
Assisted Reproductive Technology and Breech Delivery: A Nationwide Cohort Study in Singleton Pregnancies
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
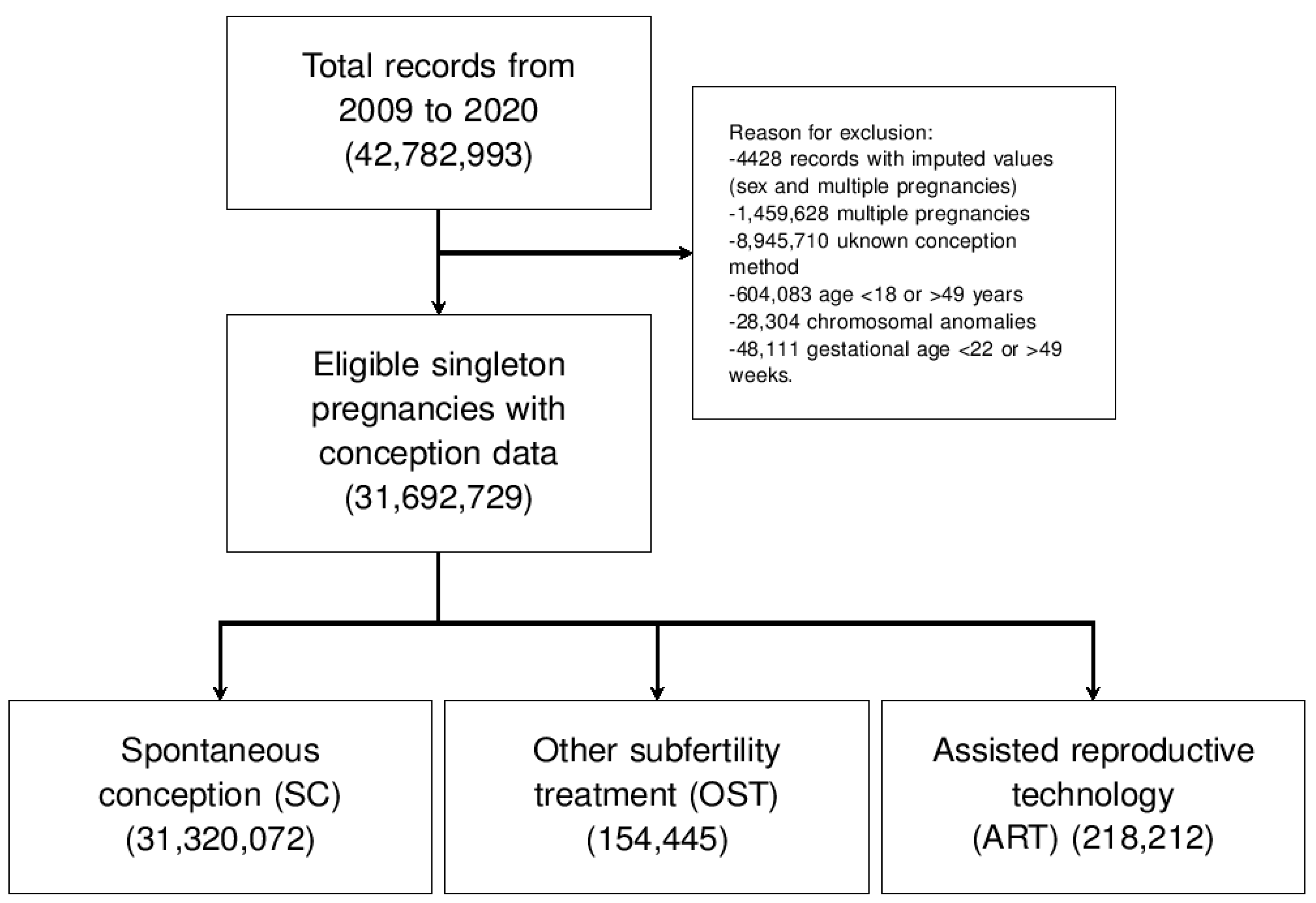
2.1. Design, Setting, and Sample
2.2. Variables
2.3. Data Analysis
3. Results
3.1. Population Characteristics
3.2. Population Characteristics and Mode of Conception
3.3. ART as a Risk Factor for Breech Presentation and Other Known Risk Factors
4. Discussion
4.1. Key Results
4.2. Interpretation and Comparison with the Literature
4.3. Strengths and Weaknesses
4.4. Generalizability, Relevance of the Findings, and Unanswered Questions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Steptoe, P.C.; Edwards, R.G. Birth after the reimplantation of a human embryo. Lancet 1978, 2, 366. [Google Scholar] [CrossRef] [PubMed]
- Romundstad, L.B.; Romundstad, P.R.; Sunde, A.; von Düring, V.; Skjaerven, R.; Vatten, L.J. Assisted fertilization and breech delivery: Risks and obstetric management. Hum. Reprod. 2009, 24, 3205–3210. [Google Scholar] [CrossRef] [Green Version]
- Boynukalin, F.K.; Turgut, N.E.; Gultomruk, M.; Ecemis, S.; Yarkiner, Z.; Findikli, N.; Bahceci, M. Impact of elective frozen vs. fresh embryo transfer strategies on cumulative live birth: Do deleterious effects still exist in normal & hyper responders? PLoS ONE 2020, 15, e0234481. [Google Scholar]
- Cobo, A.; de los Santos, M.J.; Castellò, D.; Gámiz, P.; Campos, P.; Remohí, J. Outcomes of vitrified early cleavage-stage and blastocyst-stage embryos in a cryopreservation program: Evaluation of 3,150 warming cycles. Fertil. Steril. 2012, 98, 1138–1146.e1. [Google Scholar] [CrossRef]
- Qin, J.B.; Sheng, X.Q.; Wu, D.; Gao, S.Y.; You, Y.P.; Yang, T.B.; Wang, H. Worldwide prevalence of adverse pregnancy outcomes among singleton pregnancies after in vitro fertilization/intracytoplasmic sperm injection: A systematic review and meta-analysis. Arch. Gynecol. Obstet. 2017, 295, 285–301. [Google Scholar] [CrossRef]
- Blockeel, C.; Drakopoulos, P.; Santos-Ribeiro, S.; Polyzos, N.P.; Tournaye, H. A fresh look at the freeze-all protocol: A SWOT analysis. Hum. Reprod. 2016, 31, 491–497. [Google Scholar] [CrossRef]
