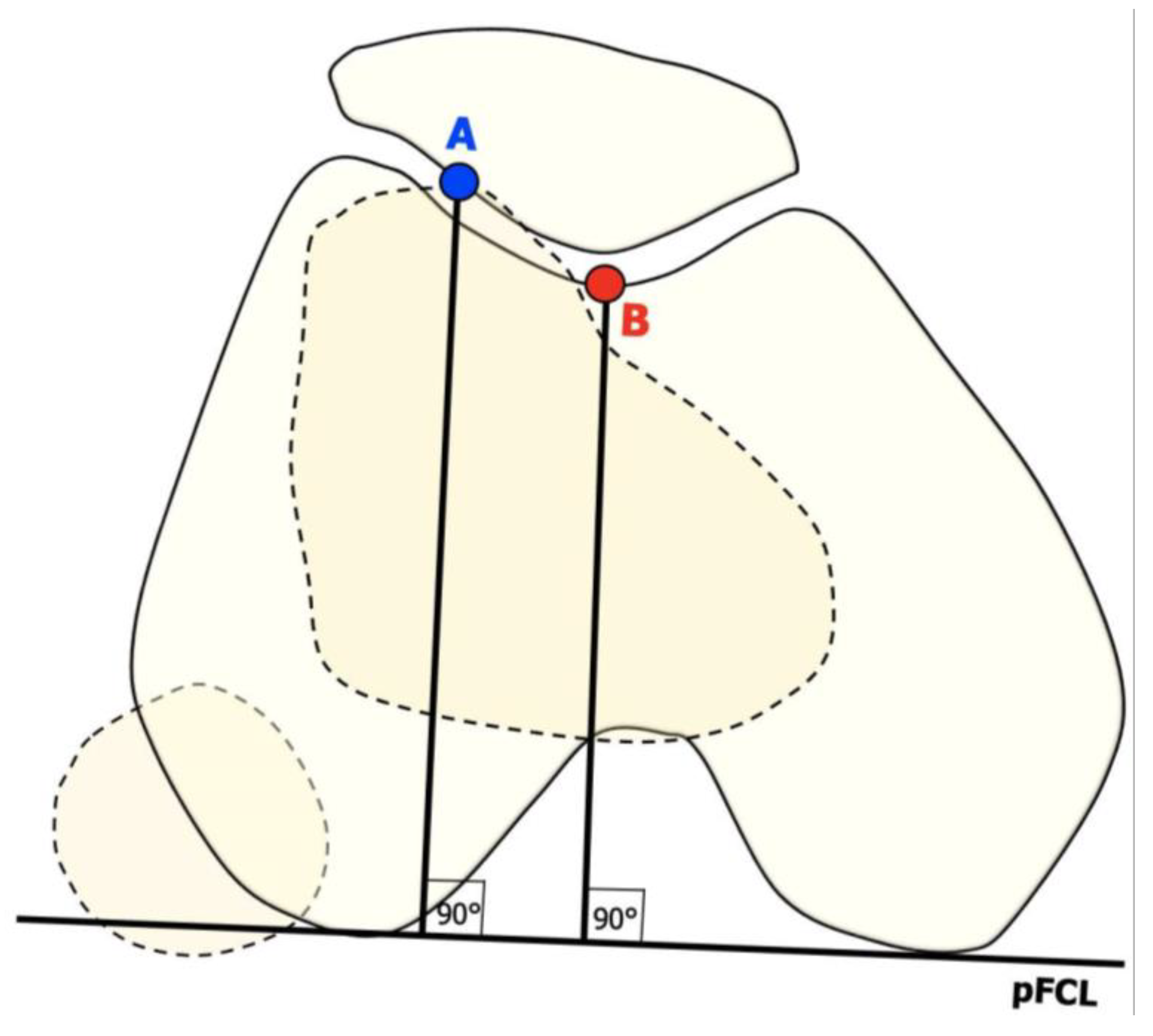
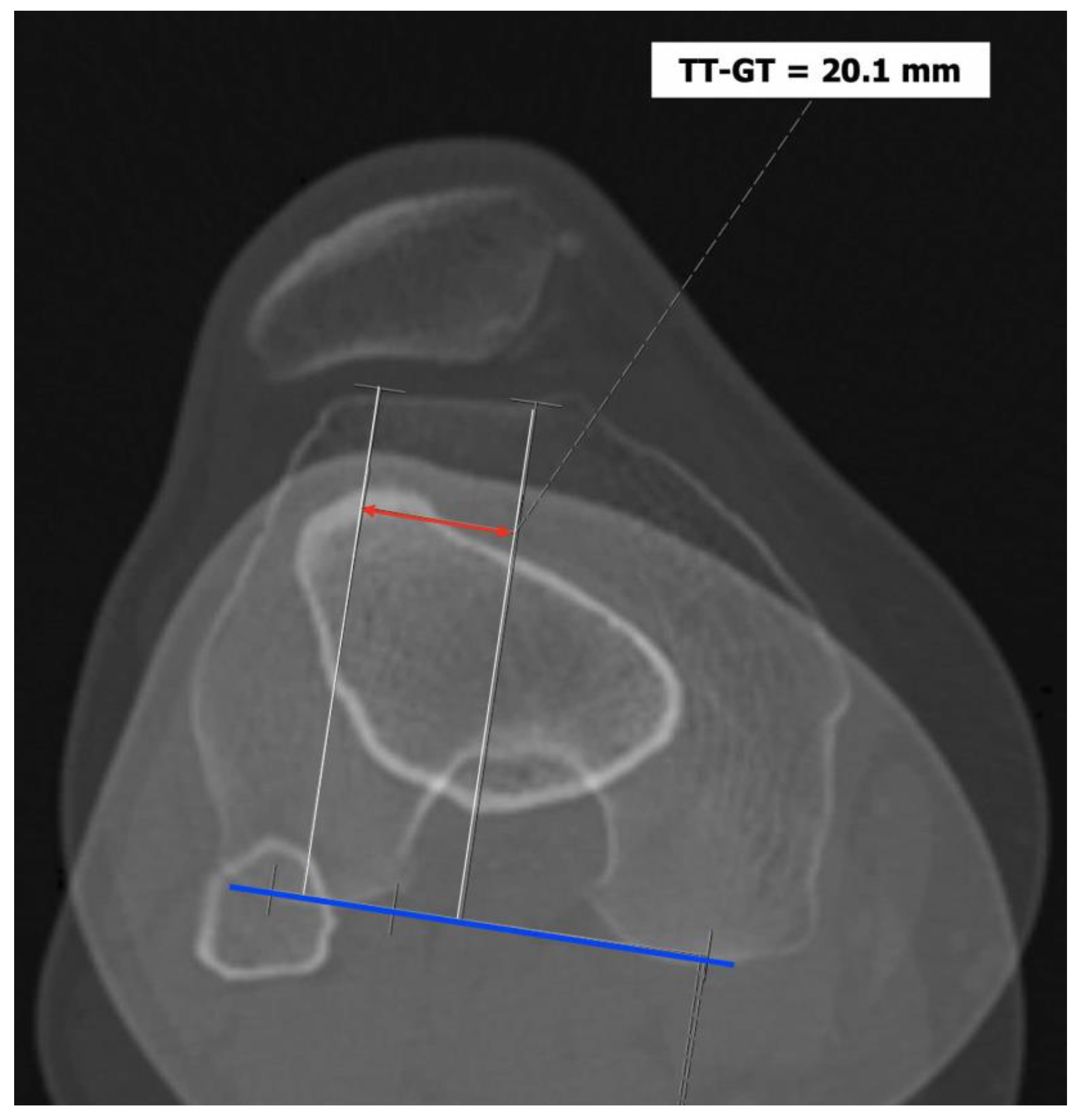
- The tibial tuberosity-trochlear groove (TT-TG) distance [13,14] is defined as the transverse length between the most prominent point of the tibial tuberosity and the trochlear groove on the femur, calculated on axial images (CT scan or MRI), representing the axial malalignment of the extensor mechanism. The greater the distance, the greater the lateralizing force acting on the patella. It is pathological when TT-TG > 13 mm on MRI or TT-TG > 20 mm on a CT scan (Figure 4 and Figure 5).
