

Proposal and Validation of a New Nonradiological Method for Postoperative Three-Dimensional Implant Position Analysis Based on the Dynamic Navigation System: An In Vitro Study

Abstract
:1. Introduction
2. Materials and Methods
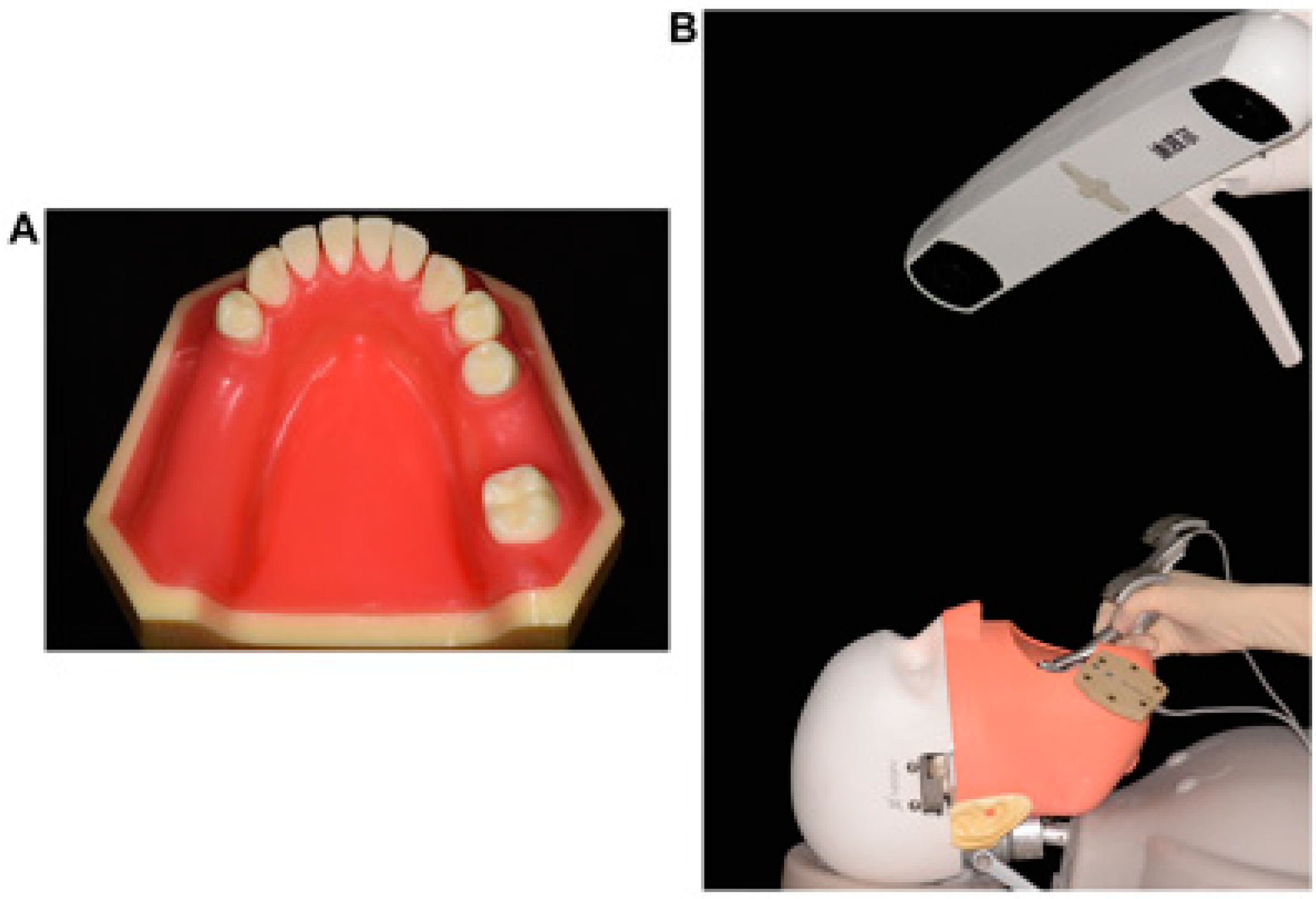
2.1. Study Model
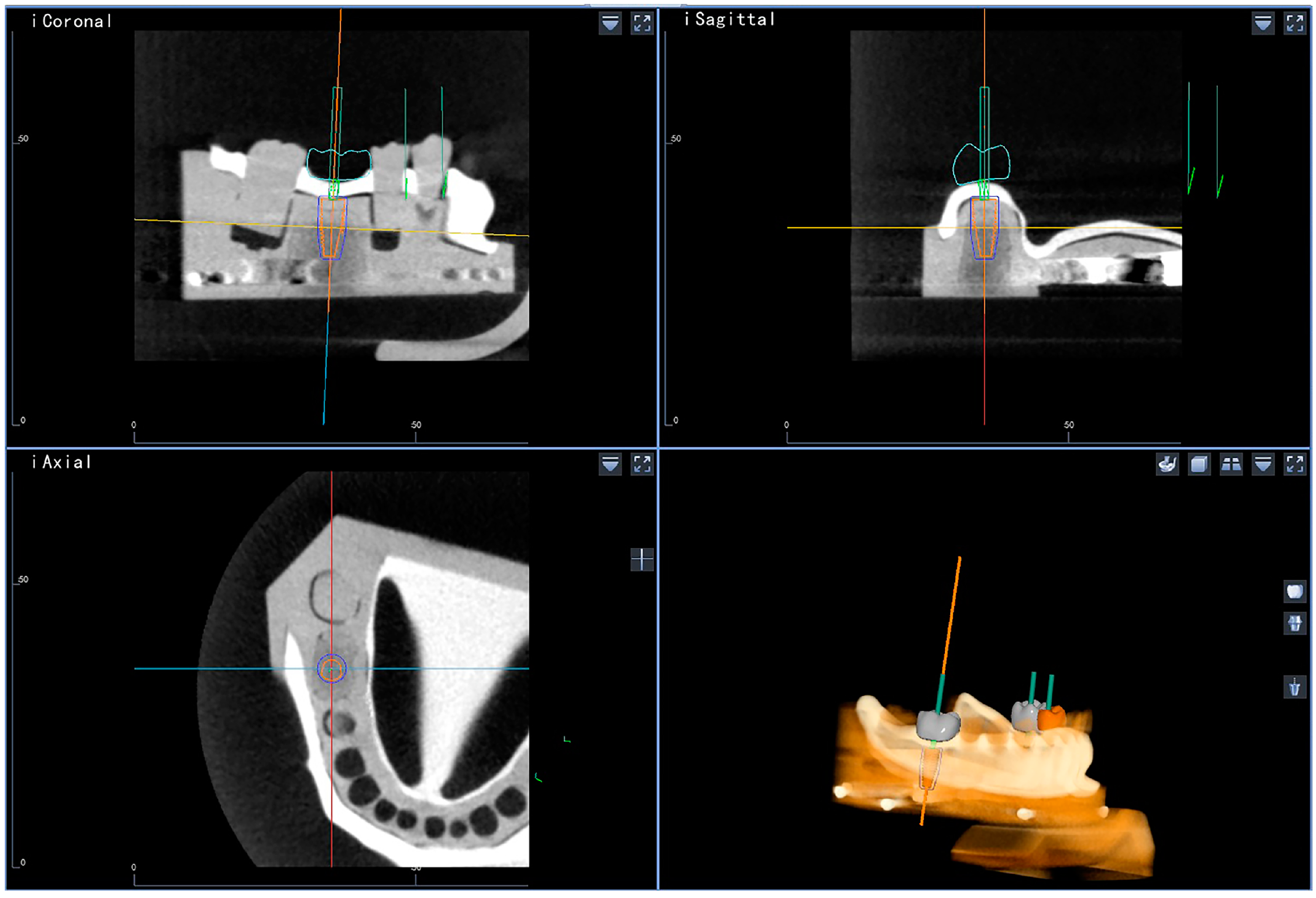
2.2. Digital Planning of Implant Position
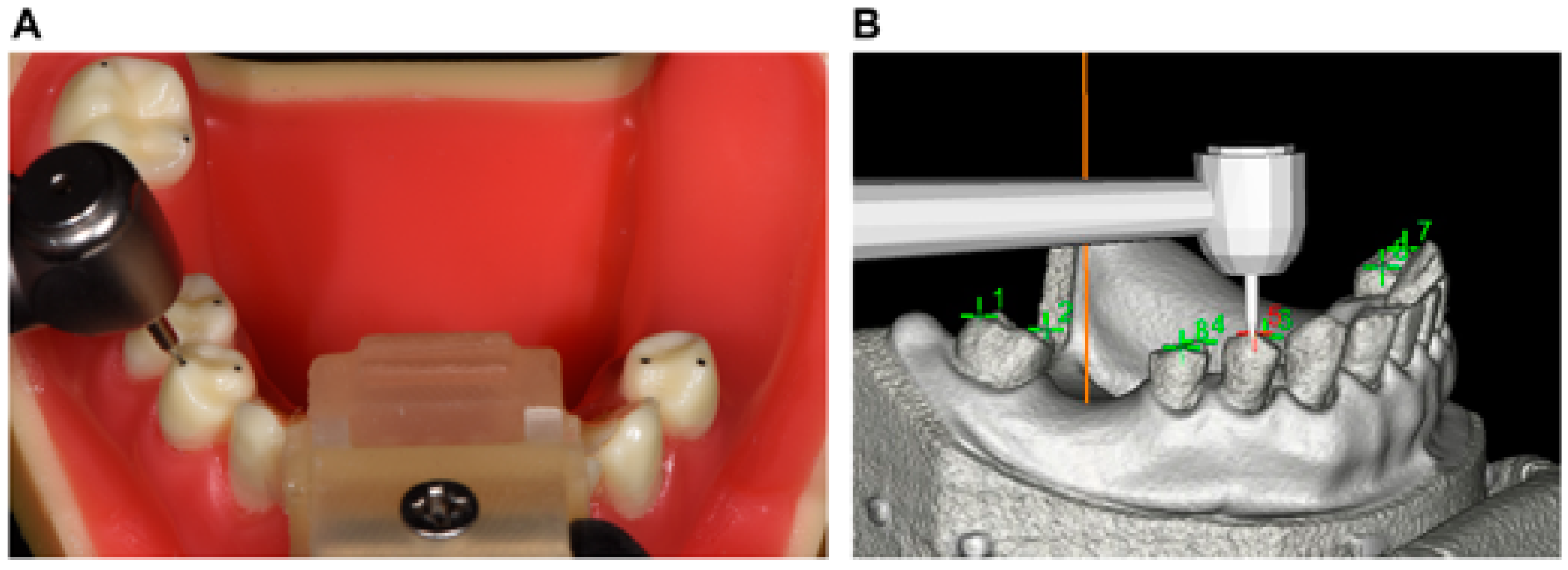
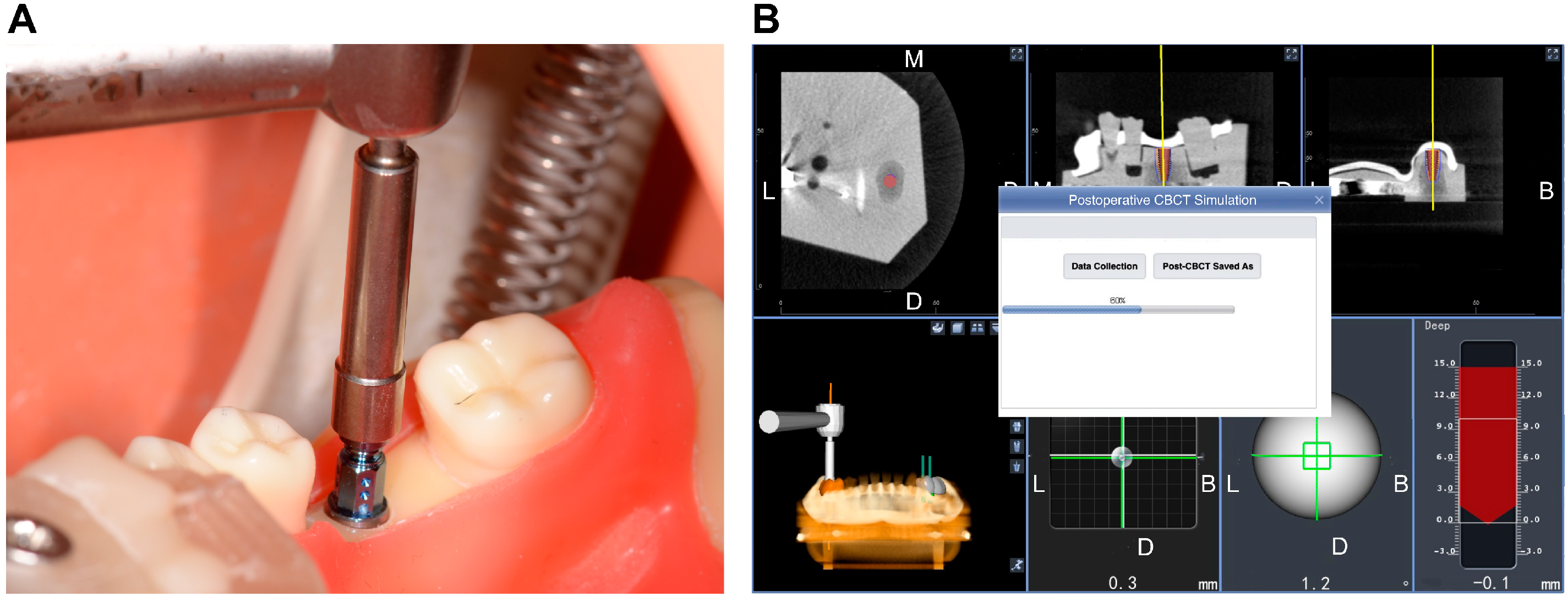
2.3. Experimental Implant Placement
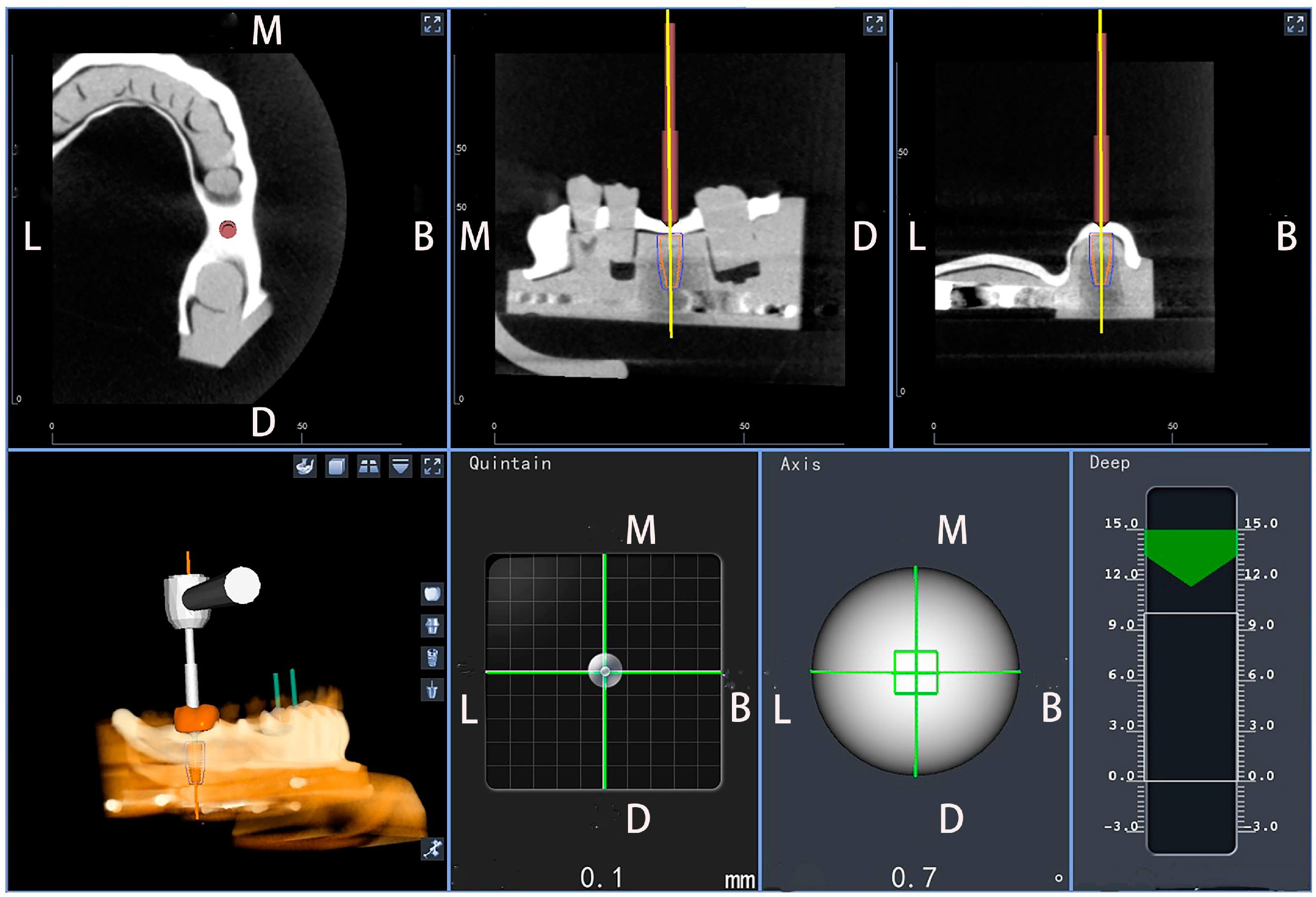
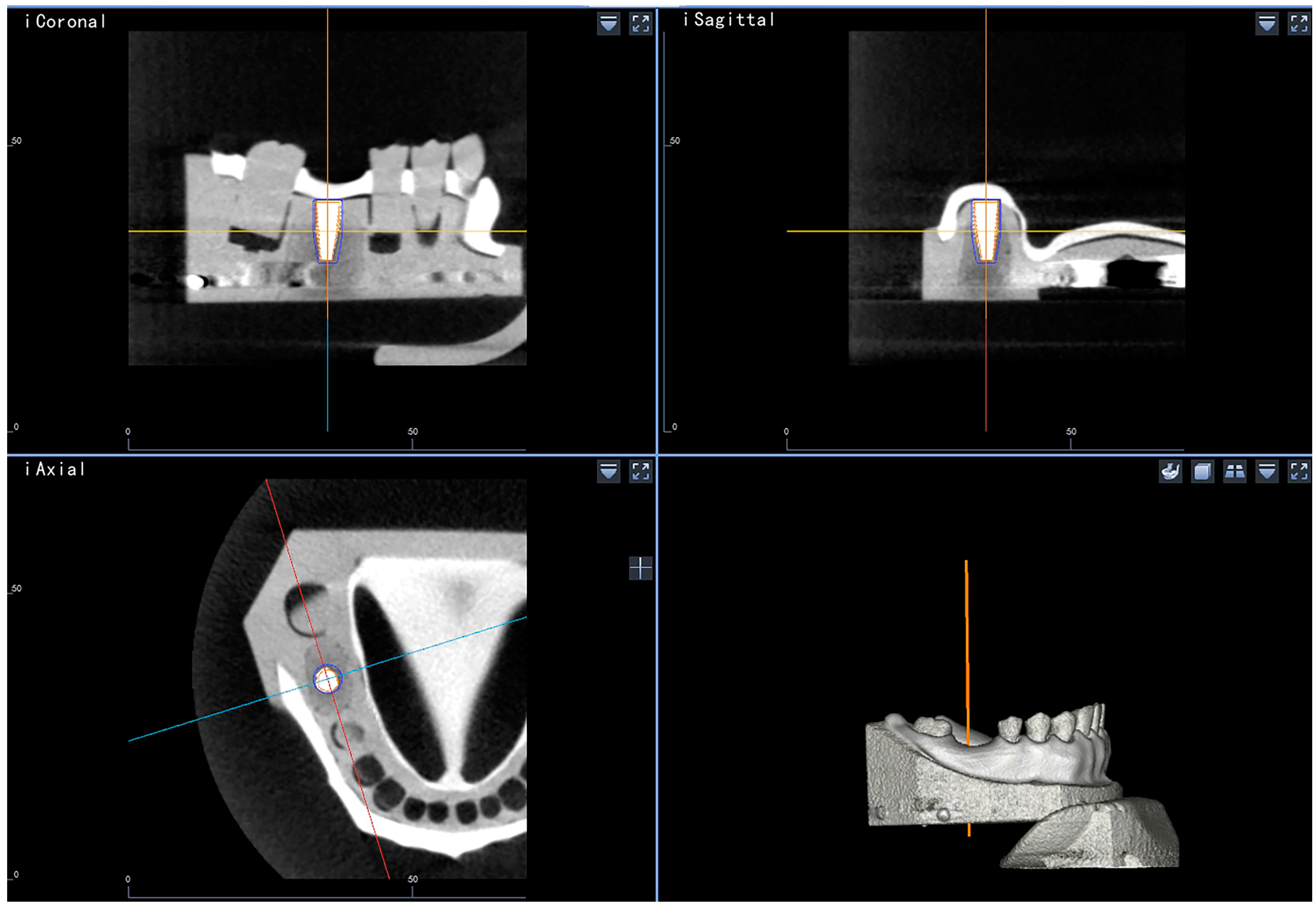
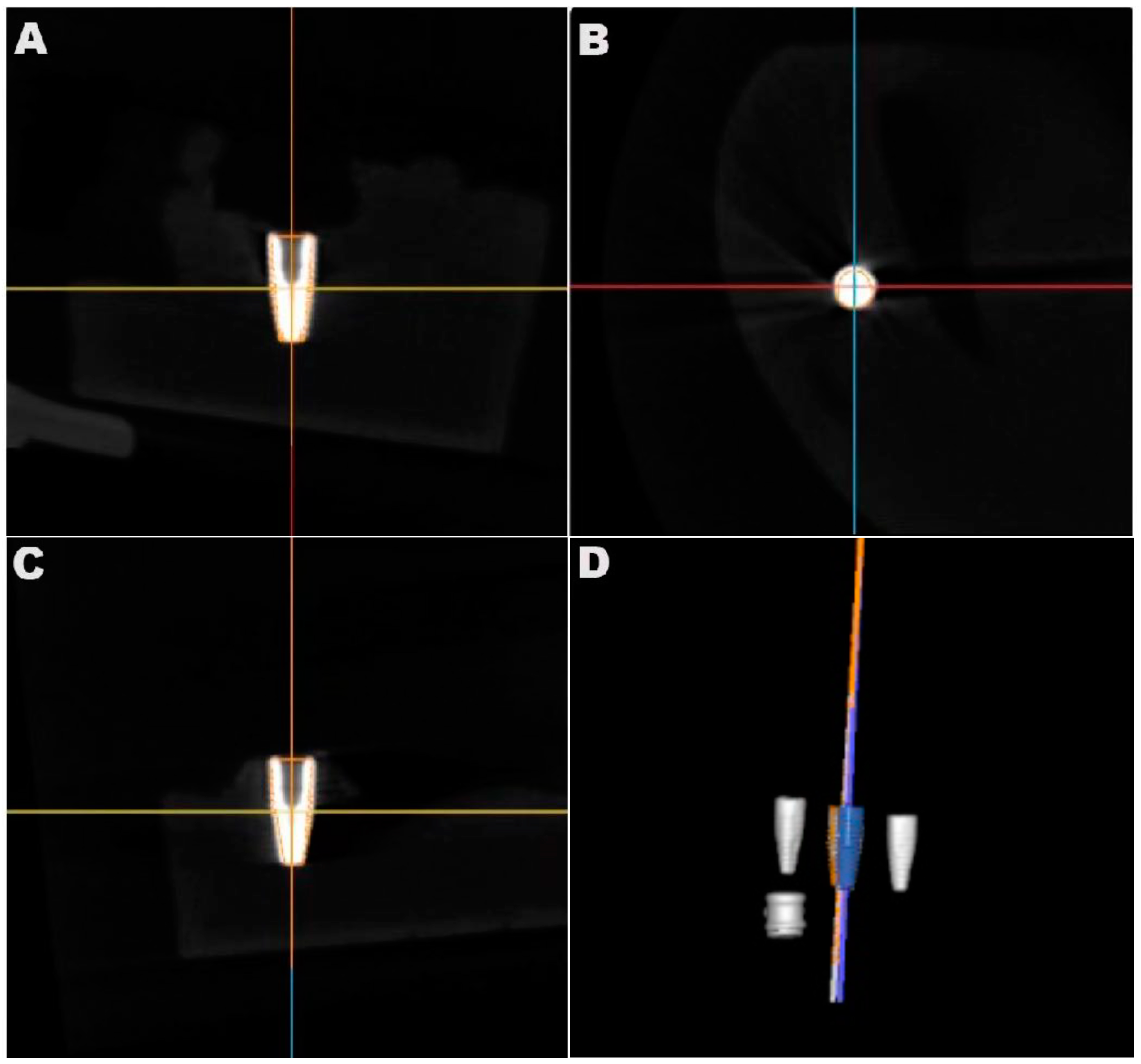
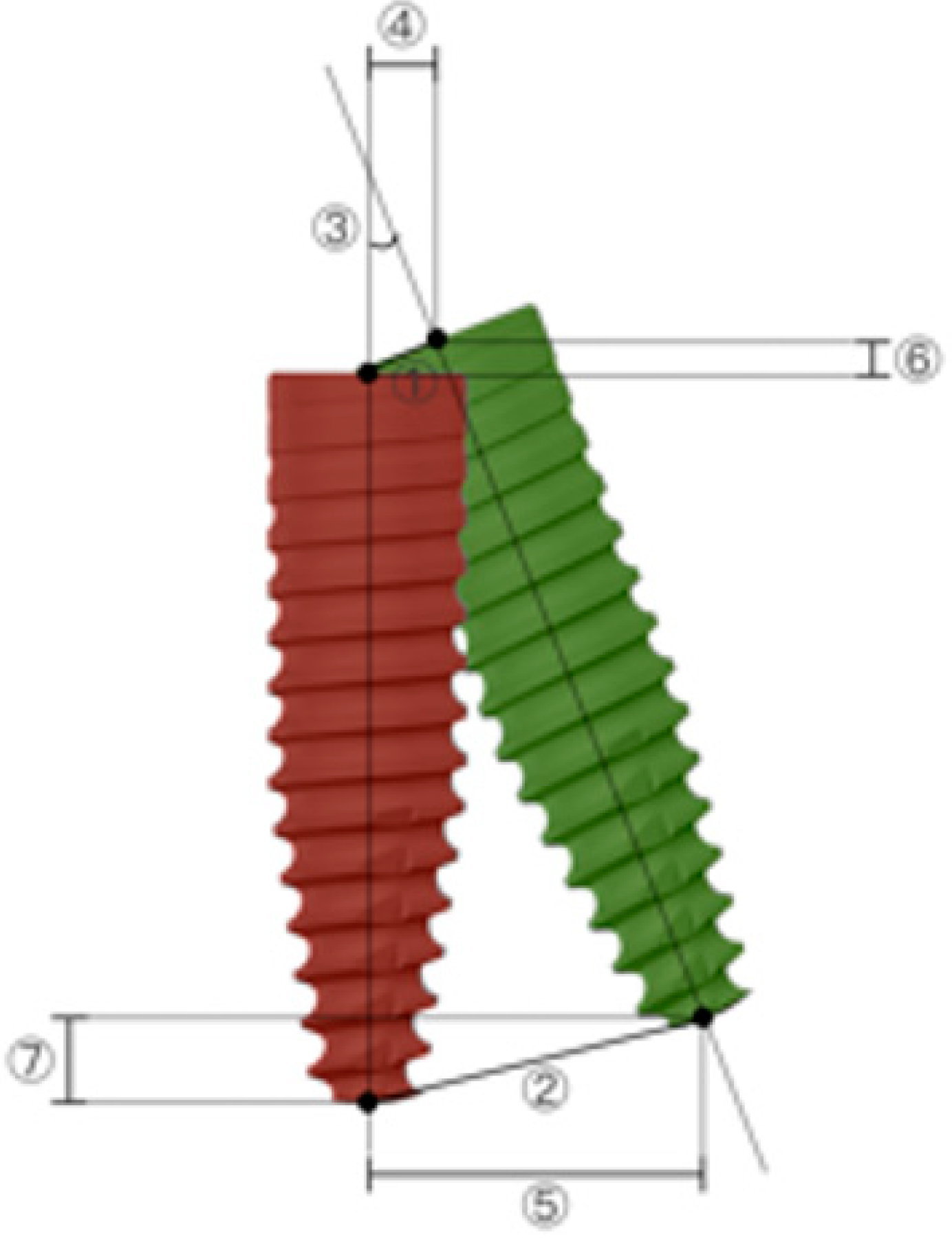
2.4. Accuracy Evaluation
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brägger, U.; Ramseier, C.A.; Salvi, G.E. 10-year survival and success rates of 511 titanium implants with a sandblasted and acid-etched surface: A retrospective study in 303 partially edentulous patients. Clin. Implant. Dent. Relat. Res. 2012, 14, 839–851. [Google Scholar]
- Fang, Y.; An, X.; Jeong, S.M.; Choi, B.H. Accuracy of computer-guided implant placement in anterior regions. J. Prosthet. Dent. 2019, 121, 836–842. [Google Scholar] [CrossRef] [PubMed]
