
Current Situation of Diagnosis and Treatment of HER2-Positive Metastatic Breast Cancer Patients in China: A Nationwide Cross-Sectional Survey of Doctors
 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
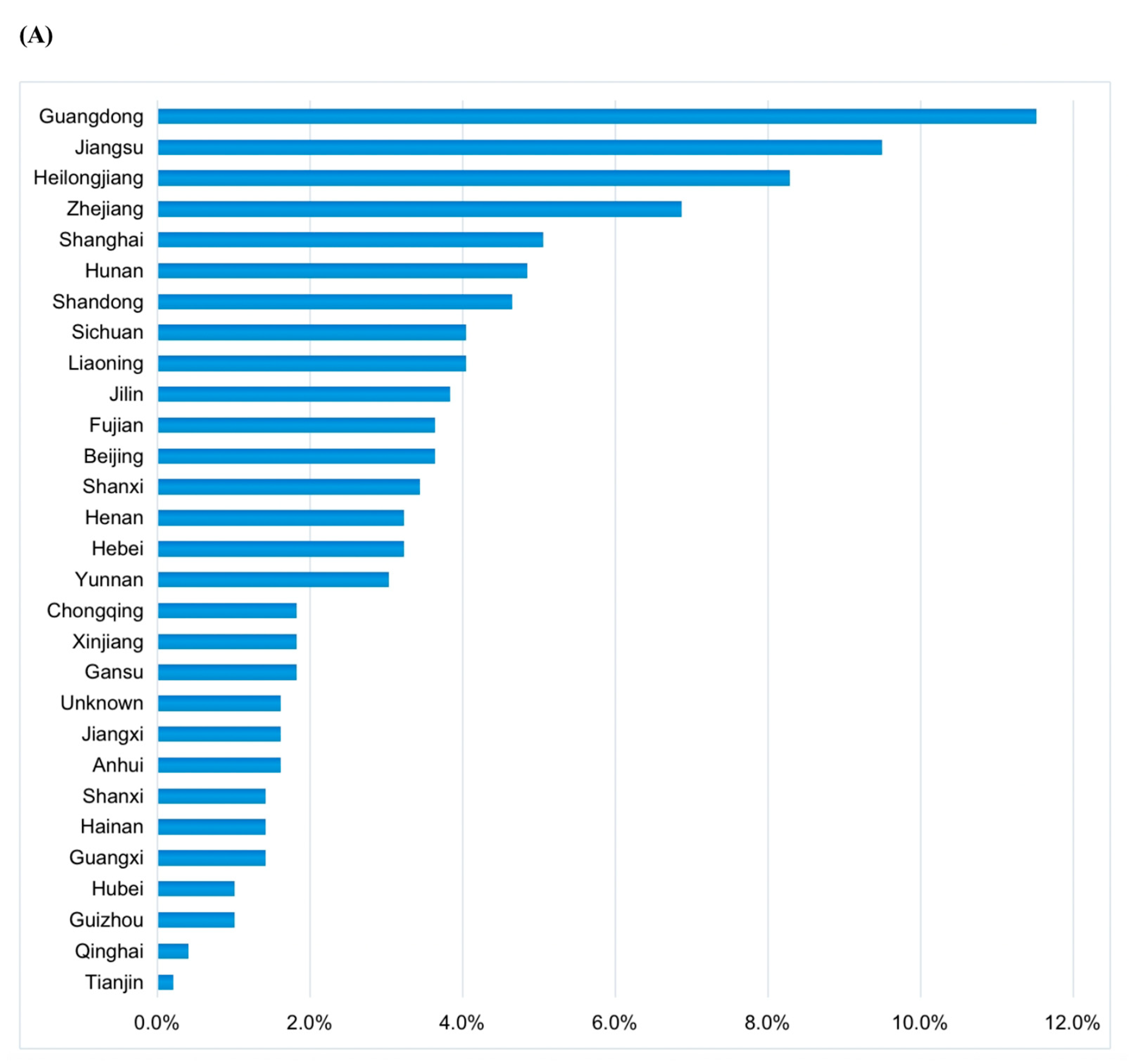
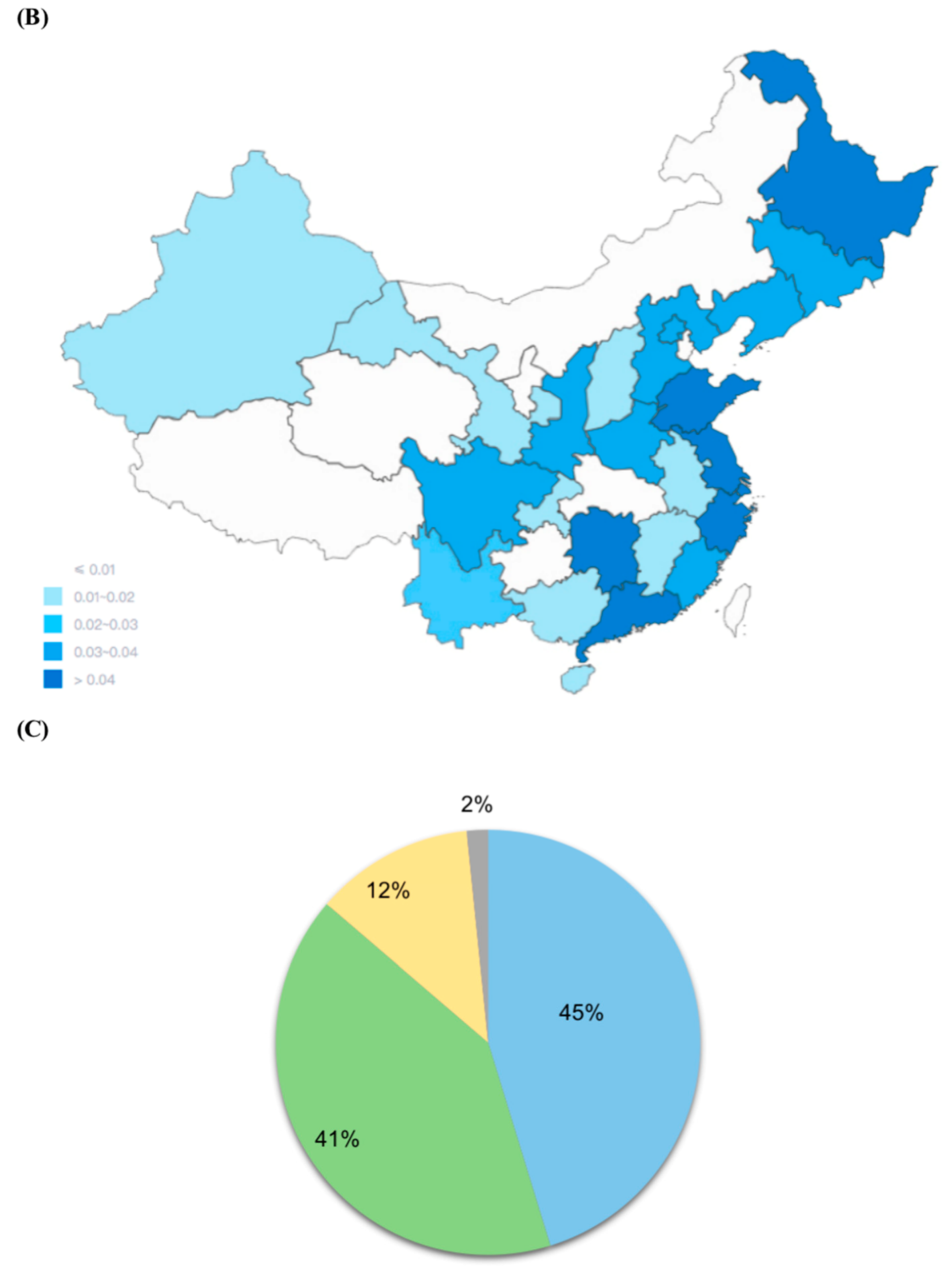
3.1. The Characteristics of Study Population
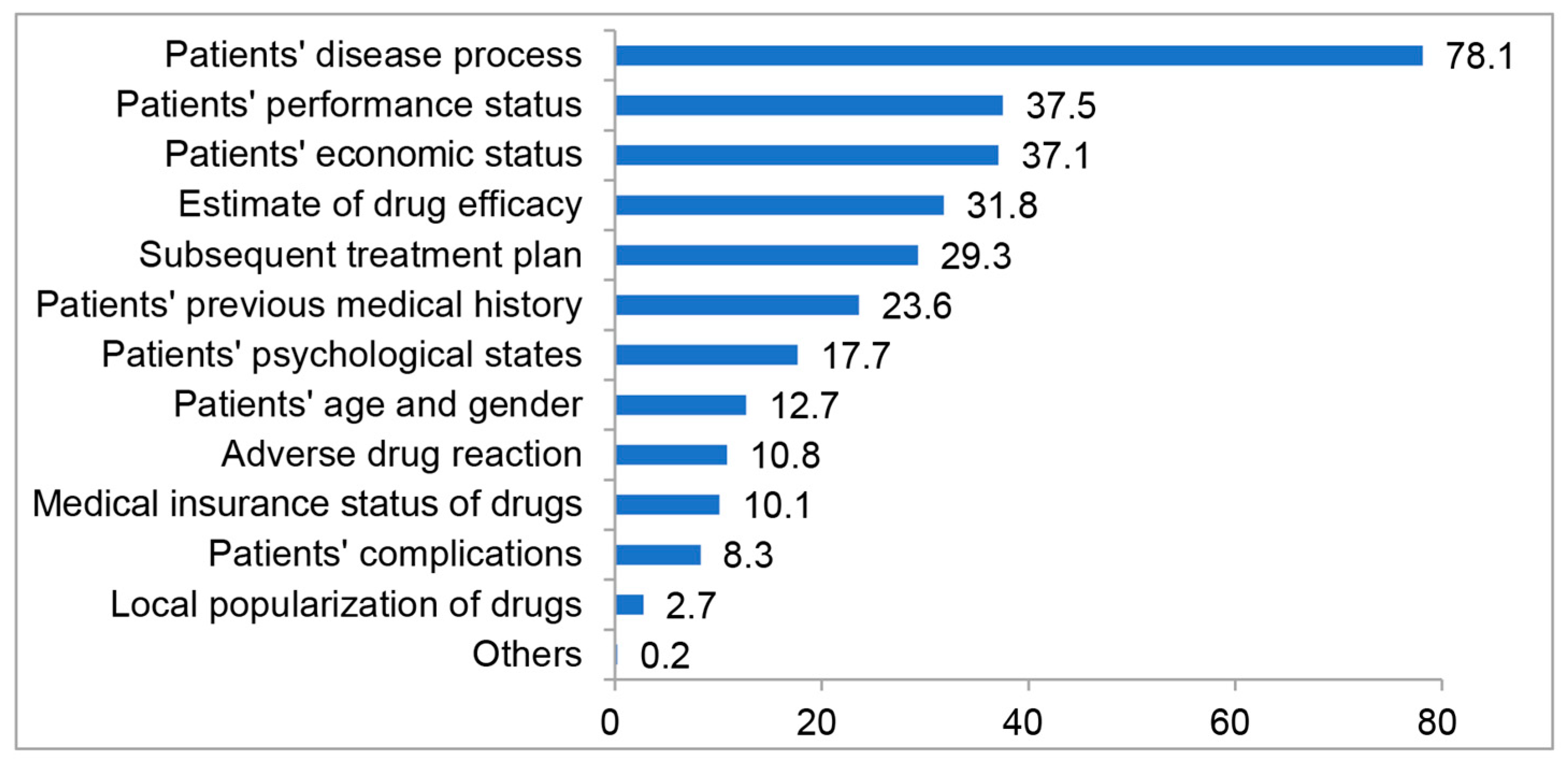
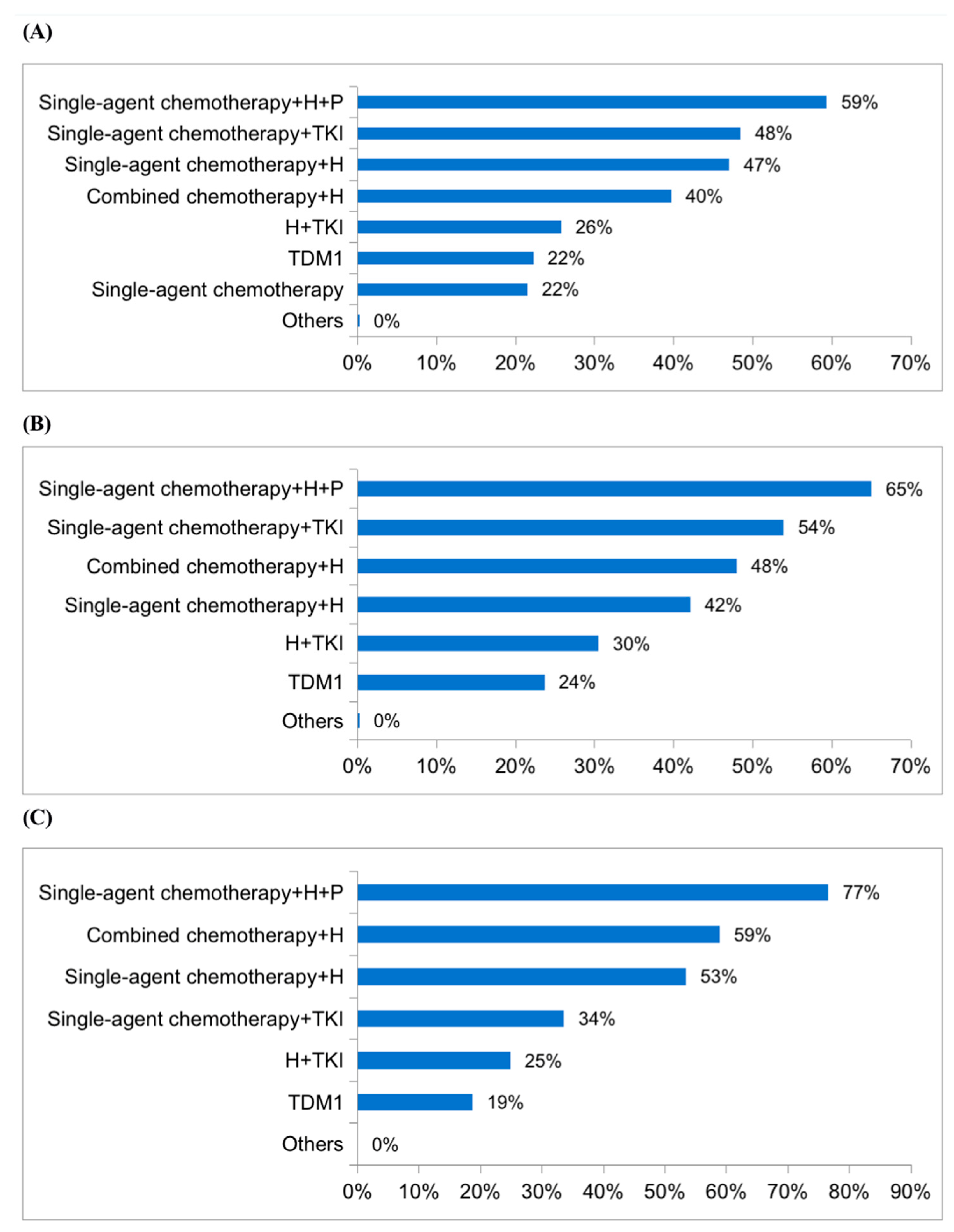
3.2. Doctors’ Perceptions and Choices in China
3.3. The Effect of the Economic Factors
3.4. Difference between First-Tier and Second-Tier or Other Cities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries, 2021. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Sun, K.; Zheng, R.; Zeng, H.; Zhang, S.; Xia, C.; Yang, Z.; Li, H.; Zou, X.; He, J. Cancer incidence and mortality in China, 2014. Chin. J. Cancer Res. 2018, 30, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Waks, A.G.; Winer, E.P. Breast Cancer Treatment: A Review. JAMA 2019, 321, 288–300. [Google Scholar] [CrossRef] [PubMed]
- Halim, A.; Ashraf, A.; Andrew, A.; Yasin, M.; Rahman, M.; Jusoh, M.; Veeraperumal, V.; Rahim, H.; Illahi, U.; Karim, M.; et al. Existing and Emerging Breast Cancer Detection Technologies and Its Challenges: A Review. Appl. Sci. 2021, 11, 10753. [Google Scholar] [CrossRef]
- Huober, J.; Thürlimann, B. The Role of Combination Chemotherapy in the Treatment of Patients with Metastatic Breast Cancer. Breast Care 2009, 4, 367–372. [Google Scholar] [CrossRef] [Green Version]
- Sorlie, T.; Tibshirani, R.; Parker, J.; Hastie, T.; Marron, J.S.; Nobel, A.; Deng, S.; Johnsen, H.; Pesich, R.; Geisler, S.; et al. Repeated observation of breast tumor subtypes in independent gene expression data sets. Proc. Natl. Acad. Sci. USA 2003, 100, 8418–8423. [Google Scholar] [CrossRef] [Green Version]
