
The Psoriatic Arthritis 5-Thermometer Scales (PsA-5Ts): Measurement Properties of a New Multidimensional Composite Tool for the Quick Assessment of the Overall Health Status in Psoriatic Arthritis
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients Characteristics
2.2. Variables
2.2.1. Minimal Disease Activity (MDA) Criteria
2.2.2. Disease Activity for Psoriatic Arthritis (DAPSA)
2.2.3. Composite Psoriatic Disease Activity Index (CPDAI)
2.2.4. Psoriatic Arthritis Disease Activity Score (PASDAS)
2.2.5. Psoriatic Arthritis Impact of Disease 12-Item (PsAID-12)
2.2.6. Short-Form 36 Health Survey Questionnaire (SF-36)
2.3. The Psoriatic Arthritis 5-Thermometer Scales, Development and Description
2.3.1. Item Pool Development
2.3.2. Testing the Provisional Questionnaire
2.4. Statistical Analysis
3. Results
3.1. Testing the Provisional Questionnaire
3.2. Patient Characteristics
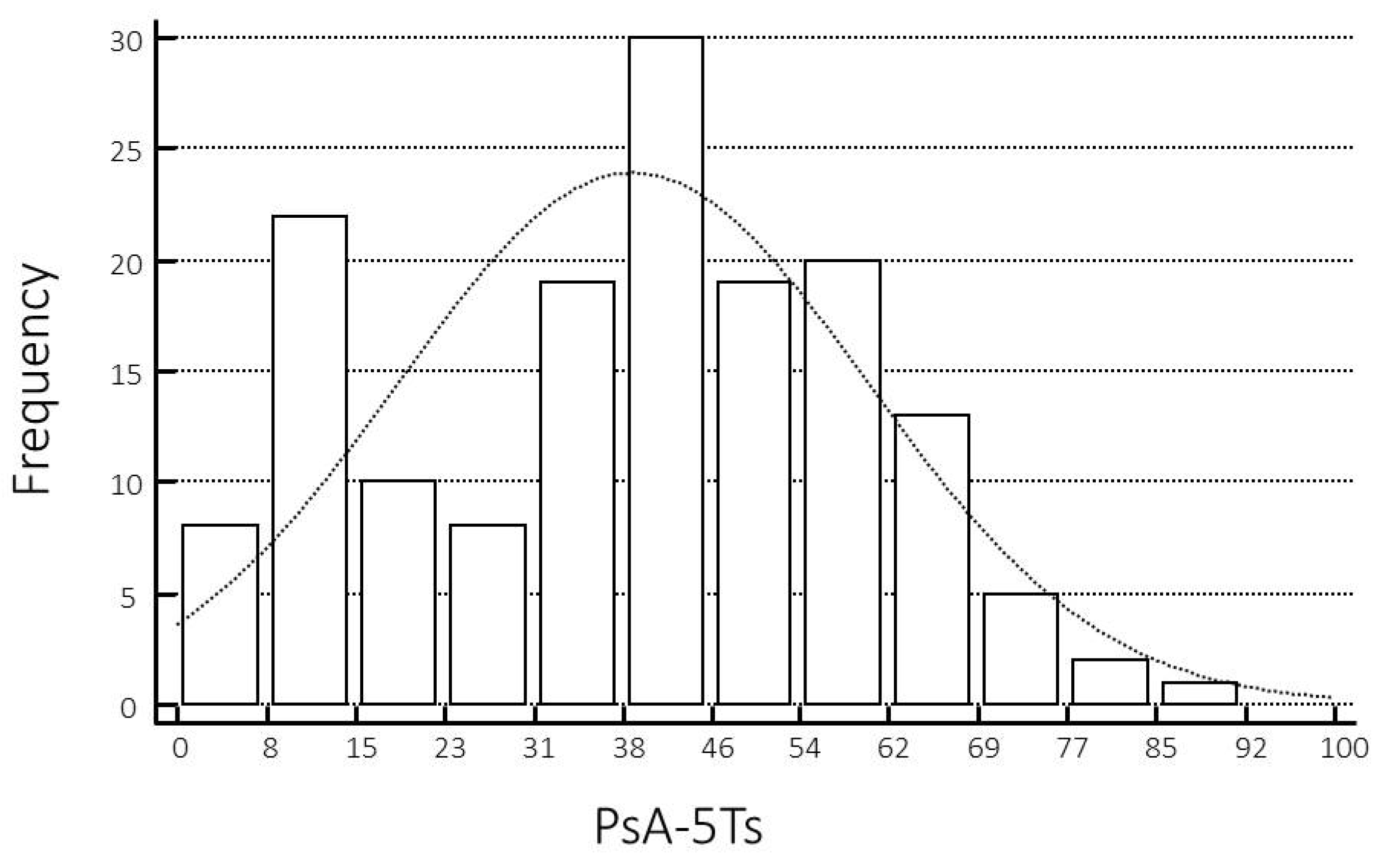
3.3. Descriptive Statistics of Composite Disease Activity Indices and Patient Self-Report Questionnaires
3.4. Convergent Validity
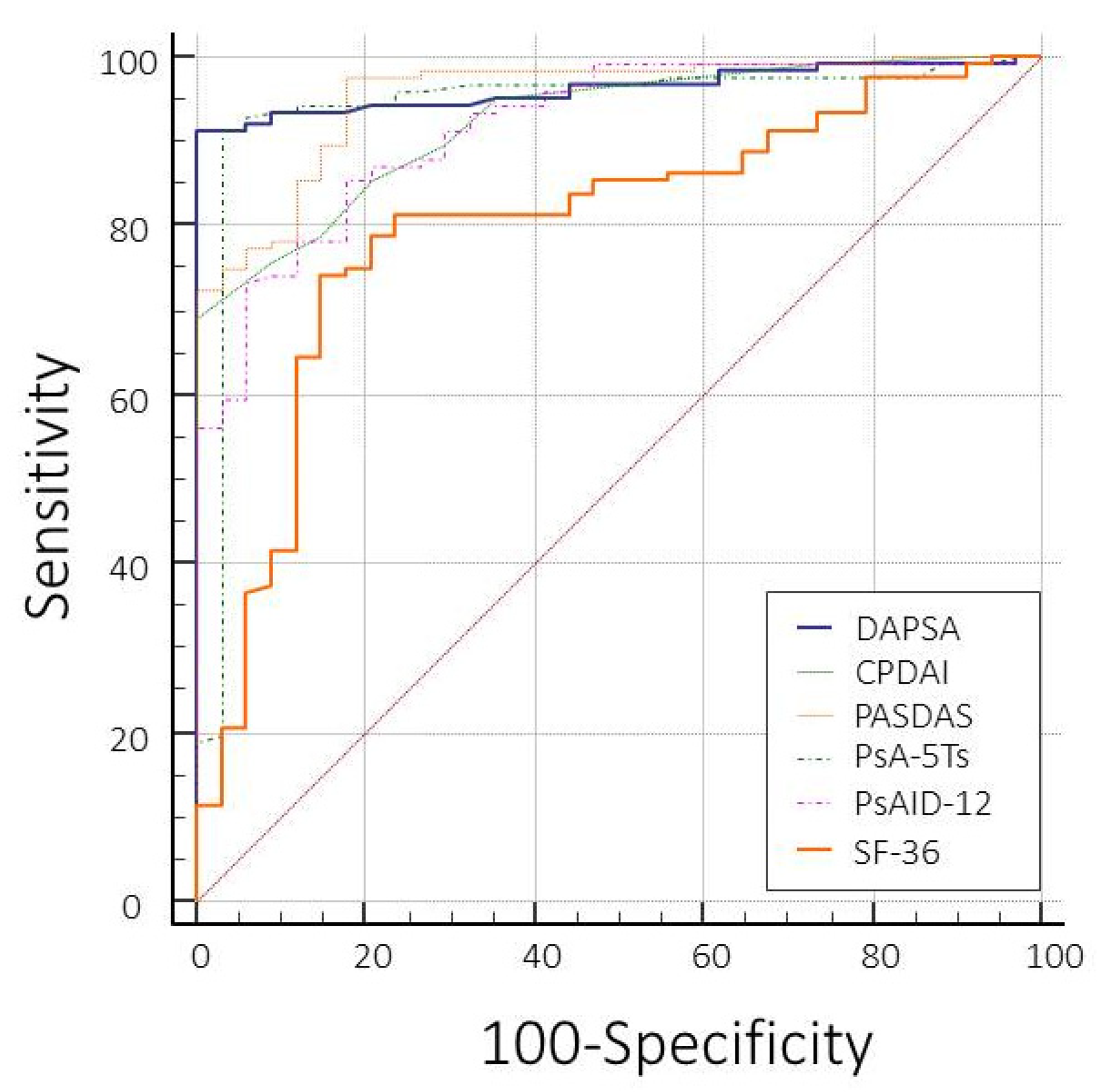
3.5. Discriminant Validity
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mease, P.J. Psoriatic Arthritis: Update on Pathophysiology, Assessment, and Management. Ann. Rheum. Dis. 2011, 70, i77–i84. [Google Scholar] [CrossRef] [PubMed]
- Salaffi, F.; Di Carlo, M.; Luchetti, M.M.; Di Donato, E.; Campanati, A.; Benfaremo, D.; Nicolini, M.; Carotti, M.; Giacchetti, A.; Ganzetti, G.; et al. A validation study of the Simple Psoriatic Arthritis Screening (SiPAS) questionnaire to screen psoriasis patients for psoriatic arthritis. Clin. Exp. Rheumatol. 2018, 36, 127–135. [Google Scholar] [PubMed]
- McArdle, A.; Pennington, S.; FitzGerald, O. Clinical Features of Psoriatic Arthritis: A Comprehensive Review of Unmet Clinical Needs. Clin. Rev. Allergy Immunol. 2018, 55, 271–294. [Google Scholar] [CrossRef]
- Ogdie, A.; Weiss, P. The Epidemiology of Psoriatic Arthritis. Rheum. Dis. Clin. N. Am. 2015, 41, 545–568. [Google Scholar] [CrossRef] [Green Version]
- Mease, P.J.; Gladman, D.D.; Papp, K.A.; Khraishi, M.M.; Thaçi, D.; Behrens, F.; Northington, R.; Fuiman, J.; Bananis, E.; Boggs, R.; et al. Prevalence of Rheumatologist-Diagnosed Psoriatic Arthritis in Patients with Psoriasis in European/North American Dermatology Clinics. J. Am. Acad. Dermatol. 2013, 69, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Lapadula, G.; Marchesoni, A.; Salaffi, F.; Ramonda, R.; Salvarani, C.; Punzi, L.; Costa, L.; Caso, F.; Simone, D.; Baiocchi, G.; et al. Evidence-Based Algorithm for Diagnosis and Assessment in Psoriatic Arthritis: Results by Italian DElphi in Psoriatic Arthritis (IDEA). Reumatismo 2016, 68, 126–136. [Google Scholar] [CrossRef] [Green Version]
- Ramonda, R.; Marchesoni, A.; Carletto, A.; Bianchi, G.; Cutolo, M.; Ferraccioli, G.; Fusaro, E.; De Vita, S.; Galeazzi, M.; Gerli, R.; et al. Patient-Reported Impact of Spondyloarthritis on Work Disability and Working Life: The ATLANTIS Survey. Arthritis Res. Ther. 2016, 18, 78. [Google Scholar] [CrossRef] [Green Version]