- Son, K.; Huang, M.Y.; Lee, K.B. A method to evaluate the accuracy of dental implant placement without postoperative radiography after computer-guided implant surgery: A dental technique. J. Prosthet. Dent. 2020, 123, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Skjerven, H.; Olsen-Bergem, H.; Rønold, H.J.; Riis, U.H.; Ellingsen, J.E. Comparison of postoperative intraoral scan versus cone beam computerised tomography to measure accuracy of guided implant placement—A prospective clinical study. Clin. Oral Implants Res. 2019, 30, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, R.; Beinsberger, J.; Collaert, B.; Theodorakou, C.; Rogers, J.; Walker, A.; Cockmartin, L.; Bosmans, H.; Jacobs, R.; Bogaerts, R.; et al. Effective dose range for dental cone beam computed tomography scanners. Eur. J. Radiol. 2012, 81, 267–271. [Google Scholar] [CrossRef]
- Al-Ekrish, A.A.; Ekram, M. A comparative study of the accuracy and reliability of multidetector computed tomography and cone beam computed tomography in the assessment of dental implant site dimensions. Dentomaxillofac. Radiol. 2011, 40, 67–75. [Google Scholar] [CrossRef]
- Nickenig, H.J.; Eitner, S. An alternative method to match planned and achieved positions of implants, after virtual planning using cone-beam CT data and surgical guide templates--a method reducing patient radiation exposure (part I). J. Craniomaxillofac. Surg. 2010, 38, 436–440. [Google Scholar] [CrossRef]
- Von See, C.; Wagner, M.E.; Schumann, P.; Lindhorst, D.; Gellrich, N.C.; Stoetzer, M. Non-radiological method for three-dimensional implant position evaluation using an intraoral scan method. Clin. Oral Implants Res. 2014, 25, 1091–1093. [Google Scholar] [CrossRef]
