
Depression and Anxiety in Heart Transplant Recipients: Prevalence and Impact on Post-Transplant Outcomes

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Retrieval
2.2. Patient Population
2.3. Statistics
3. Results
3.1. Patient Characteristics
3.2. In-Hospital Treatment
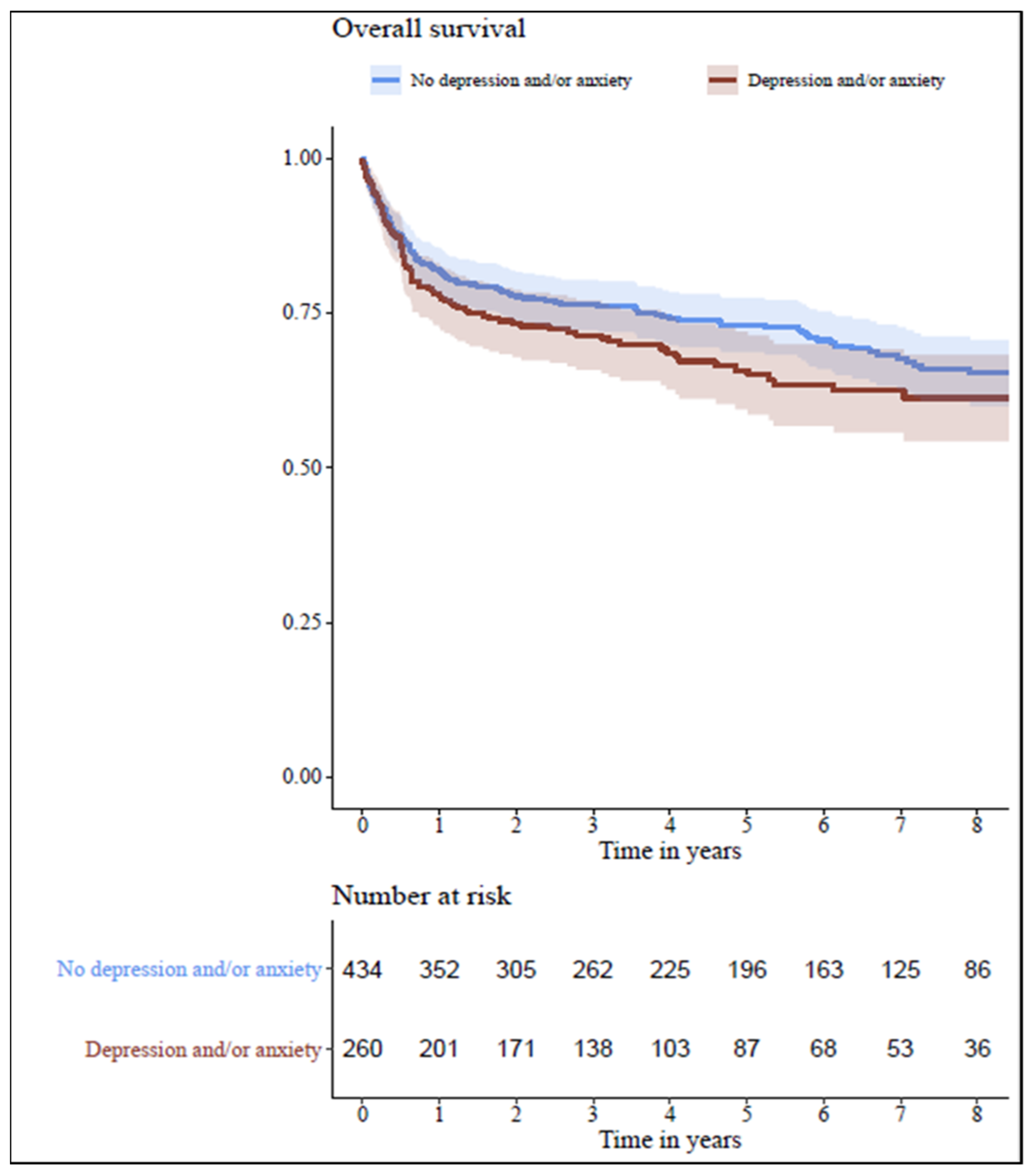
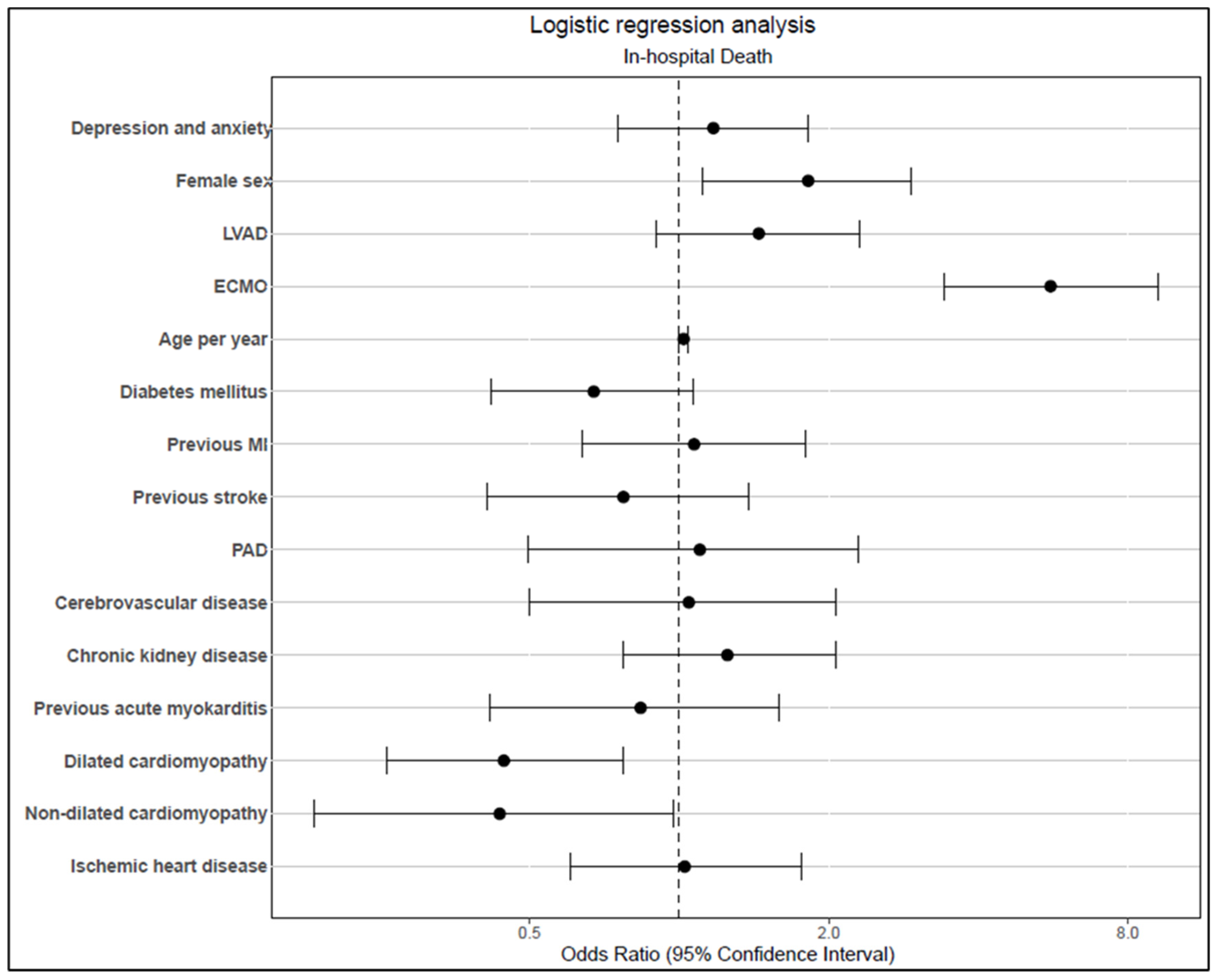
3.3. Outcome
4. Discussion
4.1. Pretransplant Diagnoses and CVRF
4.2. In-Hospital Treatment
4.3. Relapse or Post-Transplant DA
4.4. Outcome
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Depression and Other Common Mental Disorders: Global Health Estimates. World Health Organization. 2017. Available online: http://www.who.int/mental_health/management/depression/prevalence_global_health_estimates/en (accessed on 21 March 2023).
