
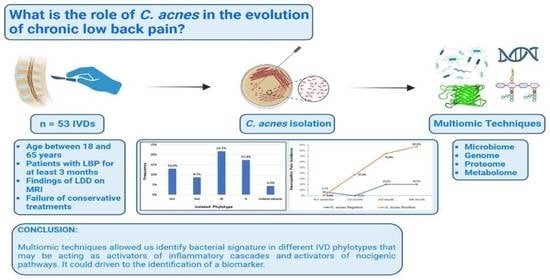
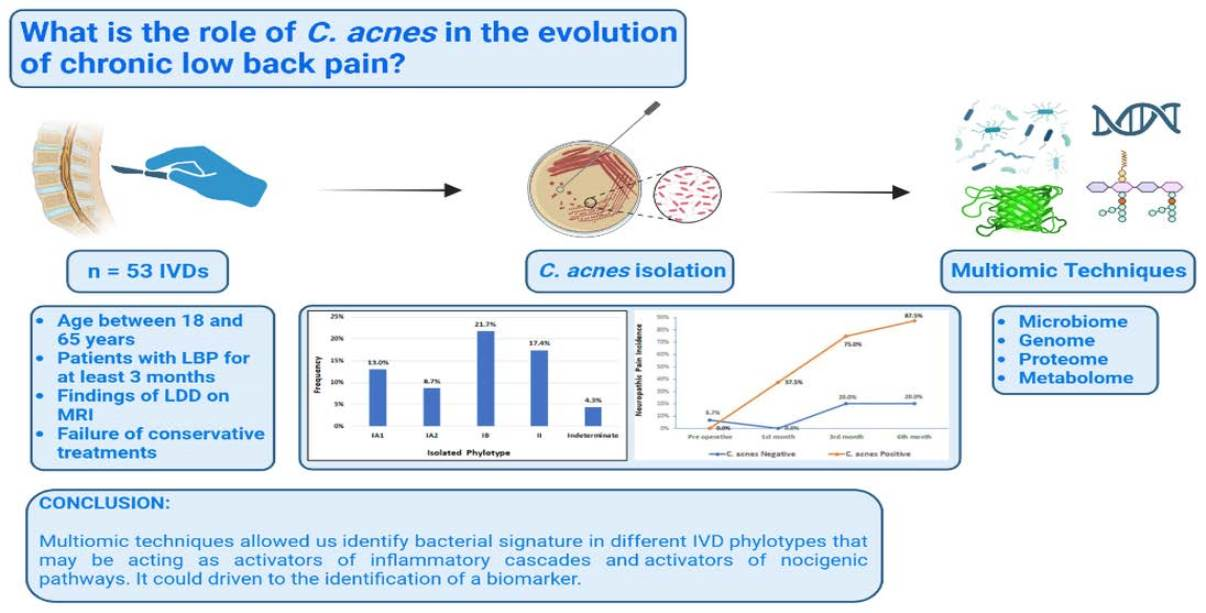
Would Cutibacterium acnes Be the Villain for the Chronicity of Low Back Pain in Degenerative Disc Disease? Preliminary Results of an Analytical Cohort
 , , and
, , and
Abstract
:
1. Introduction
2. Materials and Methods
3. Results
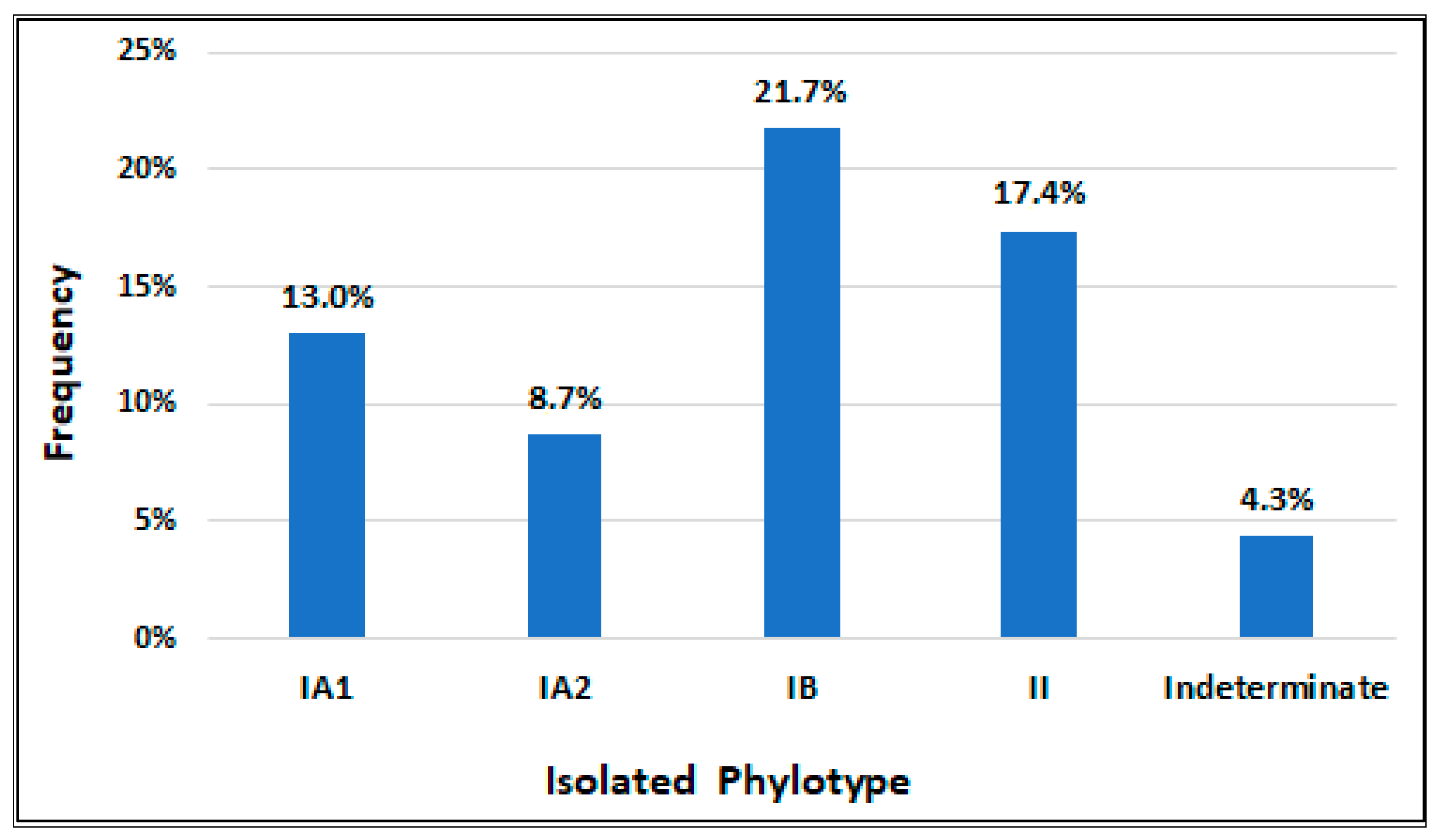
3.1. Microbiological Analyses
3.2. Preoperative Features
3.3. Operative Features
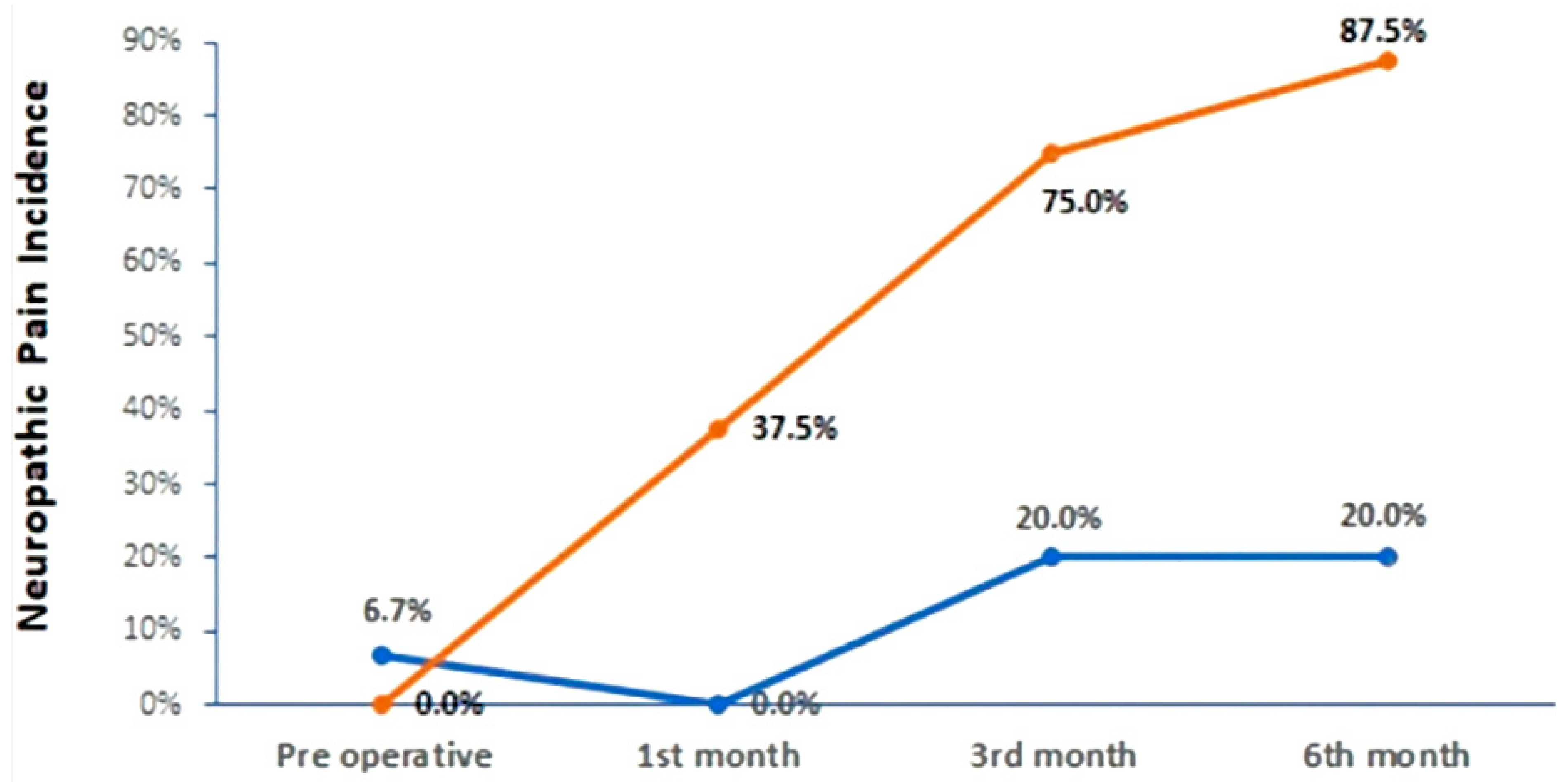
3.4. Postoperative Features
3.5. Modic Changes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Knezevic, N.N.; Candido, K.D.; Vlaeyen, J.W.S.; Van Zundert, J.; Cohen, S.P. Low back pain. Lancet 2021, 398, 78–92. [Google Scholar] [CrossRef] [PubMed]
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De David, C.N.; Deligne, L.D.M.C.; Da Silva, R.S.; Malta, D.C.; Duncan, B.B.; Passos, V.M.D.A.; Cousin, E. The burden of low back pain in Brazil: Estimates from the Global Burden of Disease 2017 Study. Popul. Health Metrics 2020, 18, 12. [Google Scholar] [CrossRef] [PubMed]
- Vasconcelos, F.H.; De Araújo, G.C. Prevalence of chronic pain in Brazil: A descriptive study. Braz. J. Pain 2018, 1. [Google Scholar] [CrossRef]
- Maher, C.; Underwood, M.; Buchbinder, R. Non-specific low back pain. Lancet 2017, 389, 736–747. [Google Scholar] [CrossRef] [Green Version]
- Patrick, N.; Emanski, E.; Knaub, M.A. Acute and Chronic Low Back Pain. Med. Clin. N. Am. 2014, 98, 777–789. [Google Scholar] [CrossRef] [PubMed]
- Vrbanić, T.S.-L. [Low back pain--from definition to diagnosis]. Reumatizam 2011, 58, 105–107. [Google Scholar] [PubMed]
- Andersson, G.B. Epidemiological features of chronic low-back pain. Lancet 1999, 354, 581–585. [Google Scholar] [CrossRef]
- Manniche, C.; Hall, G.M. Chronic low back pain, Modic changes and low-grade virulent infection: Efficacy of antibiotic treatment. Futur. Sci. OA 2021, 7, FSO703. [Google Scholar] [CrossRef]
- Bivona, L.J.; Camacho, J.E.; Usmani, F.; Nash, A.; Bruckner, J.J.; Hughes, M.; Bhandutia, A.K.; Koh, E.Y.; Banagan, K.E.; Gelb, D.E.; et al. The Prevalence of Bacterial Infection in Patients Undergoing Elective ACDF for Degenerative Cervical Spine Conditions: A Prospective Cohort Study With Contaminant Control. Glob. Spine J. 2021, 11, 13–20. [Google Scholar] [CrossRef] [Green Version]