- Stoetzer, M.; Wagner, M.E.; Wenzel, D.; Lindhorst, D.; Gellrich, N.C.; von See, C. Nonradiological method for 3-dimensional implant position assessment using an intraoral scan: New method for postoperative implant control. Implant. Dent. 2014, 23, 612–616. [Google Scholar] [CrossRef]
- Franchina, A.; Stefanelli, L.V.; Maltese, F.; Mandelaris, G.A.; Vantaggiato, A.; Pagliarulo, M.; Pranno, N.; Brauner, E.; Angelis, F.; Carlo, S.D. Validation of an Intra-Oral Scan Method Versus Cone Beam Computed Tomography Superimposition to Assess the Accuracy between Planned and Achieved Dental Implants: A Randomized In Vitro Study. Int. J. Environ. Res. Public Health 2020, 17, 9358. [Google Scholar] [CrossRef]
- DSe-Mok, O.; Du-Hyeong, L. Validation of the Accuracy of Postoperative Analysis Methods for Locating the Actual Position of Implants: An In Vitro Study. Appl. Sci. 2020, 10, 7266. [Google Scholar]
- Colombo, M.; Mangano, C.; Mijiritsky, E.; Krebs, M.; Hauschild, U.; Fortin, T. Clinical applications and effectiveness of guided implant surgery: A critical review based on randomized controlled trials. BMC Oral Health 2017, 17, 150. [Google Scholar] [CrossRef]
- Block, M.S.; Emery, R.W.; Lank, K.; Ryan, J. Implant placement accuracy using dynamic navigation. Int. J. Oral Maxillofac. Implant. 2017, 32, 92–99. [Google Scholar] [CrossRef]
