

Association between Serum Soluble Urokinase-Type Plasminogen Activator Receptor Level and Arterial Stiffness in Chronic Hemodialysis Patients
 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
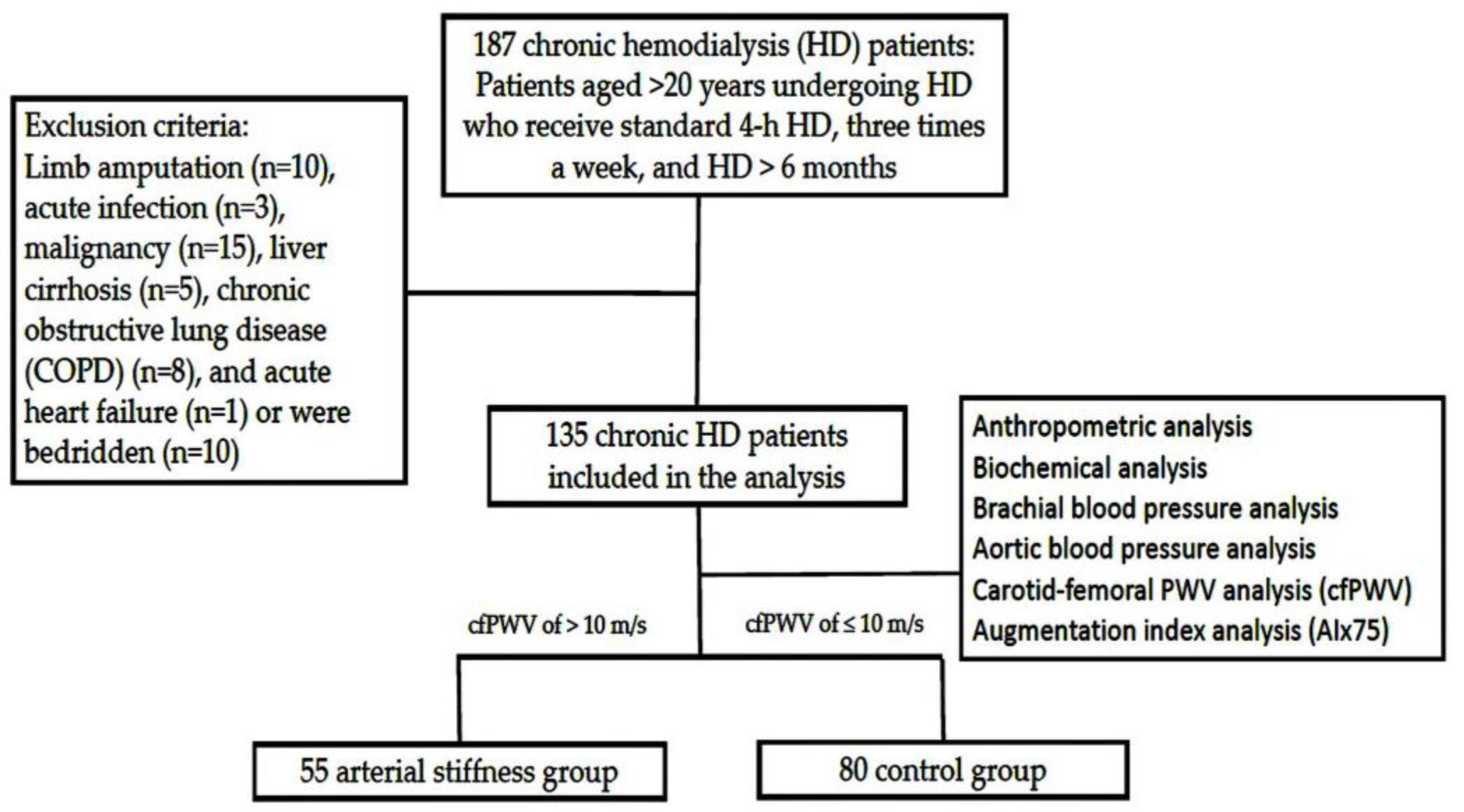
2.1. Patients
2.2. Anthropometric Analysis and Biochemical Investigations
2.3. Blood Pressure and Arterial Stiffness Measurements
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Laurent, S.; Boutouyrie, P. Arterial stiffness: A new surrogate end point for cardiovascular disease? J. Nephrol. 2007, 20, S45–S50. [Google Scholar]
- Major, R.W.; Cheng, M.R.I.; Grant, R.A.; Shantikumar, S.; Xu, G.; Oozeerally, I.; Brunskill, N.J.; Gray, L.J. Cardiovascular disease risk factors in chronic kidney disease: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0192895. [Google Scholar] [CrossRef]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Hui, X.; Matsushita, K.; Sang, Y.; Ballew, S.H.; Fülöp, T.; Coresh, J. CKD and cardiovascular disease in the Atherosclerosis Risk in Communities (ARIC) study: Interactions with age, sex, and race. Am. J. Kidney Dis. 2013, 62, 691–702. [Google Scholar] [CrossRef] [Green Version]
- Foley, R.N.; Parfrey, P.S.; Sarnak, M.J. Epidemiology of cardiovascular disease in chronic renal disease. J. Am. Soc. Nephrol. 1998, 9 (Suppl. S12), S16–S23. [Google Scholar] [CrossRef]
- Kakani, E.; Elyamny, M.; Ayach, T.; El-Husseini, A. Pathogenesis and management of vascular calcification in CKD and dialysis patients. Semin. Dial. 2019, 32, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, B.; Riemer, M.; Erbs, C.; Plehn, A.; Navarrete Santos, A.; Wienke, A.; Silber, R.E.; Simm, A. Carotid to femoral pulse wave velocity reflects the extent of coronary artery disease. J. Clin. Hypertens 2014, 16, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Q.; Hu, M.J.; Cui, Y.J.; Liang, L.; Zhou, M.M.; Yang, Y.W.; Huang, F. Carotid-femoral pulse wave velocity in the prediction of cardiovascular events and mortality: An updated systematic review and meta-analysis. Angiology 2018, 69, 617–629. [Google Scholar] [CrossRef]
- Tummalapalli, L.; Nadkarni, G.N.; Coca, S.G. Biomarkers for predicting outcomes in chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2016, 25, 480–486. [Google Scholar] [CrossRef]
- Goodchild, T.T.; Li, Z.; Lefer, D.J. Soluble urokinase plasminogen activator receptor: From biomarker to active participant in atherosclerosis and cardiovascular disease. J. Clin. Investig. 2022, 132, e165868. [Google Scholar] [CrossRef]