- Chapman, D.P.; Perry, G.S.; Strine, T.W. The vital link between chronic disease and depressive disorders. Prev. Chronic Dis. 2005, 2, A14. [Google Scholar] [PubMed]
- Celano, C.M.; Villegas, A.C.; Albanese, A.M.; Gaggin, H.K.; Huffman, J.C. Depression and Anxiety in Heart Failure: A Review. Harv. Rev. Psychiatry. 2018, 26, 175–184. [Google Scholar] [CrossRef]
- Rutledge, T.; Reis, V.A.; Linke, S.E.; Greenberg, B.H.; Mills, P.J. Depression in heart failure a meta-analytic review of prevalence, intervention effects, and associations with clinical outcomes. J. Am. Coll. Cardiol. 2006, 48, 1527–1537. [Google Scholar] [CrossRef] [PubMed]
- Delibasic, M.; Mohamedali, B.; Dobrilovic, N.; Raman, J. Pre-transplant depression as a predictor of adherence and morbidities after orthotopic heart transplantation. J. Cardiothorac. Surg. 2017, 12, 62. [Google Scholar] [CrossRef]
- Costanzo, M.R.; Dipchand, A.; Starling, R.; Anderson, A.; Chan, M.; Desai, S.; Fedson, S.; Fisher, P.; Gonzales-Stawinski, G.; Martinelli, L.; et al. The International Society of Heart and Lung Transplantation Guidelines for the care of heart transplant recipients. J. Heart Lung Transplant. 2010, 29, 914–956. [Google Scholar] [CrossRef]
- García-Cosío, M.D.; González-Vilchez, F.; López-Vilella, R.; Barge-Caballero, E.; Gómez-Bueno, M.; Martínez-Selles, M.; Arizón, J.M.; Rangel Sousa, D.; González-Costello, J. Gender differences in heart transplantation: Twenty-five year trends in the nationwide Spanish heart transplant registry. Clin. Transplant. 2020, 34, e14096. [Google Scholar] [CrossRef] [PubMed]
- Ronaldson, A.; Arias de la Torre, J.; Prina, M.; Armstrong, D.; Das-Munshi, J.; Hatch, S.; Stewart, R.; Hotopf, M.; Dregan, A. Associations between physical multimorbidity patterns and common mental health disorders in middle-aged adults: A prospective analysis using data from the UK Biobank. Lancet Reg. Health Eur. 2021, 8, 100149. [Google Scholar] [CrossRef] [PubMed]
- Grenard, J.L.; Munjas, B.A.; Adams, J.L.; Suttorp, M.; Maglione, M.; McGlynn, E.A.; Gellad, W.F. Depression and medication adherence in the treatment of chronic diseases in the United States: A meta-analysis. J. Gen. Intern. Med. 2011, 26, 1175–1182. [Google Scholar] [CrossRef]
- Hare, D.L.; Toukhsati, S.R.; Johansson, P.; Jaarsma, T. Depression and cardiovascular disease: A clinical review. Eur. Heart J. 2014, 35, 1365–1372. [Google Scholar] [CrossRef]
- Health Quality Ontario. Screening and management of depression for adults with chronic diseases: An evidence-based analysis. Ont. Health Technol. Assess Ser. 2013, 13, 1–45. [Google Scholar]
- Mehra, M.R.; Canter, C.E.; Hannan, M.M.; Semigran, M.J.; Uber, P.A.; Baran, D.A.; Danziger-Isakov, L.; Kirklin, J.K.; Kirk, R.; Kushwaha, S.S. The 2016 International Society for Heart Lung Transplantation listing criteria for heart transplantation: A 10-year update. J. Heart Lung Transplant. 2016, 35, 1–23. [Google Scholar] [CrossRef]
- Fergusson, D.M.; Goodwin, R.D.; Horwood, L.J. Major depression and cigarette smoking: Results of a 21-year longitudinal study. Psychol. Med. 2003, 33, 1357–1367. [Google Scholar] [CrossRef]