- Tang, G.; Chen, Y.; Chen, J.; Wang, Z.; Jiang, W. Higher proportion of low-virulence anaerobic bacterial infection in young patients with intervertebral disc herniation. Exp. Ther. Med. 2019, 18, 3085–3089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manniche, C.; O’Neill, S. New insights link low-virulent disc infections to the etiology of severe disc degeneration and Modic changes. Futur. Sci. OA 2019, 5, FSO389. [Google Scholar] [CrossRef] [Green Version]
- Tang, G.; Wang, Z.; Chen, J.; Zhang, Z.; Qian, H.; Chen, Y. Latent infection of low-virulence anaerobic bacteria in degenerated lumbar intervertebral discs. BMC Musculoskelet. Disord. 2018, 19, 445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Wang, X.; Zhang, X.; Ren, H.; Huang, B.; Chen, J.; Liu, J.; Shan, Z.; Zhu, Z.; Zhao, F. Low virulence bacterial infections in cervical intervertebral discs: A prospective case series. Eur. Spine J. 2018, 27, 2496–2505. [Google Scholar] [CrossRef] [PubMed]
- Ganko, R.; Rao, P.J.; Phan, K.; Mobbs, R.J. Can Bacterial Infection by Low Virulent Organisms Be a Plausible Cause for Symptomatic Disc Degeneration? A Systematic Review. Spine 2015, 40, E587–E592. [Google Scholar] [CrossRef] [PubMed]
- Mackenzie, W.S.; Matsumoto, H.; Williams, B.A.; Corona, J.; Lee, C.; Cody, S.R.; Covington, L.; Saiman, L.; Flynn, J.M.; Skaggs, D.L.; et al. Surgical Site Infection Following Spinal Instrumentation for Scoliosis. J. Bone Jt. Surg. 2013, 95, 800–806. [Google Scholar] [CrossRef]
- Albert, H.B.; Sorensen, J.S.; Christensen, B.S.; Manniche, C. Antibiotic treatment in patients with chronic low back pain and vertebral bone edema (Modic type 1 changes): A double-blind randomized clinical controlled trial of efficacy. Eur. Spine J. 2013, 22, 697–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senker, W.; Aspalter, S.; Radl, C.; Pichler, J.; Doppler, S.; Weis, S.; Webersinke, C.; Wagner, H.; Hermann, P.; Aichholzer, M.; et al. Frequency and characteristics of bacterial and viral low-grade infections of the intervertebral discs: A prospective, observational study. J. Orthop. Traumatol. 2022, 23, 15. [Google Scholar] [CrossRef]
- Capoor, M.N.; Ruzicka, F.; Machackova, T.; Jancalek, R.; Smrcka, M.; Schmitz, J.E.; Hermanova, M.; Sana, J.; Michu, E.; Baird, J.C.; et al. Prevalence of Propionibacterium acnes in Intervertebral Discs of Patients Undergoing Lumbar Microdiscectomy: A Prospective Cross-Sectional Study. PLoS ONE 2016, 11, e0161676. [Google Scholar] [CrossRef] [Green Version]
- Iyer, S.; Louie, P.K.; Nolte, M.T.; Phillips, F.M. The Relationship Between Low-Grade Infection and Degenerative Disk Disease. J. Am. Acad. Orthop. Surg. 2019, 27, 509–518. [Google Scholar] [CrossRef]