- Dupuy, A.M.; Kuster, N.; Bargnoux, A.S.; Aguilhon, S.; Huet, F.; Leclercq, F.; Pasquié, J.L.; Roubille, F.; Cristol, J.P. Long term pronostic value of suPAR in chronic heart failure: Reclassification of patients with low MAGGIC score. Clin. Chem. Lab. Med. 2021, 59, 1299–1306. [Google Scholar] [CrossRef]
- Sommerer, C.; Zeier, M.; Morath, C.; Reiser, J.; Scharnagl, H.; Stojakovic, T.; Delgado, G.E.; März, W.; Kleber, M.E. Soluble urokinase plasminogen activation receptor and long-term outcomes in persons undergoing coronary angiography. Sci. Rep. 2019, 9, 475. [Google Scholar] [CrossRef] [Green Version]
- Navab, K.D.; Elboudwarej, O.; Gharif, M.; Yu, J.; Hama, S.Y.; Safarpour, S.; Hough, G.P.; Vakili, L.; Reddy, S.T.; Navab, M.; et al. Chronic inflammatory disorders and accelerated atherosclerosis: Chronic kidney disease. Curr. Pharm. Des. 2011, 17, 17–20. [Google Scholar] [CrossRef]
- Hou, J.S.; Wang, C.H.; Lai, Y.H.; Kuo, C.H.; Lin, Y.L.; Hsu, B.G.; Tsai, J.P. Serum malondialdehyde-modified low-density lipoprotein is a risk factor for central arterial stiffness in maintenance hemodialysis patients. Nutrients 2020, 12, 2160. [Google Scholar] [CrossRef]
- Chiu, L.T.; Hung, C.D.; Lin, L.; Lin, Y.L.; Hsu, B.G. Serum fibroblast growth factor 21 level is associated with aortic stiffness in patients on maintenance hemodialysis. Int. J. Hypertens. 2022, 2022, 7098458. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabrera-Fischer, E.; Zocalo, Y.; Wray, S.; Bia, D. Arterial stiffness in haemodialyzed patients: Findings and controversies. Curr. Hypertens. Rev. 2018, 14, 100–106. [Google Scholar] [CrossRef]
- Tsai, J.P.; Hsu, B.G. Arterial stiffness: A brief review. Tzu Chi Med. J. 2020, 33, 115–121. [Google Scholar]
- Marchais, S.J.; Guerin, A.P.; Pannier, B.M.; Levy, B.I.; Safar, M.E.; London, G.M. Wave reflections and cardiac hypertrophy in chronic uremia. Influence of body size. Hypertension 1993, 22, 876–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, T.; Auer, J.; O’rourke, M.F.; Kvas, E.; Lassnig, E.; Lamm, G.; Stark, N.; Rammer, M.; Eber, B. Increased arterial wave reflections predict severe cardiovascular events in patients undergoing percutaneous coronary interventions. Eur. Heart J. 2005, 26, 2657–2663. [Google Scholar] [CrossRef]
- London, G.M.; Blacher, J.; Pannier, B.; Guérin, A.P.; Marchais, S.J.; Safar, M.E. Arterial wave reflections and survival in end-stage renal failure. Hypertension 2001, 38, 434–438. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, L.J.H.; Petersen, J.E.V.; Eugen-Olsen, J. Soluble urokinase plasminogen activator receptor (suPAR) as a biomarker of systemic chronic inflammation. Front. Immunol. 2021, 12, 780641. [Google Scholar] [CrossRef]
