
Comparison of Laser-Sintered and Milled Patient-Specific Reconstruction Plates for Complications and Outcomes in Mandibular Defects—Comparative Analysis of a Single-Center Cohort
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection for the Study
2.2. Statistical Analysis
3. Results
3.1. Baseline Demographic Features Comparison for System Groups
3.2. Baseline Demographic Features Comparison for Complications/No-Complications Groups
3.3. Baseline Demographic Features Comparison for Revisions/No-Revisions Groups
3.4. Model for the Risk of Complication
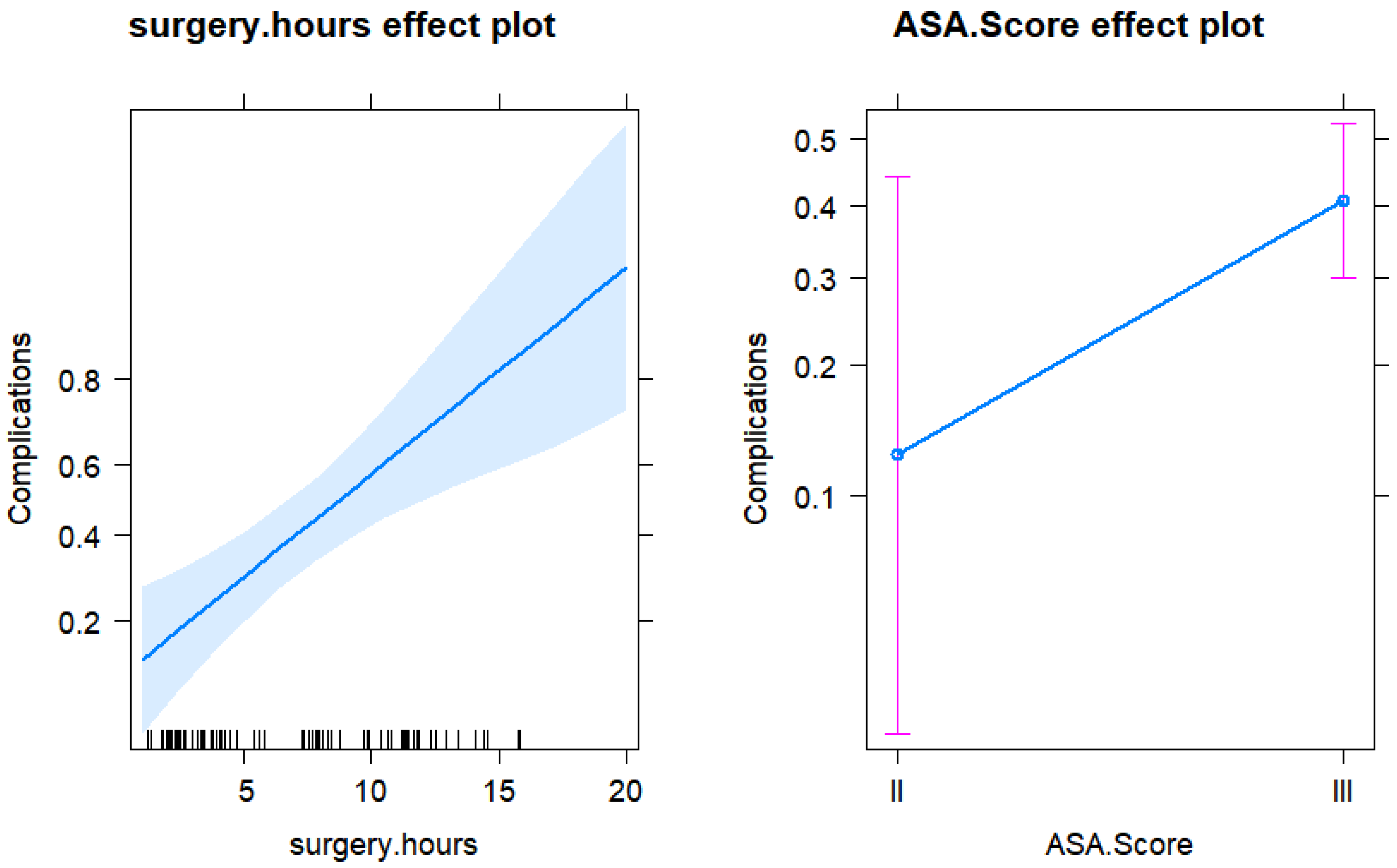
Risk Factors for Complications
3.5. Model for the Duration of the Inpatient Stay
Predictors for the Length of Stay
3.6. Model for Risk of Revision
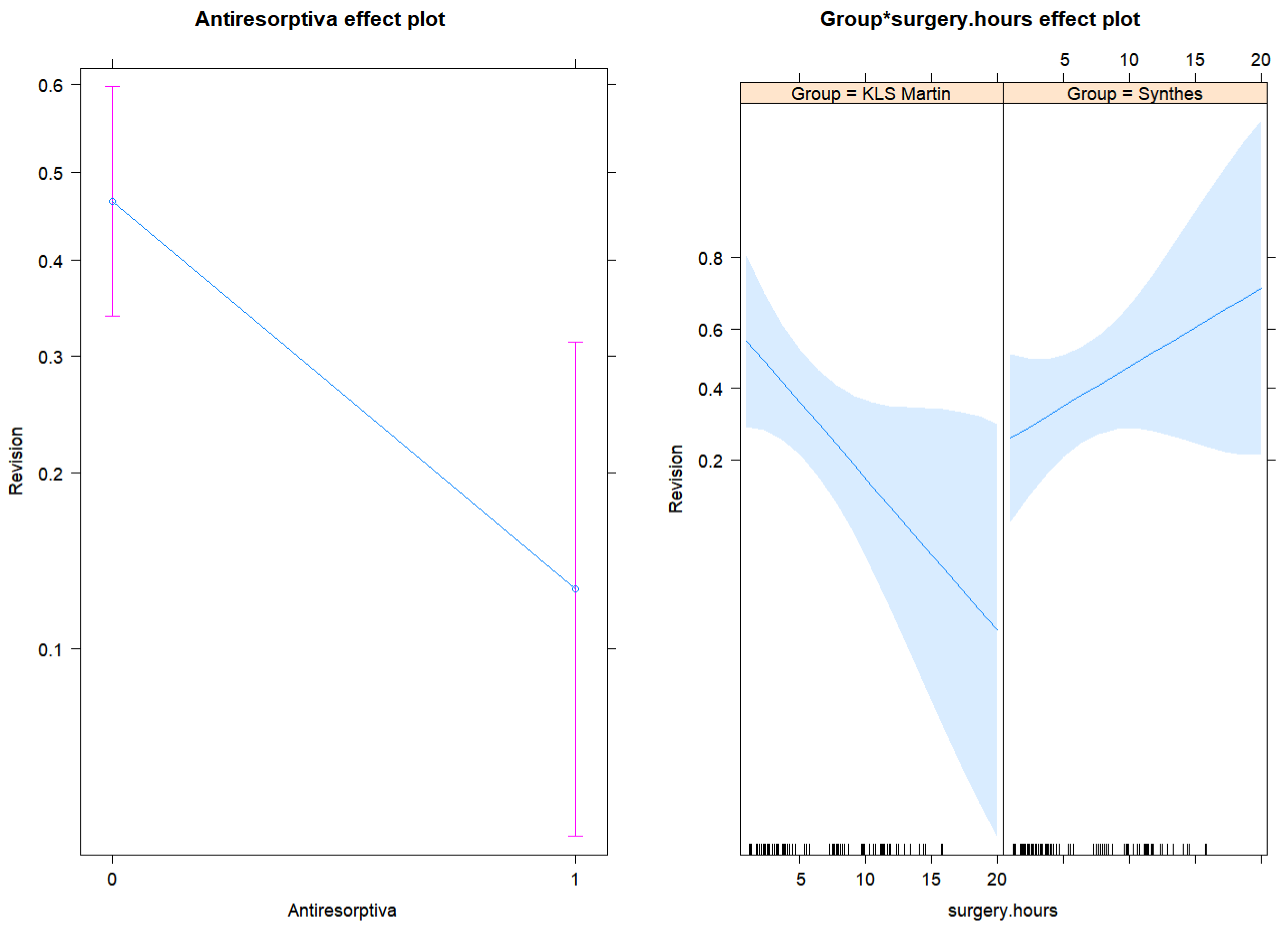
Risk Factors for the Revision
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zeller, A.N.; Neuhaus, M.T.; Weissbach, L.V.M.; Rana, M.; Dhawan, A.; Eckstein, F.M.; Gellrich, N.C.; Zimmerer, R.M. Patient-Specific Mandibular Reconstruction Plates Increase Accuracy and Long-Term Stability in Immediate Alloplastic Reconstruction of Segmental Mandibular Defects. J. Maxillofac. Oral Surg. 2020, 19, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, J.J.; Zagalo, C.M.; Oliveira, M.L.; Correia, A.M.; Reis, A.R. Mandible reconstruction: History, state of the art and persistent problems. Prosthet. Orthot. Int. 2015, 39, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Rana, M.; Chin, S.J.; Muecke, T.; Kesting, M.; Groebe, A.; Riecke, B.; Heiland, M.; Gellrich, N.C. Increasing the accuracy of mandibular reconstruction with free fibula flaps using functionalized selective laser-melted patient-specific implants: A retrospective multicenter analysis. J. Craniomaxillofac. Surg. 2017, 45, 1212–1219. [Google Scholar] [CrossRef] [PubMed]