- D’haese, J.; Ackhurst, J.; Wismeijer, D.; De Bruyn, H.; Tahmaseb, A. Current state of the art of computer-guided implant surgery. Periodontology 2000 2017, 73, 121–133. [Google Scholar] [CrossRef]
- Kaewsiri, D.; Panmekiate, S.; Subbalekha, K.; Mattheos, N.; Pimkhaokham, A. The accuracy of static vs. dynamic computer-assisted implant surgery in single tooth space: A randomized controlled trial. Clin. Oral Implants Res. 2019, 30, 505–514. [Google Scholar] [CrossRef]
- Pellegrino, G.; Ferri, A.; Del Fabbro, M.; Prati, C.; Gandolfi, M.G.; Marchetti, C. Dynamic Navigation in Implant Dentistry: A Systematic Review and Meta-analysis. Int. J. Oral Maxillofac. Implant. 2021, 36, e121–e140. [Google Scholar] [CrossRef]
- Wang, F.; Wang, Q.; Zhang, J. Role of dynamic navigation systems in enhancing the accuracy of implant placement: A systematic review and meta-analysis of clinical studies. J. Oral Maxillofac. Surg. 2021, 79, 2061–2070. [Google Scholar] [CrossRef]
- Jorba-García, A.; González-Barnadas, A.; Camps-Font, O.; Figueiredo, R.; Valmaseda-Castellón, E. Accuracy assessment of dynamic computer-aided implant placement: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 2479–2494. [Google Scholar] [CrossRef] [PubMed]