- Sha, T.; Yin, X.; Cheng, W.; Massey, I.Y. Pregnancy-related complications and perinatal outcomes resulting from transfer of cryopreserved versus fresh embryos invitro fertilization: A meta-analysis. Fertil Steril. 2018, 109, 330–342.e9. [Google Scholar] [CrossRef] [Green Version]
- Maheshwari, A.; Pandey, S.; AmalrajRaja, E.; Shetty, A.; Hamilton, M.; Bhattacharya, S. Is frozen embryo transfer better for mothers and babies? Can. cumulative meta-analysis provide a definitive answer? Hum. Reprod. Update 2018, 24, 35–58. [Google Scholar] [CrossRef] [Green Version]
- Rietberg, C.C.T.; Elferink-Stinkens, P.M.; Brand, R.; van Loon, A.J.; Van Hemel, O.J.S.; Visser, G.H.A. Term breech presentation in The Netherlands from 1995 to 1999, Mortality and morbidity in relation to the mode of delivery of 33824 infants. BJOG 2003, 110, 604–609. [Google Scholar] [CrossRef]
- Lumbiganon, P.; Laopaiboon, M.; Gülmezoglu, A.M.; Souza, J.P.; Taneepanichskul, S.; Ruyan, P.; Attygalle, D.E.; Shrestha, N.; Mori, R.; Nguyen, D.H.; et al. Method of delivery and pregnancy outcomes in Asia: The WHO global survey on maternal and perinatal health 2007-08. Lancet 2010, 375, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Fruscalzo, A.; Londero, A.P.; Salvador, S.; Bertozzi, S.; Biasioli, A.; Della Martina, M.; Driul, L.; Marchesoni, D. New and old predictive factors for breech presentation: Our experience in 14 433 singleton pregnancies and a literature review. J. Matern. Fetal Neonatal Med. 2014, 27, 167–172. [Google Scholar] [CrossRef] [Green Version]
- Hannah, M.E.; Hannah, W.J.; Hewson, S.A.; Hodnett, E.D.; Saigal, S.; Willan, A.R. Planned caesarean section versus planned vaginal birth for breech presentation at term: A randomised multicentre trial. Term Breech Trial Collaborative Group. Lancet 2000, 356, 1375–1383. [Google Scholar] [CrossRef]
- Hannah, M.E.; Hannah, W.J.; Hodnett, E.D.; Chalmers, B.; Kung, R.; Willan, A.; Amankwah, K.; Cheng, M.; Helewa, M.; Hewson, S.; et al. Outcomes at 3 months after planned cesarean vs planned vaginal delivery for breech presentation at term: The international randomized Term Breech Trial. JAMA 2002, 287, 1822–1831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isaksson, R.; Gissler, M.; Tiitinen, A. Obstetric outcome among women with unexplained infertility after IVF: A matched case-control study. Hum. Reprod. 2002, 17, 1755–1761. [Google Scholar] [CrossRef] [Green Version]