- Georgy, M.; Vaida, F.; Stern, M.; Murphy, K. Association between Type 1 Modic Changes and Propionibacterium Acnes Infection in the Cervical Spine: An Observational Study. Am. J. Neuroradiol. 2018, 39, 1764–1767. [Google Scholar] [CrossRef] [Green Version]
- Schroeder, G.D.; Markova, D.Z.; Koerner, J.D.; Rihn, J.A.; Hilibrand, A.S.; Vaccaro, A.R.; Anderson, D.G.; Kepler, C.K. Are Modic changes associated with intervertebral disc cytokine profiles? Spine J. 2017, 17, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Mirzaaghazadeh, J.; Salehpour, F.; Ziaeii, E.; Javanshir, N.; Samadi, A.; Sadeghi, J.; Mirzaei, F.; Alavi, S.A.N. Modic changes in the adjacent vertebrae due to disc material infection with Propionibacterium acnes in patients with lumbar disc herniation. Eur. Spine J. 2017, 26, 3129–3134. [Google Scholar] [CrossRef]
- Ohtori, S.; Koshi, T.; Yamashita, M.; Yamauchi, K.; Inoue, G.; Suzuki, M.; Takaso, M.; Orita, S.; Eguchi, Y.; Ochiai, N.; et al. Existence of pyogenic spondylitis in Modic type 1 change without other signs of infection: 2-year follow-up. Eur. Spine J. 2010, 19, 1200–1205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.-H.; Zhao, C.-Q.; Jiang, L.-S.; Chen, X.-D.; Dai, L.-Y. Modic changes: A systematic review of the literature. Eur. Spine J. 2008, 17, 1289–1299. [Google Scholar] [CrossRef] [Green Version]
- Albert, H.; Kjaer, P.; Jensen, T.S.; Sorensen, J.; Bendix, T.; Manniche, C. Modic changes, possible causes and relation to low back pain. Med. Hypotheses 2008, 70, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Yan, M.; Song, Z.; Kou, H.; Shang, G.; Shang, C.; Chen, X.; Ji, Y.; Bao, D.; Cheng, T.; Li, J.; et al. New Progress in Basic Research of Macrophages in the Pathogenesis and Treatment of Low Back Pain. Front. Cell Dev. Biol. 2022, 10, 866857. [Google Scholar] [CrossRef]
- Li, J.; Chen, Y.; Wu, H.; Shan, Z.; Bei, D.; Gan, K.; Liu, J.; Zhang, X.; Chen, B.; Chen, J.; et al. Different responses of cervical intervertebral disc caused by low and high virulence bacterial infection: A comparative study in rats. Bioengineered 2022, 13, 12446–12461. [Google Scholar] [CrossRef]
- Rajasekaran, S.; Tangavel, C.; Aiyer, S.N.; Nayagam, S.M.; Raveendran, M.; Demonte, N.L.; Subbaiah, P.; Kanna, R.; Shetty, A.P.; Dharmalingam, K. ISSLS PRIZE IN CLINICAL SCIENCE 2017: Is infection the possible initiator of disc disease? An insight from proteomic analysis. Eur. Spine J. 2017, 26, 1384–1400. [Google Scholar] [CrossRef]