- Abrams, H.R.; Durbin, S.; Huang, C.X.; Johnson, S.F.; Nayak, R.K.; Zahner, G.J.; Peppercorn, J. Financial toxicity in cancer care: Origins, impact, and solutions. Transl. Behav. Med. 2021, 11, 2043–2054. [Google Scholar] [CrossRef]
- Sedhom, R.; Chino, F.; Gupta, A. Financial Toxicity and Cancer Care. J. Palliat. Med. 2021, 24, 453–454. [Google Scholar] [CrossRef]
- Carrera, P.M.; Kantarjian, H.M.; Blinder, V.S. The Financial Burden and Distress of Patients With Cancer: Understanding and Stepping-Up Action on the Financial Toxicity of Cancer Treatment. CA Cancer J. Clin. 2018, 68, 153–165. [Google Scholar] [CrossRef]
- Perrone, F.; Jommi, C.; Maio, M.D.; Gimigliano, A.; Gridelli, C.; Pignata, S.; Ciardiello, F.; Nuzzo, F.; de Matteis, A.; Del Mastro, L.; et al. The association of financial difficulties with clinical outcomes in cancer patients: Secondary analysis of 16 academic prospective clinical trials conducted in Italy. Ann. Oncol. 2016, 27, 2224–2229. [Google Scholar] [CrossRef]
- Zhang, Y. An analysis of the spillover effect of the output of commercial circulation in first-tier cities to second-tier cities in China. Commer. Times 2018, 751, 158–160. [Google Scholar]
- Blumen, H.; Fitch, K.; Polkus, V. Comparison of Treatment Costs for Breast Cancer, by Tumor Stage and Type of Service. Am. Health Drug Benefits 2016, 9, 23–32. [Google Scholar]
- Diaby, V.; Tawk, R.; Sanogo, V.; Xiao, H.; Montero, A.J. A review of systematic reviews of the cost-effectiveness of hormone therapy, chemotherapy, and targeted therapy for breast cancer. Breast Cancer Res. Treat. 2015, 151, 27–40. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, R.; Peppercorn, J.; Sikora, K.; Zalcberg, J.; Meropol, N.J.; Amir, E.; Khayat, D.; Boyle, P.; Autier, P.; Tannock, I.F.; et al. Delivering affordable cancer care in high-income countries. Lancet Oncol. 2011, 12, 933–980. [Google Scholar] [CrossRef] [PubMed]