4. Patellofemoral Instability
- Recurrent, when the patella dislocates frequently during knee flexion (two or more episodes are necessary) [17];
- Habitual, when the patella dislocates every time the knee flexes in early knee flexion (<30°) and spontaneously relocates with the extension of the knee [18].
- Permanent, when the patella is permanently dislocated through the entire knee range of motion, never facing the trochlea [19].
- Type 1: patellar dislocation after trauma, without instability and without patella maltracking.
- Type 2: patella instability without clinical or radiological signs of patella maltracking.
- Type 3: a combination of patella instability and patella maltracking. This type is divided into four subtypes, according to the main cause of the maltracking: (a) soft tissue contracture; (b) patella alta; (c) an abnormal tibial tuberosity–trochlea groove distance; (d) valgus deviations; and (e) torsional deformities.
- Type 4: instability and maltracking with a loss of patella tracking due to severe trochlear dysplasia, leading to a highly unstable ‘‘floating patella”.
- Type 5: maltracking without instability.
5. Primary Dislocation: Diagnostic Framing
- Bony avulsions: depending on the size, they may require surgery [25];
- Patella alta: the CDI must be calculated. It is often the first sign of a possible PF disorder;
- Trochlear dysplasia: the crossing sign, the supra-trochlear spur, and the double contour should be identified for classification according to Dejour [9].
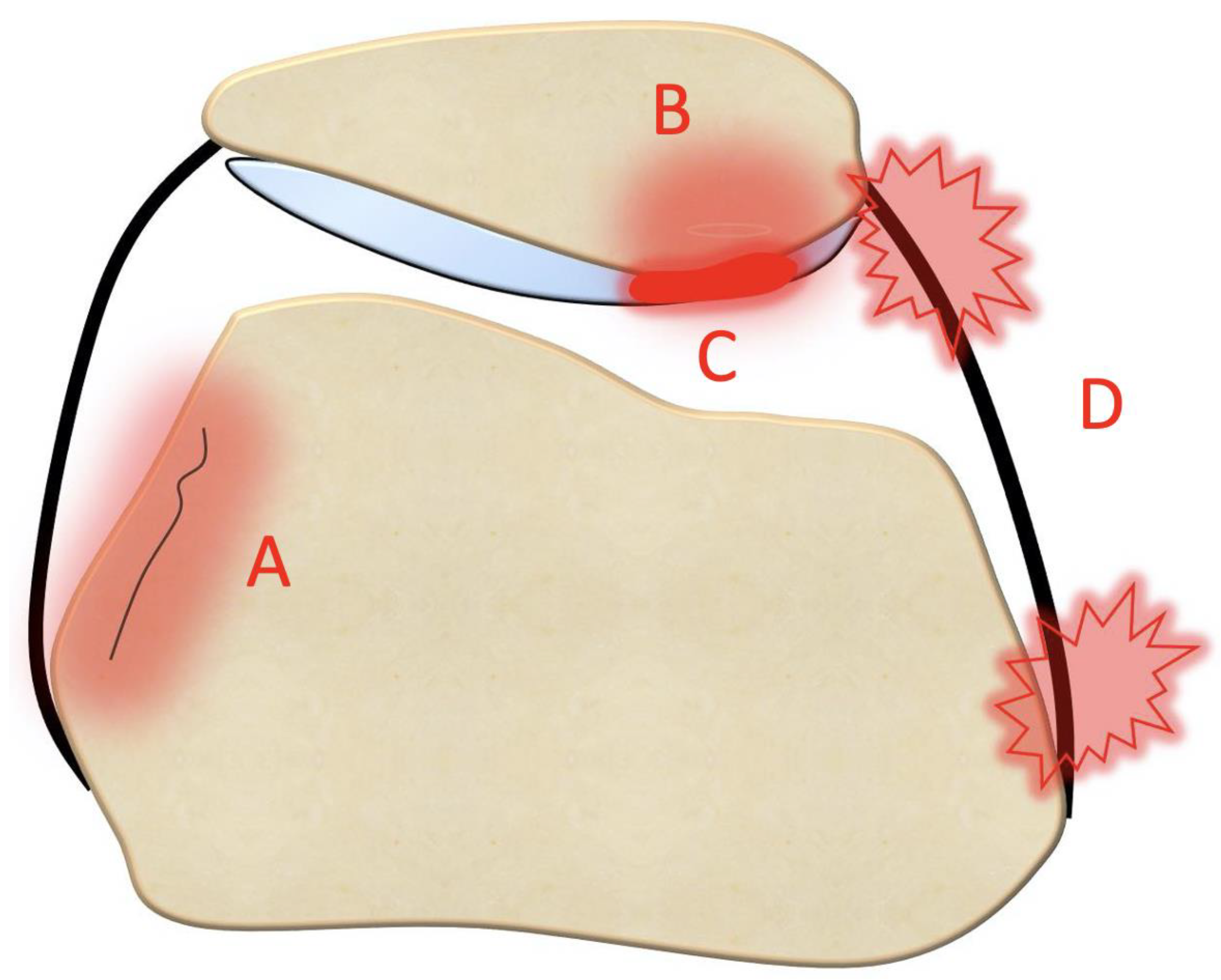
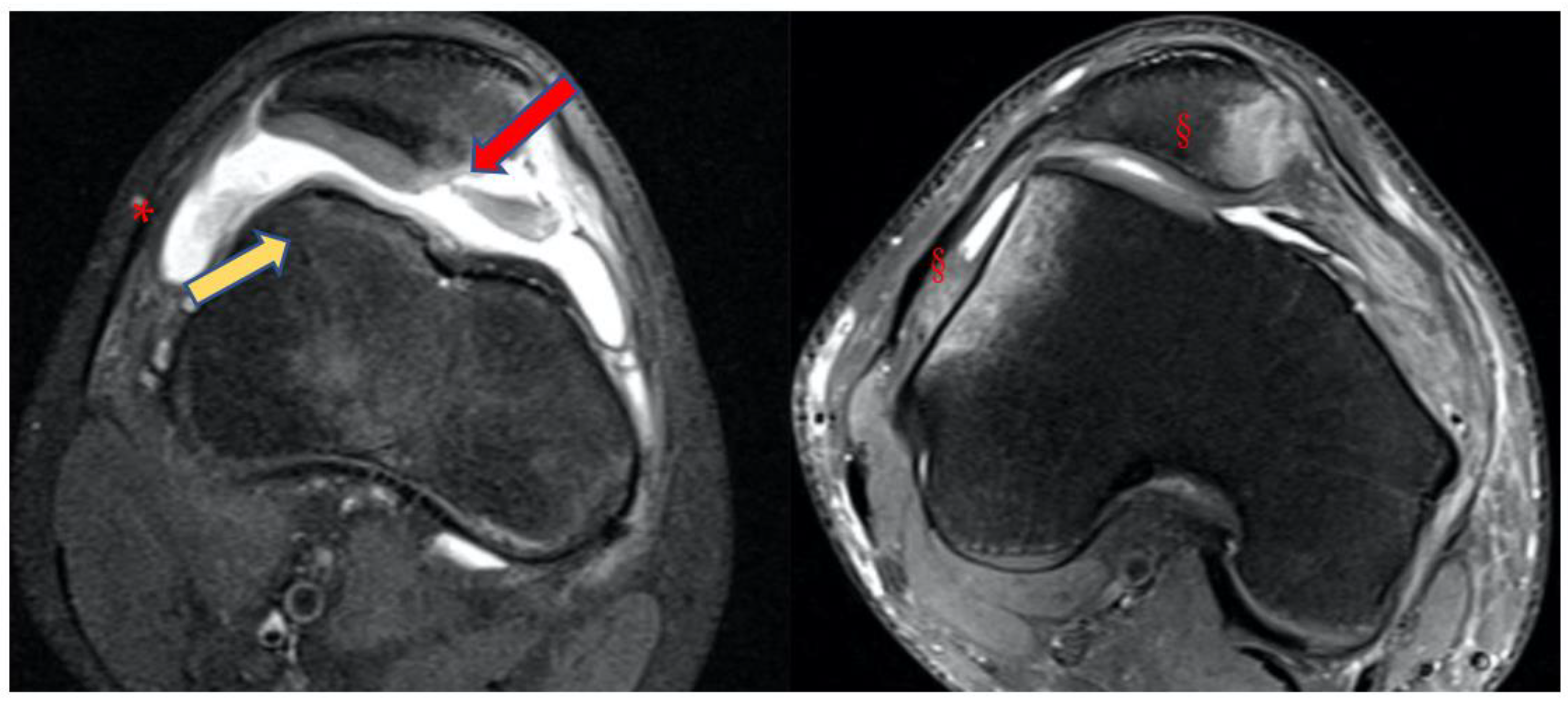
- Bone bruises on the medial side of the patella and the lateral condyle, which indicate with certainty the occurrence of a recent patellar dislocation;
- Osteochondral fracture with possible loose bodies, which are important to rule out, especially in skeletally immature patients. If the osteochondral fracture has a sufficient size (5–10 mm on MRI), urgent reduction and fixation, either open or arthroscopically, must be considered [25];
- Trochlear dysplasia, for which axial images are needed to achieve a correct classification according to the Dejour classification [9];


6. Primary Dislocation: Treatment Options
6.1. Urgent Surgery
6.2. Conservative Treatment