- Capoor, M.; Konieczna, A.; McDowell, A.; Ruzicka, F.; Smrcka, M.; Jancalek, R.; Maca, K.; Lujc, M.; Ahmed, F.; Birkenmaier, C.; et al. Pro-Inflammatory and Neurotrophic Factor Responses of Cells Derived from Degenerative Human Intervertebral Discs to the Opportunistic Pathogen Cutibacterium acnes. Int. J. Mol. Sci. 2021, 22, 2347. [Google Scholar] [CrossRef] [PubMed]
- Shan, Z.; Wang, X.; Zong, W.; Li, J.; Zheng, B.; Huang, B.; Zhang, X.; Chen, J.; Huang, Y. The Effect of Cutibacterium acnes Infection on Nerve Penetration in the Annulus Fibrosus of Lumbar Intervertebral Discs via Suppressing Oxidative Stress. Oxidative Med. Cell. Longev. 2022, 2022, 9120674. [Google Scholar] [CrossRef]
- Mayslich, C.; Grange, P.A.; Castela, M.; Marcelin, A.G.; Calvez, V.; Dupin, N. Characterization of a Cutibacterium acnes Camp Factor 1-Related Peptide as a New TLR-2 Modulator in In Vitro and Ex Vivo Models of Inflammation. Int. J. Mol. Sci. 2022, 23, 5065. [Google Scholar] [CrossRef]
- Lan, W.; Wang, X.; Tu, X.; Hu, X.; Lu, H. Different phylotypes of Cutibacterium acnes cause different modic changes in intervertebral disc degeneration. PLoS ONE 2022, 17, e0270982. [Google Scholar] [CrossRef]
- Zheng, Y.; Lin, Y.; Chen, Z.; Jiao, Y.; Yuan, Y.; Li, C.; Xu, X.; Cao, P. Propionibacterium acnes induces intervertebral discs degeneration by increasing MMP-1 and inhibiting TIMP-1 expression via the NF-kappaB pathway. Int. J. Clin. Exp. Pathol. 2018, 11, 3445–3453. [Google Scholar] [PubMed]
- Lin, Y.; Jiao, Y.; Yuan, Y.; Zhou, Z.; Zheng, Y.; Xiao, J.; Li, C.; Chen, Z.; Cao, P. Propionibacterium acnes induces intervertebral disc degeneration by promoting nucleus pulposus cell apoptosis via the TLR2/JNK/mitochondrial-mediated pathway. Emerg. Microbes Infect. 2018, 7, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Rocha, V.M.; Lima, C.O.G.X.; Ferreira, E.D.O.; de Farias, G.C.; Nogueira, F.C.S.; Antunes, L.C.M.; Cassiano, K.M.; Fiorelli, R.K.A. Colonization of intervertebral discs by Cutibacterium acnes in patients with low back pain: Protocol for an analytical study with microbiological, phenotypic, genotypic, and multiomic techniques. PLoS ONE 2022, 18, e0271773. [Google Scholar] [CrossRef]
- McDowell, A.; Barnard, E.; Nagy, I.; Gao, A.; Tomida, S.; Li, H.; Eady, A.; Cove, J.; Nord, C.E.; Patrick, S. An Expanded Multilocus Sequence Typing Scheme for Propionibacterium acnes: Investigation of ‘Pathogenic’, ‘Commensal’ and Antibiotic Resistant Strains. PLoS ONE 2012, 7, e41480. [Google Scholar] [CrossRef] [Green Version]