- Edelmann, C.; Wetzel, M.; Knipper, A.; Luthardt, R.G.; Schnutenhaus, S. Accuracy of Computer-Assisted Dynamic Navigation in Implant Placement with a Fully Digital Approach: A Prospective Clinical Trial. J. Clin. Med. 2021, 10, 1808. [Google Scholar] [CrossRef]
- Aydemir, C.A.; Arısan, V. Accuracy of dental implant placement via dynamic navigation or the freehand method: A split-mouth randomized controlled clinical trial. Clin. Oral Implants Res. 2020, 31, 255–263. [Google Scholar] [CrossRef]
- Pei, X.; Liu, X.; Iao, S.; Ma, F.; Li, H.; Sun, F. Accuracy of 3 calibration methods of computer-assisted dynamic navigation for implant placement: An in vitro study. J. Prosthet. Dent. 2022. [Google Scholar] [CrossRef] [PubMed]
- Stopp, S.; Lüth, T. A new X-ray-free measurement method for postoperative 3D-position analysis of navigated inserted implants. Biomed. Technik. Biomed. Eng. 2007, 52, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Ma, F.; Sun, F.; Wei, T.; Ma, Y. Comparison of the accuracy of two different dynamic navigation system registration methods for dental implant placement: A retrospective study. Clin. Implant. Dent. Relat. Res. 2022, 24, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Luebbers, H.T.; Messmer, P.; Obwegeser, J.A.; Zwahlen, R.A.; Kikinis, R.; Graetz, K.W.; Matthews, F. Comparison of different registration methods for surgical navigation in cranio-maxillofacial surgery. J. Cranio Maxillofac. Surg. 2008, 36, 109–116. [Google Scholar] [CrossRef] [Green Version]