- Mease, P.J. Measures of Psoriatic Arthritis: Tender and Swollen Joint Assessment, Psoriasis Area and Severity Index (PASI), Nail Psoriasis Severity Index (NAPSI), Modified Nail Psoriasis Severity Index (mNAPSI), Mander/Newcastle Enthesitis Index (MEI), Leeds Enthesitis Index (LEI), Spondyloarthritis Research Consortium of Canada (SPARCC), Maastricht Ankylosing Spondylitis Enthesis Score (MASES), Leeds Dactylitis Index (LDI), Patient Global for Psoriatic Arthritis, Dermatology Life Quality Index (DLQI), Psoriatic Arthritis Quality of Life (PsAQOL), Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F), Psoriatic Arthritis Response Criteria (PsARC), Psoriatic Arthritis Joint Activity Index (PsAJAI), Disease Activity in Psoriatic Arthritis (DAPSA), and Composite Psoriatic Disease Activity Index (CPDAI). Arthritis Care Res. 2011, 63, S64–S85. [Google Scholar]
- Goldsmith, C.H.; Smythe, H.A.; Helewa, A. Interpretation and Power of a Pooled Index. J. Rheumatol. 1993, 20, 575–578. [Google Scholar]
- van der Heijde, D.M.; van’t Hof, M.A.; van Riel, P.L.; van Leeuwen, M.A.; van Rijswijk, M.H.; van de Putte, L.B. Validity of Single Variables and Composite Indices for Measuring Disease Activity in Rheumatoid Arthritis. Ann. Rheum. Dis. 1992, 51, 177–181. [Google Scholar] [CrossRef]
- Coates, L.C.; Mumtaz, A.; Helliwell, P.S.; Mease, P.J.; Callis-Duffin, K.; Krueger, G.G.; McHugh, N.J.; Strand, V.; Gladman, D.D.; FitzGerald, O. Development of a Disease Severity and Responder Index for Psoriatic Arthritis (PsA)—Report of the OMERACT 10 PsA Special Interest Group. J. Rheumatol. 2011, 38, 1496–1501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gladman, D.D.; Helliwell, P.; Mease, P.J.; Nash, P.; Ritchlin, C.; Taylor, W. Assessment of Patients with Psoriatic Arthritis: A Review of Currently Available Measures. Arthritis Rheum. 2004, 50, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Gladman, D.D.; Mease, P.J.; Healy, P.; Helliwell, P.S.; Fitzgerald, O.; Cauli, A.; Lubrano, E.; Chandler, D.; Beltran, A.; Chandran, V.; et al. Outcome Measures in Psoriatic Arthritis. J. Rheumatol. 2007, 34, 1159–1166. [Google Scholar]
- Ritchlin, C.T.; Kavanaugh, A.; Gladman, D.D.; Mease, P.J.; Helliwell, P.; Boehncke, W.H.; de Vlam, K.; Fiorentino, D.; Fitzgerald, O.; Gottlieb, A.B.; et al. Treatment Recommendations for Psoriatic Arthritis. Ann. Rheum. Dis. 2009, 68, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Mumtaz, A.; Gallagher, P.; Kirby, B.; Waxman, R.; Coates, L.C.; Veale, J.D.; Helliwell, P.S.; FitzGerald, O. Development of a Preliminary Composite Disease Activity Index in Psoriatic Arthritis. Ann. Rheum. Dis. 2011, 70, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Eberl, G.; Studnicka-Benke, A.; Hitzelhammer, H.; Aringer, M.; Smolen, J.S. Development of a Disease Activity Index for the Assessment of Reactive Arthritis (DAREA). Rheumatology 2000, 39, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Nell-Duxneuner, V.P.; Stamm, T.A.; Machold, K.P.; Pflugbeil, S.; Aletaha, D.; Smolen, J.S.; Steiner, G. Evaluation of the Appropriateness of Composite Disease Activity Measures for Assessment of Psoriatic Arthritis. Ann. Rheum. Dis. 2010, 69, 546–549. [Google Scholar] [CrossRef]
