
Increased Red Blood Cell Distribution Predicts Severity of Chronic Obstructive Pulmonary Disease Exacerbation

Abstract
:1. Introduction
2. Materials and Methods
- Active cancer.
- The patient has a diagnosis of connective tissue disorder, inflammatory bowel disease, or hematological system diseases (such as malignancy, thalassemia, hemolytic anemia).
- The patient was treated with blood transfusion or anti-inflammatory drug (systemic steroids, immunosuppressive drugs) in the last 2 months.
3. Variables
- The maximal partial pressure of carbon dioxide in the arterial blood (PaCO2) during hospital stay.
- The length of hospital stay.
4. Statistics
5. Results
5.1. Demographic and Clinical Characteristics of the Patients
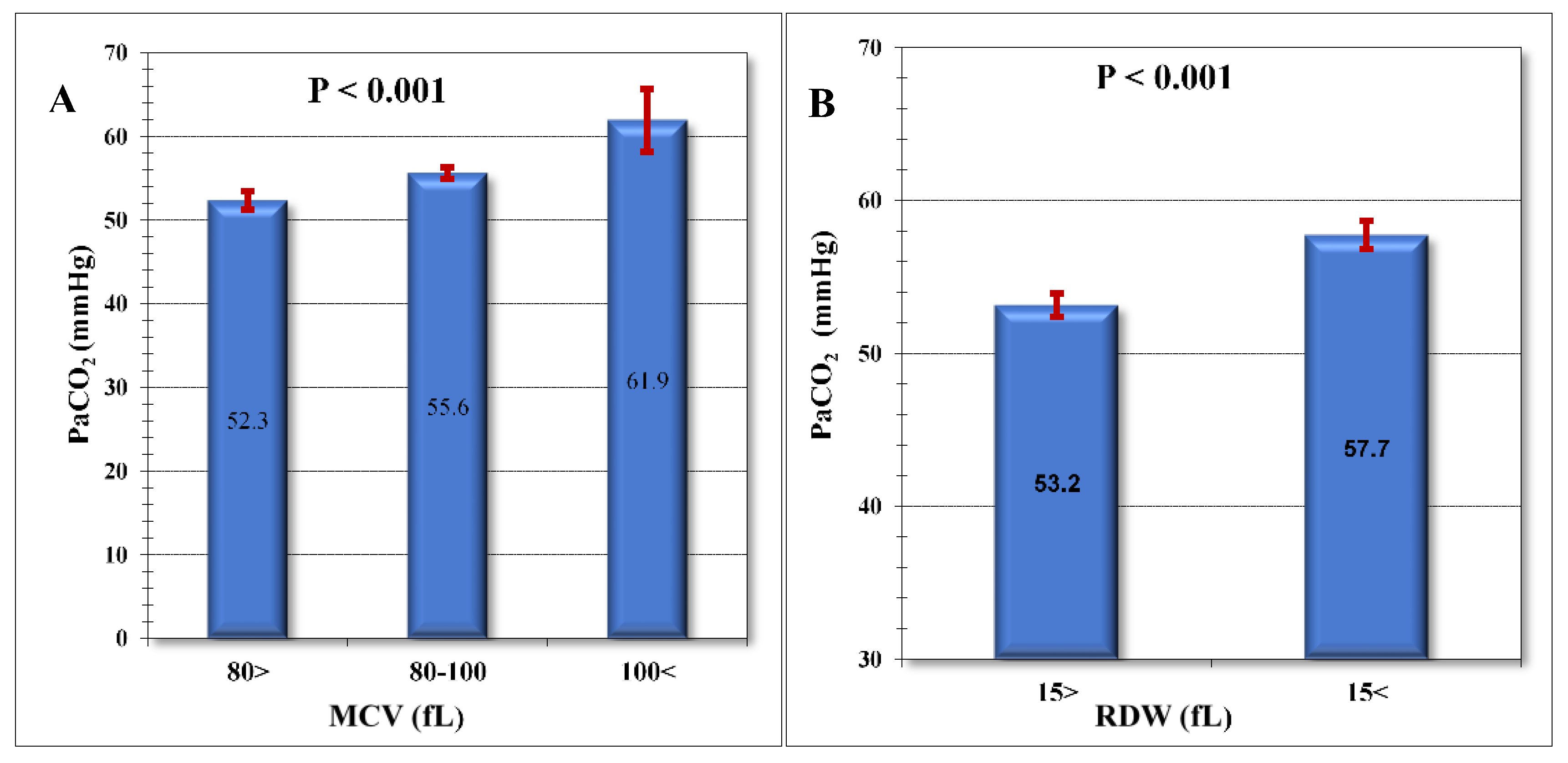
5.2. The Correlation between Maximal PaCO2 during Hospitalization and CBC Parameters
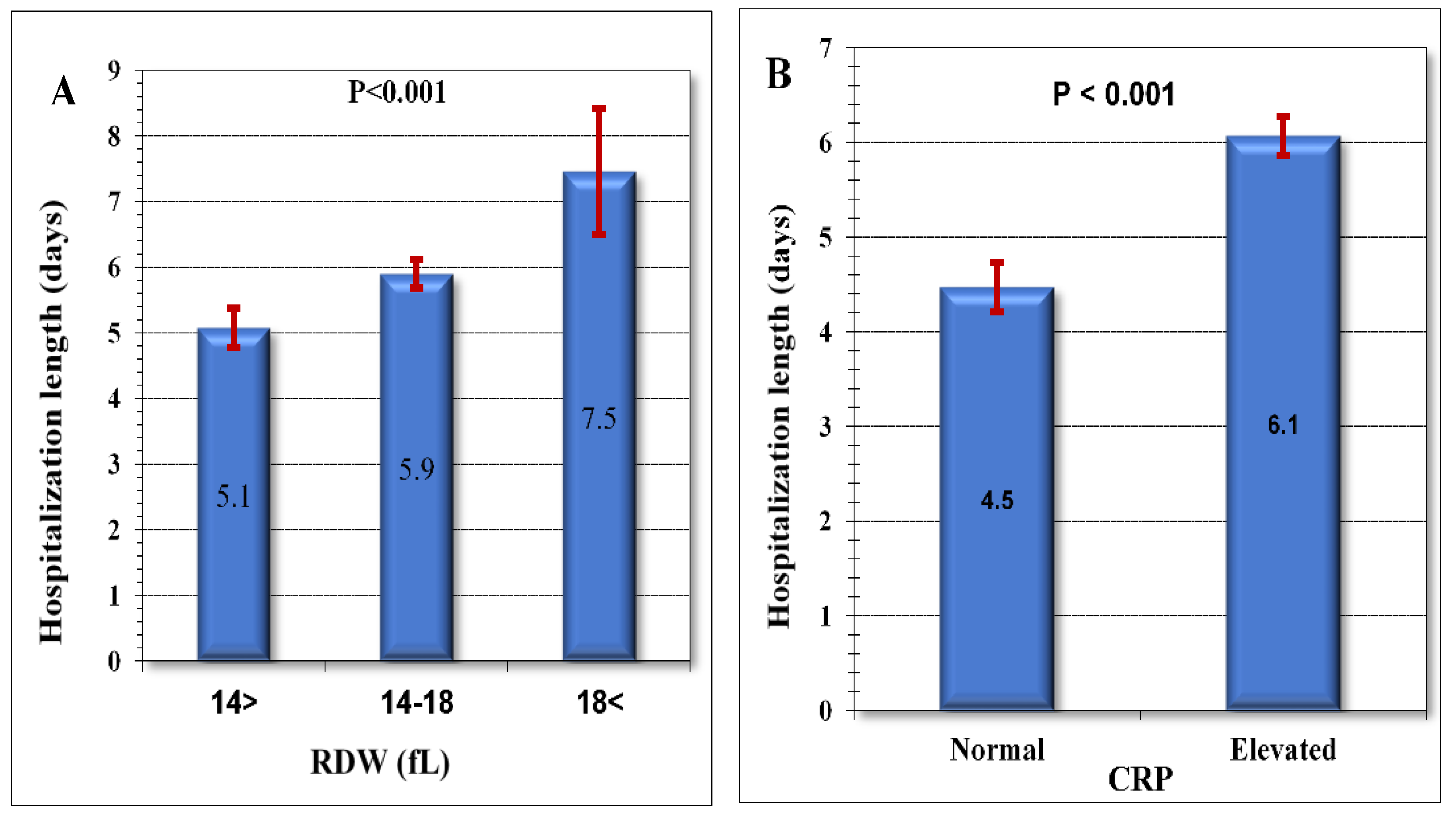
5.3. The Correlation between Hospitalization Duration and CBC Parameters
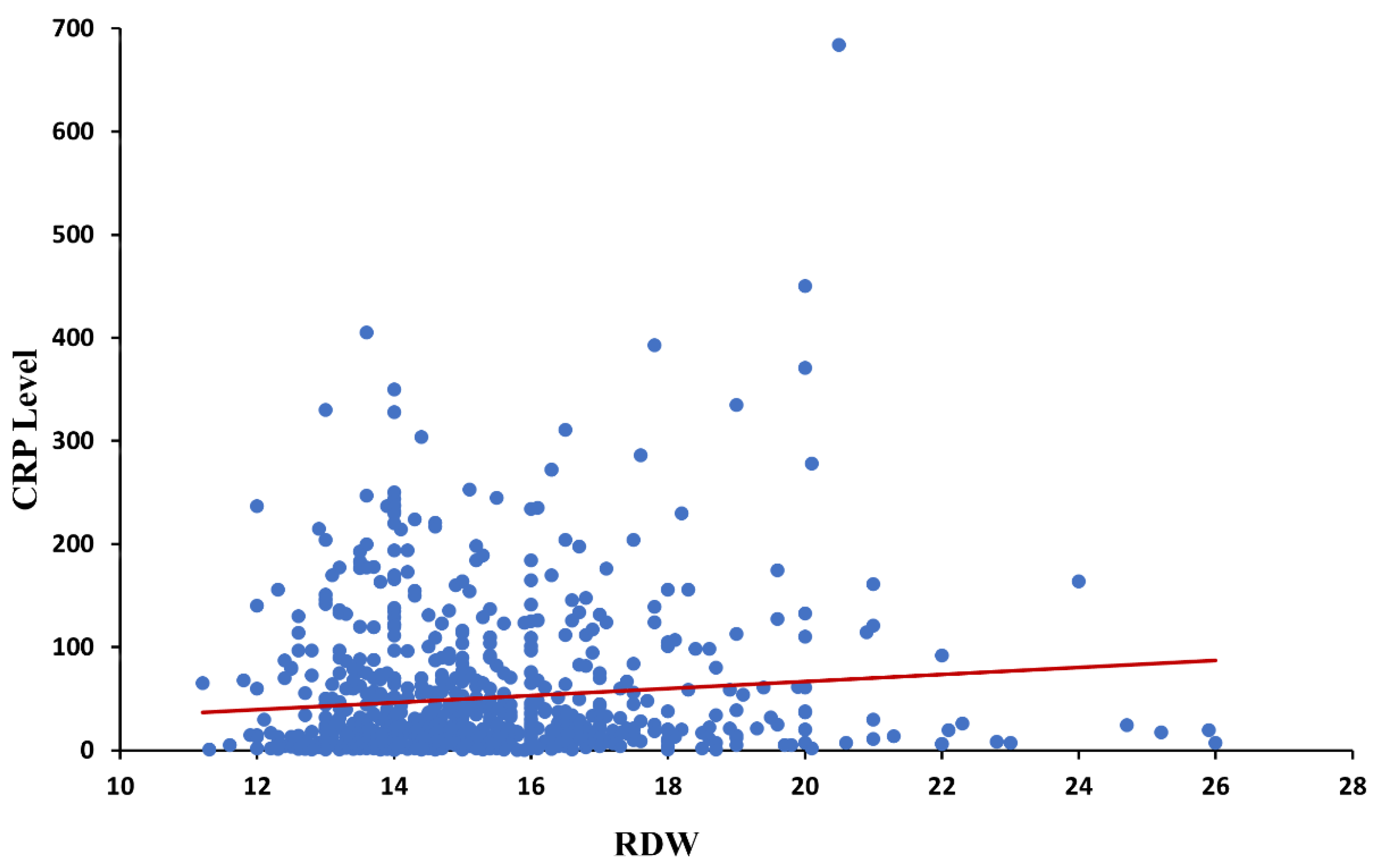
5.4. CRP and Its Correlation with CBC Papameters
6. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- Celli, B.R.; Fabbri, L.M.; Aaron, S.D.; Agusti, A.; Brook, R.; Criner, G.J.; Franssen, F.M.E.; Humbert, M.; Hurst, J.R.; O’donnell, D.; et al. An updated definition and severity classification of COPD exacerbations: The Rome proposal. Am. J. Respir. Crit. Care Med. 2021, 204, 1251–1258. [Google Scholar] [CrossRef] [PubMed]
- Miravitlles, M.; Guerrero, T.; Mayordomo, C.; Sánchez-Agudo, L.; Nicolau, F.; Segú, J.L. Factors associated with increased risk of exacerbation and hospital admission in a cohort of ambulatory COPD patients: A multiple logistic regression analysis. Respiration 2000, 67, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Rascon-Aguilar, I.E.; Pamer, M.; Wludyka, P.; Cury, J.; Coultas, D.; Lambiase, L.R.; Nahman, N.S.; Vega, K.J. Role of gastroesophageal reflux symptoms in exacerbations of COPD. Chest 2006, 130, 1096–1101. [Google Scholar] [CrossRef]
