
The Role of Molecular Imaging in Personalized Medicine
 , ,
, ,
Abstract
:1. Introduction
2. Ultrasound (US)
3. Magnetic Resonance Imaging (MRI)
4. Single-Photon Emission Computerized Tomography (SPECT)
4.1. Hybrid SPECT
4.2. SPECT/CT
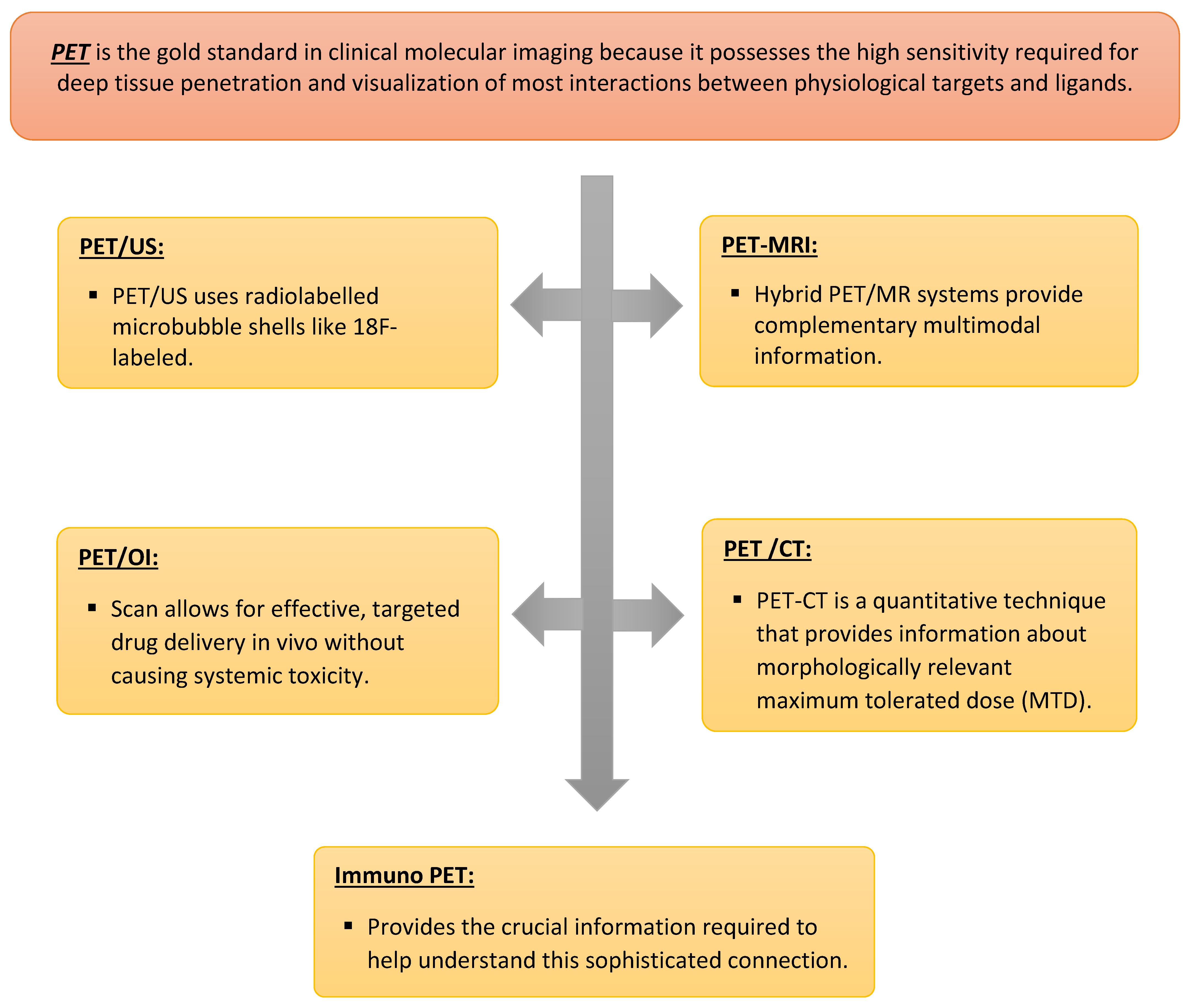
5. Positron Emission Tomography (PET)
5.1. PET-US
5.2. PET-MRI
5.3. Positron Emission Tomography-Optical Imaging (PET-OI)
5.4. Immuno-PET
5.5. PET-CT
6. Conclusions and Future Direction
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schillaci, O.; Urbano, N. Personalized Medicine: A New Option for Nuclear Medicine and Molecular Imaging in the Third Millennium. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 563–566. [Google Scholar] [CrossRef] [Green Version]
- Papp, L.; Spielvogel, C.P.; Rausch, I.; Hacker, M.; Beyer, T. Personalizing Medicine through Hybrid Imaging and Medical Big Data Analysis. Front. Phys. 2018, 6, 51. [Google Scholar] [CrossRef]
- Kircher, M.F.; Hricak, H.; Larson, S.M. Molecular Imaging for Personalized Cancer Care. Mol. Oncol. 2012, 6, 182–195. [Google Scholar] [CrossRef]
- Muresanu, C.; Khalchitsky, S. Updated Understanding of the Causes of Cancer, and a New Theoretical Perspective of Combinational Cancer Therapies, a Hypothesis. DNA Cell Biol. 2022, 41, 342–355. [Google Scholar] [CrossRef]
- Balber, T.; Tran, L.; Benčurová, K.; Raitanen, J.; Egger, G.; Mitterhauser, M. Experimental Nuclear Medicine Meets Tumor Biology. Pharmaceuticals 2022, 15, 227. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Ning, N.; Meng, X.; Chittasupho, C.; Jiang, L.; Zhao, Y. Sequential Drug Delivery in Targeted Cancer Therapy. Pharmaceutics 2022, 14, 573. [Google Scholar] [CrossRef] [PubMed]
- Preuss, K.; Thach, N.; Liang, X.; Baine, M.; Chen, J.; Zhang, C.; Du, H.; Yu, H.; Lin, C.; Hollingsworth, M.A.; et al. Using Quantitative Imaging for Personalized Medicine in Pancreatic Cancer: A Review of Radiomics and Deep Learning Applications. Cancers 2022, 14, 1654. [Google Scholar] [CrossRef]
- Chakravarty, R.; Goel, S.; Cai, W. Nanobody: The “Magic Bullet” for Molecular Imaging? Theranostics 2014, 4, 386–398. [Google Scholar] [CrossRef]
- Lyra, V.; Chatziioannou, S.; Kallergi, M. Clinical Perspectives for 18F-FDG PET Imaging in Pediatric Oncology: Μetabolic Tumor Volume and Radiomics. Metabolites 2022, 12, 217. [Google Scholar] [CrossRef] [PubMed]
- Balma, M.; Liberini, V.; Racca, M.; Laudicella, R.; Bauckneht, M.; Buschiazzo, A.; Nicolotti, D.G.; Peano, S.; Bianchi, A.; Albano, G.; et al. Non-Conventional and Investigational Pet Radiotracers for Breast Cancer: A Systematic Review. Front. Med. 2022, 9, 881551. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.C. Paving the Way to Personalized Medicine: Production of Some Promising Theragnostic Radionuclides at Brookhaven National Laboratory. Semin. Nucl. Med. 2012, 42, 151–163. [Google Scholar] [CrossRef]
- Rowe, S.P.; Pomper, M.G. Molecular Imaging in Oncology: Current Impact and Future Directions. CA A Cancer J. Clin. 2021, 72, 333–352. [Google Scholar] [CrossRef]
- Pither, R. Pet and the Role of in Vivo Molecular Imaging in Personalized Medicine. Expert Rev. Mol. Diagn. 2003, 3, 703–713. [Google Scholar] [CrossRef]
- Ghasemi, M.; Nabipour, I.; Omrani, A.; Alipour, Z.; Assadi, M. Precision Medicine and Molecular Imaging: New Targeted Approaches toward Cancer Therapeutic and Diagnosis. Am. J. Nucl. Med. Mol. Imaging 2016, 6, 310–327. [Google Scholar] [PubMed]
- Jain, K.K. Role of Nano-Biotechnology in the Development of Personalized Medicine. Technol. Cancer Res. Treat. 2005, 4, 645–650. [Google Scholar]