- Leheste, J.R.; Ruvolo, K.E.; Chrostowski, J.E.; Rivera, K.; Husko, C.; Miceli, A.; Selig, M.K.; Brüggemann, H.; Torres, G.P. acnes-Driven Disease Pathology: Current Knowledge and Future Directions. Front. Cell. Infect. Microbiol. 2017, 7, 81. [Google Scholar] [CrossRef] [Green Version]
- Rollason, J.; McDowell, A.; Albert, H.B.; Barnard, E.; Worthington, T.; Hilton, A.C.; Vernallis, A.; Patrick, S.; Elliott, T.; Lambert, P. Genotypic and Antimicrobial Characterisation of Propionibacterium acnes Isolates from Surgically Excised Lumbar Disc Herniations. BioMed. Res. Int. 2013, 2013, 530382. [Google Scholar] [CrossRef] [Green Version]
- Gharamti, A.A.; Kanafani, Z.A. Cutibacterium (formerly Propionibacterium) acnes infections associated with implantable devices. Expert Rev. Anti-Infect. Ther. 2017, 15, 1083–1094. [Google Scholar] [CrossRef] [PubMed]
- Mayslich, C.; Grange, P.; Dupin, N. Cutibacterium acnes as an Opportunistic Pathogen: An Update of Its Virulence-Associated Factors. Microorganisms 2021, 9, 303. [Google Scholar] [CrossRef] [PubMed]
- Nazipi, S.; Stødkilde, K.; Scavenius, C.; Brüggemann, H. The Skin Bacterium Propionibacterium acnes Employs Two Variants of Hyaluronate Lyase with Distinct Properties. Microorganisms 2017, 5, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lheure, C.; Grange, P.A.; Ollagnier, G.; Morand, P.; Désiré, N.; Sayon, S.; Corvec, S.; Raingeaud, J.; Marcelin, A.-G.; Calvez, V.; et al. TLR-2 Recognizes Propionibacterium acnes CAMP Factor 1 from Highly Inflammatory Strains. PLoS ONE 2016, 11, e0167237. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Che, M.; Xin, J.; Zheng, Z.; Li, J.; Zhang, S. The role of IL-1β and TNF-α in intervertebral disc degeneration. Biomed. Pharmacother. 2020, 131, 110660. [Google Scholar] [CrossRef]
- Slaby, O.; McDowell, A.; Brüggemann, H.; Raz, A.; Demir-Deviren, S.; Freemont, T.; Lambert, P.; Capoor, M.N. Is IL-1β Further Evidence for the Role of Propionibacterium acnes in Degenerative Disc Disease? Lessons From the Study of the Inflammatory Skin Condition Acne Vulgaris. Front. Cell. Infect. Microbiol. 2018, 8, 272. [Google Scholar] [CrossRef] [Green Version]
- Zhao, H.; Yu, X.; Tang, X.S.; He, F.; Yang, Y.D.; Xiong, Y.; Hu, Z.G.; Xu, L. [Relationship between inflammatory cytokines of IL-1beta and TNF-alpha and intervertebral disc degeneration]. Zhongguo Gu Shang 2017, 30, 866–871. [Google Scholar] [CrossRef]
- Johnson, Z.; Schoepflin, Z.; Choi, H.; Shapiro, I.; Risbud, M. Disc in flames: Roles of TNF-α and IL-1β in intervertebral disc degeneration. Eur. Cells Mater. 2015, 30, 104–117. [Google Scholar] [CrossRef]