- Fuhrman, B. The urokinase system in the pathogenesis of atherosclerosis. Atherosclerosis 2012, 222, 8–14. [Google Scholar] [CrossRef]
- Zeng, M.; Chang, M.; Zheng, H.; Li, B.; Chen, Y.; He, W.; Huang, C. Clinical value of soluble urokinase-type plasminogen activator receptor in the diagnosis, prognosis, and therapeutic guidance of sepsis. Am. J. Emerg. Med. 2016, 34, 375–380. [Google Scholar] [CrossRef]
- Toldi, G.; Bekő, G.; Kádár, G.; Mácsai, E.; Kovács, L.; Vásárhelyi, B.; Balog, A. Soluble urokinase plasminogen activator receptor (suPAR) in the assessment of inflammatory activity of rheumatoid arthritis patients in remission. Clin. Chem. Lab. Med. 2013, 51, 327–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galliera, E.; Drago, L.; Marazzi, M.G.; Romanò, C.; Vassena, C.; Corsi Romanelli, M.M. Soluble urokinase-type plasminogen activator receptor (suPAR) as new biomarker of the prosthetic joint infection: Correlation with inflammatory cytokines. Clin. Chim. Acta 2015, 441, 23–28. [Google Scholar] [CrossRef]
- Heraclides, A.; Jensen, T.M.; Rasmussen, S.S.; Eugen-Olsen, J.; Haugaard, S.B.; Borch-Johnsen, K.; Sandbæk, A.; Lauritzen, T.; Witte, D.R. The pro-inflammatory biomarker soluble urokinase plasminogen activator receptor (suPAR) is associated with incident type 2 diabetes among overweight but not obese individuals with impaired glucose regulation: Effect modification by smoking and body weight status. Diabetologia 2013, 56, 1542–1546. [Google Scholar] [PubMed] [Green Version]
- Persson, M.; Östling, G.; Smith, G.; Hamrefors, V.; Melander, O.; Hedblad, B.; Engström, G. Soluble urokinase plasminogen activator receptor: A risk factor for carotid plaque, stroke, and coronary artery disease. Stroke 2014, 45, 18–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayek, S.S.; Sever, S.; Ko, Y.A.; Trachtman, H.; Awad, M.; Wadhwani, S.; Altintas, M.M.; Wei, C.; Hotton, A.L.; French, A.L.; et al. Soluble urokinase receptor and chronic kidney disease. N. Engl. J. Med. 2015, 373, 1916–1925. [Google Scholar] [CrossRef] [PubMed]
- Schutte, A.E.; Myburgh, A.; Olsen, M.H.; Eugen-Olsen, J.; Schutte, R. Exploring soluble urokinase plasminogen activator receptor and its relationship with arterial stiffness in a bi-ethnic population: The SAfrEIC-study. Thromb. Res. 2012, 130, 273–277. [Google Scholar] [CrossRef]
