
Patient Specific Implants for Orbital Reconstruction in the Treatment of Silent Sinus Syndrome: Two Case Reports

Abstract
:1. Introduction
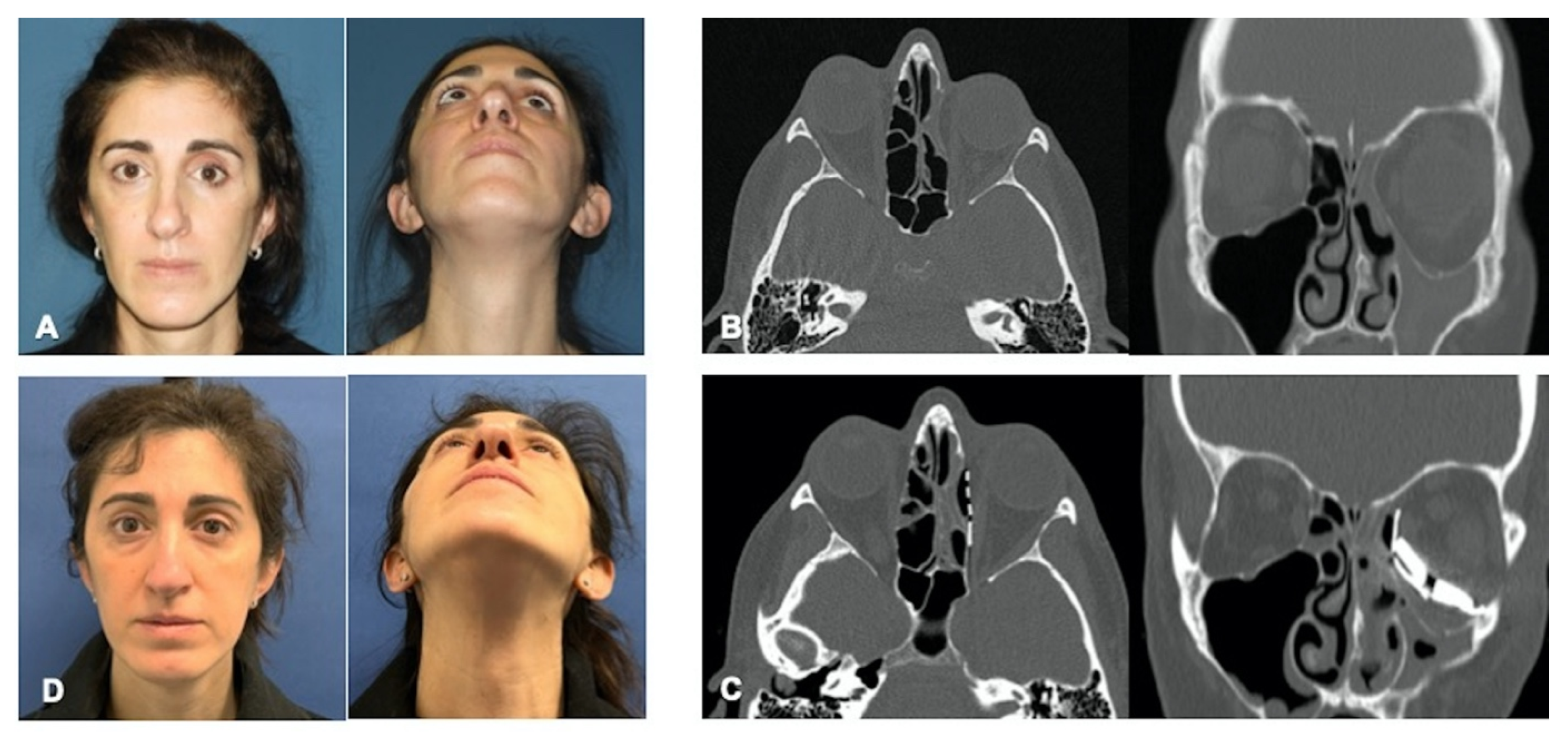
2. Case Report 1
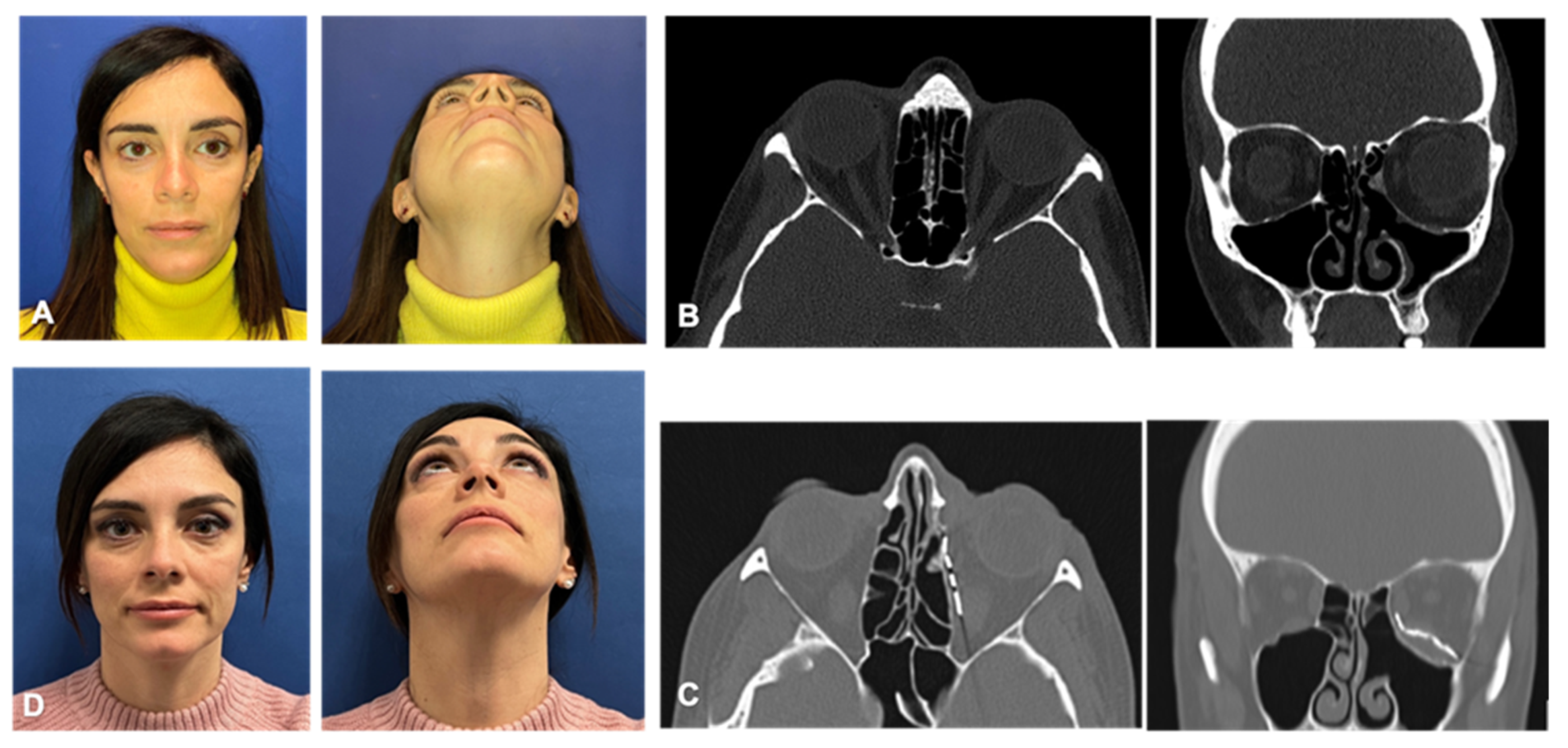
3. Case Report 2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lim, B.W.; Jung, J.H.; Kim, S.T.; Kim, D.H.; Park, J.W.; Cha, H.E.; Kang, I.G. Autologous Fat Injection for the Correction of Facial Depression Resulting From Silent Sinus Syndrome. J. Craniofacial Surg. 2019, 30, e191. [Google Scholar] [CrossRef]
- Rosso, C.; Saibene, A.M.; Felisati, G.; Pipolo, C. Silent Sinus Syndrome: Systematic Review and Proposal of Definition, Diagnosis and Management. Acta Otorhinolaryngol. Ital. 2022, 42, 305–316. [Google Scholar] [CrossRef]
- Baig, M.Z.; Weber, J.F.; Bhora, F.; Al Shetawi, A.H. Surgical Advances in the Management of the Silent Sinus Syndrome: Our Experience and Review of the Literature. J. Oral Maxillofac. Surg. 2020, 78, 2289–2295. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, W.W. Mucocele of the Maxillary Sinus Causing Enophthalmos. Eye Ear Nose Throat Mon. 1964, 43, 41–44. [Google Scholar] [PubMed]
- Kass, E.S.; Salman, S.; Montgomery, W.W. Manometric Study of Complete Ostial Occlusion in Chronic Maxillary Atelectasis. Laryngoscope 1996, 106, 1255–1258. [Google Scholar] [CrossRef]
- Bossolesi, P.; Autelitano, L.; Brusati, R.; Castelnuovo, P. The Silent Sinus Syndrome: Diagnosis and Surgical Treatment. Rhinology 2008, 46, 308–316. [Google Scholar]
- Tieghi, R.; Malagutti, N.; Valente, L.; Carnevali, G.; Clauser, L.C. Combined Endoscopic and Trans Palpebral Orbital Reconstruction for Silent Sinus Syndrome. J. Craniofacial Surg. 2017, 28, 955–958. [Google Scholar] [CrossRef]
- Bhalla, N.; Rosenstein, J.; Dym, H. Silent Sinus Syndrome: Interesting Clinical and Radiologic Findings. J. Oral Maxillofac. Surg. 2019, 77, 2040–2043. [Google Scholar] [CrossRef] [PubMed]
- Borràs Perera, M.; Palomar Asenjo, V.; Soteras Ollé, J.; Fortuny Llanses, J.C.; Palomar García, V. The silent sinus syndrome. Acta Otorrinolaringol. Esp. 2007, 58, 491–493. [Google Scholar] [CrossRef]