- Ombelet, W.; Cadron, I.; Gerris, J.; DeSutter, P.; Bosmans, E.; Martens, G.; Ruyssinck, G.; Defoort, P.; Molenberghs, G.; Gyselaers, W. Obstetric and perinatal outcome of 1655 ICSI and 3974 IVF singleton and 1102 ICSI and 2901 IVF twin births: A comparative analysis. Reprod. Biomed. Online 2005, 11, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Zádori, J.; Kozinszky, Z.; Orvos, H.; Katona, M.; Pál, A.; Kovács, L. Dilemma of increased obstetric risk in pregnancies following IVF-ET. J. Assist. Reprod. Genet. 2003, 20, 216–221. [Google Scholar] [CrossRef] [Green Version]
- Weiniger, C.F.; Lyell, D.J.; Tsen, L.C.; Butwick, A.J.; Shachar, B.; Callaghan, W.M.; Creanga, A.A.; Bateman, B.T. Maternal outcomes of term breech presentation delivery: Impact of successful external cephalic version in a nationwide sample of delivery admissions in the United States. BMC Pregnancy Childbirth 2016, 16, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macharey, G.; Toijonen, A.; Hinnenberg, P.; Gissler, M.; Heinonen, S.; Ziller, V. Term cesarean breech delivery in the first pregnancy is associated with an increased risk for maternal and neonatal morbidityinthe subsequent delivery: A national cohort study. Arch. Gynecol. Obstet. 2020, 302, 85–91. [Google Scholar] [CrossRef]
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.K.; Driscoll, A.K. Births: Final Data for 2019. Natl. Vital Stat. Rep. 2021, 70, 1–51. [Google Scholar] [PubMed]
- Soneji, S.; Beltrán-Sánchez, H. Association of Maternal Cigarette Smoking and Smoking Cessation with Preterm Birth. JAMA Netw. Open 2019, 2, e192514. [Google Scholar] [CrossRef] [Green Version]
- Sunderam, S.; Kissin, D.M.; Zhang, Y.; Jewett, A.; Boulet, S.L.; Warner, L.; Kroelinger, C.D.; Barfield, W.D. Assisted Reproductive Technology Surveillance—United States, 2017. MMWR Surveill Summ. 2020, 69, 1–20. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Moaddab, A.; Bateni, Z.H.; Dildy, G.A.; Clark, S.L. Poor compliance and lack of improvement in birth certificate reporting of assisted reproductive technology pregnancies in the United States. Am. J. Obstet. Gynecol. 2016, 215, 528–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thoma, M.E.; Boulet, S.; Martin, J.A.; Kissin, D. Births resulting from assisted reproductive technology: Comparing birth certificate and National ART Surveillance System Data, 2011. Natl. Vital Stat. Rep. 2014, 63, 1–11. [Google Scholar]