- Capoor, M.N.; Ruzicka, F.; Sandhu, G.; Rollason, J.; Mavrommatis, K.; Ahmed, F.S.; Schmitz, J.E.; Raz, A.; Brüggemann, H.; Lambert, P.A.; et al. Importance of Propionibacterium acnes hemolytic activity in human intervertebral discs: A microbiological study. PLoS ONE 2018, 13, e0208144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freemont, A.; Peacock, T.; Goupille, P.; Hoyland, J.; O’Brien, J.; Jayson, M. Nerve ingrowth into diseased intervertebral disc in chronic back pain. Lancet 1997, 350, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Aroke, E.N.; Powell-Roach, K.L. The Metabolomics of Chronic Pain Conditions: A Systematic Review. Biol. Res. Nurs. 2020, 22, 458–471. [Google Scholar] [CrossRef]
- Riekeberg, E.; Powers, R. New frontiers in metabolomics: From measurement to insight. F1000Research 2017, 6, 1148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clish, C.B. Metabolomics: An emerging but powerful tool for precision medicine. Mol. Case Stud. 2015, 1, a000588. [Google Scholar] [CrossRef] [Green Version]
- Johnson, C.H.; Ivanisevic, J.; Siuzdak, G. Metabolomics: Beyond biomarkers and towards mechanisms. Nat. Rev. Mol. Cell Biol. 2016, 17, 451–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vlahou, A.; Fountoulakis, M. Proteomic approaches in the search for disease biomarkers. J. Chromatogr. B 2005, 814, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Teckchandani, S.; Gowda, G.A.N.; Raftery, D.; Curatolo, M. Metabolomics in chronic pain research. Eur. J. Pain 2021, 25, 313–326. [Google Scholar] [CrossRef]
- Swank, K.R.; Furness, J.E.; Baker, E.A.; Gehrke, C.K.; Biebelhausen, S.P.; Baker, K.C. Metabolomic Profiling in the Characterization of Degenerative Bone and Joint Diseases. Metabolites 2020, 10, 223. [Google Scholar] [CrossRef]
- Qiu, C.; Wu, X.; Bian, J.; Ma, X.; Zhang, G.; Guo, Z.; Wang, Y.; Ci, Y.; Wang, Q.; Xiang, H.; et al. Differential proteomic analysis of fetal and geriatric lumbar nucleus pulposus: Immunoinflammation and age-related intervertebral disc degeneration. BMC Musculoskelet. Disord. 2020, 21, 339. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Xiang, H.; Zhang, G.; Hu, Y.; Wang, Y.; Chen, B. A metabolic profiling analysis of degenerative intervertebral disc disease in a rabbit model via GC/TOF-MS. Res. Sq. 2019. [Google Scholar] [CrossRef] [Green Version]
- Rinschen, M.M.; Ivanisevic, J.; Giera, M.; Siuzdak, G. Identification of bioactive metabolites using activity metabolomics. Nat. Rev. Mol. Cell Biol. 2019, 20, 353–367. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Inclusion | Exclusion |
|---|---|