- Böcskei, R.M.; Benczúr, B.; Losonczy, G.; Illyés, M.; Cziráki, A.; Müller, V.; Bohács, A.; Bikov, A. Soluble urokinase-type plasminogen activator receptor and arterial stiffness in patients with COPD. Lung 2019, 197, 189–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theilade, S.; Lyngbaek, S.; Hansen, T.W.; Eugen-Olsen, J.; Fenger, M.; Rossing, P.; Jeppesen, J.L. Soluble urokinase plasminogen activator receptor levels are elevated and associated with complications in patients with type 1 diabetes. J. Intern Med. 2015, 277, 362–371. [Google Scholar] [CrossRef] [PubMed]
- Erdan, A.; Ozkok, A.; Alpay, N.; Akkaya, V.; Yildiz, A. Volume status and arterial blood pressures are associated with arterial stiffness in hemodialysis patients. Int. J. Artif. Organs 2018, 41, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Georgianos, P.I.; Sarafidis, P.A.; Malindretos, P.; Nikolaidis, P.; Lasaridis, A.N. Hemodialysis reduces augmentation index but not aortic or brachial pulse wave velocity in dialysis-requiring patients. Am. J. Nephrol. 2011, 34, 407–414. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | All Patients (n = 135) | Control Group (n = 80) | Arterial Stiffness Group (n = 55) | p Value |
|---|---|---|---|---|
| Age (years) | 62.8 ± 13.3 | 60.2 ± 13.6 | 66.4 ± 12.1 | 0.007 * |
| HD vintage (months) | 56.2 (23.5–123.6) | 65.9 (21.8–132.9) | 53.4 (25.8–104.6) | 0.483 |
| Height (cm) | 159.9 ± 8.4 | 159.5 ± 8.6 | 160.5 ± 8.1 | 0.524 |
| Pre-HD BW (Kg) | 63.6 ± 14.8 | 62.9 ± 15.7 | 64.5 ± 13.5 | 0.551 |
| Post-HD BW (Kg) | 61.4 ± 14.3 | 60.8 ± 15.2 | 62.2 ± 13.1 | 0.559 |
| BMI (Kg/m2) | 25.00 ± 5.0 | 24.8 ± 5.4 | 25.3 ± 4.5 | 0.556 |
| Aortic SBP (mmHg) | 133.8 ± 26.0 | 129.9 ± 25.8 | 139.6 ± 25.5 | 0.034 * |
| Aortic DBP (mmHg) | 79.5 ± 18.5 | 79.5 ± 18.8 | 79.5 ± 18.1 | 0.993 |
| Carotid–femoral PWV (m/s) | 9.4 ± 2.1 | 7.9 ± 1.1 | 11.5 ± 1.0 | <0.001 * |
| AIx75 (%) | 31.3 ± 6.7 | 30.0 ± 7.2 | 33.4 ± 25.2 | 0.003 * |
| Brachial SBP (mmHg) | 144.0 ± 27.0 | 139.7 ± 27.3 | 150.2 ± 25.4 | 0.025 * |
| Brachial DBP (mmHg) | 78.1 ± 16.7 | 78.3 ± 16.2 | 77.8 ± 17.7 | 0.861 |
| Albumin (g/dL) | 4.1 (3.9–4.4) | 4.1 (3.9–4.4) | 4.1 (3.9–4.3) | 0.397 |
| Total cholesterol (mg/dL) | 145.3 ± 34.5 | 148.1 ± 38.0 | 141.2 ± 28.6 | 0.257 |
| Triglyceride (mg/dL) | 117.0 (84.0–178.0) | 110.5 (83.3–199.5) | 122.0 (89.0–175.0) | 0.722 |
| Glucose (mg/dL) | 132.0 (105.0–173.0) | 127.5 (103.0–151.0) | 145.0 (111.0–194.0) | 0.019 * |
| BUN (mg/dL) | 61.4 ± 15.0 | 60.7 ± 14.2 | 62.5 ± 16.0 | 0.497 |
| Creatinine (mg/dL) | 9.37 ± 2.05 | 9.43 ± 2.09 | 9.28 ± 2.00 | 0.675 |
| Total calcium (mg/dL) | 9.01 ± 0.78 | 8.92 ± 0.73 | 9.14 ± 0.83 | 0.108 |
| Phosphorus (mg/dL) | 4.72 ± 1.29 | 4.75 ± 1.32 | 4.66 ± 1.26 | 0.696 |