- Kim, J.; Lee, N.; Hyeon, T. Recent Development of Nanoparticles for Molecular Imaging. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2017, 375, 20170022. [Google Scholar] [CrossRef] [PubMed]
- Ryu, J.H.; Lee, S.; Son, S.; Kim, S.H.; Leary, J.F.; Choi, K.; Kwon, I.C. Theranostic Nanoparticles for Future Personalized Medicine. J. Control. Release 2014, 190, 477–484. [Google Scholar] [CrossRef]
- Pan, D.; Lanza, G.M.; Wickline, S.A.; Caruthers, S.D. Nanomedicine: Perspective and Promises with Ligand-Directed Molecular Imaging. Eur. J. Radiol. 2009, 70, 274–285. [Google Scholar] [CrossRef]
- Cai, W.; Chen, X. Nanoplatforms for Targeted Molecular Imaging in Living Subjects. Small 2007, 3, 1840–1854. [Google Scholar] [CrossRef] [PubMed]
- Eckelman, W.C.; Reba, R.C.; Kelloff, G.J. Targeted Imaging: An Important Biomarker for Understanding Disease Progression in the Era of Personalized Medicine. Drug Discov. Today 2008, 13, 748–759. [Google Scholar] [CrossRef] [PubMed]
- Dhingra, V.K.; Mahajan, A.; Basu, S. Emerging Clinical Applications of PET Based Molecular Imaging in Oncology: The Promising Future Potential for Evolving Personalized Cancer Care. Indian J. Radiol. Imaging 2015, 25, 332–341. [Google Scholar] [CrossRef] [PubMed]
- Tymińska, A.; Ozierański, K.; Skwarek, A.; Kapłon-Cieślicka, A.; Baritussio, A.; Grabowski, M.; Marcolongo, R.; Caforio, A.L.P. Personalized Management of Myocarditis and Inflammatory Cardiomyopathy in Clinical Practice. J. Pers. Med. 2022, 12, 183. [Google Scholar] [CrossRef]
- Gennisson, J.-L.; Deffieux, T.; Fink, M.; Tanter, M. Ultrasound Elastography: Principles and Techniques. Diagn. Interv. Imaging 2013, 94, 487–495. [Google Scholar] [CrossRef]
- Wang, H.; Mislati, R.; Ahmed, R.; Vincent, P.; Nwabunwanne, S.F.; Gunn, J.R.; Pogue, B.W.; Doyley, M.M. Elastography Can Map the Local Inverse Relationship between Shear Modulus and Drug Delivery within the Pancreatic Ductal Adenocarcinoma Microenvironment. Clin. Cancer Res. 2019, 25, 2136–2143. [Google Scholar] [CrossRef] [Green Version]
- Garra, B.S. Elastography: History, Principles, and Technique Comparison. Abdom. Imaging 2015, 40, 680–697. [Google Scholar] [CrossRef] [PubMed]
- Sigrist, R.M.S.; Liau, J.; Kaffas, A.E.; Chammas, M.C.; Willmann, J.K. Ultrasound Elastography: Review of Techniques and Clinical Applications. Theranostics 2017, 7, 1303–1329. [Google Scholar] [CrossRef] [PubMed]
- Itoh, A.; Ueno, E.; Tohno, E.; Kamma, H.; Takahashi, H.; Shiina, T.; Yamakawa, M.; Matsumura, T. Breast Disease: Clinical Application of US Elastography for Diagnosis. Radiology 2006, 239, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, B.F.; Kennedy, K.M.; Sampson, D.D. A Review of Optical Coherence Elastography: Fundamentals, Techniques and Prospects. IEEE J. Sel. Top. Quantum Electron. 2014, 20, 272–288. [Google Scholar] [CrossRef]
- Jin, J.; Yang, L.; Chen, F.; Gu, N. Drug Delivery System Based on Nanobubbles. Interdiscip. Mater. 2022, 1, 471–494. [Google Scholar] [CrossRef]
- Dammes, N.; Peer, D. Monoclonal Antibody-Based Molecular Imaging Strategies and Theranostic Opportunities. Theranostics 2020, 10, 938–955. [Google Scholar] [CrossRef] [PubMed]
- Chakravarty, R.; Hong, H.; Cai, W. Positron Emission Tomography Image-Guided Drug Delivery: Current Status and Future Perspectives. Mol. Pharm. 2014, 11, 3777–3797. [Google Scholar] [CrossRef]
- Frinking, P.; Segers, T.; Luan, Y.; Tranquart, F. Three Decades of Ultrasound Contrast Agents: A Review of the Past, Present and Future Improvements. Ultrasound Med. Biol. 2020, 46, 892–908. [Google Scholar] [CrossRef] [Green Version]
