
Morphological Variation of the Mandible in the Orthognathic Population—A Morphological Study Using Statistical Shape Modelling

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
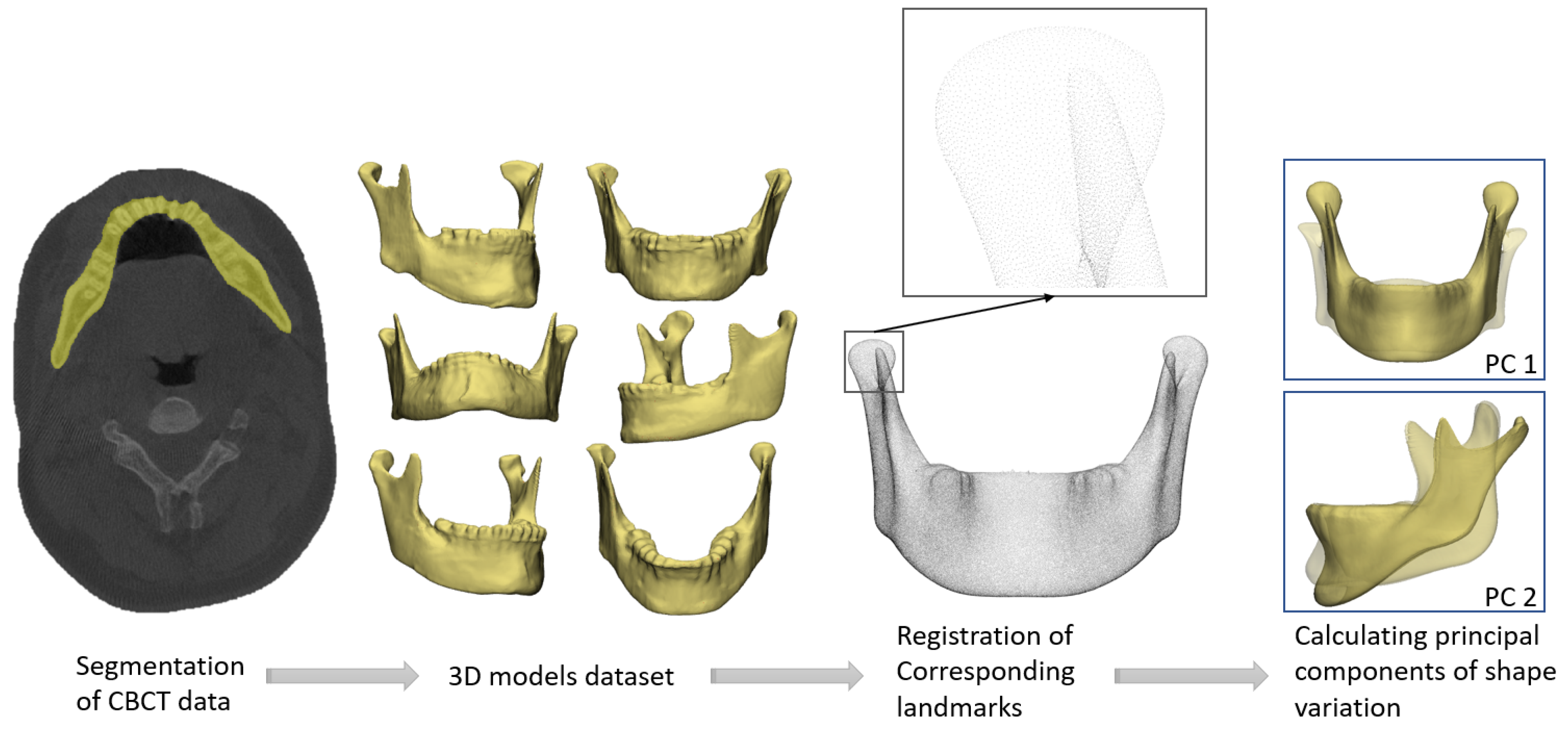
2.2. Generation of 3D Models
2.3. Statistical Shape Model
2.4. Evaluation of the Statistical Shape Model
2.5. Difference between Male and Female Mandibles
3. Results
3.1. Inclusion and Evaluation of the Statistical Shape Model
3.2. Orthognathic Population Shape Variation
3.3. D VSP Based on the Principal Components of Orthognathic Shape Variation
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gunson, M.J.; Arnett, G. Orthognathic virtual treatment planning for functional esthetic results. Semin. Orthod. 2019, 25, 230–247. [Google Scholar] [CrossRef]
- Swennen, G.R.; Mollemans, W.; Schutyser, F. Three-Dimensional Treatment Planning of Orthognathic Surgery in the Era of Virtual Imaging. J. Oral Maxillofac. Surg. 2009, 67, 2080–2092. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.T.; Lin, H.H.; Liou, E.J.W.; Lo, L.J. Three-dimensional surgical simulation improves the planning for correction of facial prognathism and asymmetry: A qualitative and quantitative study. Sci. Rep. 2017, 7, 40423. [Google Scholar] [CrossRef] [PubMed]
- Bashour, M. History and Current Concepts in the Analysis of Facial Attractiveness. Plast. Reconstr. Surg. 2006, 118, 741–756. [Google Scholar] [CrossRef] [PubMed]
- Raffaini, M.; Arcuri, F. Fully Digitalized Workflow for One-Stage Mandibular Contouring and Orthognathic Surgery to Correct Severe Facial Asymmetry. Aesthetic Plast. Surg. 2022, 46, 2905–2911. [Google Scholar] [CrossRef] [PubMed]
- La Padula, S.; Hersant, B.; Chatel, H.; Aguilar, P.; Bosc, R.; Roccaro, G.; Ruiz, R.; Meningaud, J.P. One-step facial feminization surgery: The importance of a custom-made preoperative planning and patient satisfaction assessment. J. Plast. Reconstr. Aesthetic Surg. 2019, 72, 1694–1699. [Google Scholar] [CrossRef] [PubMed]
- Qiu, B.; van der Wel, H.V.D.; Kraeima, J.; Glas, H.H.; Guo, J.; Borra, R.J.H.; Witjes, M.J.H.; van Ooijen, P.M.A.V. Robust and Accurate Mandible Segmentation on Dental CBCT Scans Affected by Metal Artifacts Using a Prior Shape Model. J. Pers. Med. 2021, 11, 364. [Google Scholar] [CrossRef] [PubMed]
- Manu. nonrigidICP. MATLAB Central File Exchange. 2022. Available online: https://www.mathworks.com/matlabcentral/fileexchange/41396-nonrigidicp (accessed on 12 September 2022).