- Helliwell, P.S.; FitzGerald, O.; Fransen, J.; Gladman, D.D.; Kreuger, G.G.; Callis-Duffin, K.; McHugh, N.; Mease, P.J.; Strand, V.; Waxman, R.; et al. The Development of Candidate Composite Disease Activity and Responder Indices for Psoriatic Arthritis (GRACE Project). Ann. Rheum. Dis. 2013, 72, 986–991. [Google Scholar] [CrossRef]
- Kirwan, J.R.; Bartlett, S.J.; Beaton, D.E.; Boers, M.; Bosworth, A.; Brooks, P.M.; Choy, E.; De Wit, M.; Guillemin, F.; Hewlett, S.; et al. Updating the OMERACT Filter: Implications for Patient-Reported Outcomes. J. Rheumatol. 2014, 41, 1011–1015. [Google Scholar] [CrossRef] [Green Version]
- Coates, L.C.; FitzGerald, O.; Mease, P.J.; Gladman, D.D.; Strand, V.; Goel, N.; Campbell, I.; Krueger, G.; McHugh, N.J.; Helliwell, P.S. Development of a Disease Activity and Responder Index for Psoriatic Arthritis—Report of the Psoriatic Arthritis Module at OMERACT 11. J. Rheumatol. 2014, 41, 782–791. [Google Scholar] [CrossRef] [Green Version]
- Coates, L.C.; FitzGerald, O.; Merola, J.F.; Smolen, J.; van Mens, L.J.J.; Bertheussen, H.; Boehncke, W.H.; Callis Duffin, K.; Campbell, W.; de Wit, M.; et al. Group for Research and Assessment of Psoriasis and Psoriatic Arthritis/Outcome Measures in Rheumatology Consensus-Based Recommendations and Research Agenda for Use of Composite Measures and Treatment Targets in Psoriatic Arthritis. Arthritis Rheumatol. 2018, 70, 345–355. [Google Scholar] [CrossRef]
- Poddubnyy, D.; Baraliakos, X.; Van den Bosch, F.; Braun, J.; Coates, L.C.; Chandran, V.; Diekhoff, T.; van Gaalen, F.A.; Gensler, L.S.; Goel, N.; et al. Axial Involvement in Psoriatic Arthritis Cohort (AXIS): The Protocol of a Joint Project of the Assessment of SpondyloArthritis International Society (ASAS) and the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA). Ther. Adv. Musculoskelet. Dis. 2021, 13, 1759720X211057975. [Google Scholar] [CrossRef] [PubMed]
- Weisman, M.H. Patient-Reported Outcomes in Rheumatic Diseases. Rheum. Dis. Clin. North Am. 2016, 42, xiii–xiv. [Google Scholar] [CrossRef] [PubMed]
- Barton, J.L.; Katz, P. The Patient Experience: Patient-Reported Outcomes in Rheumatology. Rheum. Dis. Clin. N. Am. 2016, 42, xv–xvi. [Google Scholar] [CrossRef]
- Palominos, P.E.; Gaujoux-Viala, C.; Fautrel, B.; Dougados, M.; Gossec, L. Clinical Outcomes in Psoriatic Arthritis: A Systematic Literature Review. Arthritis Care Res. 2012, 64, 397–406. [Google Scholar] [CrossRef]
- Mathew, A.J.; Chandran, V. Depression in Psoriatic Arthritis: Dimensional Aspects and Link with Systemic Inflammation. Rheumatol. Ther. 2020, 7, 287–300. [Google Scholar] [CrossRef]
- Lada, G.; Chinoy, H.; Heal, C.; Warren, R.B.; Talbot, P.S.; Kleyn, C.E. Depression and Suicidality in Patients with Psoriasis and the Role of Psoriatic Arthritis: A Cross-Sectional Study in a Tertiary Setting. J. Acad. Consult. Liaison Psychiatry 2022, 63, 372–383. [Google Scholar] [CrossRef]
- Tran, F.; Schirmer, J.H.; Ratjen, I.; Lieb, W.; Helliwell, P.; Burisch, J.; Schulz, J.; Schrinner, F.; Jaeckel, C.; Müller-Ladner, U.; et al. Patient-Reported Outcomes in Chronic Inflammatory Diseases: Current State, Limitations, and Perspectives. Front. Immunol. 2021, 12, 614653. [Google Scholar] [CrossRef]