- Stride, E.; Saffari, N. Microbubble Ultrasound Contrast Agents: A Review. J. Eng. Med. 2003, 217, 429–447. [Google Scholar] [CrossRef]
- Keller, M.W.; Glasheen, W.; Kaul, S. Albunex: A Safe and Effective Commercially Produced Agent for Myocardial Contrast Echocardiography. J. Am. Soc. Echocardiogr. 1989, 2, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Caskey, C.F.; Ferrara, K.W. Ultrasound Contrast Microbubbles in Imaging and Therapy: Physical Principles and Engineering. Phys. Med. Biol. 2009, 54, 4621. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Miyoshi, H.; Nakamura, M. Encapsulated Ultrasound Microbubbles: Therapeutic Application in Drug/Gene Delivery. J. Control. Release 2006, 114, 89–99. [Google Scholar] [CrossRef]
- Yeh, C.-K.; Kang, S.-T. Ultrasound Microbubble Contrast Agents for Diagnostic and Therapeutic Applications: Current Status and Future Design. Biomed. J. 2012, 35, 125–139. [Google Scholar] [CrossRef] [PubMed]
- Yusefi, H.; Helfield, B. Ultrasound Contrast Imaging: Fundamentals and Emerging Technology. Front. Phys. 2022, 10, 1–16. [Google Scholar] [CrossRef]
- Nihonmatsu, H.; Numata, K.; Fukuda, H.; Tanaka, K.; Ooba, M.; Maeda, S. Low Mechanical Index Contrast Mode versus High Mechanical Index Contrast Mode: Which Is a More Sensitive Method for Detecting Sonazoid Microbubbles in the Liver of Normal Subjects? J. Med. Ultrason. 2015, 43, 211–217. [Google Scholar] [CrossRef]
- Bartolotta, T.V.; Taibb, A.; Midiri, M.; Lagalla, R. Contrast Enhanced Ultrasound of Hepatocellular Carcinoma. Korean Soc. Ultrasound Med. 2019, 38, 200–214. [Google Scholar]
- Kotopoulis, S.; Popa, M.; Mayoral Safont, M.; Murvold, E.; Haugse, R.; Langer, A.; Dimcevski, G.; Lam, C.; Bjånes, T.; Gilja, O.H.; et al. SonoVue® vs. Sonazoid™ vs. Optison™: Which Bubble Is Best for Low-Intensity Sonoporation of Pancreatic Ductal Adenocarcinoma? Pharmaceutics 2022, 14, 98. [Google Scholar] [CrossRef] [PubMed]
- Dijkmans, P.A.; Juffermans, L.J.M.; Musters, R.J.P.; van Wamel, A.; Ten Cate, F.J.; van Gilst, W.; Visser, C.A.; de Jong, N.; Kamp, O. Microbubbles and Ultrasound: From Diagnosis to Therapy. Eur. J. Echocardiogr. 2004, 5, 245–256. [Google Scholar] [CrossRef]
- Tinkov, S.; Bekeredjian, R.; Winter, G.; Coester, C. Microbubbles as Ultrasound Triggered Drug Carriers. J. Pharm. Sci. 2009, 98, 1935–1961. [Google Scholar] [CrossRef] [PubMed]
- Porter, T.R.; LeVeen, R.F.; Fox, R.; Kricsfeld, A.; Xie, F. Thrombolytic Enhancement with Perfluorocarbon-Exposed Sonicated Dextrose Albumin Microbubbles. Am. Heart J. 1996, 132, 964–968. [Google Scholar] [CrossRef]
- Rosa, L.; Blackledge, J.; Boretti, A. Nano-Magnetic Resonance Imaging (Nano-MRI) Gives Personalized Medicine a New Perspective. Biomedicines 2017, 5, 7. [Google Scholar] [CrossRef] [Green Version]
- Simonsen, S.A.; West, A.S.; Heiberg, A.V.; Wolfram, F.; Jennum, P.J.; Iversen, H.K. Is the Toast Classification Suitable for Use in Personalized Medicine in Ischemic Stroke? J. Pers. Med. 2022, 12, 496. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.J.; Tsai, F.Y.; Inoue, T.; Liao, M.-H.; Kong, F.-L.; Song, S. Molecular Imaging-Guided Theranostics and Personalized Medicine. BioMed Res. Int. 2013, 2013, 859453. [Google Scholar] [CrossRef] [Green Version]
- Belkić, D.; Belkić, K. Molecular Imaging in the Framework of Personalized Cancer Medicine. Isr. Med. Assoc. J. 2013, 15, 665–672. [Google Scholar]