- Tierney, K.; Cai, Y. Assisted reproductive technology use in the United States: A population assessment. Fertil. Steril. 2019, 112, 1136–1143.e4. [Google Scholar] [CrossRef]
- Albrechtsen, S.; Rasmussen, S.; Dalaker, K.; Irgens, L.M. The occurrence of breech presentation in Norway 1967–1994. Acta Obstet. Gynecol. Scand. 1998, 77, 410–415. [Google Scholar]
- Ezra, Y.; McParland, P.; Farine, D. High delivery intervention rates in nulliparous women over age 35. Eur. J. Obstet. Gynecol. Reprod. Biol. 1995, 62, 203–207. [Google Scholar] [CrossRef]
- Fawole, A.O.; Adeyemi, A.S.; Adewole, I.F.; Omigbodun, A.O. A ten-year review of breech deliveries at Ibadan. Afr. J. Med. Med. Sci. 2001, 30, 87–90. [Google Scholar]
- Fox, A.J.S.; Chapman, M.G. Longitudinal ultrasound assessment of fetal presentation: A review of 1010 consecutive cases. Aust. N. Z. J. Obstet. Gynaecol. 2006, 46, 341–344. [Google Scholar] [CrossRef]
- Getahun, D.; Strickland, D.; Lawrence, J.M.; Fassett, M.J.; Koebnick, C.; Jacobsen, S.J. Racial and ethnic disparities in the trends in primary cesarean delivery based on indications. Am. J. Obstet. Gynecol. 2009, 201, 422.e1–422.e7. [Google Scholar] [CrossRef]
- Jolly, M.; Sebire, N.; Harris, J.; Robinson, S.; Regan, L. The risks associated with pregnancy in women aged 35 years or older. Hum. Reprod. 2000, 15, 2433–2437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kale, A.; Kuyumcuoğlu, U.; Güzel, A. Is pregnancy over 45 with very high parity related with adverse maternal and fetal outcomes? Clin. Exp. Obstet. Gynecol. 2009, 36, 120–122. [Google Scholar] [PubMed]
- Kalogiannidis, I.; Masouridou, N.; Dagklis, T.; Masoura, S.; Goutzioulis, M.; Prapas, Y.; Prapas, N. Previous cesarean section increases the risk for breech presentation at term pregnancy. Clin. Exp. Obstet. Gynecol. 2010, 37, 29–32. [Google Scholar] [PubMed]
- Nordtveit, T.I.; Melve, K.K.; Albrechtsen, S.; Skjaerven, R. Maternal and paternal contribution to intergenerational recurrence of breech delivery: Population based cohort study. BMJ 2008, 336, 872–876. [Google Scholar] [CrossRef] [Green Version]