- Rashidian, A.; Barfar, E.; Hosseini, H.; Nosratnejad, S.; Barooti, E. Cost Effectiveness of Breast Cancer Screening Using Mammography; a Systematic Review. Iran J. Public Health 2013, 42, 347–357. [Google Scholar] [PubMed]
- Geuzinge, H.A.; Obdeijn, I.M.; Rutgers, E.J.T.; Saadatmand, S.; Mann, R.M.; Oosterwijk, J.C.; Tollenaar, R.A.E.M.; de Roy van Zuidewijn, D.B.W.; Lobbes, M.B.I.; van ’t Riet, M.; et al. Cost-effectiveness of Breast Cancer Screening With Magnetic Resonance Imaging for Women at Familial Risk. JAMA Oncol. 2020, 6, 1381–1389. [Google Scholar] [CrossRef]
- Leung, J.H.; Tai, Y.S.; Wang, S.Y.; Yip Fion, H.T.; Tsung-Chin, H.; Chan, A.L. Cost-effectiveness of trastuzumab biosimilar combination therapy and drug wastage as first-line treatment for HER2-positive metastatic breast cancer. Breast 2022, 65, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Dreyer, M.S.; Nattinger, A.B.; McGinley, E.L.; Pezzin, L.E. Socioeconomic status and breast cancer treatment. Breast Cancer Res. Treat. 2018, 167, 1–8. [Google Scholar] [CrossRef]
- Huang, H.Y.; Shi, J.F.; Guo, L.W.; Zhu, X.Y.; Wang, L.; Liao, X.Z.; Liu, G.X.; Bai, Y.N.; Mao, A.Y.; Ren, J.S. Expenditure and financial burden for common cancers in China: A hospital-based multicentre cross-sectional study. Lancet 2016, 388, S10. [Google Scholar] [CrossRef]
- Su, M.; Lao, J.; Zhang, N.; Wang, J.; Anderson, R.T.; Sun, X.; Yao, N. Financial hardship in Chinese cancer survivors. Cancer 2020, 126, 3312–3321. [Google Scholar] [CrossRef]