| Age between 18 and 65 years | History of previous lumbar spine surgery |
| LBP a lasting more than 3 months | Chemotherapy or pulse therapy with corticoids |
| MRI b performed less than 6 months before surgery | History of spinal infection |
| Failure of conservative treatment for at least 6 weeks | Previous intradiscal therapies |
| Data | Moment of Collection | |||
|---|---|---|---|---|
| Enrollment. | 1st Postop. Mo. | 3rd Postop. Mo | 6th Postop. Mo | |
| Age, gender, BMI a, No. of levels | X | |||
| Sedentary lifestyle, smoking | X | |||
| SAH b, diabetes, other comorbities | X | |||
| MRI c (Modic changes) | X | |||
| VNS d, DN4 e, ODI f | X | X | X | X |
| EuroQol questionnaire (EQ-5D) | X | X | ||
| Time off work | X | X | X | |
| Variable | Category | Global (n = 23) | C. acnes (−) (n = 15) | C. acnes (+) (n = 8) | p-Value |
|---|---|---|---|---|---|
| Gender | Female | 52.2% | 60.0% | 37.5% | 0.400 a |
| Male | 47.8% | 40.0% | 62.5% | ||
| BMI | Normal weight | 21.7% | 20.0% | 25.0% | 0.728 b |
| Overweight | 34.8% | 40.0% | 25.0% | ||
| Obesity I | 30.4% | 26.7% | 37.5% | ||
| Obesity II | 13.0% | 13.3% | 12.5% | ||
| Comorbidities | Diabetes | 47.8% | 33.3% | 75.0% | 0.089 a |
| Obesity | 43.5% | 40.0% | 50.0% | 0.667 a | |
| SAH c | 39.1% | 40.0% | 37.5% | 1.000 a | |
| Bad Habits | Smoking | 39.1% | 26.7% | 62.5% | 0.179 a |
| Sedentary Lifestyle | 60.9% | 53.3% | 75.0% | 0.400 a | |
| Preop. Pain | Sciatica | 56.5% | 53.3% | 62.5% | 1.000 a |
| Mechanics | 43.5% | 46.7% | 37.5% | ||
| Preop DN4 d | ≤1 | 26.1% | 26.7% | 25.0% | 0.899 a |
| 2 | 47.8% | 40.0% | 62.5% | ||
| 3 | 21.7% | 26.7% | 12.5% | ||
| ≥4 | 4.3% | 6.7% | 0.0% | ||
| Preop ODI e | Minimal/Moderate | 47.8% | 53.3% | 37.5% | 0.294 b |
| Severe/Crippled | 52.2% | 46.7% | 62.5% | 0.667 a |
| Number of Patients | 23 |
| Number of evaluated discs | 53 |
| Number of discs samples | 265 |
| Number of C. acnes positive patients | 8 |
| Number of C. acnes positive discs | 18 |
| Number of C. acnes positive samples | 79 |
| Prevalence of C. acnes positive patients | 34.8% |
| Variable | Category | Global (n = 23) | C. acnes (−) (n = 15) | C. acnes (+) (n = 8) | p-Value |
|---|---|---|---|---|---|
| Preoperative DN4 | Absent | 26.1% | 26.7% | 25.0% | 0.776 a |
| Possible | 21.7% | 26.7% | 12.5% | ||
| Probable | 47.8% | 40.0% | 62.5% | ||
| Present | 4.3% | 6.7% | 0.0% | ||
| DN4 1st month | Absent | 26.1% | 26.7% | 25.0% | 0.265 a |
| Possible | 47.8% | 73.3% | 0.0% | ||
| Probable | 13.0% | 0.0% | 37.5% | ||
| Present | 13.0% | 0.0% | 37.5% | ||