7. Primary Dislocation: Follow-Up
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arendt, E.A.; Dejour, D. Patella instability: Building bridges across the ocean a historic review. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 279–293. [Google Scholar] [CrossRef]
- Flandry, F.; Hommel, G. Normal anatomy and biomechanics of the knee. Sports Med. Arthrosc. Rev. 2011, 19, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Fox, A.J.S.; Wanivenhaus, F.; Rodeo, S.A. The basic science of the patella: Structure, composition, and function. J. Knee Surg. 2012, 25, 127–141. [Google Scholar] [CrossRef]
- Van Kampen, A.; Huiskes, R. The three-dimensional tracking pattern of the human patella. J. Orthop. Res. 1990, 8, 372–382. [Google Scholar] [CrossRef] [PubMed]
- Nagamine, R.; Otani, T.; White, S.E.; McCarthy, D.S.; Whiteside, L.A. Patellar tracking measurement in the normal knee. J. Orthop. Res. 1995, 13, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Wheatley, M.G.A.; Rainbow, M.J.; Clouthier, A.L. Patellofemoral Mechanics: A Review of Pathomechanics and Research Approaches. Curr. Rev. Musculoskelet. Med. 2020, 13, 326–337. [Google Scholar] [CrossRef]
- Dejour, H.; Walch, G.; Nove-Josserand, L.; Guier, C. Factors of patellar instability: An anatomic radiographic study. Knee Surg. Sports Traumatol. Arthrosc. 1994, 2, 19–26. [Google Scholar] [CrossRef]
- Crossley, K.M.; van Middelkoop, M.; Callaghan, M.J.; Collins, N.J.; Rathleff, M.S.; Barton, C.J. 2016 Patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester. Part 2: Recommended physical interventions (exercise, taping, bracing, foot orthoses and combined interventions). Br. J. Sports Med. 2016, 50, 844–852. [Google Scholar] [CrossRef] [Green Version]
- Dejour, D.; Saggin, P. The sulcus deepening trochleoplasty-the Lyon’s procedure. Int. Orthop. 2010, 34, 311–316. [Google Scholar] [CrossRef] [Green Version]
- Malghem, J.; Maldague, B. Patellofemoral joint: 30 degrees axial radiograph with lateral rotation of the leg. Radiology 1989, 170, 566–567. [Google Scholar] [CrossRef]
- Caton, J. Method of measuring the height of the patella. Acta Orthop. Belg. 1989, 55, 385–386. [Google Scholar] [PubMed]