- Baselga, J.; Bradbury, I.; Eidtmann, H.; Di Cosimo, S.; de Azambuja, E.; Aura, C.; Gómez, H.; Dinh, P.; Fauria, K.; Van Dooren, V.; et al. Lapatinib with trastuzumab for HER2-positive early breast cancer (NeoALTTO): A randomised, open-label, multicentre, phase 3 trial. Lancet 2012, 379, 633–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pernas, S.; Barroso-Sousa, R.; Tolaney, S.M. Optimal treatment of early stage HER2-positive breast cancer. Cancer 2018, 124, 4455–4466. [Google Scholar] [CrossRef] [Green Version]
- Guarneri, V.; Griguolo, G.; Miglietta, F.; Conte, P.F.; Dieci, M.V.; Girardi, F. Survival after neoadjuvant therapy with trastuzumab-lapatinib and chemotherapy in patients with HER2-positive early breast cancer: A meta-analysis of randomized trials. ESMO Open 2022, 7, 100433. [Google Scholar] [CrossRef]
- Wu, J.; Jiang, Z.F.; Liu, Z.Z.; Yang, B.; Yang, H.; Tang, J.; Wang, K.; Liu, Y.; Wang, H.; Fu, P.; et al. Neoadjuvant pyrotinib, trastuzumab, and docetaxel for HER2-positive breast cancer (PHEDRA): A double-blind, randomized phase 3 trial. BMC Med. 2022, 20, 498. [Google Scholar] [CrossRef] [PubMed]
- Yin, W.J.; Wang, Y.H.; Wu, Z.P.; Ye, Y.; Zhou, L.; Xu, S.; Lin, Y.; Du, Y.; Yan, T.; Yang, F.; et al. Neoadjuvant Trastuzumab and Pyrotinib for Locally Advanced HER2-Positive Breast Cancer (NeoATP): Primary Analysis of a Phase II Study. Clin. Cancer Res. 2022, 28, 3677–3685. [Google Scholar] [CrossRef]
- Piccartgebhart, M.; Holmes, E.; Baselga, J.; de Azambuja, E.; Dueck, A.C.; Viale, G.; Zujewski, J.A.; Goldhirsch, A.; Armour, A.; Pritchard, K.I.; et al. Adjuvant Lapatinib and Trastuzumab for Early Human Epidermal Growth Factor Receptor 2–Positive Breast Cancer: Results From the Randomized Phase III Adjuvant Lapatinib and/or Trastuzumab Treatment Optimization Trial. J. Clin. Oncol. 