- Salaffi, F.; Di Carlo, M.; Carotti, M.; Farah, S. The Patient-Reported Outcomes Thermometer-5-Item Scale (5T-PROs): Validation of a New Tool for the Quick Assessment of Overall Health Status in Painful Rheumatic Diseases. Pain Res. Manag. 2018, 2018, 3496846. [Google Scholar] [CrossRef]
- Taylor, W.; Gladman, D.; Helliwell, P.; Marchesoni, A.; Mease, P.; Mielants, H. Classification Criteria for Psoriatic Arthritis: Development of New Criteria from a Large International Study. Arthritis Rheum. 2006, 54, 2665–2673. [Google Scholar] [CrossRef] [PubMed]
- Rudwaleit, M.; Landewé, R.; van der Heijde, D.; Listing, J.; Brandt, J.; Braun, J.; Burgos-Vargas, R.; Collantes-Estevez, E.; Davis, J.; Dijkmans, B.; et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part I): Classification of paper patients by expert opinion including uncertainty appraisal. Ann. Rheum. Dis. 2009, 68, 770–776. [Google Scholar] [CrossRef] [PubMed]
- Rudwaleit, M.; van der Heijde, D.; Landewé, R.; Listing, J.; Akkoc, N.; Brandt, J.; Braun, J.; Chou, C.T.; Collantes-Estevez, E.; Dougados, M.; et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part II): Validation and final selection. Ann. Rheum. Dis. 2009, 68, 777–783. [Google Scholar] [CrossRef]
- Helliwell, P.; Marchesoni, A.; Peters, M.; Barker, M.; Wright, V. A re-evaluation of the osteoarticular manifestations of psoriasis. Br. J. Rheumatol. 1991, 30, 339–345. [Google Scholar] [CrossRef] [PubMed]
- van der Linden, S.; Valkenburg, H.A.; Cats, A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum. 1984, 27, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Sieper, J.; van der Heijde, D.; Landewé, R.; Brandt, J.; Burgos-Vagas, R.; Collantes-Estevez, E.; Dijkmans, B.; Dougados, M.; A Khan, M.; Leirisalo-Repo, M.; et al. New criteria for inflammatory back pain in patients with chronic back pain: A real patient exercise by experts from the Assessment of SpondyloArthritis International Society (ASAS). Ann. Rheum. Dis. 2009, 68, 784–788. [Google Scholar] [CrossRef] [PubMed]
- Salvarani, C.; Pipitone, N.; Marchesoni, A.; Cantini, F.; Cauli, A.; Lubrano, E.; Punzi, L.; Scarpa, R.; Spadaro, A.; Matucci-Cerinic, M.; et al. Recommendations for the use of biologic therapy in the treatment of psoriatic arthritis: Update from the Italian Society for Rheumatology. Clin. Exp. Rheumatol. 2011, 29, S28–S34. [Google Scholar]
- Fries, J.F.; Spitz, P.; Kraines, R.G.; Holman, H.R. Measurement of patient outcome in arthritis. Arthritis Rheum. 1980, 23, 137–145. [Google Scholar] [CrossRef]
- Coates, L.C.; Fransen, J.; Helliwell, P.S. Defining minimal disease activity in psoriatic arthritis: A proposed objective target for treatment. Ann. Rheum. Dis. 2010, 69, 48–53. [Google Scholar] [CrossRef]
- Schoels, M.M.; Aletaha, D.; Alasti, F.; Smolen, J.S. Disease activity in psoriatic arthritis (PsA): Defining remission and treatment success using the DAPSA score. Ann. Rheum. Dis. 2016, 75, 811–818. [Google Scholar] [CrossRef]