- Styner, M.A.; Rajamani, K.T.; Nolte, L.P.; Zsemlye, G.; Székely, G.; Taylor, C.J.; Davies, R.H. Evaluation of 3D Correspondence Methods for Model Building. Lect. Notes Comput. Sci. 2003, 18, 63–75. [Google Scholar] [CrossRef]
- Gollmer, S.T.; Buzug, T.M. A method for quantitative evaluation of statistical shape models using morphometry. In Proceedings of the 2010 IEEE International Symposium on Biomedical Imaging: From Nano to Macro 2010, Rotterdam, The Netherlands, 14–17 April 2010. [Google Scholar] [CrossRef]
- Vancleef, S.; Herteleer, M.; Carette, Y.; Herijgers, P.; Duflou, J.R.; Nijs, S.; Vander Sloten, J. Why off-the-shelf clavicle plates rarely fit: Anatomic analysis of the clavicle through statistical shape modeling. J. Shoulder Elb. Surg. 2019, 28, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.; Tran, K.L.; D’heygere, E.; Prisman, E. Predicting the Premorbid Shape of a Diseased Mandible. Laryngoscope 2020, 131, E781–E786. [Google Scholar] [CrossRef] [PubMed]
- Raith, S.; Wolff, S.; Steiner, T.; Modabber, A.; Weber, M.; Hölzle, F.; Fischer, H. Planning of mandibular reconstructions based on statistical shape models. Int. J. Comput. Assist. Radiol. Surg. 2016, 12, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Zachow, S.; Lamecker, H.; Elsholtz, B.; Stiller, M. Reconstruction of mandibular dysplasia using a statistical 3D shape model. Int. Congr. Ser. 2005, 1281, 1238–1243. [Google Scholar] [CrossRef]
- Vallabh, R.; Zhang, J.; Fernandez, J.; Dimitroulis, G.; Ackland, D.C. The morphology of the human mandible: A computational modelling study. Biomech. Model. Mechanobiol. 2019, 19, 1187–1202. [Google Scholar] [CrossRef] [PubMed]
- Raith, S.; Varga, V.; Steiner, T.; Hölzle, F.; Fischer, H. Computational geometry assessment for morphometric analysis of the mandible. Comput. Methods Biomech. Biomed. Eng. 2016, 20, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Chaweeborisuit, P.; Yurasakpong, L.; Kruepunga, N.; Tubbs, R.S.; Chaiyamoon, A.; Suwannakhan, A. The prevalence of Stafne bone cavity: A meta-analysis of 355,890 individuals. J. Dent. Sci. 2022, 18, 594–603. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PC | Mean Male Weighting Factor | Mean Female Weighting Factor | Mean Difference | p-Value |
|---|---|---|---|---|
| 1 | 0.23 ± 0.89 | −0.11 ± 1.03 | 0.34 | 0.026 |
| 3 | −0.33 ± 0.86 | 0.01 ± 0.98 | 0.49 | <0.001 |
| 5 | 0.41 ± 1.02 | −0.21 ± 0.93 | 0.61 | <0.001 |
| 6 | −0.34 ± 0.97 | 0.17 ± 0.98 | 0.50 | <0.001 |
| 8 | 0.24 ± 0.92 | −0.12 ± 1.02 | 0.36 | 0.017 |
| 13 | 0.38 ± 0.99 | −0.18 ± 0.96 | 0.56 | <0.001 |
| 20 | −0.21 ± 0.95 | 0.10 ± 1.01 | 0.31 | 0.042 |
| 24 | 0.24 ± 1.07 | −0.12 ± 0.94 | 0.36 | 0.018 |
| 29 | −0.32 ± 1.01 | 0.16 ± 0.96 | 0.47 | 0.002 |
| 43 | −0.23 ± 1.10 | 0.11 ± 0.93 | 0.33 | 0.029 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van der Wel, H.; Qiu, B.; Spijkervet, F.K.L.; Jansma, J.; Schepers, R.H.; Kraeima, J. Morphological Variation of the Mandible in the Orthognathic Population—A Morphological Study Using Statistical Shape Modelling. J. Pers. Med. 2023, 13, 854. https://doi.org/10.3390/jpm13050854
van der Wel H, Qiu B, Spijkervet FKL, Jansma J, Schepers RH, Kraeima J. Morphological Variation of the Mandible in the Orthognathic Population—A Morphological Study Using Statistical Shape Modelling. Journal of Personalized Medicine. 2023; 13(5):854. https://doi.org/10.3390/jpm13050854
Chicago/Turabian Stylevan der Wel, Hylke, Bingjiang Qiu, Fred K. L. Spijkervet, Johan Jansma, Rutger H. Schepers, and Joep Kraeima. 2023. "Morphological Variation of the Mandible in the Orthognathic Population—A Morphological Study Using Statistical Shape Modelling" Journal of Personalized Medicine 13, no. 5: 854. https://doi.org/10.3390/jpm13050854