- Breslau, N.; Peterson, E.L.; Schultz, L.R.; Chilcoat, H.D.; Andreski, P. Major depression and stages of smoking. A longitudinal investigation. Arch. Gen. Psychiatry 1998, 55, 161–166. [Google Scholar] [CrossRef]
- Flensborg-Madsen, T.; von Scholten, M.B.; Flachs, E.M.; Mortensen, E.L.; Prescott, E.; Tolstrup, J.S. Tobacco smoking as a risk factor for depression. A 26-year population-based follow-up study. J. Psychiatr. Res. 2011, 45, 143–149. [Google Scholar] [CrossRef]
- Vaccarino, V.; Badimon, L.; Bremner, J.D.; Cenko, E.; Cubedo, J.; Dorobantu, M.; Duncker, D.J.; Koller, A.; Manfrini, O.; Milicic, D.; et al. Depression and coronary heart disease: 2018 position paper of the ESC working group on coronary pathophysiology and microcirculation. Eur. Heart J. 2020, 41, 1687–1696. [Google Scholar] [CrossRef]
- Lichtman, J.H.; Bigger, J.T.; Blumenthal, J.A.; Frasure-Smith, N.; Kaufmann, P.G.; Lespérance, F.; Mark, D.B.; Sheps, D.S.; Taylor, C.B.; Froelicher, E.S. AHA science advisory. Depression and coronary heart disease. Recommendations for screening, referral, and treatment. A science advisory from the American Heart Association Prevention Committee to the Council on Cardiovascular Nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention, and Interdisciplinary Council on Quality of Care Outcomes Research. Endorsed by the American Psychiatric Association. Prog. Cardiovasc. Nurs. 2009, 24, 19–26. [Google Scholar]
- Linden, W.; Vodermaier, A.; Mackenzie, R.; Greig, D. Anxiety and depression after cancer diagnosis: Prevalence rates by cancer type, gender, and age. J. Affect. Disord. 2012, 141, 343–351. [Google Scholar] [CrossRef]
- Zipfel, S.; Löwe, B.; Paschke, T.; Immel, B.; Lange, R.; Zimmermann, R.; Herzog, W.; Bergmann, G. Psychological distress in patients awaiting heart transplantation. J. Psychosom. Res. 1998, 45, 465–470. [Google Scholar] [CrossRef]
- Renoux, C.; Vahey, S.; Dell’Aniello, S.; Boivin, J.F. Association of Selective Serotonin Reuptake Inhibitors with the Risk for Spontaneous Intracranial Hemorrhage. JAMA Neurol. 2017, 74, 173–180. [Google Scholar] [CrossRef]
- Schalekamp, T.; Klungel, O.H.; Souverein, P.C.; de Boer, A. Increased bleeding risk with concurrent use of selective serotonin reuptake inhibitors and coumarins. Arch. Intern. Med. 2008, 168, 180–185. [Google Scholar] [CrossRef]
- Hoirisch-Clapauch, S.; Nardi, A.E. Antidepressants: Bleeding or thrombosis? Thromb. Res. 2019, 181 (Suppl. S1), S23–S28. [Google Scholar] [CrossRef]
- Spina, E.; Barbieri, M.A.; Cicala, G.; Bruno, A.; de Leon, J. Clinically relevant drug interactions between newer antidepressants and oral anticoagulants. Expert Opin. Drug Metab. Toxicol. 2020, 16, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Labos, C.; Dasgupta, K.; Nedjar, H.; Turecki, G.; Rahme, E. Risk of bleeding associated with combined use of selective serotonin reuptake inhibitors and antiplatelet therapy following acute myocardial infarction. Can. Med. Assoc. J. 2011, 183, 1835–1843. [Google Scholar] [CrossRef] [PubMed]
- Olff, M. Stress, depression and immunity: The role of defense and coping styles. Psychiatry Res. 1999, 85, 7–15. [Google Scholar] [CrossRef]