- Wilde, F.; Cornelius, C.P.; Schramm, A. Computer-Assisted Mandibular Reconstruction using a Patient-Specific Reconstruction Plate Fabricated with Computer-Aided Design and Manufacturing Techniques. Craniomaxillofac. Trauma Reconstr. 2014, 7, 158–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasper, R.; Winter, K.; Pietzka, S.; Schramm, A.; Wilde, F. Biomechanical In Vitro Study on the Stability of Patient-Specific CAD/CAM Mandibular Reconstruction Plates: A Comparison between Selective Laser Melted, Milled, and Hand-Bent Plates. Craniomaxillofac. Trauma Reconstr. 2021, 14, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, M.; Monteiro, F.J.; Ferraz, M.P. Infection of orthopedic implants with emphasis on bacterial adhesion process and techniques used in studying bacterial-material interactions. Biomatter 2012, 2, 176–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, K.; Guo, Y.; Zhao, S.; Wang, L.; Wu, J.; Tan, J.; Yang, Y.; Wu, W.; Jiang, W.; Hao, Y. Partially Melted Ti6Al4V Particles Increase Bacterial Adhesion and Inhibit Osteogenic Activity on 3D-printed Implants: An In Vitro Study. Clin. Orthop. Relat. Res. 2019, 477, 2772–2782. [Google Scholar] [CrossRef] [PubMed]
- Arciola, C.R.; Campoccia, D.; Montanaro, L. Implant infections: Adhesion, biofilm formation and immune evasion. Nat. Rev. Microbiol. 2018, 16, 397–409. [Google Scholar] [CrossRef] [PubMed]
- Wilde, F.; Hanken, H.; Probst, F.; Schramm, A.; Heiland, M.; Cornelius, C.P. Multicenter study on the use of patient-specific CAD/CAM reconstruction plates for mandibular reconstruction. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 2035–2051. [Google Scholar] [CrossRef] [PubMed]
- Aramanadka, C.; Kamath, A.T.; Srikanth, G.; Pai, D.; Singla, N.; Daundiyal, S.; Desai, A. Hardware Removal in Maxillofacial Trauma: A Retrospective Study. Sci. World J. 2021, 2021, 9947350. [Google Scholar] [CrossRef] [PubMed]