- Woźniak, M.; Płoska, A.; Siekierzycka, A.; Dobrucki, L.W.; Kalinowski, L.; Dobrucki, I.T. Molecular Imaging and Nanotechnology—Emerging Tools in Diagnostics and Therapy. Int. J. Mol. Sci. 2022, 23, 2658. [Google Scholar] [CrossRef]
- Boustani, A.M.; Pucar, D.; Saperstein, L. Molecular Imaging of Prostate Cancer. Br. Inst. Radiol. 2018, 91, 1–10. [Google Scholar] [CrossRef]
- Jain, K.K. The Handbook of Nanomedicine; Humana Press/Springer: Totowa, NJ, USA, 2019; pp. 569–574. [Google Scholar]
- Pysz, M.A.; Gambhir, S.S.; Willmann, J.K. Molecular Imaging: Current Status and Emerging Strategies. Clin. Radiol. 2010, 65, 500–516. [Google Scholar] [CrossRef] [Green Version]
- Hu, H.; Quintana, J.; Weissleder, R.; Parangi, S.; Miller, M. Deciphering Albumin-Directed Drug Delivery by Imaging. Adv. Drug Deliv. Rev. 2022, 185, 114237. [Google Scholar] [CrossRef]
- Nunn, A.D. Update: Molecular Imaging and Personalized Medicine: An Uncertain Future. Cancer Biother. Radiopharm. 2007, 22, 722–739. [Google Scholar] [CrossRef]
- Sevick-Muraca, E.M.; Rasmussen, J.C. Molecular Imaging with Optics: Primer and Case for near-Infrared Fluorescence Techniques in Personalized Medicine. J. Biomed. Opt. 2008, 13, 1–39. [Google Scholar] [CrossRef] [PubMed]
- Tassa, C.; Shaw, S.Y.; Weissleder, R. Dextran-Coated Iron Oxide Nanoparticles: A Versatile Platform for Targeted Molecular Imaging, Molecular Diagnostics, and Therapy. Acc. Chem. Res. 2011, 44, 842–852. [Google Scholar] [CrossRef] [Green Version]
- Aboagye, E.O.; Kraeber-Bodéré, F. Highlights Lecture EANM 2016: “Embracing Molecular Imaging and Multi-Modal Imaging: A Smart Move for Nuclear Medicine towards Personalized Medicine. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1559–1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barajas, R.; Krohn, K.; Link, J.; Hawkins, R.; Clarke, J.; Pampaloni, M.; Cha, S. Glioma FMISO PET/MR Imaging Concurrent with Antiangiogenic Therapy: Molecular Imaging as a Clinical Tool in the Burgeoning Era of Personalized Medicine. Biomedicines 2016, 4, 24. [Google Scholar] [CrossRef] [Green Version]
- Sala, E.; Vargas, H.A.; Donati, O.F.; Weber, W.A.; Hricak, H. Role of Molecular Imaging in the Era of Personalized Medicine: A Review. Funct. Imaging Oncol. 2013, 49, 43–58. [Google Scholar]
- Jung, K.-H.; Lee, K.-H. Molecular Imaging in the Era of Personalized Medicine. J. Pathol. Transl. Med. 2015, 49, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.M.; Fadaie, F.; Gill, R.; Caldairou, B.; Sziklas, V.; Crane, J.; Hong, S.-J.; Bernhardt, B.C.; Bernasconi, A.; Bernasconi, N. Decomposing MRI Phenotypic Heterogeneity in Epilepsy: A Step towards Personalized Classification. Brain 2021, 145, 897–908. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-K.; Chu, P.-C.; Chai, W.-Y.; Kang, S.-T.; Tsai, C.-H.; Fan, C.-H.; Yeh, C.-K.; Liu, H.-L. Characterization of Different Microbubbles in Assisting Focused Ultrasound-Induced Blood-Brain Barrier Opening. Sci. Rep. 2017, 7, 46689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subramaniam, R.M. Science to Practice: Molecular Targeting with SPECT/CT and MR Imaging in Oncology—Integration of Functional and Structural Imaging. Radiology 2013, 267, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, V.M.; Urroz, P.D.; Bajc, M.; Rutherford, N.; Brooker, B.; Gibson, P.G. Imaging for Precision Medicine: Can V-P Spect Measure Mepolizumab Response in Asthma? Respirol. Case Rep. 2021, 9, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Ljungberg, M.; Sjögreen Gleisner, K. Personalized Dosimetry for Radionuclide Therapy Using Molecular Imaging Tools. Biomedicines 2016, 4, 25. [Google Scholar] [CrossRef] [Green Version]