- Lewallen, L.; McIntosh, A.; Dahm, D. First-Time Patellofemoral Dislocation: Risk Factors for Recurrent Instability. J. Knee Surg. 2015, 28, 303–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bayhan, I.A.; Kirat, A.; Alpay, Y.; Ozkul, B.; Kargin, D. Tibial tubercle-trochlear groove distance and angle are higher in children with patellar instability. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 3566–3571. [Google Scholar] [CrossRef] [PubMed]
- Polat, A.E.; Polat, B.; Gürpınar, T.; Sarı, E.; Çarkçı, E.; Erler, K. Tibial tubercle-trochlear groove (TT-TG) distance is a reliable measurement of increased rotational laxity in the knee with an anterior cruciate ligament injury. Knee 2020, 27, 1601–1607. [Google Scholar] [CrossRef]
- Ahmad Khan, H.; Bashir Shah, A.; Kamal, Y. Vertical Patellar Dislocation: Reduction by the Push Up and Rotate Method, A Case Report and Literature Review. Trauma. Mon. 2016, 21, e24705. [Google Scholar] [CrossRef] [Green Version]
- Udogwu, U.N.; Sabatini, C.S. Vertical patellar dislocation: A pediatric case report and review of the literature. Orthop. Rev. 2018, 10, 7688. [Google Scholar] [CrossRef] [Green Version]
- Weber, A.E.; Nathani, A.; Dines, J.S.; Allen, A.A.; Shubin-Stein, B.E.; Arendt, E.A.; Bedi, A. An Algorithmic Approach to the Management of Recurrent Lateral Patellar Dislocation. J. Bone Jt. Surg. Am. 2016, 98, 417–427. [Google Scholar] [CrossRef] [Green Version]
- Batra, S.; Arora, S. Habitual dislocation of patella: A review. J. Clin. Orthop. Trauma. 2014, 5, 245–251. [Google Scholar] [CrossRef] [Green Version]
- Noda, M.; Saegusa, Y.; Kashiwagi, N.; Seto, Y. Surgical treatment for permanent dislocation of the patella in adults. Orthopedics 2011, 34, e948–e951. [Google Scholar] [CrossRef] [Green Version]
- Fithian, D.C.; Paxton, E.W.; Stone, M.L.; Silva, P.; Davis, D.K.; Elias, D.A.; White, L.M. Epidemiology and natural history of acute patellar dislocation. Am. J. Sports Med. 2004, 32, 1114–1121. [Google Scholar] [CrossRef]
- Pagliazzi, G.; Napoli, F.; Previtali, D.; Filardo, G.; Zaffagnini, S.; Candrian, C. A Meta-analysis of Surgical Versus Nonsurgical Treatment of Primary Patella Dislocation. Arthroscopy 2019, 35, 2469–2481. [Google Scholar] [CrossRef] [PubMed]