- Garrett, S.; Jenkinson, T.; Kennedy, L.G.; Whitelock, H.; Gaisford, P.; Calin, A. A new approach to defining disease status in ankylosing spondylitis: The Bath Ankylosing Spondylitis Disease Activity Index. J. Rheumatol. 1994, 21, 2286–2291. [Google Scholar]
- Salaffi, F.; Stancati, A.; Silvestri, A.; Carotti, M.; Grassi, W. Validation of the Italian versions of the Bath Ankylosing Spondylitis Functional Index (BASFI) and the Dougados Functional Index (DFI) in patients with ankylosing spondylitis. Reumatismo 2005, 57, 161–173. [Google Scholar] [CrossRef] [PubMed]
- da Cruz Ribeiro E Souza, E.; da Silva Carneiro, S.C.; Yazbek, M.A.; de Cássia Menin, R.; Campanholo, C.B.; Carneiro, J.N.; da Silva, C.H.M.; Ranza, R. Validation and clinical interpretability of PsAID—Psoriatic arthritis impact of disease. Adv. Rheumatol. 2020, 60, 49. [Google Scholar] [CrossRef] [PubMed]
- Di Carlo, M.; Becciolini, A.; Lato, V.; Crotti, C.; Favalli, E.G.; Salaffi, F. The 12-item Psoriatic Arthritis Impact of Disease Questionnaire: Construct Validity, Reliability, and Interpretability in a Clinical Setting. J. Rheumatol. 2017, 44, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–481. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Kosinski, M.; Keller, S.D. SF-36 Physical and Mental Health Summary Scales: A User’s Manual; The Health Institute, New England Medical Centre: Boston, MA, USA, 1994. [Google Scholar]
- Apolone, G.; Mosconi, P. The Italian SF-36 Health Survey: Translation, validation, and norming. J. Clin. Epidemiol. 1998, 51, 1025–1036. [Google Scholar] [CrossRef]
- Husted, J.A.; Gladman, D.D.; Farewell, V.T.; Cook, R.J. Health-related quality of life of patients with psoriatic arthritis: A comparison with patients with rheumatoid arthritis. Arthritis Rheum. 2001, 45, 151–158. [Google Scholar] [CrossRef]
- Boulkedid, R.; Abdoul, H.; Loustau, M.; Sibony, O.; Alberti, C. Using and reporting the Delphi method for selecting healthcare quality indicators: A systematic review. PLoS ONE 2011, 6, e20476. [Google Scholar] [CrossRef]
- Di Carlo, M.; Luchetti, M.M.; Benfaremo, D.; Di Donato, E.; Mosca, P.; Maltoni, S.; Benedetti, A.; Gabrielli, A.; Grassi, W.; Salaffi, F. The DETection of Arthritis in Inflammatory boweL diseases (DETAIL) questionnaire: Development and preliminary testing of a new tool to screen patients with inflammatory bowel disease for the presence of spondyloarthritis. Clin. Rheumatol. 2018, 37, 1037–1044. [Google Scholar] [CrossRef]
- Lynn, M.R. Determination and Quantification of Content Validity. Nurs. Res. 1986, 35, 382–385. [Google Scholar] [CrossRef]
- Orbai, A.M.; Ogdie, A. Patient-Reported Outcomes in Psoriatic Arthritis. Rheum. Dis. Clin. North Am. 2016, 42, 265–283. [Google Scholar] [CrossRef] [Green Version]
- Smolen, J.S.; Schöls, M.; Braun, J.; Dougados, M.; FitzGerald, O.; Gladman, D.D.; Kavanaugh, A.; Landewé, R.; Mease, P.; Sieper, J.; et al. Treating axial spondyloarthritis and peripheral spondyloarthritis, especially psoriatic arthritis, to target: 2017 update of recommendations by an international Task force. Ann. Rheum. Dis. 2018, 77, 3–17. [Google Scholar] [CrossRef] [PubMed]