- Gardiazabal, J.; Esposito, M.; Matthies, P.; Okur, A.; Vogel, J.; Kraft, S.; Frisch, B.; Lasser, T.; Navab, N. Towards Personalized Interventional SPECT-CT Imaging. Med. Image Comput. Comput. Assist. Interv. MICCAI 2014, 17, 504–511. [Google Scholar]
- Delbeke, D.; Schöder, H.; Martin, W.H.; Wahl, R.L. Hybrid Imaging (SPECT/CT and PET/CT): Improving Therapeutic Decisions. Semin. Nucl. Med. 2009, 39, 308–340. [Google Scholar] [CrossRef] [PubMed]
- Kao, Y.H.; Magsombol, B.M.; Toh, Y.; Tay, K.H.; Chow, P.K.H.; Goh, A.S.W.; Ng, D.C.E. Personalized Predictive Lung Dosimetry by Technetium-99m Macroaggregated Albumin SPECT/CT for Yttrium-90 Radioembolization. EJNMMI Res. 2014, 4, 33–45. [Google Scholar] [CrossRef] [Green Version]
- Khalil, M.M.; Tremoleda, J.L.; Bayomy, T.B.; Gsell, W. Molecular SPECT Imaging: An Overview. Int. J. Mol. Imaging 2011, 2011, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Ahn, B.-C. Personalized Medicine Based on Theranostic Radioiodine Molecular Imaging for Differentiated Thyroid Cancer. BioMed Res. Int. 2016, 2016, 1680464. [Google Scholar] [CrossRef] [Green Version]
- Ahn, B.-C. Nuclear Medicine in the Era of Precision Medicine. Nucl. Med. Mol. Imaging 2017, 51, 99–100. [Google Scholar] [CrossRef] [Green Version]
- Baum, R.P.; Kulkarni, H.R. Theranostics: From Molecular Imaging Using GA-68 Labeled Tracers and PET/CT to Personalized Radionuclide Therapy—The Bad Berka Experience. Theranostics 2012, 2, 437–447. [Google Scholar] [CrossRef] [Green Version]
- Urbano, N.; Scimeca, M.; Bonanno, E.; Schillaci, O. Nuclear Medicine and Anatomic Pathology in Personalized Medicine: A Challenging Alliance. Pers. Med. 2018, 15, 457–459. [Google Scholar] [CrossRef] [PubMed]
- Nutt, R.; Vento, L.J.; Ridinger, M.H. In Vivo Molecular Imaging Biomarkers: Clinical Pharmacology’s New “Pet”? Clin. Pharmacol. Ther. 2007, 81, 792–795. [Google Scholar] [CrossRef]
- Dimitrakopoulou-Strauss, A. PET-Based Molecular Imaging in Personalized Oncology: Potential of the Assessment of Therapeutic Outcome. Future Oncol. 2015, 11, 1083–1091. [Google Scholar] [CrossRef]
- Carrete, L.R.; Young, J.S.; Cha, S. Advanced Imaging Techniques for Newly Diagnosed and Recurrent Gliomas. Front. Neurosci. 2022, 16, 1–22. [Google Scholar] [CrossRef] [PubMed]
- van Rijsewijk, N.D.; IJpma, F.F.A.; Wouthuyzen-Bakker, M.; Glaudemans, A.W.J.M. Molecular Imaging of Fever of Unknown Origin: An Update. Semin. Nucl. Med. 2023, 53, 4–17. [Google Scholar] [CrossRef] [PubMed]
- Petersen, A.L.; Hansen, A.E.; Gabizon, A.; Andresen, T.L. Liposome Imaging Agents in Personalized Medicine. Adv. Drug Deliv. Rev. 2012, 64, 1417–1435. [Google Scholar] [CrossRef]
- Alsaab, H.O.; Al-Hibs, A.S.; Alzhrani, R.; Alrabighi, K.K.; Alqathama, A.; Alwithenani, A.; Almalki, A.H.; Althobaiti, Y.S. Nanomaterials for Antiangiogenic Therapies for Cancer: A Promising Tool for Personalized Medicine. Int. J. Mol. Sci. 2021, 22, 1631. [Google Scholar] [CrossRef]
- Holland, J.P. The Role of Molecular Imaging in Personalised Healthcare. CHIMIA 2016, 70, 787–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaz, S.C.; Oliveira, F.; Herrmann, K.; Veit-Haibach, P. Nuclear Medicine and Molecular Imaging Advances in the 21st Century. Br. J. Radiol. 2020, 93, 1–12. [Google Scholar] [CrossRef]
- Hamada, K.; Myoui, A.; Ueda, T.; Higuchi, I.; Inoue, A.; Tamai, N.; Yoshikawa, H.; Hatazawa, J. FDG-PET Imaging for Chronic Expanding Hematoma in Pelvis with Massive Bone Destruction. Skelet. Radiol. 2005, 34, 807–811. [Google Scholar] [CrossRef]