- Niewoehner, D.E.; Lokhnygina, Y.; Rice, K.; Kuschner, W.G.; Sharafkhaneh, A.; Sarosi, G.A.; Krumpe, P.; Pieper, K.; Kesten, S. Risk indexes for exacerbations and hospitalizations due to COPD. Chest 2007, 131, 20–28. [Google Scholar] [CrossRef]
- Burgel, P.-R.; Nesme-Meyer, P.; Chanez, P.; Caillaud, D.; Carré, P.; Perez, T.; Roche, N. Cough and sputum production are associated with frequent exacerbations and hospitalizations in COPD subjects. Chest 2009, 135, 975–982. [Google Scholar] [CrossRef]
- Sapey, E.; Bafadhel, M.; Bolton, C.; Wilkinson, T.; Hurst, J.R.; Quint, J.K. Building toolkits for COPD exacerbations: Lessons from the past and present. Thorax 2019, 74, 898–905. [Google Scholar] [CrossRef]
- Beasley, V.; Joshi, P.V.; Singanayagam, A.; Molyneaux, P.L.; Johnston, S.L.; Mallia, P. Lung microbiology and exacerbations in COPD. Int. J. Chronic Obstr. Pulm. Dis. 2012, 7, 555–569. [Google Scholar] [CrossRef]
- Duffy, N.; Walker, P.; Diamantea, F.; Calverley, P.M.A.; Davies, L. Intravenous aminophylline in patients admitted to hospital with non-acidotic exacerbations of chronic obstructive pulmonary disease: A prospective randomised controlled trial. Thorax 2005, 60, 713–717. [Google Scholar] [CrossRef]
- Calverley, P.M.; Page, C.; Negro, R.W.D.; Fontana, G.; Cazzola, M.; Cicero, A.F.; Pozzi, E.; Wedzicha, J.A. Effect of Erdosteine on COPD Exacerbations in COPD Patients with Moderate Airflow Limitation. Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 2733–2744. [Google Scholar] [CrossRef]
- Maclay, J.D.; McAllister, D.A.; Macnee, W. Cardiovascular risk in chronic obstructive pulmonary disease. Respirology 2007, 12, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Berry, C.E.; Wise, R.A. Mortality in COPD: Causes, risk factors, and prevention. COPD 2010, 7, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Aulakh, R.; Sohi, I.; Singh, T.; Kakkar, N. Red cell distribution width (RDW) in the diagnosis of iron deficiency with microcytic hypochromic anemia. Indian J. Pediatr. 2009, 76, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Gottfried, E.L. Erythrocyte indexes with the electronic counter. N. Engl. J. Med. 1979, 300, 1277. [Google Scholar] [CrossRef] [PubMed]