| iPTH (pg/mL) | 222.9 (126.7–410.1) | 249.4 (130.3–449.4) | 192.9 (118.5–374.2) | 0.298 |
| Alkaline phosphatase (IU/L) | 76.0 (61.0–107.0) | 77.0 (62.0–102.0) | 76.0 (60.0–113.0) | 0.757 |
| suPAR (ng/mL) | 3.13 (2.29–5.30) | 2.54 (2.07–3.58) | 5.14 (3.16–7.87) | <0.001 * |
| C-reactive protein (mg/dL) | 0.30 (0.08–0.95) | 0.23 (0.05–0.92) | 0.45 (0.18–1.01) | 0.039 * |
| Urea reduction rate | 0.73 ± 0.04 | 0.73 ± 0.05 | 0.73 ± 0.04 | 0.936 |
| Kt/V (Gotch) | 1.34 ± 0.17 | 1.34 ± 0.18 | 1.34 ± 0.16 | 0.966 |
| Female, n (%) | 66 (48.9) | 42 (52.5) | 24 (43.6) | 0.311 |
| Diabetes mellitus, n (%) | 56 (41.5) | 24 (30.0) | 32 (58.2) | 0.001 * |
| Hypertension, n (%) | 74 (54.8) | 38 (47.5) | 36 (65.5) | 0.039 * |
| Angiotensin receptor blocker, n (%) | 39 (28.9) | 20 (25.0) | 19 (34.5) | 0.229 |
| β-blocker, n (%) | 42 (31.1) | 22 (27.5) | 20 (36.4) | 0.274 |
| Calcium channel blocker, n (%) | 51 (37.8) | 27 (33.8) | 24 (43.6) | 0.244 |
| Arteriovenous fistula, n (%) | 96 (71.1) | 56 (70.0) | 40 (72.7) | 0.552 |
| Arteriovenous graft, n (%) | 36 (26.7) | 23 (63.9) | 13 (36.1) | |
| Perm catheter, n (%) | 3 (2.2) | 1 (1.3) | 2 (3.6) |
| Variables | Odds Ratio | 95% Confidence Interval | p Value |
|---|---|---|---|
| suPAR, 1 ng/mL | 2.05 | 1.58–2.70 | <0.001 * |
| Age, 1 year | 1.04 | 1.00–1.08 | 0.046 * |
| Glucose, 1 mg/dL | 1.01 | 1.00–1.02 | 0.007 * |
| C-reactive protein, 0.1 mg/dL | 0.98 | 0.94–1.02 | 0.243 |
| Aortic SBP, 1 mmHg | 1.04 | 1.00–1.09 | 0.055 |
| Brachial SBP, 1 mmHg | 0.97 | 0.94–1.02 | 0.209 |
| Diabetes mellitus (present) | 2.50 | 0.76–5.53 | 0.155 |
| Hypertension (present) | 1.94 | 0.65–5.82 | 0.235 |
| Variables | Carotid–Femoral Pulse Wave Velocity (m/s) | ||||
|---|---|---|---|---|---|
| Simple Linear Regression | Multivariable Linear Regression | ||||
| r | p Value | Beta | Adjusted R2 Change | p Value | |
| Female | −0.12 | 0.162 | — | — | — |
| Diabetes mellitus | 0.26 | 0.003 * | — | — | — |
| Hypertension | 0.16 | 0.057 | — | — | — |
| Age (years) | 0.26 | 0.002 * | 0.17 | 0.023 | 0.021 * |
| Log-HD vintage (months) | −0.14 | 0.096 | — | — | — |
| Height (cm) | 0.05 | 0.587 | — | — | — |
| Pre-HD BW (Kg) | 0.10 | 0.265 | — | — | — |
| BMI (Kg/m2) | 0.11 | 0.202 | — | — | — |
| Aortic SBP (mmHg) | 0.23 | 0.009 * | 0.25 | 0.052 | 0.001 * |
| Aortic DBP (mmHg) | 0.06 | 0.493 | — | — | — |
| Brachial SBP (mmHg) | 0.18 | 0.041 * | — | — | — |
| Brachial DBP (mmHg) | 0.05 | 0.592 | — | — | — |
| Log-Albumin (g/dL) | −0.07 | 0.453 | — | — | — |
| TCH (mg/dL) | −0.08 | 0.339 | — | — | — |