- Coates, L.C.; Gottlieb, A.B.; Merola, J.F.; Boone, C.; Szumski, A.; Chhabra, A. Comparison of different remission and low disease definitions in psoriatic arthritis and evaluation of their prognostic value. J. Rheumatol. 2019, 46, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Churruca, K.; Pomare, C.; Ellis, L.A.; Long, J.C.; Henderson, S.B.; Murphy, L.E.D.; Leahy, C.J.; Braithwaite, J. Patient-Reported Outcome Measures (PROMs): A Review of Generic and Condition-Specific Measures and a Discussion of Trends and Issues. Health Expect. 2021, 24, 1015–1024. [Google Scholar] [CrossRef] [PubMed]
- Rothrock, N.E.; Kaiser, K.A.; Cella, D. Developing a Valid Patient-Reported Outcome Measure. Clin. Pharmacol. Ther. 2011, 90, 737–742. [Google Scholar] [CrossRef] [Green Version]
- Gossec, L.; de Wit, M.; Kiltz, U.; Braun, J.; Kalyoncu, U.; Scrivo, R.; Maccarone, M.; Carton, L.; Otsa, K.; Sooäär, I.; et al. A patient-derived and patient-reported outcome measure for assessing psoriatic arthritis: Elaboration and preliminary validation of the Psoriatic Arthritis Impact of Disease (PsAID) questionnaire, a 13-country EULAR initiative. Ann. Rheum. Dis. 2014, 73, 1012–1019. [Google Scholar] [CrossRef]
- Grossman, L.V.; Feiner, S.K.; Mitchell, E.G.; Masterson Creber, R.M. Leveraging Patient-Reported Outcomes Using Data Visualization. Appl. Clin. Inform. 2018, 9, 565–575. [Google Scholar] [CrossRef] [Green Version]
- Benesh, L.R.; Szigeti, E.; Ferraro, F.R.; Gullicks, J.N. Tools for assessing chronic pain in rural elderly women. Home Healthc. Nurse 1997, 15, 207–211. [Google Scholar] [CrossRef]
- Leung, Y.Y.; Ho, K.W.; Li, E.K.; Li, M.; Kwok, L.W.; Wong, P.C.; Li, T.K.; Zhu, T.Y.; Kun, E.W.; Tam, L.S. Predictors of functional deterioration in Chinese patients with psoriatic arthritis: A longitudinal study. BMC Musculoskelet. Disord. 2014, 15, 284. [Google Scholar] [CrossRef] [Green Version]
- Gladman, D.D.; Mease, P.J.; Strand, V.; Healy, P.; Helliwell, P.S.; Fitzgerald, O.; Gottlieb, A.B.; Krueger, G.G.; Nash, P.; Ritchlin, C.T.; et al. Consensus on a core set of domains for psoriatic arthritis. J. Rheumatol. 2007, 34, 1167–1170. [Google Scholar]
- Krajewska-Włodarczyk, M.; Owczarczyk-Saczonek, A.; Placek, W. Fatigue—An underestimated symptom in psoriatic arthritis. Reumatologia 2017, 55, 125–130. [Google Scholar] [CrossRef] [Green Version]
- Husted, J.A.; Tom, B.D.; Schentag, C.T.; Farewell, V.T.; Gladman, D.D. Occurrence and correlates of fatigue in psoriatic arthritis. Ann. Rheum. Dis. 2009, 68, 1553–1558. [Google Scholar] [CrossRef]
- Orbai, A.M.; de Wit, M.; Mease, P.; Shea, J.A.; Gossec, L.; Leung, Y.Y.; Tillett, W.; Elmamoun, M.; Callis Duffin, K.; Campbell, W.; et al. International patient, and physician consensus on a psoriatic arthritis core outcome set for clinical trials. Ann. Rheum. Dis. 2017, 76, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, L.; Johannesson, M.; Silverdahl, M.; Hermansson, C.; Lindberg, M. Health-related quality of life in patients with psoriasis and atopic dermatitis measured with SF-36, DLQI and a subjective measure of disease activity. Acta Derm. Venereol. 2000, 80, 430–434. [Google Scholar] [PubMed] [Green Version]