- Wood, C.B.; Shinn, J.R.; Amin, S.N.; Rohde, S.L.; Sinard, R.J. Risk of plate removal in free flap reconstruction of the mandible. Oral Oncol. 2018, 83, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Kreutzer, K.; Steffen, C.; Nahles, S.; Koerdt, S.; Heiland, M.; Rendenbach, C.; Beck-Broichsitter, B. Removal of patient-specific reconstruction plates after mandible reconstruction with a fibula free flap: Is the plate the problem? Int. J. Oral Maxillofac. Surg. 2022, 51, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Knitschke, M.; Sonnabend, S.; Roller, F.C.; Pons-Kühnemann, J.; Schmermund, D.; Attia, S.; Streckbein, P.; Howaldt, H.P.; Böttger, S. Osseous Union after Mandible Reconstruction with Fibula Free Flap Using Manually Bent Plates vs. Patient-Specific Implants: A Retrospective Analysis of 89 Patients. Curr. Oncol. 2022, 29, 3375–3392. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Depuy Synthes® (n = 54) | KLS Martin® (n = 44) | p-Value | |
|---|---|---|---|
| Age | |||
| (Mean, SD) | 59.48, 13.09 | 59.54, 10.20 | 0.597 |
| Sex | |||
| Males | 30 (44%) | 26 (59%) | |
| Females | 24 (56%) | 18 (41%) | 0.838 |
| ASA score | |||
| II | 7 (13%) | 4 (9%) | |
| III | 47 (87%) | 40 (91%) | 0.749 |
| Diabetes (YES) | 5 (7%) | 11 (25%) | 0.053 |
| Smoking | |||
| Current | 25 (53%) | 24 (67%) | |
| Ex | 5 (10%) | 0 | |
| Never | 17 (37%) | 12 (33%) | 0.211 |
| Alcohol | |||
| Daily | 15 (34%) | 15 (40%) | |
| Never | 18 (41%) | 17 (46%) | |
| Occasionally | 11 (25%) | 5 (14%) | 0.475 |
| Antiresorptive medication | |||
| (YES) | 21 (39%) | 8 (18%) | 0.028 |
| Immunomodulating medication | |||
| (YES) | 11 (21%) | 1 (2%) | 0.006 |
| Indication for the surgery | |||
| 1 = Tumor | 20 (37%) | 15 (34%) | |
| 2 = Osteonecrosis | 7 (13%) | 11 (25%) | |
| 3 = AR/BPONJ | 21 (39%) | 8 (18%) | |
| 4 = Other indication | 6 (11%) | 10 (23%) | 0.059 |
| Complications | |||
| (YES) | 20 (37%) | 18 (41%) | 0.835 |
| Revisions | |||
| (YES) | 20 (37%) | 16 (36%) | 1 |
| Radiation | |||
| (YES) | 29 (54%) | 22 (50%) | 0.685 |
| Chemo | |||
| (YES) | 24 (44%) | 16 (36%) | 0.534 |
| Length of stay | |||
| Median, Q1, Q3 | 9, 7, 18.5 | 13, 7, 19 | 0.053 |
| Indication for Revision | |||
| 0 = No revision | 34 (63%) | 28 (64%) | |
| 1 = Fistula/abscess/infection | 16 (29%) | 11 (25%) | |