- Rayl, J.; Gibson, P.J.; Hickok, D.E. A population-based case-control study of risk factors for breech presentation. Am. J. Obstet. Gynecol. 1996, 174, 28–32. [Google Scholar] [CrossRef]
- Roberts, C.L.; Algert, C.S.; Peat, B.; Henderson-Smart, D. Small fetal size: A risk factor for breech birth at term. Int. J. Gynaecol. Obstet. 1999, 67, 1–8. [Google Scholar] [CrossRef]
- Vendittelli, F.; Rivière, O.; Crenn-Hébert, C.; Rozan, M.A.; Maria, B.; Jacquetin, B.; AUDIPOG Sentinel Network. Is a breech presentation at term more frequent in women with a history of cesarean delivery? Am. J. Obstet. Gynecol. 2008, 198, 521.e1–521.e6. [Google Scholar] [CrossRef]
- Witkop, C.T.; Zhang, J.; Sun, W.; Troendle, J. Natural history of fetal position during pregnancy and risk of nonvertex delivery. Obstet. Gynecol. 2008, 111, 875–880. [Google Scholar] [CrossRef]
- Londero, A.P.; Salvador, S.; Fruscalzo, A.; Bertozzi, S.; Biasioli, A.; Ceraudo, M.; Visentin, S.; Driul, L.; Marchesoni, D. First trimester PAPP-A MoM values predictive for breech presentation at term of pregnancy. Gynecol. Endocrinol. 2013, 29, 503–507. [Google Scholar] [CrossRef]
- Fenton, T.R.; Kim, J.H. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013, 13, 59. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Frydman, R.; Belaisch-Allart, J.; Fries, N.; Hazout, A.; Glissant, A.; Testart, J. An obstetric assessment of the first 100 births from the in vitro fertilization program at Clamart, France. Am. J. Obstet. Gynecol. 1986, 154, 550–555. [Google Scholar] [CrossRef]
- Poikkeus, P.; Gissler, M.; Unkila-Kallio, L.; Hyden-Granskog, C.; Tiitinen, A. Obstetric and neonatal outcome after single embryo transfer. Hum. Reprod. 2007, 22, 1073–1079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romundstad, L.B.; Romundstad, P.R.; Sunde, A.; von Düring, V.; Skjaerven, R.; Gunnell, D.; Vatten, L.J. Effects of technology or maternal factors on perinatal outcome after assisted fertilisation: A population-based cohort study. Lancet 2008, 372, 737–743. [Google Scholar] [CrossRef] [PubMed]
- Londero, A.P.; Bertozzi, S.; Visentin, S.; Fruscalzo, A.; Driul, L.; Marchesoni, D. High placental index and poor pregnancy outcomes: A retrospective study of 18,386 pregnancies. Gynecol. Endocrinol. 2013, 29, 666–669. [Google Scholar] [CrossRef] [PubMed]