- Ferri, A.; Ferri, T.; Sesenna, E. Bilateral Silent Sinus Syndrome: Case Report and Surgical Solution. J. Oral Maxillofac. Surg. 2012, 70, e103–e106. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Dalmau, B.F.; Pascual, L.; Lao, X.; Maiz, J. Sinus syndrome, an uncommon cause of enophthalmos. Arch. Soc. Esp. Oftalmol. 2008, 83, 125–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, D.T.; Truong, M.T. A Child with Silent Sinus Syndrome and Spontaneous Improvement after Sinus Surgery. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 1993–1995. [Google Scholar] [CrossRef] [PubMed]
- Bonavolontà, P.; Dell’Aversana Orabona, G.; Cama, A.; Romano, A.; Abbate, V.; Salzano, G.; Boschetti, C.E.; D’Andrea, L.; Iaconetta, G.; Califano, L. Application of a Computer Navigation System in the Treatment of Silent Sinus Syndrome: Case Reports and Technical Note. J. Plast. Reconstr. Aesthet. Surg. 2020, 73, 783–808. [Google Scholar] [CrossRef] [PubMed]
- de Dorlodot, C.; Collet, S.; Rombaux, P.; Horoi, M.; Hassid, S.; Eloy, P. Chronic Maxillary Atelectasis and Silent Sinus Syndrome: Two Faces of the Same Clinical Entity. Eur. Arch. Otorhinolaryngol. 2017, 274, 3367–3373. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.D.; Graham, S.M.; Carter, K.D.; Nerad, J.A. Management of the Orbital Floor in Silent Sinus Syndrome. Am. J. Rhinol. 2003, 17, 97–100. [Google Scholar] [CrossRef]
- Numa, W.A.; Desai, U.; Gold, D.R.; Heher, K.L.; Annino, D.J. Silent Sinus Syndrome: A Case Presentation and Comprehensive Review of All 84 Reported Cases. Ann. Otol. Rhinol. Laryngol. 2005, 114, 688–694. [Google Scholar] [CrossRef]
- Sivasubramaniam, R.; Sacks, R.; Thornton, M. Silent Sinus Syndrome: Dynamic Changes in the Position of the Orbital Floor after Restoration of Normal Sinus Pressure. J. Laryngol. Otol. 2011, 125, 1239–1243. [Google Scholar] [CrossRef] [Green Version]
- Babar-Craig, H.; Kayhanian, H.; De Silva, D.J.; Rose, G.E.; Lund, V.J. Spontaneous Silent Sinus Syndrome (Imploding Antrum Syndrome): Case Series of 16 Patients. Rhinology 2011, 49, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Arnon, R.; Gluck, O.; Winter, H.; Pikkel, J.; Rubinov, A. Combined Single-Step Procedure for Correction of Silent Sinus Syndrome. Case Rep. Ophthalmol. 2019, 10, 95–100. [Google Scholar] [CrossRef]
- Sesenna, E.; Oretti, G.; Anghinoni, M.L.; Ferri, A. Simultaneous Management of the Enophthalmos and Sinus Pathology in Silent Sinus Syndrome: A Report of Three Cases. J. Cranio-Maxillofac. Surg. 2010, 38, 469–472. [Google Scholar] [CrossRef]