- Kita, K.; Tanaka, Y.; Toritsuka, Y.; Amano, H.; Uchida, R.; Takao, R.; Horibe, S. Factors Affecting the Outcomes of Double-Bundle Medial Patellofemoral Ligament Reconstruction for Recurrent Patellar Dislocations Evaluated by Multivariate Analysis. Am. J. Sports Med. 2015, 43, 2988–2996. [Google Scholar] [CrossRef] [PubMed]
- Frosch, K.-H.; Schmeling, A. A new classification system of patellar instability and patellar maltracking. Arch. Orthop. Trauma. Surg. 2016, 136, 485–497. [Google Scholar] [CrossRef] [PubMed]
- Nikku, R.; Nietosvaara, Y.; Aalto, K.; Kallio, P.E. The mechanism of primary patellar dislocation: Trauma history of 126 patients. Acta Orthop. 2009, 80, 432–434. [Google Scholar] [CrossRef]
- Placella, G.; Tei, M.M.; Sebastiani, E.; Criscenti, G.; Speziali, A.; Mazzola, C.; Georgoulis, A.; Cerulli, G. Shape and size of the medial patellofemoral ligament for the best surgical reconstruction: A human cadaveric study. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2327–2333. [Google Scholar] [CrossRef]
- Sillanpää, P.J.; Peltola, E.; Mattila, V.M.; Kiuru, M.; Visuri, T.; Pihlajamäki, H. Femoral avulsion of the medial patellofemoral ligament after primary traumatic patellar dislocation predicts subsequent instability in men: A mean 7-year nonoperative follow-up study. Am. J. Sports Med. 2009, 37, 1513–1521. [Google Scholar] [CrossRef] [Green Version]
- Elias, D.A.; White, L.M.; Fithian, D.C. Acute lateral patellar dislocation at MR imaging: Injury patterns of medial patellar soft-tissue restraints and osteochondral injuries of the inferomedial patella. Radiology 2002, 225, 736–743. [Google Scholar] [CrossRef]
- Conlan, T.; Garth, W.P.; Lemons, J.E. Evaluation of the medial soft-tissue restraints of the extensor mechanism of the knee. J. Bone Jt. Surg. Am. 1993, 75, 682–693. [Google Scholar] [CrossRef]
- McCrum, E.; Cooper, K.; Wittstein, J.; French, R.J. Imaging of Patellofemoral Instability. Clin. Sports Med. 2021, 40, 693–712. [Google Scholar] [CrossRef]
- Maas, K.-J.; Warncke, M.L.; Leiderer, M.; Krause, M.; Dust, T.; Frings, J.; Frosch, K.-H.; Adam, G.; Henes, F.O.G. Diagnostic Imaging of Patellofemoral Instability. ROFO Fortschr Geb Rontgenstr Nukl. 2021, 193, 1019–1033. [Google Scholar] [CrossRef]