- Seppä, K.; Sillanaukee, P.; Saarni, M. Blood count and hematologic morphology in non-anemic macrocytosis: Differences between alcohol abuse and pernicious anemia. Alcohol 1993, 10, 343–347. [Google Scholar] [CrossRef] [PubMed]
- Pierce, C.N.; Larson, D.F. Inflammatory cytokine inhibition of erythropoiesis in patients implanted with a mechanical circulatory asist device. Perfusion 2005, 20, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Ozkalemkas, F.; Ali, R.; Ozkocaman, V.; Ozcelik, T.; Ozan, U.; Ozturk, H.; Kurt, E.; Evrensel, T.; Yerci, O.; Tunali, A. The bone marrow aspirate and biopsy in the diagnosis of unsuspected non hematologic malignancy: A clinical study of 19 cases. BMC Cancer 2005, 5, 144. [Google Scholar] [CrossRef]
- Lippi, G.; Targher, G.; Montagnana, M.; Salvagno, G.L.; Zoppini, G.; Guidi, G.C. Relation between red blood cell distribution width and inflammatory biomarkers in a large cohort of unselected outpatients. Arch. Pathol. Lab. Med. 2009, 133, 628–632. [Google Scholar] [CrossRef]
- Hampole, C.V.; Mehrotra, A.K.; Thenappan, T.; Gomberg-Maitland, M.; Shah, S.J. Usefulness of red cell distribution width as a prognostic marker in pulmonary hypertension. Am. J. Cardiol. 2009, 104, 868–872. [Google Scholar] [CrossRef]
- Allen, L.A.; Felker, G.M.; Mehra, M.R.; Chiong, J.R.; Dunlap, S.H.; Ghali, J.K.; Lenihan, D.J.; Oren, R.M.; Wagoner, L.E.; Schwartz, T.A.; et al. Validation and potential mechanisms of red cell distribution width as a prognostic marker in heart failure. J. Card. Fail. 2010, 16, 230–238. [Google Scholar] [CrossRef]