- Cobb, A.R.M.; Murthy, R.; Cousin, G.C.S.; El-Rasheed, A.; Toma, A.; Uddin, J.; Manisali, M. Silent Sinus Syndrome. Br. J. Oral. Maxillofac. Surg. 2012, 50, e81–e85. [Google Scholar] [CrossRef] [PubMed]
- Behbehani, R.; Vacareza, N.; Bilyk, J.R.; Rubin, P.A.D.; Pribitkin, E.A. Simultaneous Endoscopic Antrostomy and Orbital Reconstruction in Silent Sinus Syndrome. Orbit 2006, 25, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Ali, K.; Schultz, K.P.; Marx, D.P.; Hollier, L.H.; Buchanan, E.P. Secondary Repair of Posttraumatic Enophthalmos and Extraocular Movement Disorders. Facial Plast. Surg. 2017, 33, 606–612. [Google Scholar] [CrossRef]
- Al-Moraissi, E.A.; Thaller, S.R.; Ellis, E. Subciliary vs. Transconjunctival Approach for the Management of Orbital Floor and Periorbital Fractures: A Systematic Review and Meta-Analysis. J. Cranio-Maxillofac. Surg. 2017, 45, 1647–1654. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.D.; Schorn, L.; Strong, E.B.; Grant, M.; Schramm, A.; Hufendiek, K.; Gellrich, N.-C.; Rana, M. Computer-Assisted Secondary Orbital Reconstruction. Craniomaxillofac. Trauma. Reconstr. 2021, 14, 29–35. [Google Scholar] [CrossRef]
- Spalthoff, S.; Dittmann, J.; Zimmerer, R.; Jehn, P.; Tavassol, F.; Gellrich, N.-C. Intraorbital Volume Augmentation with Patient-Specific Titanium Spacers. J. Stomatol. Oral. Maxillofac. Surg. 2020, 121, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Gerbino, G.; Zavattero, E.; Viterbo, S.; Ramieri, G. Treatment of Orbital Medial Wall Fractures with Titanium Mesh Plates Using Retrocaruncular Approach: Outcomes with Different Techniques. Craniomaxillofac. Trauma. Reconstr. 2015, 8, 326–333. [Google Scholar] [CrossRef] [Green Version]
- Kempster, R.; Beigi, B.; Galloway, G.D. Use of Enophthalmic Implants in the Repair of Orbital Floor Fractures. Orbit 2005, 24, 219–225. [Google Scholar] [CrossRef]
- Habib, L.A.; Yoon, M.K. Patient Specific Implants in Orbital Reconstruction: A Pilot Study. Am. J. Ophthalmol. Case Rep. 2021, 24, 101222. [Google Scholar] [CrossRef]
- Canzi, G.; Morganti, V.; Novelli, G.; Bozzetti, A.; Sozzi, D. Posttraumatic Delayed Enophthalmos: Analogies with Silent Sinus Syndrome? Case Report and Literature Review. Craniomaxillofac. Trauma. Reconstr. 2015, 8, 251–256. [Google Scholar] [CrossRef] [Green Version]
- Vahdani, K.; Rose, G.E. Bilateral Silent Sinus (Imploding Antrum) Syndrome. Ophthalmic. Plast. Reconstr. Surg. 2019, 35, e67. [Google Scholar] [CrossRef]