| DN4 3rd month | Absent | 43.5% | 60.0% | 12.5% | 0.019 a |
| Possible | 0,0% | 0.0% | 0.0% | ||
| Probable | 17.4% | 10.0% | 12.5% | ||
| Present | 39.1% | 10.0% | 75.0% | ||
| DN4 6th month | Absent | 60.0% | 60.0% | 0.0% | 0.011 a |
| Possible | 6.7% | 6.7% | 0.0% | ||
| Probable | 13.3% | 13.3% | 12.5% | ||
| Present | 20.0% | 20.0% | 87.5% |
| Domain | Assessment | Median Score in the Domain | ||
|---|---|---|---|---|
| C. acnes (−) | C. acnes (+) | p-Value b (Mann– Whitney b) | ||
| Mobility | Preoperative | 2.0 | 2.0 | 0.169 |
| Postoperative (6th month) | 1.0 | 1.0 | 0.213 | |
| 0.008 a | 0.025 a | - | ||
| Self-Care | Preoperative | 1.0 | 1.0 | 0.169 |
| Postoperative (6th month) | 1.0 | 1.0 | 0.056 | |
| 0.083 a | 0.157 a | - | ||
| Usual Activities | Preoperative | 1.5 | 1.5 | 0.875 |
| Postoperative (6th month) | 1.0 | 1.0 | 1.000 | |
| 0.025 a | 0.046 a | - | ||
| Pain or Discomfort | Preoperative | 2.0 | 3.0 | 0.591 |
| Postoperative (6th month) | 1.0 | 2.0 | 0.825 | |
| 0.001 a | 0.014 a | - | ||
| Anxiety or Depression | Preoperative | 2.00 | 2.00 | 0.548 |
| Postoperative (6th month) | 1.00 | 1.00 | 0.131 | |
| 0.008 a | 0.025 a | - | ||
| EQVas c | Preoperative | 80.0 | 90.0 | 1.000 |
| Postoperative (6th month) | 30.0 | 60.0 | 0.875 | |
| p-valor teste Wilcoxon a | 0.001 a | 0.011 a | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
da Rocha, V.M.; Lima, C.O.G.X.; Candido, G.B.; Mara Cassiano, K.; Lewandrowski, K.-U.; de Oliveira Ferreira, E.; Fiorelli, R.K.A. Would Cutibacterium acnes Be the Villain for the Chronicity of Low Back Pain in Degenerative Disc Disease? Preliminary Results of an Analytical Cohort. J. Pers. Med. 2023, 13, 598. https://doi.org/10.3390/jpm13040598
da Rocha VM, Lima COGX, Candido GB, Mara Cassiano K, Lewandrowski K-U, de Oliveira Ferreira E, Fiorelli RKA. Would Cutibacterium acnes Be the Villain for the Chronicity of Low Back Pain in Degenerative Disc Disease? Preliminary Results of an Analytical Cohort. Journal of Personalized Medicine. 2023; 13(4):598. https://doi.org/10.3390/jpm13040598
Chicago/Turabian Styleda Rocha, Vinícius Magno, Carla Ormundo Gonçalves Ximenes Lima, Gustavo Baptista Candido, Keila Mara Cassiano, Kai-Uwe Lewandrowski, Eliane de Oliveira Ferreira, and Rossano Kepler Alvim Fiorelli. 2023. "Would Cutibacterium acnes Be the Villain for the Chronicity of Low Back Pain in Degenerative Disc Disease? Preliminary Results of an Analytical Cohort" Journal of Personalized Medicine 13, no. 4: 598. https://doi.org/10.3390/jpm13040598