- Levin, D.; Lantsberg, S.; Giladi, M.R.; Kazap, D.E.; Hod, N. Post Contusion Breast Hematoma Mimicking Malignancy on FDG PET/CT. Clin. Nucl. Med. 2020, 45, 552–554. [Google Scholar] [CrossRef]
- Tokue, H.; Tokue, A.; Okauchi, K.; Tsushima, Y. 2-[18 f]Fluoro-2-Deoxy-d-Glucose (FDG) Positron-Emission Tomography (PET) Findings of Chronic Expanding Intrapericardial Hematoma: A Potential Interpretive Pitfall That Mimics a Malignant Tumor. J. Cardiothorac. Surg. 2013, 8, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Achenbach, S.; Fuchs, F.; Goncalves, A.; Kaiser-Albers, C.; Ali, Z.A.; Bengel, F.M.; Dimmeler, S.; Fayad, Z.A.; Mebazaa, A.; Meder, B.; et al. Non-Invasive Imaging as the Cornerstone of Cardiovascular Precision Medicine. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 465–475. [Google Scholar] [CrossRef]
- Sriranjan, R.S.; Tarkin, J.M.; Evans, N.R.; Le, E.P.V.; Chowdhury, M.M.; Rudd, J.H.F. Atherosclerosis Imaging Using PET: Insights and Applications. Br. J. Pharmacol. 2019, 178, 2186–2203. [Google Scholar] [CrossRef]
- Cook, G.J.R.; Goh, V. A Role for FDG Pet Radiomics in Personalized Medicine? Semin. Nucl. Med. 2020, 50, 532–540. [Google Scholar] [CrossRef] [PubMed]
- Peñuelas, I.; Domínguez-Prado, I.; García-Velloso, M.J.; Martí-Climent, J.M.; Rodríguez-Fraile, M.; Caicedo, C.; Sánchez-Martínez, M.; Richter, J.A. Pet Tracers for Clinical Imaging of Breast Cancer. J. Oncol. 2012, 2012, 710561. [Google Scholar] [CrossRef] [PubMed]
- Bao, W.; Xie, F.; Zuo, C.; Guan, Y.; Huang, Y.H. Pet Neuroimaging of Alzheimer’s Disease: Radiotracers and Their Utility in Clinical Research. Front. Aging Neurosci. 2021, 13, 1–22. [Google Scholar] [CrossRef]
- Tiepolt, S.; Patt, M.; Aghakhanyan, G.; Meyer, P.M.; Hesse, S.; Barthel, H.; Sabri, O. Current Radiotracers to Image Neurodegenerative Diseases. EJNMMI Radiopharm. Chem. 2019, 4, 2–23. [Google Scholar] [CrossRef] [Green Version]
- Schillaci, O.; Scimeca, M.; Trivigno, D.; Chiaravalloti, A.; Facchetti, S.; Anemona, L.; Bonfiglio, R.; Santeusanio, G.; Tancredi, V.; Bonanno, E.; et al. Prostate Cancer and Inflammation: A New Molecular Imaging Challenge in the Era of Personalized Medicine. Nucl. Med. Biol. 2019, 68, 66–79. [Google Scholar] [CrossRef] [PubMed]
- Marciscano, A.E.; Thorek, D.L.J. Role of Noninvasive Molecular Imaging in Determining Response. Adv. Radiat. Oncol. 2018, 3, 534–547. [Google Scholar] [CrossRef] [Green Version]
- Kiessling, F.; Fokong, S.; Bzyl, J.; Lederle, W.; Palmowski, M.; Lammers, T. Recent Advances in Molecular, Multimodal and Theranostic Ultrasound Imaging. Adv. Drug Deliv. Rev. 2014, 72, 15–27. [Google Scholar] [CrossRef] [Green Version]
- Massoud, T.F.; Gambhir, S.S. Integrating Noninvasive Molecular Imaging into Molecular Medicine: An Evolving Paradigm. Trends Mol. Med. 2007, 13, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Fathinul Fikri, A.S. Molecular Imaging—A Way Forward in Translating Disease Behaviour in an Era of Personalized Medicine. J. Int. Med. Res. 2017, 46, 652–653. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.M.; Jeong, Y.J.; Kim, H.W.; Ahn, B.-C. KSNM60 In Nuclear Endocrinology: From the Beginning to the Future. Nucl. Med. Mol. Imaging 2022, 56, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Schillaci, O.; Urbano, N. Digital Pet/CT: A New Intriguing Chance for Clinical Nuclear Medicine and Personalized Molecular Imaging. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1222–1225. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Trademark Name | Shell Material | Gas | Diameter in Volume (μm) | Microbubbles Volume Concentration (Bubbles/mL) | Recommended Dose (μm) | Application (Example) | Side Effects/Contraindications | References |