2016, 34, 1034–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, A.; Delaloge, S.; Holmes, F.A.; Moy, B.; Iwata, H.; Harvey, V.J.; Robert, N.J.; Silovski, T.; Gokmen, E.; von Minckwitz, G.; et al. Neratinib after trastuzumab-based adjuvant therapy in patients with HER2-positive breast cancer (ExteNET): A multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2016, 17, 367–377. [Google Scholar] [CrossRef]
- Brufsky, A.M.; Mayer, M.; Rugo, H.S.; Kaufman, P.A.; Tan-Chiu, E.; Tripathy, D.; Tudor, I.C.; Wang, L.I.; Brammer, M.G.; Shing, M.; et al. Central Nervous System Metastases in Patients with HER2-Positive Metastatic Breast Cancer: Incidence, Treatment, and Survival in Patients from registHER. Clin. Cancer Res. 2011, 17, 4834–4843. [Google Scholar] [CrossRef] [Green Version]
- Lin, N.U.; Pegram, M.; Sahebjam, S.; Ibrahim, N.; Fung, A.; Cheng, A.; Nicholas, A.; Kirschbrown, W.; Kumthekar, P. Pertuzumab Plus High-Dose Trastuzumab in Patients With Progressive Brain Metastases and HER2-Positive Metastatic Breast Cancer: Primary Analysis of a Phase II Study. J. Clin. Oncol. 2021, 39, 2667–2675. [Google Scholar] [CrossRef]
- Krop, I.; Lin, N.; Blackwell, K.; Guardino, E.; Huober, J.; Lu, M.; Miles, D.; Samant, M.; Welslau, M.; Diéras, V. Trastuzumab emtansine (T-DM1) versus lapatinib plus capecitabine in patients with HER2-positive metastatic breast cancer and central nervous system metastases: A retrospective, exploratory analysis in EMILIA. Ann. Oncol. 2014, 26, 113–119. [Google Scholar] [CrossRef]