- Wilhelm, M.J. Long-term outcome following heart transplantation: Current perspective. J. Thorac. Dis. 2015, 7, 549–551. [Google Scholar]
- Aziz, T.; Burgess, M.; Rahman, A.N.; Campbell, C.S.; Yonan, N. Cardiac transplantation for cardiomyopathy and ischemic heart disease: Differences in outcome up to 10 years. J. Heart Lung Transplant. 2001, 20, 525–533. [Google Scholar] [CrossRef]
- Khush, K.K.; Cherikh, W.S.; Chambers, D.C.; Harhay, M.O.; Hayes, D., Jr.; Hsich, E.; Meiser, B.; Potena, L.; Robinson, A.; Rossano, J.W.; et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-sixth adult heart transplantation report-2019; focus theme: Donor and recipient size match. J. Heart Lung Transplant. 2019, 38, 1056–1066. [Google Scholar] [CrossRef]
- De Santo, L.S.; Marra, C.; De Feo, M.; Amarelli, C.; Romano, G.; Cotrufo, M. The impact of gender on heart transplantation outcomes: A single center experience. Ital. Heart J. 2002, 3, 419–423. [Google Scholar]
- Gonzalez, M.H.; Acharya, D.; Lee, S.; Leacche, M.; Boeve, T.; Manandhar-Shrestha, N.; Jovinge, S.; Loyaga-Rendon, R.Y. Improved survival after heart transplantation in patients bridged with extracorporeal membrane oxygenation in the new allocation system. J. Heart Lung Transplant. 2021, 40, 149–157. [Google Scholar] [CrossRef]
- Mihaljevic, T.; Jarrett, C.M.; Gonzalez-Stawinski, G.; Smedira, N.G.; Nowicki, E.R.; Thuita, L.; Mountis, M.; Blackstone, E.H. Mechanical circulatory support after heart transplantation. Eur. J. Cardiothorac. Surg. 2012, 41, 200–206. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Non-DA n = 434 | DA n = 260 | Study Population n = 694 | p-Value |
|---|---|---|---|---|
| Female, n (%) | 90 (20.7) | 64 (24.6) | 154 (22.2) | 0.234 |
| Male, n (%) | 344 (79.3) | 196 (75.4) | 540 (77.8) | 0.234 |
| VAD, n (%) | 105 (24.2) | 70 (26.9) | 175 (25.2) | 0.423 |
| Age, median (IQR) | 52.52 (14.53) | 54.28(11.70) | 53.12 (13.56) | 0.053 |
| Previous acute myocarditis, n (%) | 56 (12.9) | 34 (13.1) | 90 (13.0) | 0.947 |
| Dilated cardiomyopathy, n (%) | 325 (74.9) | 195 (75.0) | 520 (74.9) | 0.973 |
| Non-dilated cardiomyopathy, n (%) | 44 (10.1) | 23 (8.8) | 67 (9.7) | 0.577 |
| Ischaemic heart disease, n (%) | 276 (63.6) | 200 (76.9) | 476 (68.6) | <0.001 |
| Hypertension, n (%) | 356 (82.0) | 237 (91.2) | 593 (85.4) | <0.001 |
| Diabetes, n (%) | 144 (33.2) | 115 (44.2) | 259 (37.3) | 0.004 |
| Dyslipidaemia, n (%) | 290 (66.8) | 207 (79.6) | 497 (71.6) | <0.001 |
| Obesity, n (%) | 127 (29.3) | 86 (33.1) | 213 (30.7) | 0.292 |
| Smoking, n (%) | 95 (21.9) | 88 (33.8) | 183 (26.4) | <0.001 |
| Atrial flutter/fibrillation, n (%) | 297 (68.4) | 177 (68.1) | 474 (68.3) | 0.922 |
| PAD, n (%) | 30 (6.9) | 23 (8.8) | 53 (7.6) | 0.353 |
| CVD, n (%) | 40 (9.2) | 26 (10.0) | 66 (9.5) | 0.733 |
| Chronic kidney disease, n (%) | 288 (66.4) | 200 (76.9) | 488 (70.3) | 0.003 |
| Cancer, n (%) | 44 (10.1) | 24 (9.2) | 68 (9.8) | 0.697 |
| No previous listing, n (%) | 187 (43.1) | 82 (31.5) | 269 (38.8) | 0.003 |
| Previous MI, n (%) | 129 (29.7) | 108 (41.5) | 237 (34.1) | 0.001 |
| Previous PCI, n (%) | 54 (12.4) | 51 (19.6) | 105 (15.1) | 0.011 |