- Bhosle, M.J.; Kulkarni, A.; Feldman, S.R.; Balkrishnan, R. Quality of life in patients with psoriasis. Health Qual. Life Outcomes 2006, 4, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Carlo, M.; Becciolini, A.; Incorvaia, A.; Beci, G.; Smerilli, G.; Biggioggero, M.; Tardella, M.; De Angelis, R.; Salaffi, F. Mild cognitive impairment in psoriatic arthritis: Prevalence and associated factors. Medicine 2021, 100, e24833. [Google Scholar] [CrossRef]
- Di Carlo, M.; Salaffi, F. Is It Good to Simplify Clinimetry in Chronic Inflammatory Joint Diseases? J. Rheumatol. 2022, 49, 1079–1081. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Domain Number (Ordered According to FIP) | Domain and Short Defining Statement | % of Rheumatologists Considering This Domain a Priority (CVI) | Mean Importance | FIP |
|---|---|---|---|---|
| 1 | Pain (pain in joints, spine, and skin) * | 98% | 2.93 | 287.14 |
| 2 | Fatigue (being physically tired but also mental fatigue, lack of energy) * | 90% | 2.16 | 194.40 |
| 3 | Functional capacity (capacity to perform daily physical activities, loss of independence) * | 88% | 2.18 | 193.60 |
| 4 | Skin problems (including itching) * | 87% | 2.20 | 191.40 |
| 5 | Depressive mood (feeling sad or depressed) * | 71% | 2.01 | 142.71 |
| 6 | Patient global assessment (PtGA) of disease activity (patient’s overall experience of their disease) | 68% | 1.87 | 127.16 |
| 7 | Ability to work and for leisure (ability to work and/or do leisure activities) | 63% | 1.83 | 115.29 |
| 8 | Sleep disturbance (sleep quality, sleep interruptions) | 61% | 1.82 | 111.02 |
| 9 | Feeling of discomfort (discomfort and annoyance with everyday tasks) | 56% | 1.60 | 89.60 |
| 10 | Anxiety, fear, and uncertainty (e.g., about the future, treatments, fear of loneliness) | 55% | 1.61 | 88.55 |
| 11 | Embarrassment or shame due to appearance (feeling embarrassed/ashamed due to appearance) | 52% | 1.65 | 85.80 |
| 12 | Social participation (participating fully in social activities) | 49% | 1.69 | 82.81 |
| 13 | Relationship with family (relationship with family or people very close to you) | 47% | 1.60 | 75.20 |
| 14 | Concentration difficulties (difficulty concentrating and memorising) | 45% | 1.58 | 71.10 |
| 15 | Sexual life (sexual difficulties or dissatisfaction) | 40% | 1.80 | 72.00 |
| 16 | Coping (adjustment to the disease, managing, being in charge, making do with the disease) | 37% | 1.61 | 63.27 |
| 17 | Financial impact (experiencing financial loss due to treatment cost, work loss, early retirement, cost of assistive devices, etc) | 35% | 1.70 | 59.50 |
| Variables | Mean | Median | SD | IQR |
|---|---|---|---|---|
| Age (years) | 56.81 | 56.00 | 11.36 | 49.00–65.25 |
| Disease duration (years) | 8.36 | 8.00 | 5.23 | 3.00–12.00 |
| Educational level (years) | 11.13 | 13.00 | 3.25 | 8.00–13.00 |
| Comorbidites (number) | 2.61 | 3.00 | 1.91 | 1.00–4.00 |
| Sangha Index | 4.79 | 4.65 | 3.60 | 1.55–7.02 |
| TJC (68 joints) | 6.73 | 6.00 | 6.66 | 0.00–11.00 |
| SJC (66 ioints) | 3.71 | 4.00 | 3.87 | 0.00–6.00 |
| CRP (mg/dL) | 3.62 | 3.11 | 2.95 | 1.63–4.75 |
| LEI | 1.41 | 1.00 | 3.38 | 0.00–2.00 |
| Dactilitis (count) | 2.19 | 1.00 | 2.42 | 0.00–4.00 |