- Arendt, E.A.; Askenberger, M.; Agel, J.; Tompkins, M.A. Risk of Redislocation After Primary Patellar Dislocation: A Clinical Prediction Model Based on Magnetic Resonance Imaging Variables. Am. J. Sports Med. 2018, 46, 3385–3390. [Google Scholar] [CrossRef] [PubMed]
- Parikh, S.N.; Lykissas, M.G.; Gkiatas, I. Predicting Risk of Recurrent Patellar Dislocation. Curr. Rev. Musculoskelet. Med. 2018, 11, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Balcarek, P.; Oberthür, S.; Hopfensitz, S.; Frosch, S.; Walde, T.A.; Wachowski, M.M.; Schüttrumpf, J.P.; Stürmer, K.M. Which patellae are likely to redislocate? Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2308–2314. [Google Scholar] [CrossRef]
- Frings, J.; Balcarek, P.; Tscholl, P.; Liebensteiner, M.; Dirisamer, F.; Koenen, P. Conservative Versus Surgical Treatment for Primary Patellar Dislocation. Dtsch. Arztebl. Int. 2020, 117, 279–286. [Google Scholar] [CrossRef]
- Medina Pérez, G.; Barrow, B.; Krueger, V.; Cruz, A.I. Treatment of Osteochondral Fractures After Acute Patellofemoral Instability: A Critical Analysis Review. JBJS Rev. 2022, 10, e21. [Google Scholar] [CrossRef]
- Watts, R.E.; Gorbachova, T.; Fritz, R.C.; Saad, S.S.; Lutz, A.M.; Kim, J.; Chaudhari, A.S.; Shea, K.G.; Sherman, S.L.; Boutin, R.D. Patellar Tracking: An Old Problem with New Insights. Radiographics 2023, 43, e220177. [Google Scholar] [CrossRef]
- Panni, A.S.; Cerciello, S.; Maffulli, N.; Di Cesare, M.; Servien, E.; Neyret, P. Patellar shape can be a predisposing factor in patellar instability. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 663–670. [Google Scholar] [CrossRef]
- Hughston, J.C. Subluxation of the patella. J. Bone Jt. Surg. Am. 1968, 50, 1003–1026. [Google Scholar] [CrossRef]
- Fairbank, H.A. Internal Derangement of the Knee in Children and Adolescents: (Section of Orthopaedics). Proc. R. Soc. Med. 1937, 30, 427–432. [Google Scholar]
- Alshaban, R.M.; Ghaddaf, A.A.; Alghamdi, D.M.; Aghashami, A.; Alqrni, A.; Alyasi, A.A.; Bogari, H.; Qadi, S. Operative versus non-operative management of primary patellar dislocation: A systematic review and network meta-analysis. Injury 2023, 54, 110926. [Google Scholar] [CrossRef]
- Xu, T.; Xu, L.-H.; Li, X.-Z.; Fu, H.-J.; Zhou, Y. Original surgical technique for the treatment of patellofemoral instability after failure of conservative treatment. Orthop. Traumatol. Surg. Res. 2023, 103657. [Google Scholar] [CrossRef]