- Lin, Y.; Lin, M.; Zhang, J.; Wang, B.; Tao, Z.; Du, Y.; Zhang, S.; Cao, J.; Wang, L.; Hu, X. Real-World Data of Pyrotinib-Based Therapy in Metastatic HER2-Positive Breast Cancer: Promising Efficacy in Lapatinib-Treated Patients and in Brain Metastasis. Cancer Res. Treat. 2020, 52, 1059–1066. [Google Scholar] [CrossRef]
- Yan, M.; Ouyang, Q.; Sun, T.; Niu, L.; Yang, J.; Li, L.; Song, Y.; Hao, C.; Chen, Z.; Orlandi, A.; et al. Pyrotinib plus capecitabine for patients with human epidermal growth factor receptor 2-positive breast cancer and brain metastases (PERMEATE): A multicentre, single-arm, two-cohort, phase 2 trial. Lancet Oncol. 2022, 23, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Song, G.; Li, H.; Di, L.; Yan, Y.; Wang, H. Real-world efficacy and safety of oral pyrotinib in HER2 positive metastatic breast cancer. J. Peking Univ. 2020, 52, 254–260. [Google Scholar]
- Jiang, Z.; Yan, M.; Hu, X.; Zhang, Q.; Zhu, X. Pyrotinib combined with capecitabine in women with HER2+ metastatic breast cancer previously treated with trastuzumab and taxanes: A randomized phase III study. J. Clin. Oncol. 2019, 37 (Suppl. S15), 1001. [Google Scholar] [CrossRef]
- Bachelot, T.; Romieu, G.; Campone, M.; Diéras, V.; Cropet, C.; Dalenc, F.; Jimenez, M.; Le Rhun, E.; Pierga, J.Y.; Gonçalves, A.; et al. Lapatinib plus capecitabine in patients with previously untreated brain metastases from HER2-positive metastatic breast cancer (LANDSCAPE): A single-group phase 2 study. Lancet Oncol. 2013, 14, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Montemurro, F.; Ellis, P.; Delaloge, S.; Wuerstlein, R.; Barrios, C. Abstract P1-12-10: Safety and efficacy of trastuzumab emtansine (T-DM1) in 399 patients with central nervous system metastases: Exploratory subgroup analysis from the KAMILLA study. Cancer Res. 2017, 77 (Suppl. S4), P1-12-10. [Google Scholar] [CrossRef]