- Mediavilla Guzman, A.; Riad Deglow, E.; Zubizarreta-Macho, A.; Agustin-Panadero, R.; Hernandez Montero, S. Accuracy of computer-aided dynamic navigation compared to computer-aided static navigation for dental implant placement: An in vitro study. J. Clin. Med. 2019, 8, 2123. [Google Scholar] [CrossRef] [Green Version]
- Pellegrino, G.; Taraschi, V.; Andrea, Z.; Ferri, A.; Marchetti, C. Dynamic naviga- tion: A prospective clinical trial to evaluate the accuracy of implant placement. Int. J. Comput. Dent. 2019, 22, 139–147. [Google Scholar]
- Stefanelli, L.V.; DeGroot, B.S.; Lipton, D.I.; Mandelaris, G.A. Accuracy of a dynamic dental implant navigation system in a private practice. Int. J. Oral Maxillofac. Implant. 2019, 34, 205–213. [Google Scholar] [CrossRef]
- Wei, S.; Zhu, Y.; Wei, J.; Zhang, C.; Shi, J.; Lai, H. Accuracy of dynamic navigation in implant surgery: A systematic review and meta-analysis. Clin. Oral Implants Res. 2021, 32, 383–393. [Google Scholar] [CrossRef]
- Pellegrino, G.; Bellini, P.; Cavallini, P.F.; Ferri, A.; Zacchino, A.; Taraschi, V.; Marchetti, C.; Consolo, U. Dynamic Navigation in Dental Implantology: The Influence of Surgical Experience on Implant Placement Accuracy and Operating Time. An in Vitro Study. Int. J. Environ. Res. Public Health 2020, 17, 2153. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Minimum | Maximum | Mean | SD | 95% CI | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Entry deviation (mm) | 0.32 | 1.66 | 0.88 | 0.37 | 0.78 | 0.97 |