| 2 = Fracture | 2 (2%) | 2 (4.5%) | |
| 3 = Relapse | 2 (2%) | 2 (4.5%) | |
| 4 = Various | 2 (4%) | 1 (2%) | 0.839 |
| Complications (n = 38) | No-Complications (n = 60) | p-Value | |
|---|---|---|---|
| Age | |||
| (Mean, SD) | 65.6, 9.79 | 66.7, 9.94 | 0.594 |
| Sex | |||
| Males | 24 (63%) | 32 (53%) | |
| Females | 14 (37%) | 28 (47%) | 0.404 |
| ASA score | |||
| II | 2 (5%) | 9 (15%) | |
| III | 36 (95%) | 51 (85%) | 0.194 |
| Diabetes (YES) | 7 (18%) | 9 (15%) | 0.740 |
| Smoking | |||
| Current | 19 (59%) | 30 (59%) | |
| Ex | 2 (6%) | 3 (6%) | |
| Never | 11 (34%) | 18 (35%) | 1 |
| Alcohol | |||
| Daily | 14 (45%) | 16 (32%) | |
| Never | 11 (35%) | 24 (48%) | |
| Occasionally | 6 (20%) | 10 (20%) | 0.442 |
| Antiresorptive medication | |||
| (YES) | 6 (16%) | 23 (39%) | 0.007 |
| Immunomodulating medication | |||
| (YES) | 2 (5%) | 10 (17%) | 0.118 |
| Indication for the surgery | |||
| 1 = Tumor | 21 (55%) | 14 (23%) | |
| 2 = Osteonecrosis | 9 (24%) | 9 (15%) | |
| 3 = AR/BPONJ | 5 (13%) | 14 (40%) | |
| 4 = Other indication | 3 (8%) | 13 (22%) | 0.001 |
| Revisions | |||
| (YES) | 12 (32%) | 24 (40%) | 0.519 |
| Radiation | |||
| (YES) | 18 (47%) | 33 (55%) | 0.535 |
| Chemo | |||
| (YES) | 13 (34%) | 27 (45%) | 0.399 |
| Length of stay | |||
| Median, Q1, Q3 | 19, 13, 22 | 7, 6, 11.75 | 0.173 |
| Indication for Revision | |||
| 0 = No revision | 26 (68%) | 26 (60%) | |
| 1 = Fistula/abscess/infection | 9 (24%) | 18 (30%) | |
| 2 = Fracture | 0 (0%) | 3 (5%) | |
| 3 = Relapse | 2 (5%) | 1 (2%) | |
| 4 = Various | 1 (3%) | 2 (3%) | 0.544 |
| Revisions (n = 36) | No-Revisions (n = 62) | p-Value | |
|---|---|---|---|
| Age | |||
| (Mean, SD) | 66.33, 9.38 | 66.24, 10.19 | 0.964 |
| Sex | |||
| Males | 21 (42%) | 35 (56%) | |
| Females | 15 (58%) | 27 (44%) | 0.835 |
| ASA score | |||
| II | 5 (14%) | 6 (10%) | |
| III | 31 (86%) | 56 (90%) | 0.745 |
| Diabetes (YES) | 6 (17%) | 10 (16%) | 1 |
| Smoking | |||
| Current | 17 (65%) | 32 (56%) | |