- Herdea, A.; Pencea, V.; Lungu, C.N.; Charkaoui, A.; Ulici, A. A Prospective Cohort Study on Quality of Life among the Pediatric Population after Surgery for Recurrent Patellar Dislocation. Child 2021, 8, 830. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, S.; Varacallo, M.; Thomas, J.D.; Carroll, J.J.; Kahwaji, C.I. Patellar Instability. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Trivellas, M.; Arshi, A.; Beck, J.J. Roux-Goldthwait and Medial Patellofemoral Ligament Reconstruction for Patella Realignment in the Skeletally Immature Patient. Arthrosc. Tech. 2019, 8, e1479–e1483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Felli, L.; Capello, A.G.; Lovisolo, S.; Chiarlone, F.; Alessio-Mazzola, M. Goldthwait technique for patellar instability: Surgery of the past or here to stay procedure? A systematic review of the literature. Musculoskelet. Surg. 2019, 103, 107–113. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | |
|---|---|
| >16 | 0 |
| ≤16 | 1 |
| Bilateral instability | |
| No | 0 |
| Yes | 1 |
| Trochlear dysplasia | |
| None | 0 |
| Mild (type A) | 1 |
| Severe (type B–D) | 2 |
| Patellar height, IS ratio | |
| ≤1.2 | 0 |
| >1.2 | 1 |
| TT-TG distance | |
| <16 mm | 0 |
| ≥16 mm | 1 |
| Patellar tilt | |
| ≤20° | 0 |
| >20° | 1 |
| Total points | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maggioni, D.M.; Giorgino, R.; Messina, C.; Albano, D.; Peretti, G.M.; Mangiavini, L. Framing Patellar Instability: From Diagnosis to the Treatment of the First Episode. J. Pers. Med. 2023, 13, 1225. https://doi.org/10.3390/jpm13081225
Maggioni DM, Giorgino R, Messina C, Albano D, Peretti GM, Mangiavini L. Framing Patellar Instability: From Diagnosis to the Treatment of the First Episode. Journal of Personalized Medicine. 2023; 13(8):1225. https://doi.org/10.3390/jpm13081225
Chicago/Turabian StyleMaggioni, Davide Maria, Riccardo Giorgino, Carmelo Messina, Domenico Albano, Giuseppe Michele Peretti, and Laura Mangiavini. 2023. "Framing Patellar Instability: From Diagnosis to the Treatment of the First Episode" Journal of Personalized Medicine 13, no. 8: 1225. https://doi.org/10.3390/jpm13081225