| Apex deviation (mm) | 0.39 | 1.73 | 1.02 | 0.35 | 0.93 | 1.11 |
| Angular deviation (°) | 0.25 | 3.82 | 1.83 | 0.79 | 1.62 | 2.03 |
| EH (mm) | 0.07 | 1.22 | 0.59 | 0.26 | 0.53 | 0.66 |
| AH (mm) | 0.23 | 1.73 | 0.94 | 0.42 | 0.83 | 1.05 |
| ED (mm) | −3.26 | 2.47 | 0.17 | 1.10 | −0.11 | 0.45 |
| AD (mm) | −3.23 | 3.43 | 0.32 | 1.31 | −0.02 | 0.65 |
| BM | BD | LM | LD | ||
|---|---|---|---|---|---|
| Entry deviation | No. | 19 | 9 | 15 | 17 |
| Value (mm) | 0.59 ± 0.35 | 0.83 ± 0.48 | 0.6 ± 0.24 | 0.7 ± 0.39 | |
| Apex deviation | No. | 11 | 10 | 20 | 19 |
| Value (mm) | 0.94 ± 0.36 | 1.19 ± 0.6 | 0.97 ± 0.48 | 0.97 ± 0.34 |
| Mann–Whitney U Test | |||||
|---|---|---|---|---|---|
| Mean Difference (DE-STG) | SD | p-Value | 95% CI | ||
| Lower | Upper | ||||
| Entry deviation (mm) | 0.07 | 0.10 | 0.433 | −0.13 | 0.28 |
| Apex deviation (mm) | 0.04 | 0.09 | 0.520 | −0.15 | 0.23 |
| Angular deviation (°) | 0.26 | 0.21 | 0.246 | −0.17 | 0.69 |
| EH (mm) | −0.04 | 0.07 | 0.655 | −0.19 | 0.10 |
| AH (mm) | 0.03 | 0.12 | 0.724 | −0.20 | 0.26 |
| ED (mm) | 0.46 | 0.30 | 0.224 | −0.14 | 1.05 |
| AD (mm) | 0.70 | 0.35 | 0.122 | 0.01 | 1.40 |
| t-Test | |||||
|---|---|---|---|---|---|
| Mean Difference (35-36) | SD | p-Value | 95% CI | ||
| Lower | Upper | ||||