| PASI | 5.41 | 4.40 | 5.09 | 1.17–8.52 |
| HAQ | 1.08 | 1.12 | 0.70 | 0.50–1.62 |
| PsA-5Ts | 39.39 | 42.50 | 20.18 | 16.00–59.60 |
| DAPSA | 23.34 | 25.00 | 12.98 | 9.67–32.67 |
| CPDAI | 7.89 | 8.00 | 4.48 | 4.00–11.25 |
| PASDAS | 4.46 | 5.04 | 1.74 | 2.99–5.70 |
| PsAID-12 | 4.90 | 3.50 | 4.11 | 3.74–4.59 |
| SF-36 | 41.14 | 39.19 | 9.55 | 37.20–41.62 |
| DAPSA | CPDAI | PASDAS | |
|---|---|---|---|
| Lowest value | 3.92 | 0.00 | 0.54 |
| Highest value | 58.20 | 19.00 | 8.33 |
| Arithmetic mean | 23.34 | 7.76 | 4.49 |
| 95% CI for the arithmetic mean | 21.29–25.38 | 7.07–8.45 | 4.22–4.75 |
| Median | 25.00 | 8.00 | 5.00 |
| 95% CI for the median | 20.27–27.15 | 7.00–9.00 | 4.45–5.23 |
| Variance | 168.68 | 19.27 | 2.87 |
| Standard deviation | 12.98 | 4.38 | 1.69 |
| Relative standard deviation | 0.55 (55.64%) | 0.56 (56.54%) | 0.37 (37.77%) |
| Standard error of the mean | 1.03 | 0.35 | 0.13 |
| Coefficient of Skewness | 0.27 (p = 0.1563) | 0.032 (p = 0.8640) | −0.53 (p = 0.0073) |
| Coefficient of Kurtosis | −0.72 (p = 0.0050) | −0.97 (p < 0.0001) | −0.52 (p = 0.0887) |
| Shapiro–Wilk test for normal distribution | W = 0.94 reject normality (p < 0.0001) | W = 0.96 reject normality (p = 0.0003) | W = 0.94 reject normality (p < 0.0001) |
| CPDAI | PASDAS | PsA-5Ts | PSAID-12 | SF-36 | ||
|---|---|---|---|---|---|---|
| DAPSA | correlation coefficient p | 0.720 <0.0001 | 0.829 <0.0001 | 0.664 <0.0001 | 0.423 <0.0001 | −0.625 <0.0001 |
| CPDAI | correlation coefficient p | 0.766 <0.0001 | 0.582 <0.0001 | 0.402 <0.0001 | −0.592 <0.0001 | |
| PASDAS | correlation coefficient p | 0.694 <0.0001 | 0.529 <0.0001 | −0.639 <0.0001 | ||
| PsA-5Ts | correlation coefficient p | 0.735 <0.0001 | −0.469 <0.0001 | |||
| PsAID-12 | correlation coefficient p | −0.165 0.0389 | ||||
| Variable | AUC | SE a | 95% CI b |
|---|---|---|---|
| DAPSA | 0.963 | 0.014 | 0.920–0.986 |
| CPDAI | 0.924 | 0.021 | 0.871–0.961 |
| PASDAS | 0.955 | 0.016 | 0.909–0.981 |
| PsA-5Ts | 0.944 | 0.026 | 0.895–0.974 |
| PsAID-12 | 0.917 | 0.024 | 0.863–0.955 |
| SF-36 | 0.799 | 0.042 | 0.728–0.859 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salaffi, F.; Carotti, M.; Farah, S.; Di Carlo, M. The Psoriatic Arthritis 5-Thermometer Scales (PsA-5Ts): Measurement Properties of a New Multidimensional Composite Tool for the Quick Assessment of the Overall Health Status in Psoriatic Arthritis. J. Pers. Med. 2023, 13, 1153. https://doi.org/10.3390/jpm13071153
Salaffi F, Carotti M, Farah S, Di Carlo M. The Psoriatic Arthritis 5-Thermometer Scales (PsA-5Ts): Measurement Properties of a New Multidimensional Composite Tool for the Quick Assessment of the Overall Health Status in Psoriatic Arthritis. Journal of Personalized Medicine. 2023; 13(7):1153. https://doi.org/10.3390/jpm13071153
Chicago/Turabian StyleSalaffi, Fausto, Marina Carotti, Sonia Farah, and Marco Di Carlo. 2023. "The Psoriatic Arthritis 5-Thermometer Scales (PsA-5Ts): Measurement Properties of a New Multidimensional Composite Tool for the Quick Assessment of the Overall Health Status in Psoriatic Arthritis" Journal of Personalized Medicine 13, no. 7: 1153. https://doi.org/10.3390/jpm13071153