- Tonelli, M.; Sacks, F.; Arnold, M.; Moye, L.; Davis, B.; Pfeffer, M.; for the Cholesterol and Recurrent Events (CARE) Trial Investigators. Relation Between Red Blood Cell Distribution Width and Cardiovascular Event Rate in People with Coronary Disease. Circulation 2008, 117, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Oudijk, E.J.; Lammers, J.W.; Koenderman, L. Systemic inflammation in chronic obstructive pulmonary disease. Eur. Respir. J. 2003, 22, 5–13. [Google Scholar] [CrossRef]
- Gan, W.Q.; Man, S.F.P.; Senthilselvan, A.; Sin, D.D. Association between chronic obstructive pulmonary disease and systemic inflammation: A systematic review and a meta-analysis. Thorax 2004, 59, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Palange, P.; Testa, U.; Huertas, A.; Calabrò, L.; Antonucci, R.; Petrucci, E.; Pelosi, E.; Pasquini, L.; Satta, A.; Morici, G.; et al. Circulating haemopoietic and endothelial progenitor cells are decreased in COPD. Eur. Respir. J. 2006, 27, 529–541. [Google Scholar] [CrossRef] [PubMed]
- Schols, A.M.; Buurman, W.A.; Staal van den Brekel, A.J.; Dentener, M.A.; Wouters, E.F. Evidence for a relation between metabolic derangements and increased levels of inflammatory mediators in a subgroup of patients with chronic obstructive pulmonary disease. Thorax 1996, 51, 819–824. [Google Scholar] [CrossRef]
- Anderson, J.L.; Ronnow, B.S.; Horne, B.D.; Carlquist, J.F.; May, H.T.; Bair, T.L.; Jensen, K.R.; Muhlestein, J.B. Usefulness of a complete blood count-derived risk score to predict incident mortality in patients with suspected cardiovascular disease. Am. J. Cardiol. 2007, 99, 169–174. [Google Scholar] [CrossRef]
- Borné, Y.; Smith, J.G.; Melander, O.; Hedblad, B.; Engström, G. Red cell distribution width and risk for first hospitalization due to heart failure: A population-based cohort study. Eur. J. Heart Fail. 2011, 13, 1355–1361. [Google Scholar] [CrossRef]
- Van Kimmenade, R.R.; Mohammed, A.A.; Uthamalingam, S.; Van Der Meer, P.; Felker, G.M.; Januzzi, J.L., Jr. Red blood cell distribution width and 1-year mortality in acute heart failure. Eur. J. Heart Fail. 2010, 12, 129–136. [Google Scholar] [CrossRef]