| Previous stroke, n (%) | 54 (12.4) | 55 (21.1) | 109 (15.7) | 0.002 |
| PAIs, n (%) | 51 (11.8) | 34 (13.1) | 85 (12.2) | 0.606 |
| OACs, n (%) | 106 (24.4) | 65 (25.0) | 171 (24.6) | 0.865 |
| PAIs in combination with OACs, n (%) | 44 (10.1) | 26 (10.0) | 70 (10.1) | 0.953 |
| ACE-Is/AT1-antagonists, n (%) | 204 (47.0) | 126 (48.5) | 330 (47.6) | 0.710 |
| Statins, n (%) | 109 (25.1) | 67 (25.8) | 176 (25.4) | 0.848 |
| Betablockers, n (%) | 252 (58.1) | 153 (58.8) | 405 (58.4) | 0.840 |
| Characteristics | Non-DA n = 434 | DA n = 260 | Overall Population n = 694 | p-Value |
|---|---|---|---|---|
| ECMO, n (%) | 65 (15.0) | 34 (13.1) | 99 (14.3) | 0.488 |
| Acute renal failure, n (%) | 184 (42.4) | 107 (41.2) | 291 (41.9) | 0.748 |
| Renal replacement therapy, n (%) | 287 (66.1) | 173 (66.5) | 460 (66.3) | 0.912 |
| Death (discharge status), n (%) | 62 (14.3) | 42 (16.2) | 104 (15.0) | 0.505 |
| Ischaemic stroke, n (%) | 27 (6.2) | 37 (14.2) | 64 (9.2) | <0.001 |
| Haemorrhagic stroke, n (%) | 10 (2.3) | 14 (5.4) | 24 (3.5) | 0.032 |
| Bleeding, n (%) | 172 (39.6) | 106 (40.8) | 278 (40.1) | 0.767 |
| Ventilation, median (IQR) | 71 (279) | 66 (306) | 70 (289) | 0.933 |
| Hospitalisation, median (IQR) | 129 (130.3) | 137 (142.8) | 133 (137.0) | 0.511 |
| In-hospital CPR, n (%) | 63 (14.5) | 33 (12.7) | 96 (13.8) | 0.501 |
| Blood transfusion, n (%) | 393 (90.6) | 234 (90.0) | 627 (90.3) | 0.811 |
| Septicaemia, n (%) | 65 (15.0) | 54 (20.8) | 119 (17.1) | 0.050 |
| Allograft rejection, n (%) | 88 (20.3) | 58 (22.3) | 146 (21.0) | 0.525 |
| New depression, n (%) | 26 (6.0) | N/A | 26 (3.7) | N/A |
| Depression relapse, n (%) | N/A | 59 (22.7) | 59 (8.5) | N/A |
| New anxiety, n (%) | <10 | N/A | N/A | N/A |
| Anxiety relapse, n (%) | N/A | 29 (11.2) | 29 (4.2) | N/A |
| PAIs | 36 (10.0) | 25 (11.9) | 61 (10.7) | 0.478 |
| OACs, n (%) | <10 | <10 | N/A | 0.740 |
| PAIs in combination with OACs, n (%) | <10 | <10 | N/A | 0.190 |
| ACE-Is/AT-blockers, n (%) | 41 (11.4) | 27 (12.9) | 68 (11.9) | 0.602 |
| Statins, n (%) | 59 (16.4) | 46 (21.9) | 105 (18.4) | 0.101 |
| Betablockers, n (%) | 14 (3.9) | 15 (7.1) | 29 (5.1) | 0.088 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alyaydin, E.; Sindermann, J.R.; Köppe, J.; Gerss, J.; Dröge, P.; Ruhnke, T.; Günster, C.; Reinecke, H.; Feld, J. Depression and Anxiety in Heart Transplant Recipients: Prevalence and Impact on Post-Transplant Outcomes. J. Pers. Med. 2023, 13, 844. https://doi.org/10.3390/jpm13050844
Alyaydin E, Sindermann JR, Köppe J, Gerss J, Dröge P, Ruhnke T, Günster C, Reinecke H, Feld J. Depression and Anxiety in Heart Transplant Recipients: Prevalence and Impact on Post-Transplant Outcomes. Journal of Personalized Medicine. 2023; 13(5):844. https://doi.org/10.3390/jpm13050844
Chicago/Turabian StyleAlyaydin, Emyal, Juergen Reinhard Sindermann, Jeanette Köppe, Joachim Gerss, Patrik Dröge, Thomas Ruhnke, Christian Günster, Holger Reinecke, and Jannik Feld. 2023. "Depression and Anxiety in Heart Transplant Recipients: Prevalence and Impact on Post-Transplant Outcomes" Journal of Personalized Medicine 13, no. 5: 844. https://doi.org/10.3390/jpm13050844