- Février, E.; Vandersteen, C.; Castillo, L.; Savoldelli, C. Silent Sinus Syndrome: A Traumatic Case. J. Stomatol. Oral. Maxillofac. Surg. 2017, 118, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Copperman, T.S.; Idowu, O.O.; Jalaj, S.; Winn, B.J.; Pham, C.; Setabutr, P.; Kersten, R.C.; Vagefi, M.R. Patient-Specific Implants in Oculofacial Plastic Surgery. Ophthalmic. Plast. Reconstr. Surg. 2021, 37, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Scolozzi, P.; Martinez, A.; Jaques, B. Complex Orbito-Fronto-Temporal Reconstruction Using Computer-Designed PEEK Implant. J. Craniofac. Surg. 2007, 18, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Eufinger, H.; Wehmöller, M.; Machtens, E.; Heuser, L.; Harders, A.; Kruse, D. Reconstruction of Craniofacial Bone Defects with Individual Alloplastic Implants Based on CAD/CAM-Manipulated CT-Data. J. Craniomaxillofac. Surg. 1995, 23, 175–181. [Google Scholar] [CrossRef]
- Kärkkäinen, M.; Wilkman, T.; Mesimäki, K.; Snäll, J. Primary Reconstruction of Orbital Fractures Using Patient-Specific Titanium Milled Implants: The Helsinki Protocol. Br. J. Oral. Maxillofac. Surg. 2018, 56, 791–796. [Google Scholar] [CrossRef] [Green Version]
- Ono, I.; Tateshita, T.; Satou, M.; Sasaki, T.; Matsumoto, M.; Kodama, N. Treatment of Large Complex Cranial Bone Defects by Using Hydroxyapatite Ceramic Implants. Plast. Reconstr. Surg. 1999, 104, 339–349. [Google Scholar] [CrossRef]
- Cohen, L.M.; Habib, L.A.; Yoon, M.K. Post-Traumatic Enophthalmos Secondary to Orbital Fat Atrophy: A Volumetric Analysis. Orbit 2020, 39, 319–324. [Google Scholar] [CrossRef]
- Pedemonte, C.; Sáez, F.; Vargas, I.; González, L.E.; Canales, M.; Salazar, K. Can Customized Implants Correct Enophthalmos and Delayed Diplopia in Post-Traumatic Orbital Deformities? A Volumetric Analysis. Int. J. Oral. Maxillofac. Surg. 2016, 45, 1086–1094. [Google Scholar] [CrossRef]
- Manson, P.N.; Clifford, C.M.; Su, C.T.; Iliff, N.T.; Morgan, R. Mechanisms of Global Support and Posttraumatic Enophthalmos: I. The Anatomy of the Ligament Sling and Its Relation to Intramuscular Cone Orbital Fat. Plast. Reconstr. Surg. 1986, 77, 193–202. [Google Scholar] [CrossRef]
- Andrades, P.; Hernandez, D.; Falguera, M.I.; Millan, J.M.; Heredero, S.; Gutierrez, R.; Sánchez-Aniceto, G. Degrees of Tolerance in Post-Traumatic Orbital Volume Correction: The Role of Prefabricated Mesh. J. Oral. Maxillofac. Surg. 2009, 67, 2404–2411. [Google Scholar] [CrossRef] [PubMed]