- Londero, A.P.; Orsaria, M.; Parisi, N.; Tassi, A.; Pittini, C.; Driul, L.; Mariuzzi, L. In vitro fertilization is associated with placental accelerated villous maturation. Int. J. Clin. Exp. Pathol. 2021, 14, 734–740. [Google Scholar]
- Terho, A.M.; Pelkonen, S.; Opdahl, S.; Romundstad, L.B.; Bergh, C.; Wennerholm, U.B.; Henningsen, A.A.; Pinborg, A.; Gissler, M.; Tiitinen, A. High birth weight and large-for-gestational-age in singletons born after frozen compared to fresh embryo transfer, by gestational week: A Nordic register study from the CoNARTaS group. Hum. Reprod. 2021, 36, 1083–1092. [Google Scholar] [CrossRef]
- Källén, B.; Finnström, O.; Nygren, K.G.; OtterbladOlausson, P.; Wennerholm, U.B. In vitro fertilisation in Sweden: Obstetric characteristics, maternal morbidity and mortality. BJOG 2005, 112, 1529–1535. [Google Scholar] [CrossRef]
- Danielian, P.J.; Wang, J.; Hall, M.H. Long-term outcome by method of delivery of fetuses in breech presentation at term: Population based follow up. BMJ 1996, 312, 1451–1453. [Google Scholar] [CrossRef] [Green Version]
- Dieke, A.C.; Zhang, Y.; Kissin, D.M.; Barfield, W.D.; Boulet, S.L. Disparities in Assisted Reproductive Technology Utilization by Race and Ethnicity, United States, 2014, A Commentary. J. Womens Health 2017, 26, 605–608. [Google Scholar] [CrossRef]
- Lin, P.C. Reproductive outcomes in women with uterine anomalies. J. Womens Health 2004, 13, 33–39. [Google Scholar] [CrossRef]
- Grimbizis, G.F.; Camus, M.; Tarlatzis, B.C.; Bontis, J.N.; Devroey, P. Clinical implications of uterine malformations and hysteroscopic treatment results. Hum. Reprod. Update 2001, 7, 161–174. [Google Scholar] [CrossRef] [PubMed]
- Klatsky, P.C.; Tran, N.D.; Caughey, A.B.; Fujimoto, V.Y. Fibroids and reproductive outcomes: A systematic literature review from conception to delivery. Am. J. Obstet. Gynecol. 2008, 198, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Johnson, G.; MacLehose, R.F.; Baird, D.D.; Laughlin-Tommaso, S.K.; Hartmann, K.E. Uterine leiomyomata and fecundability in the Right from the Start study. Hum. Reprod. 2012, 27, 2991–2997. [Google Scholar] [CrossRef] [Green Version]