| Ex | 1 (4%) | 4 (7%) | |
| Never | 8 (31%) | 21 (37%) | 0.740 |
| Alcohol | |||
| Daily | 14 (50%) | 16 (30%) | |
| Never | 11 (39%) | 24 (45%) | |
| Occasionally | 3 (11%) | 13 (25%) | 0.167 |
| Antiresorptive medication | |||
| (YES) | 4 (11%) | 25 (41%) | 0.002 |
| Immunomodulating medication | |||
| (YES) | 4 (11%) | 8 (13%) | 1 |
| Indication for the surgery | |||
| 1 = Tumor | 17 (47%) | 18 (29%) | |
| 2 = Osteonecrosis | 9 (25%) | 9 (15%) | |
| 3 = AR/BPONJ | 25 (11%) | 25 (40%) | |
| 4 = Other indication | 10 (17%) | 10 (16%) | 0.013 |
| Complications | |||
| (YES) | 12 (33%) | 26 (42%) | 0.519 |
| Radiation | |||
| (YES) | 17 (47%) | 34 (55%) | 0.532 |
| Chemo | |||
| (YES) | 12 (33%) | 28 (45%) | 0.399 |
| Length of stay | |||
| Median, Q1, Q3 | 13, 9, 19 | 9, 6, 17.25 | 0.026 |
| (A) Initial model for risk of complications | ||
| Complications | ||
| Predictors | Odds Ratios | p |
| (Intercept) | 0.01 (0.00–22.83) | 0.254 |
| Group | 24.78 (0.00–523425.07) | 0.514 |
| Surgery hours | 1.55 (1.10–2.55) | 0.033 |
| Age | 0.96 (0.87–1.07) | 0.478 |
| Gender [M] | 1.35 (0.12–17.53) | 0.805 |
| ASA score [III] | 8.61 (1.13–111.70) | 0.055 |
| Diabetes | 0.59 (0.18–1.53) | 0.308 |
| Alcohol [never] | 4.92 (0.40–82.59) | 0.228 |
| Alcohol [occasionally] | 6.77 (0.24–309.39) | 0.278 |
| Smoking [ex] | 2.10 (0.14–36.00) | 0.586 |
| Smoking [never] | 4.42 (0.44–71.14) | 0.232 |
| Med immun | 0.33 (0.04–2.13) | 0.267 |
| Antiresorptiva [1] | 0.40 (0.01–8.88) | 0.578 |
| Group-surgery hours | 0.73 (0.42–1.13) | 0.196 |
| Group-age | 1.02 (0.90–1.17) | 0.719 |
| Group-gender [M] | 0.49 (0.02–12.36) | 0.666 |
| Group-alcohol [never] | 0.10 (0.00–2.85) | 0.190 |
| Group-alcohol [occasionally] | 0.06 (0.00–5.01) | 0.228 |
| Group-smoking [never] | 0.16 (0.01–2.89) | 0.229 |
| Group-Antiresorptives [1] | 1.70 (0.05–102.76) | 0.776 |
| Observations | 77 | |
| R2 Tjur | 0.306 | |
| (B) Final model for risk of complications | ||
| Complications | ||
| Predictors | Odds Ratios | p |
| (Intercept) | 0.03 (0.00–0.19) | 0.001 |