|---|---|---|---|---|---|---|---|---|
| Albunex | Sonicated serum albumin | Air | 4.0 | 437 million/mL | 0.033 to 0.5 mL/kg | Transpulmonary imaging, myocardial contrast echocardiography | Significantly increase thrombolysis with thrombolytics | [32,33,34] |
| Optison | Cross-linked serum albumin | Octafluropropane/Perflutren/Perfluoropentane | 7.11 ± 0.24 | 0.078 ± 0.017 (×108 mb/mL) | 0.5 mL | Left ventricle opacification, endocardial | Hypersensitivity to perflutren, blood, blood products or albumin | [32,33,35,36,37] |
| Definity/Luminity | Phospholipids/DPPA/DPPC/MPEG5000 DPPE | Perfluoropropane/Octafluropropane/Perflutren | 8.19 ± 0.77 | 0.143 ± 0.042 (×108 mb/mL) | 10 Ul kg−1 | Echocardiography, liver and kidney imaging | Hypersensitivity to perflutren | [32,35,37,38] |
| Sonazoid | Hydrogenated egg yolk phosphatidyl serine (HEPS)/Phospholipid | Perfluoropropane | 2.6 ± 0.1 | 1.27 × 109 ppml | 0.015 to 0.2 mL/kg | Myocardial perfusion, liver imaging, focal breast lesion | Diarrhea, albuminuria and neutropenia/Iodine Allergy and renal dysfunction | [32,33,38,39,40,41] |
| Lumason/SonoVue | Phospholipid/DPSC, DPPG-Na, palmitic acid | Sulphur hexafluoride | 8.01 ± 0.85 | 0.022 ± 0.006(×108 mb/mL) | 4 × 107 (bubbles/kg) | Left ventricle opacification, microvascular enhancement (liver, and breast lesion detection) | Hypersensitivity to sulphur hexafluoride or any inactive ingredient | [28,32,37,38] |
| Perfluorocarbon-exposed sonicated dextrose albumin (PESDA) | Dextrose albumin | Perfluorobutane | - | 1.05 × 109 mb/mL | 2.5–10 (μL kg−1) | Carotid artery restenosis, Carotid intimal hyperplasia, liver, pulmonary | Thrombolysis | [35,42,43,44] |
| Radiopharmaceutical | Modality | Clinical Applications | References |
|---|---|---|---|
| 201TI chloride | SPECT | Brain tumors | [67] |
| 99mTc-tetrofosmin | SPECT | Brain tumors | [68] |
| 111In-DTPA-octreotide46 | SPECT | Brain tumors, cerebrospinal fluid kinetics | [67] |
| 99mTc-sulfur colloid | SPECT/CT | Splenosis, sentinel lymph node metastasis/biopsy | [52,67] |
| 123I-iodine | SPECT/CT and SPECT | Neuroendocrine tumors | [52,67] |
| 99mTc-sestamibi | SPECT/CT and SPECT | Breast cancer, lymph node metastasis | [52,67] |
| 99mTc-diphosphonates | SPECT/CT and SPECT | Bone detection | [67,68] |
| 99mTc-red blood cells | SPECT/CT and SPECT | Gastrointestinal bleeding and associated disorders: splenosis | [52,67] |
| 99mTc MAA | SPECT/CT | Liver and lung pulmonary perfusion | [68] |
| 99m Tc-N4-NIM | SPECT | Hypoxic | [47] |
| 125 I-IPOS | SPECT | Hypoxic | [47] |
| 99mTc-lablled | SPECT | Cardiac | [69] |
| 111 In-oxyquinoline | SPECT | Stem cells visualize binding sites in receptor-expressing neuroendocrine tumors | [17,69] |
| I-131 | SPECT/CT | Thyroid | [70] |
| Diseases/Disorders | Image Technique | Radiotracers | Applications | References |
|---|---|---|---|---|
| Pencentric Cancer | PET | [18F]-fluorodeoxyglucose (FDG) | Diagnosis, post-therapy monitoring | [7] |
| Prostate Cancer | PET, choline PET/CT, PET/MRI | [18F]-fluorodeoxyglucose [18F]-FDG [11C]-acetate 3′-Deoxy-3′-[18F]-Fluorothymidine (FLT) [18F]-2′-Fluoro-5-Methyl-1-β-D-Arabinofuranosyluracil (FMAU) | First-line diagnostic and staging procedure, guide biopsies and for planning of focal therapy, lymph node and bone metastases, evaluate therapy | [11,21,50,59,76,80,81] |