- Stewart, E.A.; Laughlin-Tommaso, S.K.; Catherino, W.H.; Lalitkumar, S.; Gupta, D.; Vollenhoven, B. Uterine fibroids. Nat. Rev. Dis. Primers. 2016, 2, 16043. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| SC (31,320,072) | OST (154,445) | ART (218,212) | p | |
|---|---|---|---|---|
| Patient characteristics | ||||
| Maternal age (years) | 28.00 (24.00–33.00) | 32.00 (29.00–36.00) | 35.00 (32.00–39.00) | 1, 2, 3 |
| Pre-gestational BMI (kg/m2) | 25.20 (22.00–30.10) | 25.50 (22.10–31.10) | 24.40 (21.70–28.80) | 1, 2, 3 |
| Nulliparity | 31.11% (9,742,763/31,320,072) | 45.24% (69,878/154,445) | 41.03% (89,533/218,212) | 1, 2, 3 |
| Black-only race | 15.04% (4,709,420/31,320,072) | 4.61% (7116/154,445) | 5.26% (11,481/218,212) | 1, 2, 3 |
| Hispanic origin | 25.75% (7,998,917/31,063,364) | 8.26% (12,659/153,317) | 8.35% (17,729/212,222) | 1, 2 |
| Tobacco smoke | 7.42% (2,280,828/30,727,907) | 1.40% (2139/152,715) | 0.52% (1129/216,231) | 1, 2, 3 |
| Previous CD | 15.14% (4,743,336/31,320,072) | 11.65% (17,988/154,445) | 14.01% (30,578/218,212) | 1, 2, 3 |
| Gestational age (weeks) | 39.00 (38.00–40.00) | 39.00 (38.00–40.00) | 39.00 (38.00–40.00) | 1, 2, 3 |
| Neonatal female sex | 48.81% (15,286,830/31,320,072) | 48.83% (75,413/154,445) | 48.88% (106,663/218,212) | NS |
| Birth weight (grams) | 3323.00 (3005.00–3646.00) | 3326.00 (2990.00–3657.00) | 3340.00 (2984.00–3671.00) | 1, 2, 3 |
| Birth weight (MoM) | 0.99 (0.89–1.08) | 0.99 (0.90–1.08) | 1.00 (0.90–1.10) | 1, 2, 3 |
| Pregnancy and labor characteristics | ||||
| Fetal presentation | ||||
| Cephalic | 94.19% (29,500,700/31,320,072) | 92.99% (143,625/154,445) | 91.46% (199,568/218,212) | 1, 2, 3 |
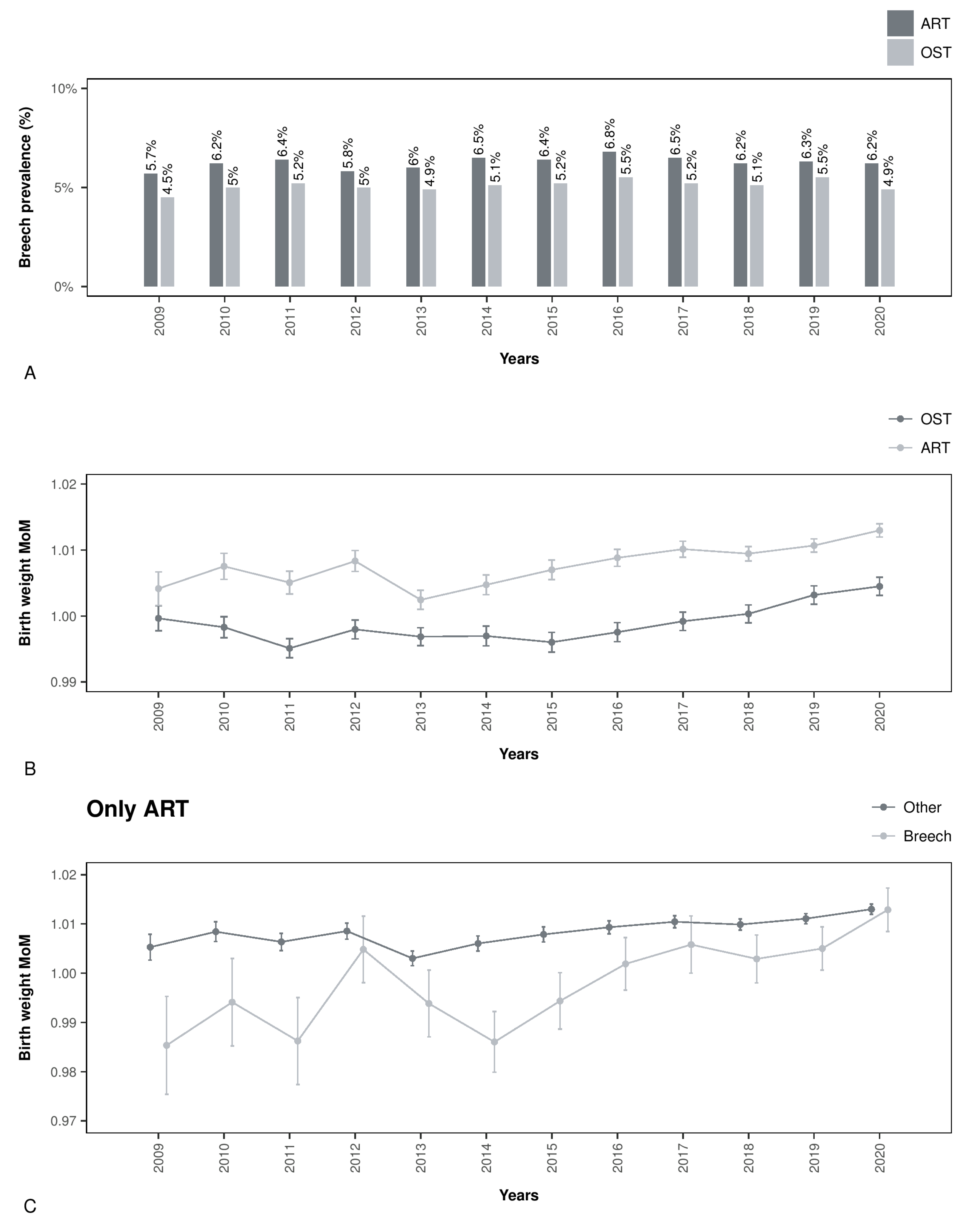
| Breech | 2.97% (930,310/31,320,072) | 5.12% (7909/154,445) | 6.32% (13,790/218,212) | 1, 2, 3 |
| Other | 1.45% (452,897/31,320,072) | 1.18% (1826/154,445) | 1.27% (2769/218,212) | 1, 2, 3 |
| Unknown | 1.39% (436,165/31,320,072) | 0.70% (1085/154,445) | 0.96% (2085/218,212) | 1, 2, 3 |
| Mode of delivery | ||||
| Spontaneous | 65.85% (20,623,069/31,320,072) | 55.69% (86,010/154,445) | 46.93% (10,2413/218,212) | 1, 2, 3 |
| Forceps | 0.56% (174,834/31,320,072) | 1.15% (1778/154,445) | 1.20% (2609/218,212) | 1, 2 |