| Surgery hours | 1.27 (1.13–1.44) | <0.001 |
| ASA score [III] | 4.79 (0.96–38.23) | 0.084 |
| Observations | 98 | |
| R2 Tjur | 0.190 | |
| (A) Initial model for the length of stay | ||
| Length of Stay | ||
|---|---|---|
| Predictors | Estimates | p |
| (Intercept) | 22.49 (3.92–137.19) | <0.001 |
| Group | 0.20 (0.02–2.00) | 0.159 |
| Surgery hours | 1.05 (0.98–1.13) | 0.138 |
| Age | 0.98 (0.96–1.01) | 0.201 |
| Gender [M] | 0.97 (0.59–1.56) | 0.890 |
| ASA score [III] | 1.13 (0.68–1.82) | 0.624 |
| Diabetes | 0.92 (0.75–1.15) | 0.447 |
| Alcohol [never] | 1.01 (0.59–1.75) | 0.967 |
| Alcohol [occasionally] | 1.25 (0.62–2.66) | 0.537 |
| Smoking [ex] | 0.68 (0.39–1.25) | 0.201 |
| Smoking [never] | 0.99 (0.62–1.62) | 0.980 |
| Med immun | 0.74 (0.48–1.13) | 0.148 |
| Antiresorptiva [1] | 0.71 (0.39–1.32) | 0.263 |
| Group-surgery hours | 1.01 (0.92–1.10) | 0.914 |
| Group-age | 1.03 (1.00–1.06) | 0.040 |
| Group-gender [M] | 1.13 (0.57–2.26) | 0.727 |
| Group-alcohol [never] | 0.67 (0.32–1.38) | 0.292 |
| Group-alcohol [occasionally] | 0.74 (0.27–1.99) | 0.550 |
| Group-smoking [never] | 0.71 (0.37–1.32) | 0.265 |
| Group-Antiresorptiva [1] | 1.02 (0.47–2.18) | 0.954 |
| Observations | 73 | |
| R2 Nagelkerke | 0.539 | |
| (B) Final model for the length of stay | ||
| Length of Stay | ||
| Predictors | Estimates | p |
| (Intercept) | 6.93 (5.51–8.79) | <0.001 |
| Surgery hours | 1.10 (1.06–1.13) | <0.001 |
| Observations | 90 | |
| R2 Nagelkerke | 0.374 | |
| (A) Initial model for risk of revision | ||
| Revision | ||
| Predictors | Odds Ratios | p |
| (Intercept) | 62.58 (0.06–161236.37) | 0.259 |
| Group | 0.00 (0.00–12.58) | 0.161 |
| Surgery hours | 0.76 (0.55–1.00) | 0.071 |
| Age | 0.96 (0.86–1.06) | 0.419 |
| Gender [M] | 0.83 (0.10–6.35) | 0.852 |
| ASA score [III] | 1.52 (0.21–13.08) | 0.684 |
| Diabetes | 0.43 (0.13–1.15) | 0.119 |
| Alcohol [never] | 0.74 (0.16–3.46) | 0.699 |
| Alcohol [occasionally] | 0.58 (0.04–6.04) | 0.664 |