- Zimmerer, R.M.; Gellrich, N.-C.; von Bülow, S.; Strong, E.B.; Ellis, E.; Wagner, M.E.H.; Sanchez Aniceto, G.; Schramm, A.; Grant, M.P.; Thiam Chye, L.; et al. Is There More to the Clinical Outcome in Posttraumatic Reconstruction of the Inferior and Medial Orbital Walls than Accuracy of Implant Placement and Implant Surface Contouring? A Prospective Multicenter Study to Identify Predictors of Clinical Outcome. J. Craniomaxillofac. Surg. 2018, 46, 578–587. [Google Scholar] [CrossRef] [PubMed]
- Kashkouli, M.B.; Pakdel, F.; Sasani, L.; Hodjat, P.; Kaghazkanani, R.; Heirati, A. High-Density Porous Polyethylene Wedge Implant in Correction of Enophthalmos and Hypoglobus in Seeing Eyes. Orbit 2011, 30, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Zavattero, E.; Ramieri, G.; Roccia, F.; Gerbino, G. Comparison of the Outcomes of Complex Orbital Fracture Repair with and without a Surgical Navigation System: A Prospective Cohort Study with Historical Controls. Plast. Reconstr. Surg. 2017, 139, 957–965. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Age | Sex | Diagnosis | Presentation | Surgical Timing | Implant Location | Implant Material | Titanium Spacers | Follow Up |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 43 | F | Left silent sinus syndrome | Hypoglobus, enophthalmos, diplopia | Concomitant surgery | Medial wall and orbital floor | Titanium | Yes, 2 | 18 months |
| 2 | 43 | F | Left silent sinus syndrome | Hypoglobus, enophthalmos, diplopia | Two-stage approach | Medial wall and orbital floor | Titanium | No | 12 months |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raveggi, E.; Sobrero, F.; Gerbino, G. Patient Specific Implants for Orbital Reconstruction in the Treatment of Silent Sinus Syndrome: Two Case Reports. J. Pers. Med. 2023, 13, 578. https://doi.org/10.3390/jpm13040578
Raveggi E, Sobrero F, Gerbino G. Patient Specific Implants for Orbital Reconstruction in the Treatment of Silent Sinus Syndrome: Two Case Reports. Journal of Personalized Medicine. 2023; 13(4):578. https://doi.org/10.3390/jpm13040578
Chicago/Turabian StyleRaveggi, Elisa, Federica Sobrero, and Giovanni Gerbino. 2023. "Patient Specific Implants for Orbital Reconstruction in the Treatment of Silent Sinus Syndrome: Two Case Reports" Journal of Personalized Medicine 13, no. 4: 578. https://doi.org/10.3390/jpm13040578