| Hematoma | PET, PET/CT | 2-Deoxy-[18F]-fluoro-D: -glucose (FDG) | Detect the presence of hematoma associated with a malignant lesion, identify the hematoma that mimics a malignant tumor | [82,83,84] |
| Hypoxia | PET | [18F]-fluoromisonidazole (FMISO) [18F]fluoroazomycin-arabinofuranoside [60/64Cu]-copper(II)-diacetyl-bis(N4-methy- lthiosemicarbazone (ATSM) | Quantify chronic tissue hypoxia, calculate tumor HV and the maximum level of hypoxia, useful in radiotherapy metabolic planning, guiding the use of chemotherapeutic drugs | [58,59,83] |
| Glioma | PET | [18F]-fluorodeoxyglucose [18F]-FDG [11C]-methionine (MET) Fluorodeoxyglucose (FDG) Amnio Acid (AA) | Tumor recurrence detection and radiation necrosis, therapy monitoring, safe resection of glioma, identifying areas of infiltrating glioma, help optimize image-guided biopsy, radiotherapy planning | [21,76,77] |
| Cardiac | PET, PET/MRI, PET/CT | [18F]-fluorodeoxyglucose [18F]-FDG [18F]-sodium fluoride [18F]-NaF | Assess cardiac diseases: ischaemia detection and quantification, coronary calcification, and myocardial inflammation. Atherosclerosis detects endocarditis, infection of cardiac devices, and metastatic measures of inflammation in the vessel wall and myocardium injury, and monitor the therapeutic effect | [23,81,85,86] |
| Hodgkin’s Lymphoma | PET, PET/CT or PET/MR | [18F]-fluorodeoxyglucose [18F]-FDG | Staging and recurrence detection, evaluating the treatment response, assessment of a variety of types of lymphomas, sarcomas, and blastomas | [9,12,59] |
| Bone Cancer (Sarcoma) | PET, PET/CT | [18F]-fluorodeoxyglucose [18F]-FDG | Detect bone/bone marrow metastases, predict the therapy response | [75] |
| Fever of Unknown Region (FUO) | PET/CT | [18F]-fluorodeoxyglucose [18F]-FDG | Investigation and management in children with FUO guide the therapy drugs | [77] |
| RENAL MASS | PET, PET/CT | [124I]-girentuximab | Utilized for renal mass characterization, identification of ccRCC | [12] |
| Lung Cancer (NSCLC) | PET, PET/CT | [18F]-fluorodeoxyglucose [18F]-FDG | checkpoint blockade immuno- therapy, predict immunotherapy toxicity, mutational status, and metastases, guide decisions during therapy | [87] |
| BREAST CANCER | PET, PET/CT | fluorodeoxyglucose (FDG) 3′-Deoxy-3′-[18F]-Fluorothymidine (18FLT) | Staging, monitoring, and prediction of response to therapy agents | [80,88] |
| Alzheimer’s Disease (AD) | PET | [18F]-fluorodeoxyglucose [18F]-FDG N-[(2-[11C]-methoxyphenyl)methyl]-N-(6-phenoxypyridin-3-yl)acetamide-[11C]-PBR-28 [N,N-diethyl-2-(2-(4-(2[18F]fluoroethoxy)phenyl)5,7dimethylpyrazolo[1,5a]pyrimidin-3- yl)acetamide] [18F]-DPA-714 | Early detection and treatment monitoring to expand our knowledge about the AD of different phenotypically | [83,84] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salih, S.; Elliyanti, A.; Alkatheeri, A.; AlYafei, F.; Almarri, B.; Khan, H. The Role of Molecular Imaging in Personalized Medicine. J. Pers. Med. 2023, 13, 369. https://doi.org/10.3390/jpm13020369
Salih S, Elliyanti A, Alkatheeri A, AlYafei F, Almarri B, Khan H. The Role of Molecular Imaging in Personalized Medicine. Journal of Personalized Medicine. 2023; 13(2):369. https://doi.org/10.3390/jpm13020369
Chicago/Turabian StyleSalih, Suliman, Aisyah Elliyanti, Ajnas Alkatheeri, Fatima AlYafei, Bashayer Almarri, and Hasina Khan. 2023. "The Role of Molecular Imaging in Personalized Medicine" Journal of Personalized Medicine 13, no. 2: 369. https://doi.org/10.3390/jpm13020369