| Log-TG (mg/dL) | 0.03 | 0.704 | — | — | — |
| Log-Glucose (mg/dL) | 0.20 | 0.023 * | — | — | — |
| BUN (mg/dL) | 0.02 | 0.800 | — | — | — |
| Creatinine (mg/dL) | −0.002 | 0.978 | — | — | — |
| Total calcium (mg/dL) | 0.07 | 0.448 | — | — | — |
| Phosphorus (mg/dL) | 0.02 | 0.794 | — | — | — |
| Log-iPTH (pg/mL) | −0.09 | 0.297 | — | — | — |
| Log-ALP (IU/L) | −0.03 | 0.758 | — | — | — |
| Log-suPAR (pg/mL) | 0.51 | <0.001 * | 0.48 | 0.250 | <0.001 * |
| Log-CRP (mg/dL) | 0.19 | 0.024 * | — | — | — |
| Urea reduction rate | −0.03 | 0.738 | — | — | — |
| Kt/V (Gotch) | −0.03 | 0.716 | — | — | — |
| Variables | Spearman’s Correlation Coefficient | p Value |
|---|---|---|
| Female | 0.020 | 0.815 |
| Diabetes mellitus | 0.171 | 0.047 * |
| Hypertension | 0.032 | 0.709 |
| Age (years) | 0.222 | 0.010 * |
| Log-HD vintage (months) | −0.001 | 0.994 |
| Height (cm) | −0029 | 0.740 |
| Pre-HD BW (Kg) | 0.029 | 0.741 |
| BMI (Kg/m2) | 0.064 | 0.463 |
| Aortic SBP (mmHg) | −0.025 | 0.774 |
| Aortic DBP (mmHg) | −0.086 | 0.322 |
| Brachial SBP (mmHg) | 0.042 | 0.632 |
| Brachial DBP (mmHg) | −0.127 | 0.142 |
| Log-Albumin (g/dL) | 0.074 | 0.391 |
| TCH (mg/dL) | 0.074 | 0.391 |
| Log-TG (mg/dL) | 0.132 | 0.128 |
| Log-Glucose (mg/dL) | 0.047 | 0.589 |
| BUN (mg/dL) | 0.124 | 0.153 |
| Creatinine (mg/dL) | −0.015 | 0.860 |
| Total calcium (mg/dL) | 0.134 | 0.120 |
| Phosphorus (mg/dL) | 0.022 | 0.804 |
| Log-iPTH (pg/mL) | −0.119 | 0.169 |
| Log-ALP (IU/L) | −0.018 | 0.837 |
| Log-CRP (mg/dL) | 0.324 | <0.001 * |
| Urea reduction rate | 0.053 | 0.538 |
| Kt/V (Gotch) | 0.036 | 0.680 |
| Carotid–femoral PWV (m/s) | 0.506 | <0.001 * |
| AIx75 (%) | 0.250 | 0.003 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, W.-C.; Wu, T.-J.; Wang, C.-H.; Hsieh, Y.-J.; Hsu, B.-G. Association between Serum Soluble Urokinase-Type Plasminogen Activator Receptor Level and Arterial Stiffness in Chronic Hemodialysis Patients. J. Pers. Med. 2023, 13, 470. https://doi.org/10.3390/jpm13030470
Lin W-C, Wu T-J, Wang C-H, Hsieh Y-J, Hsu B-G. Association between Serum Soluble Urokinase-Type Plasminogen Activator Receptor Level and Arterial Stiffness in Chronic Hemodialysis Patients. Journal of Personalized Medicine. 2023; 13(3):470. https://doi.org/10.3390/jpm13030470
Chicago/Turabian StyleLin, Wei-Chen, Tsung-Jui Wu, Chih-Hsien Wang, Yi-Jen Hsieh, and Bang-Gee Hsu. 2023. "Association between Serum Soluble Urokinase-Type Plasminogen Activator Receptor Level and Arterial Stiffness in Chronic Hemodialysis Patients" Journal of Personalized Medicine 13, no. 3: 470. https://doi.org/10.3390/jpm13030470