| Vacuum | 2.67% (835,247/31,320,072) | 3.86% (5955/154,445) | 4.11% (8978/218,212) | 1, 2, 3 |
| Cesarean | 30.88% (9,672,623/31,320,072) | 39.27% (60,658/154,445) | 47.73% (104,156/218,212) | 1, 2, 3 |
| Unknown | 0.05% (14,299/31,320,072) | 0.03% (44/154,445) | 0.03% (56/218,212) | 1, 2 |
| OR (CI.95) | p | OR (CI.95) (*) (¶) | p (*) (¶) | |
|---|---|---|---|---|
| Factors associated with breech | ||||
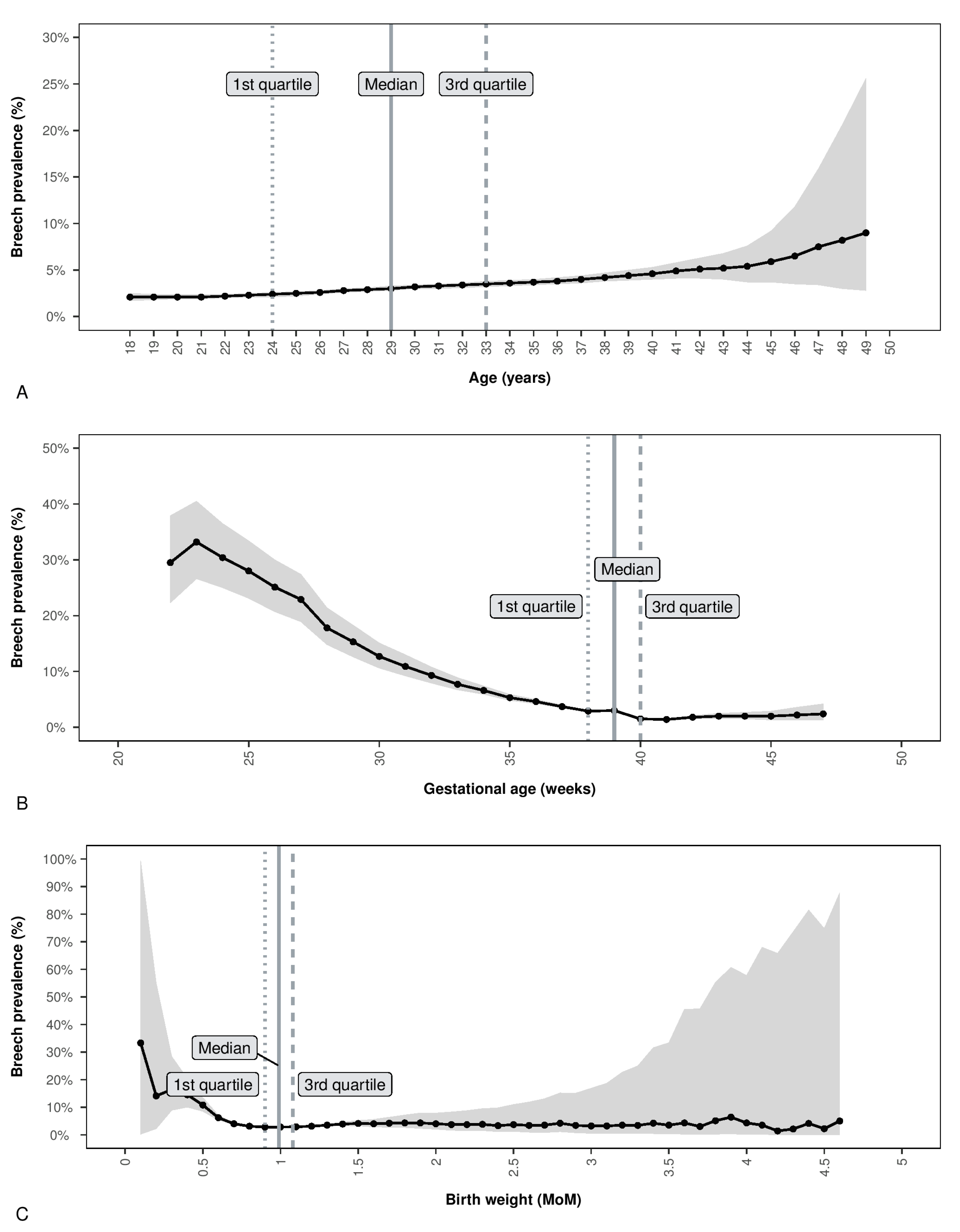
| Maternal age >33 years | 1.49 (1.48–1.49) | <0.001 | 1.39 (1.38–1.41) | <0.001 |
| Nulliparity | 1.36 (1.35–1.36) | <0.001 | 1.79 (1.78–1.81) | <0.001 |
| Black only race | 0.77 (0.76–0.77) | <0.001 | 0.75 (0.74–0.76) | <0.001 |
| Hispanic origin (†) | 0.82 (0.82–0.83) | <0.001 | 0.81 (0.8–0.82) | <0.001 |
| Tobacco smoke (‡) | 1.13 (1.12–1.13) | <0.001 | 1.18 (1.16–1.2) | <0.001 |
| Previous CD | 1.28 (1.28–1.29) | <0.001 | 1.53 (1.51–1.55) | <0.001 |
| Neonatal female sex | 1.15 (1.14–1.15) | <0.001 | 1.2 (1.19–1.21) | <0.001 |
| Gestational age > 40 weeks | 0.48 (0.48–0.49) | <0.001 | 0.41 (0.4–0.42) | <0.001 |
| Birth weight (MoM) (§) | ||||
| <0.90 MoM | 1.2 (1.2–1.21) | <0.001 | 1.47 (1.46–1.49) | <0.001 |
| 0.90–1.07 MoM | Reference | 1.000 | Reference | 1.000 |
| >1.07 MoM | 1.13 (1.13–1.14) | <0.001 | 1.06 (1.05–1.07) | <0.001 |
| OST | 1.75 (1.71–1.79) | <0.001 | 1.79 (1.71–1.87) | <0.001 |
| ART | 2.2 (2.16–2.23) | <0.001 | 2.32 (2.23–2.41) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Londero, A.P.; Massarotti, C.; Xholli, A.; Fruscalzo, A.; Cagnacci, A. Assisted Reproductive Technology and Breech Delivery: A Nationwide Cohort Study in Singleton Pregnancies. J. Pers. Med. 2023, 13, 1144. https://doi.org/10.3390/jpm13071144
Londero AP, Massarotti C, Xholli A, Fruscalzo A, Cagnacci A. Assisted Reproductive Technology and Breech Delivery: A Nationwide Cohort Study in Singleton Pregnancies. Journal of Personalized Medicine. 2023; 13(7):1144. https://doi.org/10.3390/jpm13071144
Chicago/Turabian StyleLondero, Ambrogio P., Claudia Massarotti, Anjeza Xholli, Arrigo Fruscalzo, and Angelo Cagnacci. 2023. "Assisted Reproductive Technology and Breech Delivery: A Nationwide Cohort Study in Singleton Pregnancies" Journal of Personalized Medicine 13, no. 7: 1144. https://doi.org/10.3390/jpm13071144