| Entry deviation (mm) | −0.06 | 0.12 | 0.624 | −0.31 | 0.19 |
| Apex deviation (mm) | −0.17 | 0.12 | 0.143 | −0.41 | 0.06 |
| Angular deviation (°) | −0.01 | 0.25 | 0.981 | −0.52 | 0.51 |
| EH (mm) | −0.02 | 0.08 | 0.778 | −0.18 | 0.14 |
| AH (mm) | 0.09 | 0.13 | 0.494 | −0.18 | 0.36 |
| ED (mm) | −0.27 | 0.33 | 0.429 | −0.94 | 0.41 |
| AD (mm) | −0.70 | 0.39 | 0.089 | −1.47 | 0.11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, F.; Liu, M.; Liu, X.; Wei, T.; Liu, L.; Sun, F. Proposal and Validation of a New Nonradiological Method for Postoperative Three-Dimensional Implant Position Analysis Based on the Dynamic Navigation System: An In Vitro Study. J. Pers. Med. 2023, 13, 362. https://doi.org/10.3390/jpm13020362
Ma F, Liu M, Liu X, Wei T, Liu L, Sun F. Proposal and Validation of a New Nonradiological Method for Postoperative Three-Dimensional Implant Position Analysis Based on the Dynamic Navigation System: An In Vitro Study. Journal of Personalized Medicine. 2023; 13(2):362. https://doi.org/10.3390/jpm13020362
Chicago/Turabian StyleMa, Feifei, Mingyue Liu, Xiaoqiang Liu, Tai Wei, Lilan Liu, and Feng Sun. 2023. "Proposal and Validation of a New Nonradiological Method for Postoperative Three-Dimensional Implant Position Analysis Based on the Dynamic Navigation System: An In Vitro Study" Journal of Personalized Medicine 13, no. 2: 362. https://doi.org/10.3390/jpm13020362