- Lappé, J.M.; Horne, B.D.; Shah, S.H.; May, H.T.; Muhlestein, J.B.; Lappé, D.L.; Kfoury, A.G.; Carlquist, J.F.; Budge, D.; Alharethi, R.; et al. Red cell distribution width, C-reactive protein, the complete blood count, and mortality in patients with coronary disease and a normal comparison population. Clin. Chim. Acta 2011, 412, 2094–2099. [Google Scholar] [CrossRef]
- Zorlu, A.; Bektasoglu, G.; Guven, F.M.K.; Dogan, O.T.; Gucuk, E.; Ege, M.R.; Altay, H.; Cınar, Z.; Tandogan, I.; Yilmaz, M.B. Usefulness of admission red cell distribution width as a predictor of early mortality in patients with acute pulmonary embolism. Am. J. Cardiol. 2012, 109, 128–134. [Google Scholar] [CrossRef]
- Dabbah, S.; Hammerman, H.; Markiewicz, W.; Aronson, D. Relation between red cell distribution width and clinical outcomes after acute myocardial infarction. Am. J. Cardiol. 2010, 105, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Pasquale, M.K.; Sun, S.X.; Song, F.; Hartnett, H.J.; Stemkowski, S.A. Impact of exacerbations on health care cost and resource utilization in chronic obstructive pulmonary disease patients with chronic bronchitis from a predominantly Medicare population. Int. J. Chronic Obstr. Pulm. Dis. 2012, 7, 757–764. [Google Scholar] [CrossRef] [PubMed]
- Mittmann, N.; Kuramoto, L.; Seung, S.J.; Haddon, J.M.; Bradley-Kennedy, C.; Fitzgerald, J.M. The cost of moderate and severe COPD exacerbations to the Canadian Healthcare System. Respir. Med. 2008, 102, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Ke, X.; Marvel, J.; Yu, T.-C.; Wertz, D.; Geremakis, C.; Wang, L.; Stephenson, J.J.; Mannino, D.M. Impact of lung function on exacerbations, health care utilization, and costs among patients with COPD. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 1689–1703. [Google Scholar] [CrossRef]