| Smoking [ex] | 0.56 (0.02–11.48) | 0.704 |
| Smoking [never] | 0.88 (0.11–6.17) | 0.895 |
| Med immun | 1.20 (0.13–11.20) | 0.868 |
| Antiresorptiva [1] | 0.12 (0.00–1.63) | 0.140 |
| Group-surgery hours | 1.63 (1.11–2.52) | 0.017 |
| Group-age | 1.05 (0.91–1.21) | 0.511 |
| Group-gender [M] | 4.53 (0.27–94.21) | 0.304 |
| Group-smoking [never] | 2.20 (0.14–40.70) | 0.582 |
| Group-Antiresorptiva [1] | 1.12 (0.02–64.56) | 0.952 |
| Observations | 77 | |
| R2 Tjur | 0.284 | |
| (B) Final model for risk of revision | ||
| Revision | ||
| Predictors | Odds Ratios | p |
| (Intercept) | 2.69 (0.67–11.92) | 0.171 |
| Group | 0.19 (0.03–1.20) | 0.079 |
| Surgery hours | 0.81 (0.66–0.97) | 0.035 |
| Antiresorptiva [1] | 0.17 (0.04–0.57) | 0.007 |
| Group-surgery hours | 1.37 (1.08–1.77) | 0.011 |
| Observations | 96 | |
| R2 Tjur | 0.180 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hagmann, A.; Schappacher, R.; Pietzka, S.; Sakkas, A.; Scheurer, M.; Schramm, A.; Wilde, F.; Ebeling, M. Comparison of Laser-Sintered and Milled Patient-Specific Reconstruction Plates for Complications and Outcomes in Mandibular Defects—Comparative Analysis of a Single-Center Cohort. J. Pers. Med. 2023, 13, 648. https://doi.org/10.3390/jpm13040648
Hagmann A, Schappacher R, Pietzka S, Sakkas A, Scheurer M, Schramm A, Wilde F, Ebeling M. Comparison of Laser-Sintered and Milled Patient-Specific Reconstruction Plates for Complications and Outcomes in Mandibular Defects—Comparative Analysis of a Single-Center Cohort. Journal of Personalized Medicine. 2023; 13(4):648. https://doi.org/10.3390/jpm13040648
Chicago/Turabian StyleHagmann, Alexander, Robert Schappacher, Sebastian Pietzka, Andreas Sakkas, Mario Scheurer, Alexander Schramm, Frank Wilde, and Marcel Ebeling. 2023. "Comparison of Laser-Sintered and Milled Patient-Specific Reconstruction Plates for Complications and Outcomes in Mandibular Defects—Comparative Analysis of a Single-Center Cohort" Journal of Personalized Medicine 13, no. 4: 648. https://doi.org/10.3390/jpm13040648