- Freedman, R.A.; Gelman, R.S.; Anders, C.K.; Melisko, M.E.; Parsons, H.A.; Cropp, A.M.; Silvestri, K.; Cotter, C.M.; Componeschi, K.P.; Marte, J.M.; et al. TBCRC 022: A Phase II Trial of Neratinib and Capecitabine for Patients With Human Epidermal Growth Factor Receptor 2–Positive Breast Cancer and Brain Metastases. J. Clin. Oncol. 2019, 37, 1081–1089. [Google Scholar] [CrossRef]
- Saura, C.; Oliveira, M.; Feng, Y.; Dai, M.S.; Chen, S.W.; Hurvitz, S.A.; Kim, S.B.; Moy, B.; Delaloge, S.; Gradishar, W.; et al. Neratinib Plus Capecitabine Versus Lapatinib Plus Capecitabine in HER2-Positive Metastatic Breast Cancer Previously Treated with ≥2 HER2-Directed Regimens: Phase III NALA Trial. J. Clin. Oncol. 2020, 38, 3138–3149. [Google Scholar] [CrossRef]
- Saura, C.; Garcia-Saenz, J.A.; Xu, B.; Harb, W.; Moroose, R.; Pluard, T.; Cortés, J.; Kiger, C.; Germa, C.; Wang, K.; et al. Safety and Efficacy of Neratinib in Combination With Capecitabine in Patients With Metastatic Human Epidermal Growth Factor Receptor 2-Positive Breast Cancer. J. Clin. Oncol. 2014, 32, 3626–3633. [Google Scholar] [CrossRef]
- Murthy, R.; Borges, V.F.; Conlin, A.; Chaves, J.; Chamberlain, M.; Gray, T.; Vo, A.; Hamilton, E. Tucatinib with capecitabine and trastuzumab in advanced HER2-positive metastatic breast cancer with and without brain metastases: A non-randomised, open-label, phase 1b study. Lancet Oncol. 2018, 19, 880–888. [Google Scholar] [CrossRef]
- Metro, G.; Foglietta, J.; Russillo, M.; Stocchi, L.; Vidiri, A.; Giannarelli, D.; Crinò, L.; Papaldo, P.; Mottolese, M.; Cognetti, F.; et al. Clinical outcome of patients with brain metastases from HER2-positive breast cancer treated with lapatinib and capecitabine. Ann. Oncol. 