- Faustini, A.; Marino, C.; D’Ippoliti, D.; Forastiere, F.; Belleudi, V.; Perucci, C.A. The impact on risk-factor analysis of different mortality outcomes in COPD patients. Eur. Respir. J. 2008, 32, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C.M.; Lowe, D.; Bucknall, C.E.; Ryland, I.; Kelly, Y.; Pearson, M.G. Clinical audit indicators of outcome following admission to hospital with acute exacerbation of chronic obstructive pulmonary disease. Thorax 2002, 57, 137–141. [Google Scholar] [CrossRef]
- Seyhan, E.C.; Özgül, M.A.; Tutar, N.; Ömür, I.M.; Uysal, A.; Altın, S. Red blood cell distribution and survival in patients with chronic obstructive pulmonary disease. COPD 2013, 10, 416–424. [Google Scholar] [CrossRef]
- Sincer, I.; Zorlu, A.; Yilmaz, M.B.; Dogan, O.T.; Ege, M.R.; Amioglu, G.; Aydin, G.; Ardic, I.; Tandogan, I. Relationship between red cell distribution width and right ventricular dysfunction in patients with chronic obstructive pulmonary disease. Heart Lung 2012, 41, 238–243. [Google Scholar] [CrossRef]
- Dahl, M.; Vestbo, J.; Lange, P.; Bojesen, S.E.; Tybjærg-Hansen, A.; Nordestgaard, B.G. C-reactive protein as a predictor of prognosis in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2007, 175, 250–255. [Google Scholar] [CrossRef]
- Seppä, K.; Heinilä, K.; Sillanaukee, P.; Saarni, M. Evaluation of macrocytosis by general practitioners. J. Stud. Alcohol 1996, 57, 97–100. [Google Scholar] [CrossRef]
- Savage, D.G.; Ogundipe, A.; Lindenbaum, J.; Stabler, S.P.; Hallen, R. Etiology and diagnostic evaluation of macrocytosis. Am. J. Med. Sci. 2000, 319, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, M.Y.; Lugon, M.; Anderson, C.C. Unexplained macrocytosis in elderly patients. Age Ageing 1996, 25, 310–312. [Google Scholar] [CrossRef] [PubMed]
- Christou, L.; Pappas, G.; Falagas, M.E. Bacterial infection-related morbidity and mortality in cirrhosis. Am. J. Gastroenterol. 2007, 102, 1510–1517. [Google Scholar] [CrossRef] [PubMed]
- Albillos, A.; Lario, M.; Álvarez-Mon, M. Cirrhosis-associated immune dysfunction: Distinctive features and clinical relevance. J. Hepatol. 2014, 61, 1385–1396. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Numer of Patients | |
|---|---|
| Total study group | 804 patients |
| Men, number (%) | 534 (66.4%) |
| Women, number (%) | 270 (33.6%) |
| Age, mean ± SD (years) | 67.7 years (±13) |
| Mean Age, men (year) | 68.3 years |
| Mean Age, Women (year) | 67.2 years |
| Patients with anemia, number (%) | 317 (39.4%) |
| Male patient with anemia, number (%) | 191 (35.8%) |
| Female patient with anemia, number (%) | 126 (46.7%) |
| A | ||||||
|---|---|---|---|---|---|---|
| Coefficient | 95% Conf. (±) | Std. Error | T | p Value | ||
| Constant | ||||||
| MCV | 0.34 | 0.15 | 0.07 | 4.3 | 0.00001 | |
| RDW | 1.36 | 0.6 | 0.3 | 4.4 | 0.00001 | |
| B | ||||||
| Constant | ||||||
| MCV | 0.35 | 0.15 | 0.07 | 4.6 | 0.00001 | |
| RDW | 0.007 | 0.004 | 0.002 | 3.15 | 0.001 |
| Correlations | ||||||
|---|---|---|---|---|---|---|
| HB | MCV | RDW | PLT | MPV | ||
| CRP | Correlation coefficient | −0.018 | 0.011 | 0.098 | 0.051 | 0.015 |
| One-sided significance | 0.30 | 0.37 | 0.001 | 0.06 | 0.32 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saad, E.; Maamoun, B.; Nimer, A. Increased Red Blood Cell Distribution Predicts Severity of Chronic Obstructive Pulmonary Disease Exacerbation. J. Pers. Med. 2023, 13, 843. https://doi.org/10.3390/jpm13050843
Saad E, Maamoun B, Nimer A. Increased Red Blood Cell Distribution Predicts Severity of Chronic Obstructive Pulmonary Disease Exacerbation. Journal of Personalized Medicine. 2023; 13(5):843. https://doi.org/10.3390/jpm13050843
Chicago/Turabian StyleSaad, Elias, Basheer Maamoun, and Assy Nimer. 2023. "Increased Red Blood Cell Distribution Predicts Severity of Chronic Obstructive Pulmonary Disease Exacerbation" Journal of Personalized Medicine 13, no. 5: 843. https://doi.org/10.3390/jpm13050843