2011, 22, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Altekruse, S.F.; Li, C.I.; Chen, V.W.; Clarke, C.A.; Ries, L.A.; Cronin, K.A. US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J. Natl. Cancer Inst. 2014, 106, dju055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toriola, A.T.; Colditz, G.A. Trends in breast cancer incidence and mortality in the United States: Implications for prevention. Breast Cancer Res. Treat. 2013, 138, 665–673. [Google Scholar] [CrossRef]
- Bansil, S.; Silva, A.; Taniguchi, A.; Wiedmer, C.; Fernandez, M.; Pagano, I.; Vierkoetter, K.; Killeen, J.; Fukui, J. Racial/Ethnic Differences Among Tumor-Infiltrating Lymphocytes in Breast Cancer Tumors. Oncologist 2023, 28, 116–122. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, K.; Zhou, D.; Hong, R.; Lu, Q.; Xu, F.; Xia, W.; Zheng, Q.; Wang, S. Current Situation of Diagnosis and Treatment of HER2-Positive Metastatic Breast Cancer Patients in China: A Nationwide Cross-Sectional Survey of Doctors. J. Pers. Med. 2023, 13, 365. https://doi.org/10.3390/jpm13020365
Jiang K, Zhou D, Hong R, Lu Q, Xu F, Xia W, Zheng Q, Wang S. Current Situation of Diagnosis and Treatment of HER2-Positive Metastatic Breast Cancer Patients in China: A Nationwide Cross-Sectional Survey of Doctors. Journal of Personalized Medicine. 2023; 13(2):365. https://doi.org/10.3390/jpm13020365
Chicago/Turabian StyleJiang, Kuikui, Danyang Zhou, Ruoxi Hong, Qianyi Lu, Fei Xu, Wen Xia, Qiufan Zheng, and Shusen Wang. 2023. "Current Situation of Diagnosis and Treatment of HER2-Positive Metastatic Breast Cancer Patients in China: A Nationwide Cross-Sectional Survey of Doctors" Journal of Personalized Medicine 13, no. 2: 365. https://doi.org/10.3390/jpm13020365